Health Systems &Human Resources &IPTp &Malaria in Pregnancy &Monitoring Bill Brieger | 03 Nov 2014
Jhpiego at ASTMH: Performance Quality Improvement for IPTp in Kenya
Monday afternoon (3 October 2014) at the American Society for Tropical Medicine and Hygiene Annual Meeting in New Orleans, Jhpiego and USAID/PMI are sponsoring a panel on “Integrating and Innovating: Strengthening Care for Mothers and Children with Infectious Diseases.” If you are at the meeting please attend to learn more about our Malaria activities in Kenya.
 One of the panel presentations is “Performance Quality Improvement Lending to Corrected Documented Outcomes for Intermittent Preventive Treatment in Kenya,” by Jhpiego staff Muthoni Kariuki, Augustine Ngindu Isaac Malonza, and Sanyu Kigondu, who are working with USAID’s Maternal & Child Health Integrated Project (MCHIP).
One of the panel presentations is “Performance Quality Improvement Lending to Corrected Documented Outcomes for Intermittent Preventive Treatment in Kenya,” by Jhpiego staff Muthoni Kariuki, Augustine Ngindu Isaac Malonza, and Sanyu Kigondu, who are working with USAID’s Maternal & Child Health Integrated Project (MCHIP).
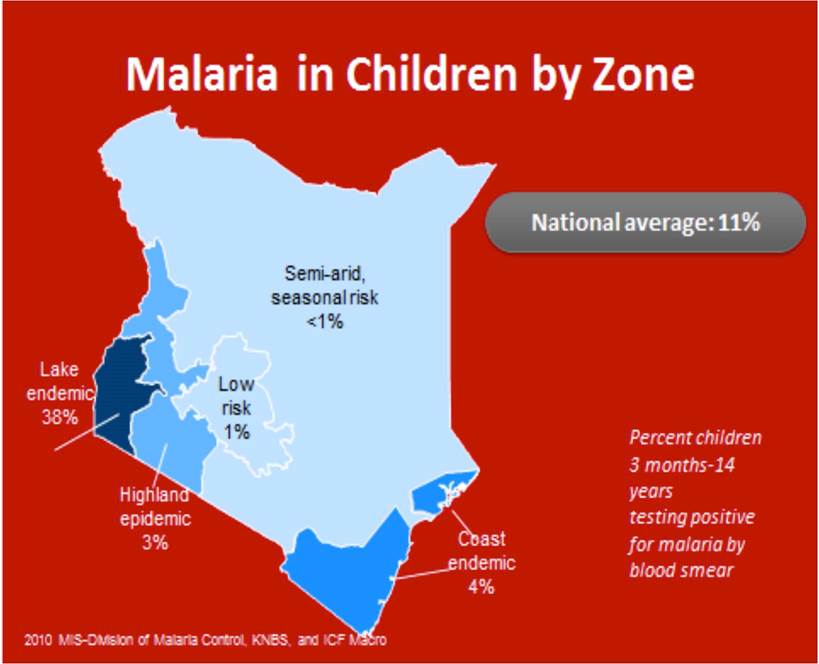
According to Malaria policy in Kenya all pregnant women in malaria endemic areas receive free intermittent preventive treatment with SP have access to free malaria diagnosis and treatment when presenting with fever have access to LLINs (National Malaria Strategy (NMS) 2009–2017).
By 2013 80% of people living in malaria risk areas should be using appropriate malaria preventive interventions. Intermittent Preventive Treatment of malaria in pregnancy using Sulfadoxine Pyrimethamine (IPTp-SP) intervention is recommended for use in malaria endemic region.
 MCHIP broadly implemented Capacity Development and service delivery and improvement interventions that also had impact on the delivery of malaria in pregnancy services through collaboration with the Ministry of Health divisions/units at national level: (malaria, reproductive health, community health).
MCHIP broadly implemented Capacity Development and service delivery and improvement interventions that also had impact on the delivery of malaria in pregnancy services through collaboration with the Ministry of Health divisions/units at national level: (malaria, reproductive health, community health).
At county level scale up provision of IPTp at facility level took place in 14 malaria endemic counties. This included 8 counties in the lake endemic region including Bondo sub-county (the MCHIP model sub-county) and 6 in the coastal endemic region.
Quality Improvement through Performance Quality Improvement (PQI) process was instituted to enhance service delivery. The MCHIP era in Bondo Strengthened ANC Services using the following:
- Development of MIP Standards-Based Management and Recognition (SBM-R) standards
- Orientation of facility in-charges, supervisors and service providers on the standards
- Monitoring of IPTp uptake using DHIS2 data
- Feedback to facility in-charges and supervisors on DHIS2 findings
- Collection of ANC data from ANC registers (2011-2013)
- Feedback to facility in-charges and supervisors on ANC data
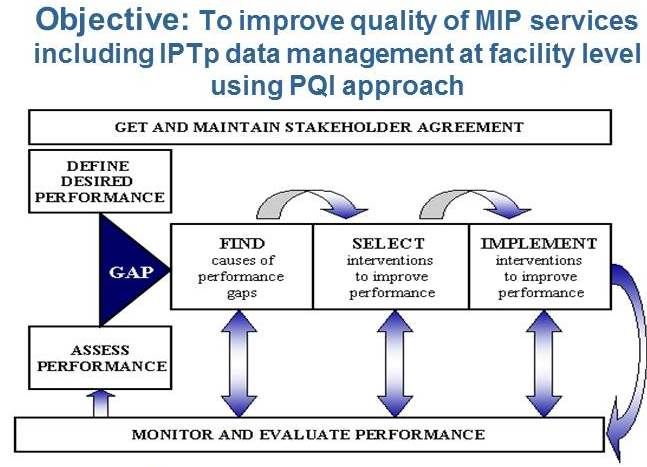
Quality improvement in the malaria in pregnancy component was undertaken with the objective to improve quality of MIP services including IPTp data management at facility level using PQI approach. An Example of a MIP SBM-R standard is seen below.
 In-service training focused on orientation of facility in-charges on PQI who then continued orientation at Facility Level. Overall we oriented 1200 facility in-charges and 100 supervisors on the standards. Facility in-charges cascaded orientation to 2,441 service providers.
In-service training focused on orientation of facility in-charges on PQI who then continued orientation at Facility Level. Overall we oriented 1200 facility in-charges and 100 supervisors on the standards. Facility in-charges cascaded orientation to 2,441 service providers.
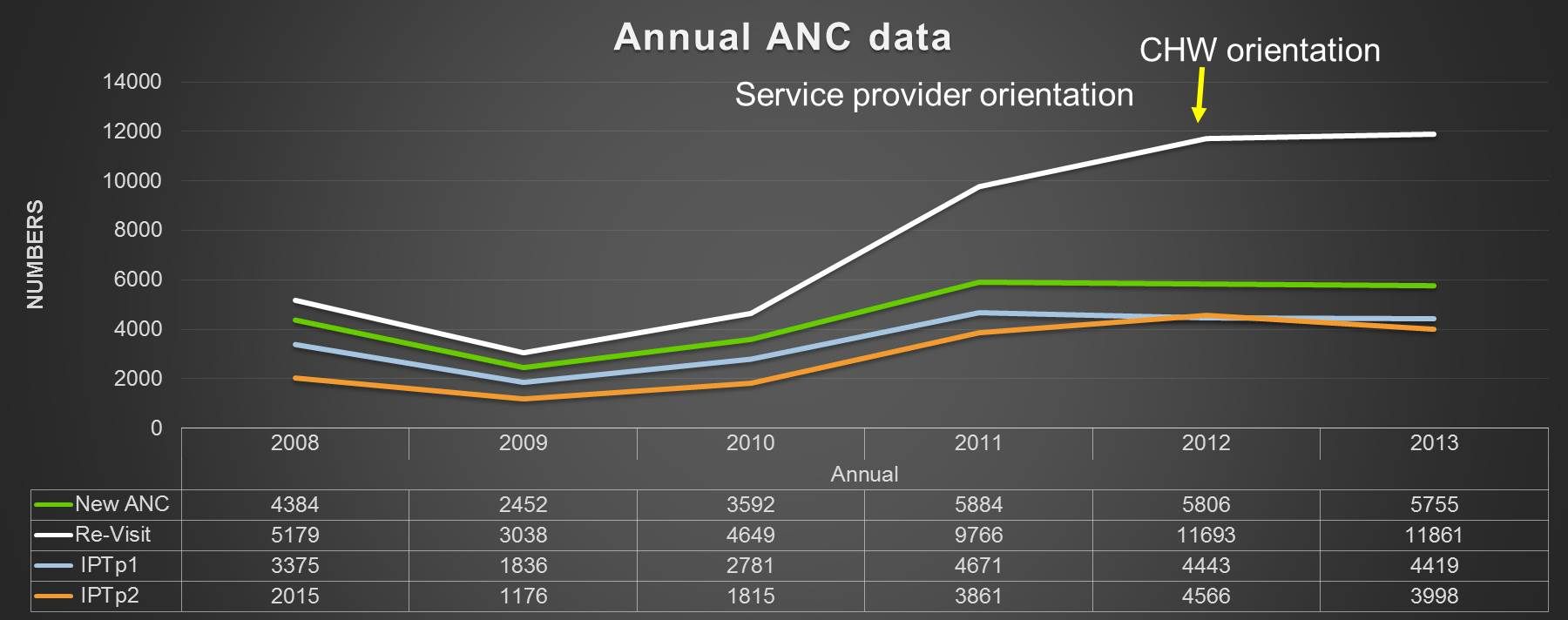 We then analysed ANC data from DHIS (2011-2013) indicated proportion of pregnant women receiving IPTp2 was higher than IPTp1 (IPTp2+ doses reported as IPTp2 dose). We helped improve reporting by service providers not oriented on use of the ANC register in order to reduce data errors.
We then analysed ANC data from DHIS (2011-2013) indicated proportion of pregnant women receiving IPTp2 was higher than IPTp1 (IPTp2+ doses reported as IPTp2 dose). We helped improve reporting by service providers not oriented on use of the ANC register in order to reduce data errors.
In conclusion, PQI is a best practice in provision of MIP services. Standardization of knowledge among service providers is essential in provision of quality MIP services. Development of facility in-charges as mentors in the facility to ensure continued orientation of new service providers.
Use of appropriate monitoring tools is necessary to assist in assessment of quality of services provided including data management. Feedback to service providers is one of the performance rewards and encourages participation in knowledge acquisition
Congenital Malaria &IPTp &ITNs &Malaria in Pregnancy &Mortality Bill Brieger | 12 Jun 2014
Congenital Malaria, an Underappreciated Neonatal Problem
The largest portion of infant deaths occurs in the neonatal period. During those first 28 days, the child is at risk from a variety of problems arising from delivery complications, infections and simply not being kept warm.
 In malaria endemic areas there is the small but important problem of malaria transferred from mother to child, or congenital malaria. The problem occurs with both Plasmodium vivax and falciparum.
In malaria endemic areas there is the small but important problem of malaria transferred from mother to child, or congenital malaria. The problem occurs with both Plasmodium vivax and falciparum.
Congenital malaria in the newborn is often hard to detect. There may be fever, but other signs and symptoms might include anaemia, jaundice, paleness, diarrhoea, vomiting, and general weakness.
Prevalence of congenital malaria in Ghana, for example, ranged from 2% by microscopy to 12% using polymerase chain reaction (PCR). In India microscopy revealed a prevalence of 3% with cases of both vivax and falciparum.
One would hope this problem could be avoided if prevention of malaria in pregnancy was practiced using insecticide treated nets, intermittent preventive treatment (IPTp) and prompt and appropriate case management, but studies still find placental and cord parasiteamia in countries where such interventions are supposed to be integrated into antenatal/prenatal care. In Colombia, “An association was found between congenital malaria and the diagnosis of malaria in the mother during the last trimester of pregnancy or during delivery, and the presence of placental infection.”
Countries are in the process of shifting to the relatively new WHO guidance on IPTp that encourages monthly doses of sulfadoxine-pyrimethamine from the beginning of the second trimester up until delivery. Countries are also trying to ensure universal coverage of ITNs so that women will be using nets prior to even becoming pregnant.
We still have trouble administering to take just two doses of IPTp, but if we want to prevent congenital malaria, we need to ensure that women are protected from malaria in their placentas and are free from parasites right up until they give birth and thereby prevent another cause of neonatal mortality.
IPTp &Malaria in Pregnancy Bill Brieger | 19 Apr 2014
Finding a Practical Approach to Folic Acid Supplementation and Intermittent Preventive Treatment of Malaria for Pregnant Women
 n 2012 the World Health Organization’s Global Malaria Program reconfirmed the use of intermittent preventive treatment for pregnant women (IPTp) using sulfadoxine-pyrimethamine (SP). IPTp now may be given at each antenatal care (ANC) visit after the first trimester as long as it is a month since the last dose.
n 2012 the World Health Organization’s Global Malaria Program reconfirmed the use of intermittent preventive treatment for pregnant women (IPTp) using sulfadoxine-pyrimethamine (SP). IPTp now may be given at each antenatal care (ANC) visit after the first trimester as long as it is a month since the last dose.
Countries have been moving forward in reviewing and adapting/adopting this guidance where appropriate. One of the key challenges countries have faced is what to do about folic acid, which is given concurrently with IPTp as part of focused ANC. Specifically the guidance states … WHO recommends the administration of folic acid at a dose of 0.4 mg daily; this dose may be safely used in conjunction with SP. Folic acid at a daily dose equal or above 5 mg should not be given together with SP as this counteracts its efficacy as an antimalarial.
This new low dose formulation of folic acid requires accessible and affordable supplies made available through a country’s pharmaceutical procurement system. Manufacturers would need to adjust, and national food and drug approval agencies would need to register the product(s).
All this worry may in fact be a case of closing the barn door after the horses have escaped. Since in many countries women do not register for antenatal care until well into their second trimester, the benefits of folic acid supplementation may in fact me missed. A broader view of the health and nutrition of women of reproductive age is needed, not just the narrow focus of giving folic acid as part of ANC.
The online encyclopedia of Medline explains that “There is good evidence that folic acid can help reduce the risk of certain birth defects (spina bifida and anencephaly). Women who are pregnant or planning to become pregnant should take at least 400 micrograms (mcg) of a folic acid supplement every day.” Let’s look at the term “planning to become pregnant.” This means that women of reproductive age (WRA) who are interested in having children need to ensure that taking folic acid. Since many pregnancies are not “planned” this means folic acid should be a regular part of their lives.
How can this be achieved? First, while it may not be practical, WRA could take regular folic acid tablets. A variety of health and social programs, including secondary schools for those who attend, may be venues to try distribution of supplements. Secondly there are food sources, and thirdly there could be fortification of commercial foods with folic acid.
Again the Medline encyclopedia informs us that, “Folate occurs naturally in the following foods: dark green leafy vegetables, dried beans and peas (legumes), and citrus fruits and juices.” These items are often available in malaria endemic countries and part of a normal diet. Of course, as the American Journal of Clinical Nutrition points out, “Naturally occurring seasonal variations in food consumption patterns have a profound effect” on the availability, cost and use of these food sources.
While commercial food fortification is common in industrialized countries, IRIN also points out that, “use local manufacturers and commercial distribution systems to reach undernourished children in Nigeria, Ghana and Tanzania. All three countries have mandatory fortification of wheat flour with iron and zinc.” Why not add folic acid? Researchers in Kenya found that “Locally available indigenous foods can be used in the formulation of acceptable, low-cost, shelf-stable, nutritious supplementary foods for vulnerable groups,” including folic acid fortification.
We should now focus our attention of the folic acid needs of WRA generally. We must plan for the three possible interventions mentioned above as appropriate to each country and as an ongoing effort to ensure women’s overall health and nutrition. If we succeed, women in malaria endemic countries will enter pregnancy with a strong foundation of folic acid supplementation and not have to depend solely on tablets during the short window when they attend ANC.
Elimination &IPTp &ITNs &Treatment Bill Brieger | 06 Dec 2013
Draft Nigeria 2013 DHS Shows Slow Progress for Malaria
The Nigeria Demographic and Health Survey (DHS) 2013 Draft Preliminary Report from the National Population Commission, Abuja, Nigeria and MEASURE DHS, ICF International, Calverton, Maryland, USA was released in-country in September 2013. These are the same organizations that conducted the 2010 Malaria Information Survey (MIS).
From the malaria perspective this has been a long anticipated event since the country has distributed over 60 million long lasting insecticide-treated nets since 2009. The 2010 MIS showed some progress over the 2008 DHS, but since it took place near the beginning of the massive net distribution effort, there was hope that a subsequent survey would highlight an improvement. If that were the expectation, people will be quite disappointed.
Lets start with nets. Our attached table shows only a slight improvement in the proportion of households owning at least one net. The idea behind the massive net campaigns from 2009-12 were achievement of universal coverage where there would be at least one net for every two people in a household. Where did these nets go? Were they damaged beyond use in the relatively short time that elapsed?
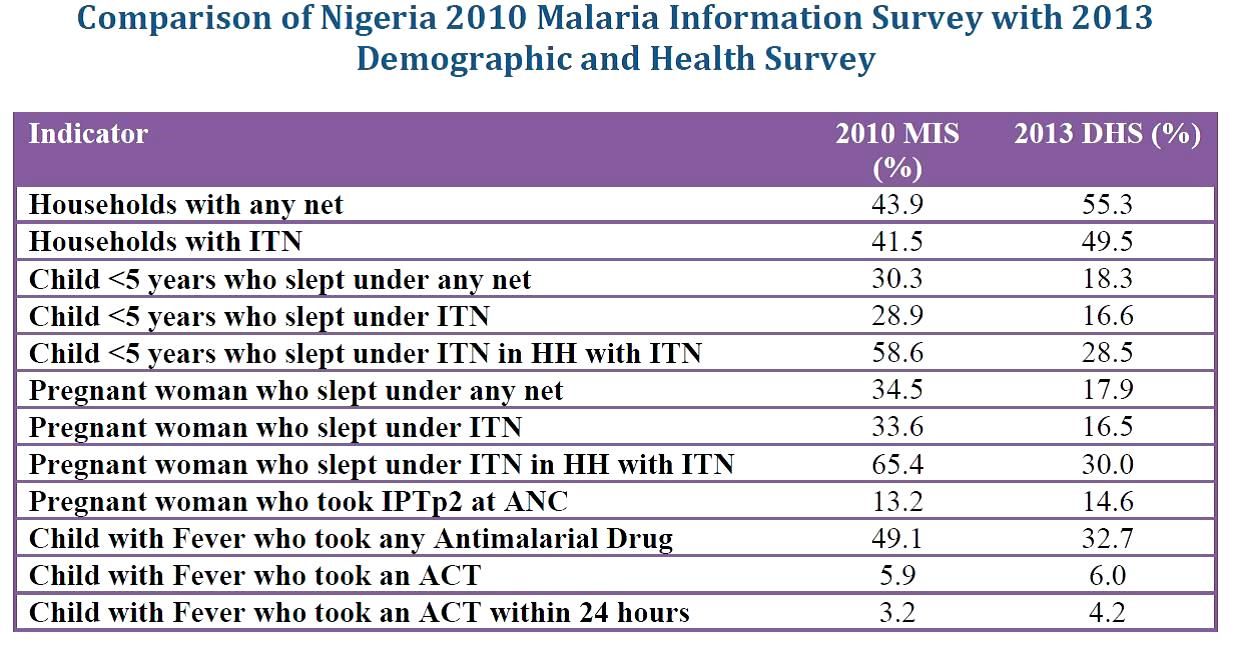 What is more disappointing is that th proportion of young children and pregnant women sleeping under an insecticide treated net (ITN) reduced to just slightly over half of the 2010 figure. This reduction also happened even in households that actually owned ITNs. This is mysterious to say the least.
What is more disappointing is that th proportion of young children and pregnant women sleeping under an insecticide treated net (ITN) reduced to just slightly over half of the 2010 figure. This reduction also happened even in households that actually owned ITNs. This is mysterious to say the least.
Prevention of malaria in pregnancy has been a neglected part of malaria control in many countries, but since the drug used for intermittent preventive treatment (IPT), sulphadoxine-pyrimethamine (SP) is so cheap, it was assumed that most health systems could afford to guarantee every woman attending antenatal care the required dosed. Unfortunately the status of IPT showed almost no improvement between 2010 and 2013 and remained far, far below the 2010 Roll Back Malaria target of 80% coverage. SP is produced in Nigeria; why can it not reach pregnant women?
Finally appropriate malaria treatment of young children is also in the doldrums. The actual number of children who received any anti-malarial drug declined, while those receiving the appropriate artemisinin-based combination therapy (ACT) remained essentially level at around 6%. Where have all the ACTs brought in through Global Fund, the US President’s Malaria Initiative and other donors gone? How can we expect infant and child mortality to decrease in the absence of appropriate treatment for one of the most common child killer diseases?
At the recently concluded 6th Pan African Malaria Conference in Durban, South Africa, participants were told that the only way to truly eliminate malaria is to tackle the high burden countries like Nigeria head on. If these data indicate how we are waging the malaria battle in Nigeria, our hopes for elimination in the near future will be dashed.
IPTp &Malaria in Pregnancy &Reproductive Health Bill Brieger | 21 Nov 2013
Malaria Products Must be Included in Life Saving Commodities for RMNCH
According to the Every Woman Every Child website (EWEC), “A strong focus on reproductive, maternal, child and newborn health (RMCNH) is integral to improving global health. RMNCH is linked to all 8 Millennium Development Goals (MDGs). MDGs 4 (Reduce Child Mortality), 5 (Improve Maternal Health) and 6 (combat HIV/AIDS, malaria and other diseases) each have specific targets and indicators related to RMNCH.” In order to achieve these goals life saving commodities must be made available to all women and children, and as implied in the statement above, they must include commodities that prevent and treat malaria in pregnancy.
The website further states that, “Based on these criteria, an initial list of 13 affordable, effective, but underutilized life-saving commodities were identified for consideration by the Commission. The UN Commission on Life-Saving Commodities for Women and Children aims to increase access to life-saving medicines and health supplies for the world’s most vulnerable people.” Ironically this suggestive list does not include medicine for intermittent preventive treatment of malaria in pregnancy (IPTp), insecticide treated nets (ITNs), malaria rapid diagnostic tests or artemisinin-based combination therapy medicines for malaria treatment.
Yes the list is only suggestive, and yes it is a global list, but WHO estimates that nearly 50 million women will become pregnant in malaria endemic areas each year. That’s a pretty big chunk of the world’s population to neglect.
EWEC does refer to two partner documents for more details on these essential commodities. One document is “The Essential Interventions, Commodities and Guidelines for Reproductive, Maternal, Newborn and Child Health – A global review of the key interventions related to reproductive, maternal, newborn and child Health.” This document mentions generically “Prevention and management of malaria with insecticide treated nets and antimalarial medicines.”
 The second document, “Priority medicines for mothers’ and children’s health, 2011”, also identifies medicines that are in need of enhanced attention and utilization in order to avoid preventable deaths of women and children. This document mentions that commodities exist for malaria services, but refers the reader to the very detailed Global Malaria Program’s “Guidelines for the treatment of malaria” (2nd ed. Geneva, World Health Organization, 2010) that discusses medications for all species of Plasmodium and does not have an easy to view take away on the essential life saving commodities within.
The second document, “Priority medicines for mothers’ and children’s health, 2011”, also identifies medicines that are in need of enhanced attention and utilization in order to avoid preventable deaths of women and children. This document mentions that commodities exist for malaria services, but refers the reader to the very detailed Global Malaria Program’s “Guidelines for the treatment of malaria” (2nd ed. Geneva, World Health Organization, 2010) that discusses medications for all species of Plasmodium and does not have an easy to view take away on the essential life saving commodities within.
Over the past year the Global Malaria Program of WHO has issued guidance for updating malaria in pregnancy interventions, including more frequency IPTp with sulphadoxine-pyrimethamine (SP). The briefing companion document to this new guidance spells out the following life saving benefits if IPTp with appropriate references:
- IPTp-SP prevents the adverse consequences of malaria on maternal and fetal outcomes, such as placental infection, clinical malaria, maternal anaemia, fetal anaemia, low birth weight and neonatal mortality.
- IPTp-SP has recently been shown to be highly cost-effective for both prevention of maternal malaria and reduction of neonatal mortality in areas with moderate or high malaria transmission.
- Despite the spread of SP resistance, IPTp-SP continues to provide significant benefit, resulting in protection against both neonatal mortality (protective efficacy 18%) and low birth weight (21% reduction in LBW) under routine program conditions.
Over the years rarely has IPTp if ever achieved high and sustained coverage. Factors relating to late antenatal care attendance are often mentioned first, but experience has shown that one of the key factors is stock-out of SP. Once SP was no longer a first line treatment drug, it was forgotten – a neglected medicine needed by an often neglected but vulnerable portion of the population. Now is the time to advocate strongly for direct and unconditional listing of SP for IPTp, ITNs and other malaria products among any list of RNMCH life saving commodities.
IPTp Bill Brieger | 20 Nov 2013
In vivo Efficacy of Sulfadoxine-Pyrimethamine for Intermittent Preventive Treatment of Malaria in Pregnancy — Mansa, Zambia
People continue to question the efficacy of Sulfadoxine-Pyrimethamine for intermittent preventive treatment of malaria during pregnancy as a preventive measure. Kathrine R. Tan, Bonnie R. Katalenich, Kimberly E. Mace, Michael Nambozi, Steve M. Taylor, Steven R. Meshnick, Ryan E. Wiegand, Victor Chalwe, Scott J. Filler, Mulakwa Kamuliwo, and Allen S. Craig presented information at the recent American Society of Tropical medicine and Hygiene 62nd Annual meeting that should allay these concerns. Below are the main points from their poster.
 Intermittent preventive treatment of malaria in pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP) decreases adverse effects of malaria during pregnancy SP resistance threatens IPTp–SP strategy. Mutations on the P. falciparum genes for dhfr and dhps are associated with SP drug resistance. Quintuple mutant haplotype (substitutions in N51I, C59R, S108N in dhfr and A437G and K540E in dhps) is a marker for SP treatment failure in non-pregnant patients. Prevalence of molecular markers for SP resistance among pregnant women and how this translates into efficacy of IPTp-SP is unknown.
Intermittent preventive treatment of malaria in pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP) decreases adverse effects of malaria during pregnancy SP resistance threatens IPTp–SP strategy. Mutations on the P. falciparum genes for dhfr and dhps are associated with SP drug resistance. Quintuple mutant haplotype (substitutions in N51I, C59R, S108N in dhfr and A437G and K540E in dhps) is a marker for SP treatment failure in non-pregnant patients. Prevalence of molecular markers for SP resistance among pregnant women and how this translates into efficacy of IPTp-SP is unknown.
 The study objectives were 1) To determine the efficacy of IPTp-SP in clearing peripheral parasitemia in asymptomatic pregnant women , 2) To estimate prevalence of molecular markers for SP resistance among pregnant women in Mansa and 3) To describe the relationship of therapeutic efficacy of IPTp-SP with prevalence of molecular markers for SP resistance.
The study objectives were 1) To determine the efficacy of IPTp-SP in clearing peripheral parasitemia in asymptomatic pregnant women , 2) To estimate prevalence of molecular markers for SP resistance among pregnant women in Mansa and 3) To describe the relationship of therapeutic efficacy of IPTp-SP with prevalence of molecular markers for SP resistance.
 Setting and population focused on Pregnant women attending two antenatal clinics in Mansa, Zambia, an area with high malaria transmission between January 2010 – March 2011 . Inclusion criteria were Pregnant women in their second trimester (by last menstrual period), HIV negative, no prior antimalarials or IPTp-SP in the current pregnancy, and asymptomatic parasitemia. The In vivo therapeutic efficacy study looked for
Setting and population focused on Pregnant women attending two antenatal clinics in Mansa, Zambia, an area with high malaria transmission between January 2010 – March 2011 . Inclusion criteria were Pregnant women in their second trimester (by last menstrual period), HIV negative, no prior antimalarials or IPTp-SP in the current pregnancy, and asymptomatic parasitemia. The In vivo therapeutic efficacy study looked for
- Asymptomatic parasitemia determined by fever history, temperature measurement, and rapid diagnostic test (confirmed with malaria smear)
- Follow up weekly for five weeks to assess for fever, parasitemia by blood smear, and hemoglobin
- Polymerase chain reaction (PCR) of parasites on follow up to determine reinfection or recrudescence
- Main Outcomes observed were –
- Adequate parasitic response — no parasitemia on follow up
- Parasitological failure — recrudescence
- Survival analysis done to describe time to failure and included those with incomplete follow up
 Molecular markers include PCR of Day 0 specimens to detect mutations on genes for dhps and dhfr.
Molecular markers include PCR of Day 0 specimens to detect mutations on genes for dhps and dhfr.
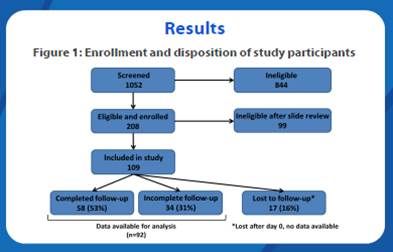
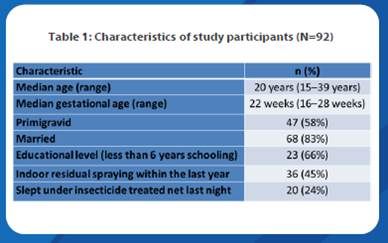
Figure 1 shows Enrollment and disposition of study participants with Molecular Markers on 84. Quintuple mutant was seen in 51 (61%). There was No association between quintuple mutation and in vivo therapeutic efficacy outcome. Triple mutant only was 20 (24%) ; Double mutant only 7 (8%); and Sextuple mutant (quintuple mutation plus mutation at codon 581 of dhps) 2 (2%). Table 1 shows the Characteristics of the study 92 participants.
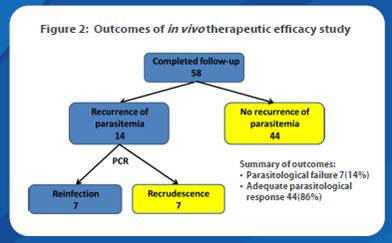
Figure 2 provides Outcomes of in vivo therapeutic efficacy study. A Summary of outcomes found Parasitological failure in 7 (14%) and Adequate parasitological response in 44 (86%). Figure 3 depicts the Kaplan-Meier survival estimates. Time to failure for all study participants (n=92, top panel) was 33.6 days, and did not significantly differ by gravidity (bottom pannel).
The study had some limitations including Small sample size — underpowered. There were No refusals for participation, but high rates for incomplete and loss to follow up — women may have enrolled as a socially desirable response, then later dropped out. Efficacy of IPTp-SP was examined in terms of parasite clearance. Care must be taken in extrapolating these results to effectiveness of IPTp-SP to prevent outcomes such as low birthweight and neonatal mortality.
IPTp-SP in Zambia still has in vivo efficacy and should be continued especially since there are no other drug alternatives for IPTp. Low in vivo failure rate relative to the moderate prevalence of molecular markers in Mansa was observed. There was No association between presence of the quintuple mutant and parasitologic failure, This is the First time the sextuple mutant has been described in Zambia. This study contributes to the paucity of data on in vivo efficacy of IPTp-SP in the setting of intermediate prevalence of SP resistance markers. Zambian IPTp-SP guidelines have been updated to reflect current WHO guidelines stressing IPTp at each ANC visit after quickening.
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Community &IPTp &Malaria in Pregnancy Bill Brieger | 15 Nov 2013
Improving Intermittent Preventive Treatment in Pregnancy and Antenatal Care Coverage
The Malaria Communities Program (MCP), supported by the US President’s Malaria Initiative, has increased local and indigenous capacity to undertake community-based malaria prevention and treatment activities; built local ownership of malaria control for the long term in partnership with communities and National Malaria Control Programs (NMCPs); and extended coverage of PMI and NMCP interventions to reach a larger beneficiary population. Below is a summary of the third in a series of MCP case studies found on the website of MCHIP – the USAID Maternal and Child Health Integrated Project.
The full case study on improving coverage of two doses of intermittent preventive treatment in pregnancy (IPTp) and attendance at antenatal care clinics, the main platform for delivering IPTp can be found at: http://www.mchip.net/node/2082
This IPTp/ANC case study focuses on four MCP partners and their contributions to improving the second dose of intermittent preventive treatment in pregnancy (IPTp2) and ANC coverage: Medical Teams International (MTI) Uganda, Episcopal Relief and Development (ERD) Angola, Caritas Senegal, and the Catholic Medical Mission Board (CMMB) Zambia. MCHIP collected multiple forms of data from each MCP partner using qualitative methods, including individual interviews with key project personnel and review of key documents.
MCHIP then compared data across organizations to better understand the total contributions made by the MCP. Some partners conducted surveys and relevant quantitative data are included in this report. Data are limited by a lack of standardized reporting on this topic. Although MIP interventions comprise more than IPTp and ANC, the three sub-themes emerging from this review are: 1) mobilizing communities to increase ANC and IPTp uptake; 2) using behavior change communication (BCC) to inform women and their families about the importance of ANC and IPTp; and 3) improving access to quality ANC services.
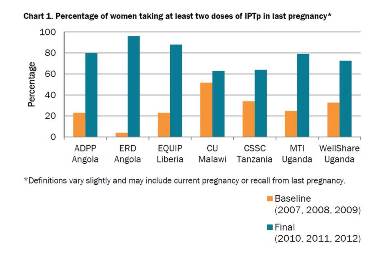 Chart 1 shows results from MCP projects that collected survey data regarding IPTp, and indicates significant improvements in coverage in those project areas. MCP partners built partnerships between communities and health facilities to improve access. As exemplified by strategies such as VHTs accompanying pregnant women to health facilities and assisting midwives in administration of IPTp, when communities and facilities work together the partnership yields not only improved outcomes but also improved attitudes among providers and clients. MTI successfully expanded the Ministry of Health package of Village Health Team services to address malaria in pregnancy in their project area.
Chart 1 shows results from MCP projects that collected survey data regarding IPTp, and indicates significant improvements in coverage in those project areas. MCP partners built partnerships between communities and health facilities to improve access. As exemplified by strategies such as VHTs accompanying pregnant women to health facilities and assisting midwives in administration of IPTp, when communities and facilities work together the partnership yields not only improved outcomes but also improved attitudes among providers and clients. MTI successfully expanded the Ministry of Health package of Village Health Team services to address malaria in pregnancy in their project area.
MCP partners implemented interpersonal communication strategies to increase demand for and use of MIP-related services. MCP partners also encouraged male participation to increase coverage of MIP-related
services.
IPTp &Malaria in Pregnancy Bill Brieger | 09 Nov 2013
Ghana: Progress on IPTp, but not yet sustained high coverage
The 2011 Multiple Indicator Cluster Survey (MICS) from Ghana demonstrates the challenges we have in moving along the pathway toward malaria elimination. People will recall that the Roll Back Malaria indicators were for endemic countries achieve 80% coverage on basic malaria interventions by 2010 and sustain these to achieve Millennium Development goals by 2015 and then move on to pre-elimination of the disease where less than 1/1000 people at risk in a country actually experienced malaria. Now of course, everyone is talking about universal coverage of basic services, not just 80%.
The 2011 Ghana MICS reports on the standard RBM indicator of two doses of intermittent preventive treatment (IPTp) with sulphadoxine-pyrimethamine (SP) during antenatal care (ANC), although Ghana has for some time aimed at three doses. Also current WHO guidance for IPTp recommends IPTp in stable endemic countries at one dose for every antenatal care visit after quickening, which could mean three or four times. So the 2011 MICS shows 83% of recently pregnant women surveyed got one dose of IPTp during ANC while only 65% received two.
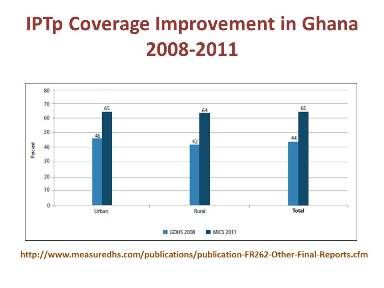 The chart to the right does show progress in IPTp coverage between the 2008 Demographic and Health Survey and the 2011 MICS. a jump from 44% to 65% for the two doses, and progress should be acknowledged, but as pointed out at the recent Pan Africa Malaria Conference in Durban, we must not work around the edges to eliminate malaria, but tackle the higher prevalence countries and areas directly and ensure that malaria is truly eliminated.
The chart to the right does show progress in IPTp coverage between the 2008 Demographic and Health Survey and the 2011 MICS. a jump from 44% to 65% for the two doses, and progress should be acknowledged, but as pointed out at the recent Pan Africa Malaria Conference in Durban, we must not work around the edges to eliminate malaria, but tackle the higher prevalence countries and areas directly and ensure that malaria is truly eliminated.
Why are coverage figures low – and this is not just a problem in Ghana? At least 96% of pregnant wom en in Ghana attend ANC with a skilled provider: 95% make two ANC visits, 89% make three and 86% are reported to make four. What we may be seeing are missed opportunities.
en in Ghana attend ANC with a skilled provider: 95% make two ANC visits, 89% make three and 86% are reported to make four. What we may be seeing are missed opportunities.
Are gaps due to health worker errors, SP stock-outs or client refusals? This needs to be investigated and rectified.
Ideally pregnant women should also get an insecticide treated net on their first ANC visit regardless of distribution through mass campaigns. Unfortunately the MICS 2011 shows that only 32% of pregnant women overall had slept under a treated net the previous night, and even in households with nets, only 58% had slept under them. Clearly malaria in pregnancy control and scale-up needs higher priority in Ghana as well as the rest of Africa.
IPTp &ITNs &Treatment Bill Brieger | 24 Oct 2013
Awareness, Accessibility and Use of Malaria Control Interventions Among At-Risk Groups In Lagos State, Nigeria
AK Adeneye, PO Ossai and TS Awolola are sharing with us a pilot study they conducted based from the Nigerian Institute of Medical Research in Yaba, Lagos.
With two years to the MDGs deadline, there is limited evidence of decreases in malaria-related mortality and morbidity in Nigeria. We therefore wanted to evaluate the awareness, accessibility and use of malaria control interventions among at-risk groups in Lagos State, Nigeria.

Lagos State Ministry of Health http://www.lsmoh.com/news/lagos-treats-300-for-malaria#.UmlR9RAQ5aw
In planning for a broader assessment we conducted a descriptive, cross-sectional pilot study of 80 consenting pregnant women and mothers of children below five years of age. It was carried out using a household survey questionnaire and observation in Ikotun and Ketu communities of Lagos State
All respondents identified mosquito as the malaria vector. Respondents’ preferred drugs for malaria treatment were as follows: sulphadoxine-pyrimethamine (31.3%); ACTs (20.2%); artemisinin monotherapies (15.0%); chloroquine (13.8); and analgesics (12.5%). Only (30.0%) had used ACTs, and 55.0% of these had practiced self-medication.
Nearly all knew of and had LLINs. From room observation, only 53.8% (31.5% mothers of under-five vs. 11.3% pregnant women) actually hung the LLINs. Reasons for non-use of LLIN included: “prefer house spraying” (28.8%) and “causes heat” (7.5%).
LLIN use was positively associated with education (p<0.05), ranging from 50.0% (no education) to 77.8% (post-secondary). Only 41.8% got their LLINs through house-to-house mass distribution. Women averaged washing their nets 3 times within an average of 21.7 months of use.
LLIN washing practices showed that 30.5% used toilet soaps compared to detergents and hard soaps (66.7%). Unfortunately, 19.4% sun dried their nets.
While 52.6% of the pregnant women were aware of IPTp, 42.1% actually had received at least one dose.
Results of this pilot showed high awareness but low and poor use of malaria control interventions in populations studied. A wider survey in the near future will inform public health education on the different malaria control interventions that need to be intensified among the women so they can benefit from improved pregnancy and child health outcomes. This is important if the malaria-related MDG targets are to be realized in Lagos and in Nigeria in general.
Community &IPTp &Malaria in Pregnancy Bill Brieger | 09 Oct 2013
Jhpiego at MIM2013 – Use of Community Health Workers to Improve Pregnancy Outcomes in Kenya
Augustine Ngindu, Sanyu Kigondu, Rose Mulindi, Christine Ayuyo, Muthoni Magu-Kariuki, Isaac Malonza, Julius Kimiteiand Elizabeth Washikaof Jhpiejo, the Ministry of Health (Kenya) and the Maisha/USAID Project reported on using Community Health Workers to identify and refer pregnant women to access intermittent preventive treatment (IPTp) in Kenya

Community Health Worker Training
Malaria in pregnancy is associated with anemia, low birth weight, miscarriages and death. Despite availability of effective MIP interventions intermittent preventive treatment using Sulfadoxine Pyrimethamine (IPTp-SP) and insecticide treated nets (ITNs), coverage rates in Kenya have remained low; IPTp2 uptake- 25% and ITN coverage- 41%.
To increase coverage rates Kenya has adapted a community strategy approach sensitizing pregnant women to start antenatal care (ANC) early to receive comprehensive care throughout pregnancy. This includes access to an ITN at first ANC visit and IPTp uptake beginning in the second trimester to increase coverage rates.
Trained community health workers (CHWs) registered pregnant women in their Community units for follow up monthly. CHWs conducted monthly follow up of all registered pregnant women to identify those not attending ANC and referred them for ANC services as well as counseled those not using ITNs.
CHWs received supportive supervision from district managers and MCHIP staff to assess performance skills on quality of data and mentorship on MIP interventions. Data collected was analyzed for pregnant women registered, accessing IPTp and referred for ANC services.
3,212 pregnant women were registered and 1,541 (48%) of the registered pregnant women were referred for ANC services because they were either late in starting ANC attendance or IPTp after 1st trimester or defaulters of scheduled visits. Among the registered pregnant women 81% had taken one or more IPTp doses.
Use of CHWs in identification of pregnant women not accessing IPTp and referral of 48% of them has shown an effective methodology of identifying defaulters in IPTp uptake among pregnant women. Scaling up of this community-based approach would ensure early ANC attendance and access to the available effective MIP interventions including IPTp.