Congenital Malaria &Elimination &IPTp &Malaria in Pregnancy Bill Brieger | 25 Jun 2015
Congenital malaria: A neglected global health concern
Reena Sethi, DrPH Candidate in International Health, The Johns Hopkins Bloomberg School of Public Health and Senior Monitoring and Evaluation Adviser, Jhpiego shares with us the challenges of malaria acquired from the pregnant mother by their newborn child.
 Strategies and recommendations to prevent the transmission of HIV from a mother to her child are known but less information is available on the epidemiology and management of malaria transmitted from pregnant women to their newborns. As presented in a review of congenital infections, one of the lesser known effects of malaria in pregnancy is the maternal-fetal transmission of infected erythrocytes that can result in poor perinatal outcomes. While clinical malaria in newborns is rare, most likely due to the transplacental transfer of maternal antibodies and the inhibitory effect of fetal hemoglobin on the development of malaria parasites, it is unclear what the true incidence of this condition is in Africa and Asia.
Strategies and recommendations to prevent the transmission of HIV from a mother to her child are known but less information is available on the epidemiology and management of malaria transmitted from pregnant women to their newborns. As presented in a review of congenital infections, one of the lesser known effects of malaria in pregnancy is the maternal-fetal transmission of infected erythrocytes that can result in poor perinatal outcomes. While clinical malaria in newborns is rare, most likely due to the transplacental transfer of maternal antibodies and the inhibitory effect of fetal hemoglobin on the development of malaria parasites, it is unclear what the true incidence of this condition is in Africa and Asia.
Recently published studies in Burkina Faso estimated the incidence of congenital malaria to be 2.1% and the prevalence of mother-to-child transmission of asymptomatic malaria to be 18.5% in one health center in Ouagadougou; in one hospital in Papua, Indonesia, congenital malaria was said to occur in 8 out of 1000 live births from 2005 to 2010; and in a study in one hospital in Madhya Pradesh, India, the incidence of congenital malaria was 29 out of 1000 live births. In a study involving six hospitals in Nigeria, the overall incidence of congenital malaria was found to be 5.1%. Transmission has been associated with both Plasmodium falciparum and Plasmodium vivax. The uncertainty and variation in estimates are likely related to the source of the tested blood (umbilical cord blood or infant peripheral blood), presentation of symptoms that are similar to neonatal sepsis, as well as the lack of capacity to conduct high quality diagnostic tests.
Since congenital malaria results from the transmission of parasites from the mother to the baby (presumably through placental transmission), prevention of malaria through the use of IPTp when appropriate reduces maternal parasitemia, most likely resulting in a lower rate of transmission of malaria to the newborn. In a study in Côte d’Ivoire, factors that protected mothers from placental malaria parasitaemia were the use of IPTp (SP) or ITNs during pregnancy and multigravidity. A study in Ibadan, Nigeria found that IPT-SP was effective in preventing maternal and placental malaria as well as improving pregnancy outcomes among parturient women. Researchers in Southern Ghana reported that placental malaria decreased after the implementation of IPTp.
However, in settings where IPTp is ineffective, the effect of alternative strategies, such as intermittent screening and testing in pregnancy (ISTp) on placental malaria should be examined. Little evidence is currently available on the efficacy of ISTp on maternal and newborn outcomes.
Further research also needs to be conducted in diverse settings to develop a standardized definition for congenital malaria and to understand the short and long-term consequences of this condition in order to establish guidelines for diagnosis and treatment. In pre-elimination contexts, where acquired malaria immunity may be reduced, further evidence is needed on the feasibility of screening all febrile babies and following newborns born to women with malaria during pregnancy and of other possible strategies to improve infant outcomes.
IPTp &ITNs &Monitoring Bill Brieger | 27 Apr 2015
Invest in Using Preventive Services: an Update from the 2014-15 Uganda Malaria Information Survey
 The Demographic and Health Survey people have just released the preliminary MIS results for Uganda. From the viewpoint to the Millennium Development Goals (MDGs), there are cautiously positive signs.
The Demographic and Health Survey people have just released the preliminary MIS results for Uganda. From the viewpoint to the Millennium Development Goals (MDGs), there are cautiously positive signs.
Insecticide treated bednet ownership by households has reached 90%. Equity appears to have been achieved with the households in the lowest, second and third wealth quintiles registering 92%, 94% and 93% ownership. The highest and next highest quintiles had 85% and 88% ownership respectively. Those in the higher wealth quintiles often have better quality housing that of itself offers preventive benefits.
An interesting number is that over 86% of households obtained their nets through campaigns. It appears that the catch up phase of net distribution is repeating itself and the more sustainable keep up phase where nets are provided through routine services has not taken effect.
Household ownership of at least one net translates into use by only 69% of residents generally, and still only 74% in homes that actually own a net. Net use by ‘vulnerable groups’ was a bit better: 74% for children below five years of age and 75& for pregnant women. Thus we can see that household ownership does not guarantee that we meet the 2010 target of 80% coverage/use.
We have moved from recommending two doses of sulfadoxine-pyrimethamine as intermittent preventive treatment for malaria in pregnancy to three or more. The MIS does not report on increased doses but even for two contacts, only 25% of recently pregnant women in Uganda were covered.
The results show that malaria prevention is still an elusive goal. Thirty per cent of children given malaria rapid diagnostic tests during the survey had malaria parasite antigens. We must invest more in ensuring that preventive interventions are routinely available and are actually used before our attention is diverted from the MDGs to the SDGs.
IPTp &Malaria in Pregnancy Bill Brieger | 23 Apr 2015
Burkina Faso: Defeating Malaria by Investing in Expanding Intermittent Preventive Treatment in Pregnancy
 In Burkina Faso, Antenatal Care (ANC) is a national platform for malaria in pregnancy prevention and control. The 2010 Demographic and Health Survey showed a good initial ANC registration rate (95%), but over 56% of pregnant women in rural areas do not register until their second or third trimester. Thus they may have missed the full regimen of ANC services including Long Lasting Insecticide-treated nets and intermittent preventive treatment of malaria in pregnancy (IPTp).
In Burkina Faso, Antenatal Care (ANC) is a national platform for malaria in pregnancy prevention and control. The 2010 Demographic and Health Survey showed a good initial ANC registration rate (95%), but over 56% of pregnant women in rural areas do not register until their second or third trimester. Thus they may have missed the full regimen of ANC services including Long Lasting Insecticide-treated nets and intermittent preventive treatment of malaria in pregnancy (IPTp).
In 2010 only 10.6% of pregnant women nationally and 8.4% in rural areas received two doses of IPTp. Now WHO recommends more doses. This had improved by the time the 2014 Malaria Information Survey was completed to 68% for one dose, 48% for two and 22% for three doses.
Jhpiego’s USAID-supported Improving Malaria Care (IMC) project in Burkina Faso has been providing technical assistance and training to health districts and their ANC staff on implementing updated (2012) WHO IPTp guidelines. The recommended provision of IPTp at every ANC visit from the 13th week of pregnancy onward leads to the possibility of 3 or more doses per woman. The new guidance was incorporated into the update of Burkina Faso’s malaria strategy and has been disseminated since September 2014.
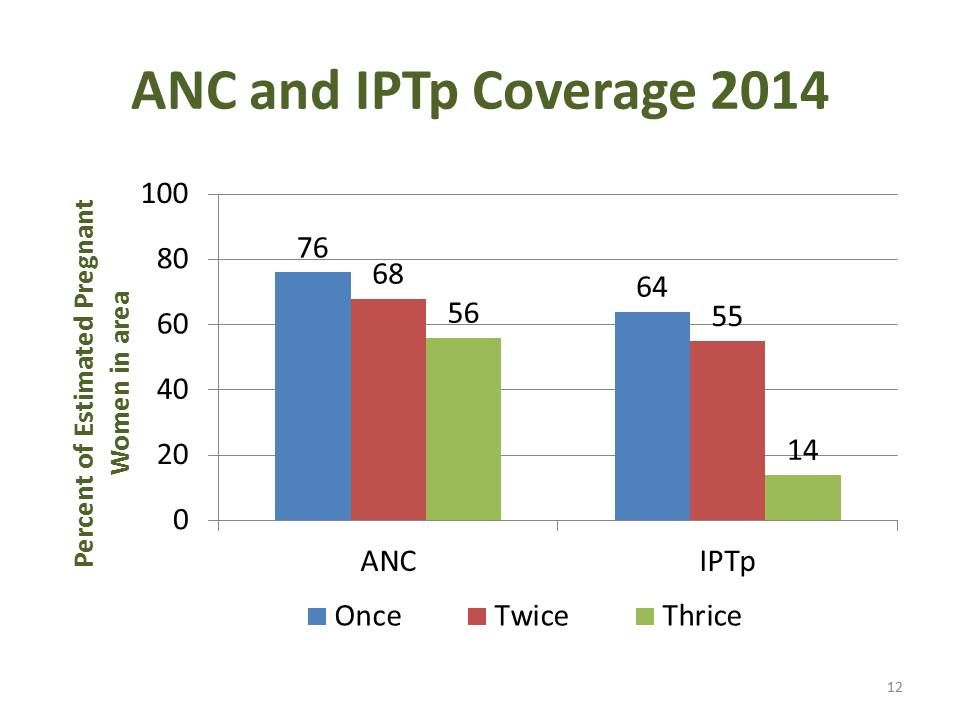 Annual data from the Health Management and information System for 2014 from three districts (Batie, Po and Ouargaye) and 61 health clinics where IMC has been working were collected and summarized. A total of 26,909 women registered for ANC our of the estimated 35,420 in the Three districts.
Annual data from the Health Management and information System for 2014 from three districts (Batie, Po and Ouargaye) and 61 health clinics where IMC has been working were collected and summarized. A total of 26,909 women registered for ANC our of the estimated 35,420 in the Three districts.
The chart at the left shows coverage of ANC visits and IPTp provision based on the estimated 2014 population of pregnant women in the districts. Eleven (17.7%) clinics had not started the updated IPTp guidance. The Ministry of Health also experienced stock-outs of sulfadoxine-pyrimethamine.
Being new IPTp3+ poses challenges and needs greater investment. The IMC project in collaboration with the National Malaria Control Program is examining ways to invest in stronger antenatal malaria prevention including capacity building for ANC staff and provision of IPTp by the existing network of volunteer community health workers.
Advocacy &Drug Quality &Invest in Malaria Control &IPTp &Malaria in Pregnancy &Treatment Bill Brieger | 22 Apr 2015
World Malaria Day 2015 Blog Postings Help #DefeatMalaria
 A special World Malaria Day 2015 Blog has been established. So far nine postings are available at http://www.worldmalariaday.org/blog. Please read and share with colleagues.
A special World Malaria Day 2015 Blog has been established. So far nine postings are available at http://www.worldmalariaday.org/blog. Please read and share with colleagues.
1. “Investing in integrated health services to defeat malaria”BY ELAINE ROMAN, MCSP Malaria Team Lead.
2. “Fake antimalarials: how big is the problem?”
BY DÉBORA MIRANDA, Technical Communications Officer, ACT Consortium (UK).
3. “Why antimalarial medicines matter”
BY PROFESSOR PAUL NEWTON AND ANDREA STEWART, Worldwide Antimalarial Resistance Network and Laos Oxford University Mahosot Hospital Wellcome Trust Research Unit.
4. “Malaria as an entry point for addressing other conditions”
BY HELEN COUNIHAN, Senior Public Health Specialist, Community Health Systems.
5. “Bridging the Care-Seeking Gap with ProAct”
BY MATT McLAUGHLIN, Program Manager of Peace Corps Stomping Out Malaria in Africa initiative.
 6. “Defeating Malaria in Pregnancy”
6. “Defeating Malaria in Pregnancy”
BY CATHERINE NDUNGU, ELAINE ROMAN AND AUGUSTINE NGINDU, Jhpiego.
7. “Intermittent Preventive Treatment, a Key Tool to Prevent and Control Malaria in Pregnancy”
BY CLARA MENÉNDEZ, Director of ISGlobal’s Maternal Child and Reproductive Health Initiative.
8. “Widespread artemisinin resistance could wipe out a decade of malaria investment”
BY TIM FRANCE, Asia Pacific Leaders Malaria Alliance.
9. “The long walk to a malaria-free world”
BY DAVID REDDY, CEO Medicines for Malaria Venture.
IPTp &Malaria in Pregnancy Bill Brieger | 11 Apr 2015
RBM Consensus Statement on Folic Acid Supplementation During Pregnancy
 The Roll Back Malaria (RBM) Partnership Malaria in Pregnancy Working Group supports the following for all pregnant women living in sub-Saharan Africa:
The Roll Back Malaria (RBM) Partnership Malaria in Pregnancy Working Group supports the following for all pregnant women living in sub-Saharan Africa:
In malaria-endemic areas, intermittent preventive treatment using sulfadoxine-pyrimethamine (IPTp-SP) should be provided to pregnant women at each scheduled antenatal care (ANC) visit for protection against malaria. This should start early in the second trimester and continue until the time of delivery, with the doses given at least one month apart [1].
- IPTp-SP has been shown to reduce maternal anemia, antenatal maternal parasitemia, low birthweight infants and neonatal deaths.
- Co-trimoxazole provides some protection through its antimalarial activity; however, IPTp-SP should NOT be given to women who are taking daily co-trimoxazole prophylaxis (i.e. mainly those living with HIV) as this increases the risk of adverse event
Daily oral supplementation of 30–60 mg elemental iron and 400 µg (0.4 mg) folic acid should be provided as early as possible in pregnancy to meet iron and folic acid requirements [2]. In cases where a combined folic acid–iron tablet is not available, a daily dose of 400 µg (0.4 mg) folic acid can be used separately.
There is evidence that high doses of folic acid (i.e. 5,000 µg or more) may interfere with the efficacy of sulfadoxine-pyrimethamine as an antimalarial [3]. The higher 5,000 µg (5 mg) dose for pregnant women should be restricted for use in very specific clinical cases.
High doses of folic acid are not needed during low-risk pregnancies and may counteract the efficacy of both sulfadoxine-pyrimethamine and co-trimoxazole as antimalarials [4]. The RBM Malaria in Pregnancy Working Group strongly advises that countries currently prioritize the procurement and distribution of the available combined dose of 400 µg (0.4 mg) folic acid plus 30–60 mg elemental iron (The current iron and folic acid preparation is 400 ?g (0.4 mg) of folic acid plus 60 mg of elemental iron) as part of routine ANC. It also recommends that countries substantially reduce current stores and supplies of folic acid at a dose of 5,000 µg (5 mg) or higher at all facilities, as this dose should only be used for specific medical conditions as outlined by the World Health Organization (WHO) [2]
References:
- Policy brief for the implementation of intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine (IPTp-SP). Geneva: World Health Organization; 20
- Guideline: daily iron and folic acid supplementation in pregnant w Geneva: World Health Organization; 2012.
- Peters PJ, Thigpen MC, Parise ME, Newman RD. Safety and toxicity of sulfadoxine-pyrimethamine: implications for malaria prevention in pregnancy using intermittent preventive Drug Saf. 2007 June; 30(6):481–501.
- Cotrimoxazole (Septrin) [Internet]. NAM Aidsmap; 2015. Available from: http://www.aidsmap.com/Cotrimoxazole-iSeptrini/page/1731332/
Partners involved in this statement include …

Frequently asked questions about iron and folic acid during pregnancy
1. What daily dose of iron and folic acid supplementation does WHO recommend during pregnancy?
Folate requirements are increased in pregnancy because of the rapidly dividing cells in the fetus and elevated urinary losses. Increased iron is needed to meet the demands for iron of the developing fetus and cell mass expansion. WHO recommends iron and folic acid supplementation for pregnant women, starting early in pregnancy and at a daily dose of 30–60 mg of elemental iron plus 400 µg (0.4 mg) of folic acid, as this has been shown to reduce the risk of low birthweight, maternal anemia and iron deficiency [2]. In settings where anemia in pregnant women is a severe public health problem (i.e. 40 percent or higher) a daily dose of 60 mg of elemental iron is preferred over a lower dose. If a woman is diagnosed with anemia, WHO recommends daily treatment with 120 mg of elemental iron and 400 µg (0.4 mg) of folic acid until her hemoglobin concentration rises to a normal level [5,6].
A combined dose of 60 mg of elemental iron and 400 µg (0.4 mg) of folic acid is included on the WHO Model List of Essential Medicines [7] and is provided by the United Nations Children’s Fund (UNICEF). Using this preparation to treat anemia would provide 800 µg (0.8 mg) of folic acid daily, which would not interfere with sulfadoxine-pyrimethamine as an antimalarial [8]. A trial conducted on pregnant women in Gambia using a 1,500 µg (1.5 mg) daily dose of folic acid showed no reduction in sulfadoxine-pyrimethamine efficacy [9]. However, to date, no data are available on sulfadoxine- pyrimethamine efficacy when administered with daily folic acid doses between 1,500 µg (1.5 mg) and less than 5,000 µg (5 mg) in pregnant women.
Women should be counseled when they receive iron and folic acid supplements to inform them why these supplements are needed, how to take them and for what duration. They should also receive information about how to manage the possible side effects of iron supplementation (mainly mild gastrointestinal symptoms), which may occur in some women.
2. What are the clinical indications for higher dose folic acid during pregnancy?
Folic acid insufficiency is associated with an increased risk of neural tube defects, a debilitating congenital anomaly in which the neural tube does not close properly. This occurs in 0.5–6.5 out of every 1,000 pregnancies. The neural tube forms in the first month after conception, with closure by about 28 days; thus, in order to prevent neural tube defects maternal intake of folic acid should begin before conception and continue through early pregnancy.
There are limited cases (e.g. for prevention of recurrent cases of neural tube defects [10] and for women on anticonvulsant treatment, diabetics and women with sickle cell anemia) where it is recommended that pregnant women take folic acid at a daily dose of 5,000 µg (5 mg).
In particular, women who have had a previous pregnancy resulting in a baby with neural tube defects are at higher risk of having another baby with neural tube defects. These women should receive folic acid at a dose of 5,000 µg (5 mg) a day starting at least one month – though preferably two to three months – before they conceive, and continuing until 12 weeks of gestation, while increasing their dietary folate intake. Given the need for supplementation prior to conception, fortification of staple foods with folic acid should also be considered as a cost-effective public health measure to reduce the incidence of neural tube defects [11].
3. How does folic acid interfere with the efficacy of sulfadoxine- pyrimethamine against malaria?
Folic acid is an essential nutrient for all organisms. Humans get folate from food or dietary supplements. Other organisms, such as the malaria parasite, synthesize folic acid de novo, or endogenously. Both sulfadoxine-pyrimethamine and co-trimoxazole are anti-folates and prevent malaria by blocking the synthesis of folic acid. Without folic acid, the parasite cannot complete its lifecycle. However, if blood folate concentrations are high enough, the malaria parasite can use this folate instead of making its own, allowing the infection to continue unchecked.
Additional References
5. World Health Organization (WHO), United Nations Children’s Fund (UNICEF), United Nations University (UNU). Iron deficiency anaemia assessment, prevention, and control: a guide for programme Geneva: WHO; 2001
6. Iron and folate Integrated Management of Pregnancy and Childbirth (IMPAC). In: Standards for maternal and neonatal care, 1.8. Geneva: World Health Organization; 2007.
7. WHO model list of essential medicines, 18th Geneva: World Health Organization; 2013. Available from: http://apps.who.int/iris/bitstream/10665/93142/1/EML_18_eng.pdf
8. Ouma P, Parise ME, Hamel MJ, et Randomized controlled trial of folate supplementation when treating malaria in pregnancy with sulfadoxine-pyrimethamine. PLoS Clin Trials. 2006 Oct 20; 1:e28. Available from: http://journals.plos.org/plosclinicaltrials/article?id=10.1371/journal.pctr.0010028
9. Mbaye A, Richardson K, Balajo B, et Lack of inhibition of the anti-malarial action of sulfadoxine-pyrimethamine by folic acid supplementation when used for intermittent preventive treatment in Gambian primigravidae. Am J Trop Med Hyg. 2006 Jun; 74(6):960–4. Available from: http://www.ajtmh.org/ content/74/6/960.long
10. Prevention of neural tube Integrated Management of Pregnancy and Childbirth (IMPAC). In: Standards for maternal and neonatal care, 1.5. Geneva: World Health Organization; 2007.
11. World Health Organization (WHO), Food and Agriculture Organization (FAO). Guidelines on food fortification with micr Geneva: WHO; 2006.
Suggested citation: Roll Back Malaria Partnership Malaria in Pregnancy Working Group: Consensus Statement on folic acid supplementation during pregnancy. Geneva; 2015.
IPTp &ITNs &Monitoring &Treatment Bill Brieger | 07 Apr 2015
Highlights from Malawi’s 2014 Malaria Information Survey
Two major forms of malaria data collection help inform national malaria control programs and their supporters about progress and help focus continued resources and interventions. Routine national health information tells us about program implementation on a regular basis. National surveys give us a point-in-time picture of coverage. For the latter, Malawi has been fortunate in recent times to have conducted Malaria Information Surveys every two years.
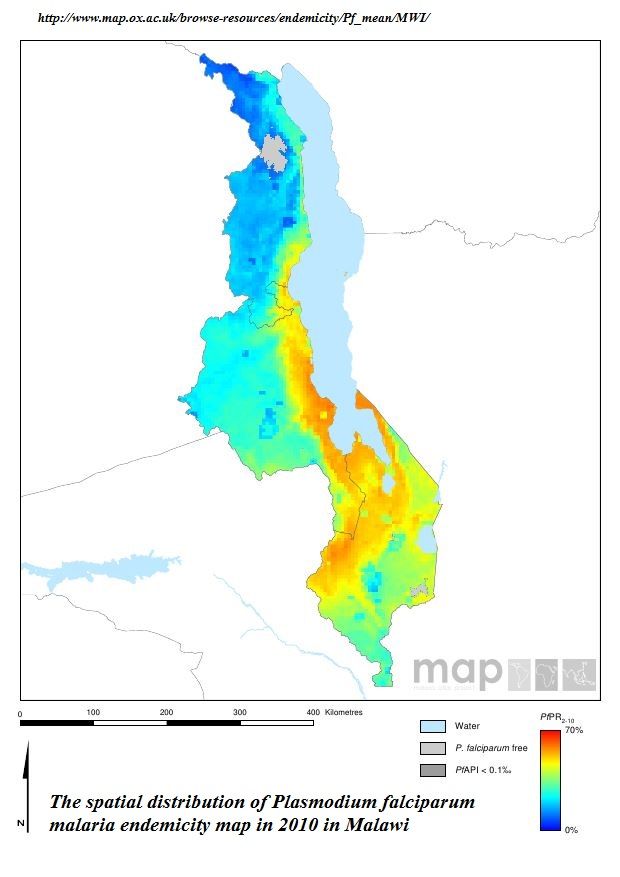 Malawi continues to have endemic malaria as documented by the MAP project in the attached graphic. While some of its neighbors in southern Africa are moving toward elimination, Malawi still experiences prevalence (as measured by rapid diagnostic test) in children below five years of age of 43%, 28% and 33% in 2010, 2012 and 2014 respectively.
Malawi continues to have endemic malaria as documented by the MAP project in the attached graphic. While some of its neighbors in southern Africa are moving toward elimination, Malawi still experiences prevalence (as measured by rapid diagnostic test) in children below five years of age of 43%, 28% and 33% in 2010, 2012 and 2014 respectively.
In the chart below we can see that malaria preventive measures have varied in coverage over the three survey periods and may be said to be on a very slightly upward trend. The Roll Back Malaria target of 80% coverage by 2010 and the US President’s Malaria Initiative target of 85% are still illusive.
In fact, simply having an ITN in the home is no guarantee that people will use it. Overall in 2014 72% of people living in a house with a net slept under one the night before the survey. The rate of use was better for children below five years of age (87%) and pregnant women (85%), but a gap remains.
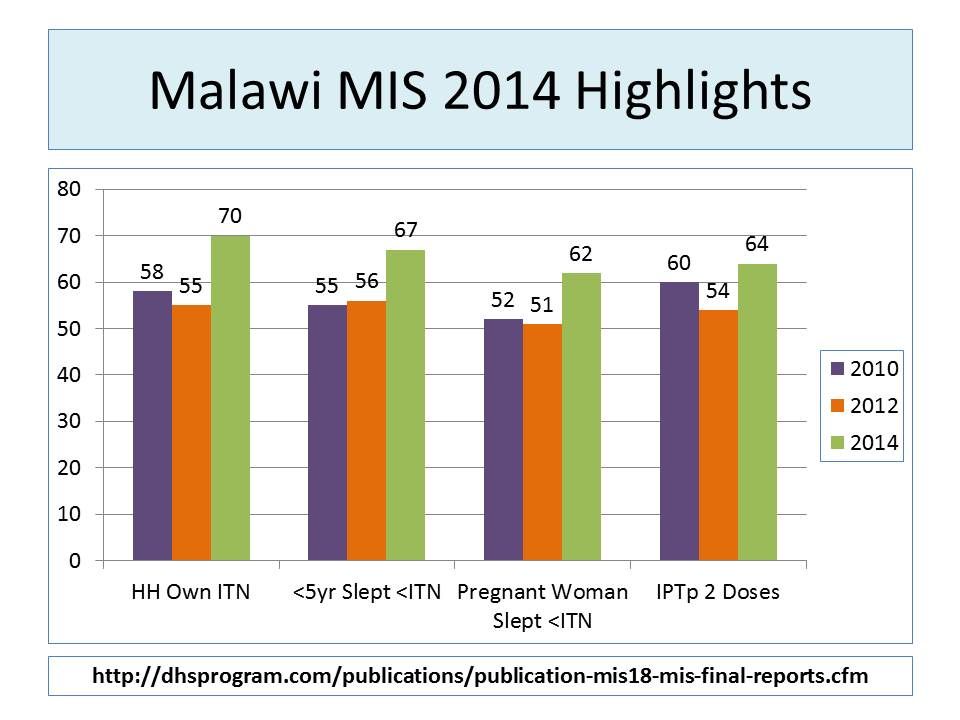 Overall coverage for two doses of sulphadoxine-pyrimethamine (SP) for intermittent preventive treatment in pregnancy (IPTp) remains low. Now that WHO is recommending IPTp with SP during each antenatal care visit after 13 weeks, we are aiming for 3, 4 or more doses. In 2014 89% pregnant women in Malawi received one dose, 63% received two and 12% received three.
Overall coverage for two doses of sulphadoxine-pyrimethamine (SP) for intermittent preventive treatment in pregnancy (IPTp) remains low. Now that WHO is recommending IPTp with SP during each antenatal care visit after 13 weeks, we are aiming for 3, 4 or more doses. In 2014 89% pregnant women in Malawi received one dose, 63% received two and 12% received three.
Malaria treatment for febrile children was the indicator with the best performance (not counting the fact that treatment was not always preceded by a diagnostic test). Most (93%) of children took an artemisinin-based combination therapy (ACT) drug, and 74% took it within a day of fever onset.
The 2014 MIS provides more detailed breakdown by region and socio-economic group, which should be helpful for planning. The major take home message though is that five years after the RBM target dates, many countries, Malawi included, have not been able to scale up and sustain the high intervention coverage needed to bring down mortality and guide us on the pathway to malaria elimination.
As the 2015 Millennium Development Goals are being replaced with a broader development agenda, we hope that malaria will not become a neglected tropical disease again. Actually using data from the MIS to take timely decisions by national programs and donors is essential to keep us on the path.
Health Systems &IPTp &Malaria in Pregnancy Bill Brieger | 07 Nov 2014
Health Systems Strengthening: Achieving Lasting Results for IPTp
 At the Call to Action for Intermittent Preventive Treatment of Malaria in Pregnancy (IPTp) during the just concluded American Society of Tropical Medicine and Hygiene Annual Meeting, Elaine Roman of Jhpiego/MCSP advocated for strengthened health systems as a basic approach to enhancing IPTp coverage. Below is a summary of her remarks.
At the Call to Action for Intermittent Preventive Treatment of Malaria in Pregnancy (IPTp) during the just concluded American Society of Tropical Medicine and Hygiene Annual Meeting, Elaine Roman of Jhpiego/MCSP advocated for strengthened health systems as a basic approach to enhancing IPTp coverage. Below is a summary of her remarks.
Why should we strengthen the Health System? Addressing the health system at all levels leads to improved outcomes and comprehensive coverage. Increasing IPTp uptake requires strengthening antenatal care (ANC) and other components of the health system.
ANC within a strong health system provides an opportunity to improve the health of pregnant women and their newborns. Malaria in pregnancy (MIP) is a maternal and newborn health issue. When health systems are weak, there is greater likelihood of negative consequences on mother and newborn.
 Improving Health Systems for enhanced IPTp addresses the following health systems components:
Improving Health Systems for enhanced IPTp addresses the following health systems components:
- Integration: Reproductive Health Programs and National Malaria Control Programs
- Policies and Guidelines: Consistency across national documents
- Capacity Development: Bother In-Service Training and Pre-Service Education
- Quality Assurance: Linked directly with support supervision
- Community Engagement: Promotion of early ANC and Promotion of IPTp uptake
- Commodities: Ensuring availability at ANC of sulfadoxine-pyrimethamine (SP) and supplies, as well as long-lasting insecticide-treated bed nets
- Monitoring and Evaluation: Facility-level data collection and Data for decision- making
- Finance: Sustained and comprehensive services
 Systems strengthening works. Strengthened Health Systems for IPTp in Kenya resulted from community engagement, training, supervision: leading to IPTp1 coverage of 91.6% and IPTp2 (or more doses) coverage at 61.1%.
Systems strengthening works. Strengthened Health Systems for IPTp in Kenya resulted from community engagement, training, supervision: leading to IPTp1 coverage of 91.6% and IPTp2 (or more doses) coverage at 61.1%.
In Ghana, Capacity development, commodities, community engagement improvements resulted in IPTp2 (or more doses) coverage of 44% to 65%
In Zambia development of clear policy, integrated training, supervision led to IPTp2 (or more doses) coverage increasing from 63% in 2007 to 72% in 2012.
Moving forward we must advocate for strengthening health systems that will lead to increased IPTp uptake and lasting gains. We must focus on ANC, complemented by efforts at community and policy levels. Finally we must address each health system component, based on country context.
IPTp &Malaria in Pregnancy &Private Sector Bill Brieger | 04 Nov 2014
A role for the private sector increasing uptake of intermittent preventive treatment for malaria in pregnancy in Kenya
Jhpiego staff will again present a poster at the Tuesday noon (Nov 4) session of the American Society of Tropical Medicine and Hygiene Annual Meeting. Augustine M. Ngindu, Muthoni M. Kariuki, Sanyu Kigondu, Johnstone Akatu, Isaac M. Malonza, with support from USAID’s Maternal and Child Health Integrated Project (MCHIP) will share experiences with a poster titled, “Improving maternal and neonatal health: Complementary role of the private sector increasing uptake of intermittent preventive treatment for malaria in pregnancy in Kenya.” The abstract is provided below.
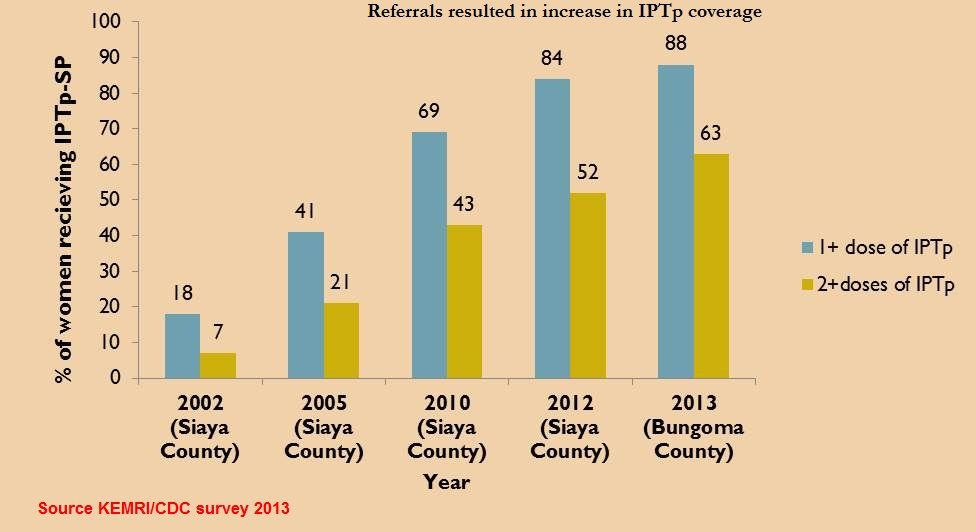
 Malaria in pregnancy (MIP) is associated with poor pregnancy outcomes including maternal anaemia, intrauterine growth retardation and low birth weight. Kenya changed its policy on intermittent preventive treatment using Sulfadoxine Pyrimethamine (IPTp-SP) in 1998. However, IPTp coverage rates have remained low: 4% in 2003, 14% in 2007, 15% in 2008 and 25 % in 2010.
Malaria in pregnancy (MIP) is associated with poor pregnancy outcomes including maternal anaemia, intrauterine growth retardation and low birth weight. Kenya changed its policy on intermittent preventive treatment using Sulfadoxine Pyrimethamine (IPTp-SP) in 1998. However, IPTp coverage rates have remained low: 4% in 2003, 14% in 2007, 15% in 2008 and 25 % in 2010.
To increase the coverage rate, MCHIP supported malaria control and reproductive health divisions of the ministry of health, first to harmonize knowledge among service providers on provision of IPTp-SP in 2011, and second to train community health workers (CHWs) on sensitization of pregnant women to start early antenatal care (ANC) attendance in 2012.
 A community survey conducted in 2013 showed a significant increase in the proportion of pregnant women receiving two or more IPTp doses from 25% to 63%, the highest increase in IPTp uptake since 1998. Following the successful scale up of IPTp, one sub-county conducted an assessment of its health facilities to determine quality of data on ANC clients accessing IPTp-SP.
A community survey conducted in 2013 showed a significant increase in the proportion of pregnant women receiving two or more IPTp doses from 25% to 63%, the highest increase in IPTp uptake since 1998. Following the successful scale up of IPTp, one sub-county conducted an assessment of its health facilities to determine quality of data on ANC clients accessing IPTp-SP.
A total of 15 (58%) out all 26 health facilities in the sub-county (public – 6 out of 8, faith-based – 2 out 3 and private – 7 out of 15) were selected. Data on new ANC clients, revisits and IPTp doses given was collected from the ANC registers.
Among th e assessed health facilities 13 (87%) out of the 15 were registering new ANC cases, revisits and provided IPTp-SP (public 6, faith based 2, private 5. One private clinic provided ANC services to revisits and IPTp2 doses only after the clients had been registered in public facilities, the second did not offer ANC services.
e assessed health facilities 13 (87%) out of the 15 were registering new ANC cases, revisits and provided IPTp-SP (public 6, faith based 2, private 5. One private clinic provided ANC services to revisits and IPTp2 doses only after the clients had been registered in public facilities, the second did not offer ANC services.
In 2013 the government declared provision of free maternity services in public facilities but ANC clients have continued to utilize services from the private sector. This is an indication of the untapped potential in the private sector in increasing access to high impact interventions and importance of supporting the sector by all partners to provide these interventions.
Such complementary efforts if implemented will not only result in enabling the country to move towards achievement of set targets but also improve pregnancy outcomes through reduction in effects of
malaria in pregnancy.
IPTp &Malaria in Pregnancy Bill Brieger | 03 Nov 2014
Call to Action at ASTMH – Intermittent Preventive Treatment of Malaria in Pregnancy
If you are interested in preventing malaria in pregnancy (MIP) join a special symposium at the American Society of Tropical Medicine and Hygiene 2014 Annual Meeting on Wednesday afternoon/evening, November 5th. The seminar is organized by the Malaria in Pregnancy Consortium and the Roll Back Malaria Malaria in Pregnancy Working Group, with support from Medicines for Malaria Venture (MMV) and London School of Hygiene and Tropical Medicine (LSHTM). The agenda can be found below.
SESSION 1 Current coverage and delivery of IPTp 3:45 – 4:15
- Welcome Koki Agarwal, Roll Back Malaria MIP Working Group, Jhpiego / Maternal and Child Survival Program
- Current coverage estimates of IPTp Annemieke van Eijk, Liverpool School of Tropical Medicine
- Factors affecting delivery of IPTp: Findings from quantitative and qualitative studies in Mali and Kenya, Jayne Webster: London School of Hygiene & Tropical Medicine
 SESSION 2 MOVING FORWARD: OPPORTUNITIES TO SCALE UP IPTp: 4:15 – 5.15
SESSION 2 MOVING FORWARD: OPPORTUNITIES TO SCALE UP IPTp: 4:15 – 5.15
- IPTp and WHO’s Global Malaria Programme, Pedro Alonso, Global Malaria Programme of the World, Health Organization
- Interventions to improve uptake of IPTp in Ghana, Harry Tagbor, Kwame Nkrumah University of Science & Technology
- Studies of cost-effectiveness of IPTp-SP: IPTp-SP2 vs. placebo in Mozambique and a meta analysis of IPTp-SP3 + vs. SP2 in a range of African settings, Elisa Sicuri Barcelona Centre for International Health Research
- Can acceptability be enhanced? Findings from quantitative and qualitative studies on IPTp against malaria and curable STIs/RTIs, Matthew Chico, London School of Hygiene & Tropical Medicine
- Delivering IPTp in the antenatal care platform, Kate Mitchell, Harvard School of Public Health/ Maternal, Health Task Force
- Health systems strengthening: Achieving lasting results for IPTp, Elaine Roman. Jhpiego / Maternal and Child Health Program
SESSION 3 Call to Action: 5:15 – 6:00
- Defining the Call to Action (group facilitation) – Koki Agarwal, Roll Back Malaria MIP Working Group, Jhpiego / Maternal and Child Survival Program, Intermittent Preventive Treatment of Malaria in Pregnancy
Community &IPTp Bill Brieger | 03 Nov 2014
Prevention of Malaria in Pregnancy with Community Health Volunteers in Kenya: Jhpiego at ASTMH
 Augustine M. Ngindu of Jhpiego’s USAID-MCHIP Project in Nairobi, Kenya will present a poster entitled, “Prevention of Malaria in Pregnancy: Community Health Volunteers (CHVs) promote community-based activities to increase uptake of Intermittent Preventive Treatment of malaria in pregnancy (IPTp) in Kenya,” at the ASTMH Annual Meeting at noon on Monday 3 October. Below is the abstract – stop by the session to learn more.
Augustine M. Ngindu of Jhpiego’s USAID-MCHIP Project in Nairobi, Kenya will present a poster entitled, “Prevention of Malaria in Pregnancy: Community Health Volunteers (CHVs) promote community-based activities to increase uptake of Intermittent Preventive Treatment of malaria in pregnancy (IPTp) in Kenya,” at the ASTMH Annual Meeting at noon on Monday 3 October. Below is the abstract – stop by the session to learn more.
Malaria in pregnancy is associated with poor pregnancy outcomes including maternal anaemia, miscarriages and intrauterine growth retardation. In an effort to increase IPTp coverage, Kenya is implementing the community strategy by using community health volunteers (CHVs) to promote community-based activities to increase uptake of malaria in pregnancy interventions (MIP).
 The CHVs visit each household every month to register new pregnant women, collect data from existing pregnant women including last IPTp dose taken and gestation, sensitize them to continue ANC visits and refer late starters and defaulters of scheduled ANC visits.
The CHVs visit each household every month to register new pregnant women, collect data from existing pregnant women including last IPTp dose taken and gestation, sensitize them to continue ANC visits and refer late starters and defaulters of scheduled ANC visits.
In Bungoma sub-county with a catchment population of 169,000, 382 CHVs from 14 community units identified a total of 4,925 (95%) out of an expected 5,092 pregnant women and followed them up between February to April 2014.
In Kenya the recommended time for starting IPTp is from weeks of pregnancy or after quickening.
 Results showed that among the registered pregnant women 92% had taken at least IPTp1 and 61% IPTp2 doses respectively. IPTp doses taken by weeks of pregnancy showed that 1.3% had accessed IPTp by 16 weeks of pregnancy, 8.6% between 16-20 weeks, 4.7% between 21-25 weeks, 5.7% between 26-30 weeks, 6.5% between 31-35 weeks and 3.7 % between 36-40 weeks.
Results showed that among the registered pregnant women 92% had taken at least IPTp1 and 61% IPTp2 doses respectively. IPTp doses taken by weeks of pregnancy showed that 1.3% had accessed IPTp by 16 weeks of pregnancy, 8.6% between 16-20 weeks, 4.7% between 21-25 weeks, 5.7% between 26-30 weeks, 6.5% between 31-35 weeks and 3.7 % between 36-40 weeks.
 However, 1.5% had not started IPTp at 40 weeks of pregnancy. The data further showed that among those who started IPTp early 1% completed 7 IPTp doses at 40 weeks of pregnancy.
However, 1.5% had not started IPTp at 40 weeks of pregnancy. The data further showed that among those who started IPTp early 1% completed 7 IPTp doses at 40 weeks of pregnancy.
CHVs can be used to effectively promote community-based activities including collection of data on the number of IPTp doses taken during pregnancy, which is a good indicator of the proportion of pregnant women protected against the adverse effects of malaria during pregnancy. This practice if scaled up can serve as an alternative method of monitoring coverage rates of interventions without waiting for the 3-5 year community survey data