ITNs &Partnership &Private Sector &Vector Control Bill Brieger | 05 Apr 2017
The Business Case for Malaria Prevention: Employer Perceptions of Workplace LLIN Distribution in Southern Ghana
Kate Klein as part of her Master of Science in Public Health program in Social and Behavioral Interventions at the Johns Hopkins Bloomberg School of Public Health undertook a study of the potential for private sector involvement in malaria prevention in Ghana. She shares a summary of her work here. During her practicum in Ghana she was hosted by JHU’s Center for Communications Programs and its USAID supported VectorWorks Program. Her practicum she was also supported by the JHU Center for Global Health, and she presented her findings in a poster at the CGH’s Global Health Day on 30th March 2017. Her essay readers/advisers were Dr. Elli Leontsini (Department of International Health) and Kathryn Bertram (Center for Communication Programs).
Malaria is endemic in all parts of Ghana and significantly burdens families, communities, and economies. Malaria remains a leading cause of morbidity and mortality in Ghana; it accounts for eight percent of deaths in the country (The Global Fund, Ghana). It was also responsible for about 38% of outpatient visits, 27.3% of admissions in health facilities, and 48.5% of under-five deaths in 2015 (Nonvignon et al., 2016). In Ghana, the estimated cost of malaria to businesses in 2014 alone was estimated to be US$6.58 million, and 90% of these were direct costs (Nonvignon et al., 2016). Malaria leads to reduced productivity due to increased worker absenteeism and increased health care spending, which negatively impact business returns and tax revenue to the state (Nabyonga et al., 2011).
Although long-lasting insecticidal treated nets (LLINs) are a well-documented strategy to prevent disease in developing countries, most governments, including Ghana, lack the resources needed to comprehensively control malaria. The Global Fund (GF), USAID/President’s Malaria Initiative (PMI Ghana), and the United Kingdom Department for International Development (DfID Ghana) are the main donors for the national malaria control strategy and have worked primarily with the public sector (World Malaria Report, 2015). As government funding remains unable to close the funding gap for malaria, there is an increasing need to revitalize the private sector in sales and distribution of this life-saving technology.
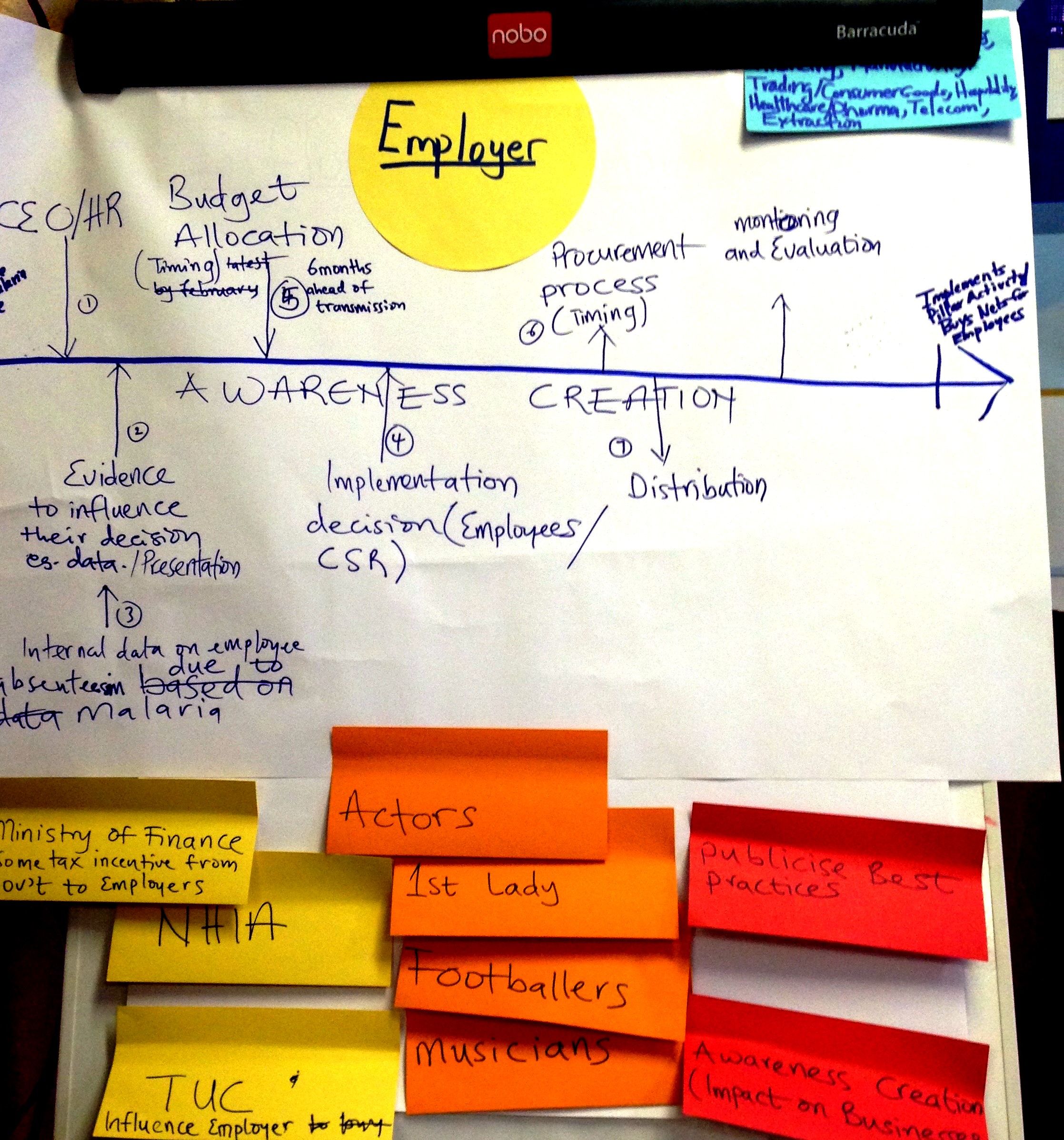
A “Journey mapping” exercise to consider the process of employers buying and distributing nets to employees, created during a PSMP advocacy workshop in December 2016
Ghana is looking to the private sector to encourage a departure from previous dependence on donor-funded free bed nets. The Private Sector Malaria Prevention (PSMP at JHU) project is being implemented in Southern Ghana to increase commercial sector distribution of LLINs. Three case studies served as a situation analysis and exemplified the potential for the PSMP: a rubber producing company, a mining company and a brewery.
All three had experience in malaria control and prevention but only one had specific experience with LLINs (which dovetailed well with its own corporate strengths in logistics management as exemplified by other bottling companies in Africa). Another supported the idea of adding LLINs to its existing indoor residual spraying and community health education efforts, but needed to consider how to develop the flexibility to engage in multiple malaria interventions.
The third had had the right climate and leadership to be able to partner with PSMP, but recently underwent a takeover by a large multinational brewing company and the resulting period of transition could potentially complicate their participation in LLIN distribution efforts from a budgetary standpoint. Generally these companies had the understanding of the potential benefits to the company of situating malaria control within their structure, and thus being early candidates for adoption of the PSMP.
 While the three case study companies recognized the business case for malaria, this was not a unanimous opinion among other five companies interviewed. Their concerns ranged from a preference toward treatment interventions to concerns expressed by employees about the difficulty of achieving high levels of net usage due to an array of complaints surrounding sleeping under LLINs. Some of these others had financial constraints.
While the three case study companies recognized the business case for malaria, this was not a unanimous opinion among other five companies interviewed. Their concerns ranged from a preference toward treatment interventions to concerns expressed by employees about the difficulty of achieving high levels of net usage due to an array of complaints surrounding sleeping under LLINs. Some of these others had financial constraints.
Through case studies and interviews PSMP was able to identify various challenges moving forward as well as areas where further clarity must be sought. PSMP learned that several companies are pouring their resources into strong treatment and case management programs, and one challenge will be determining how to push for preventative action, such as LLIN distribution, when treatment mechanisms are so established and bias exists.
For those companies who are making tremendous strides in malaria prevention, bringing recognition to these successes through advocacy will be necessary for encouraging future participation and convincing other similar employers of the benefits of starting their own LLIN distribution programs. Finally, PSMP needs to prioritize clarifying viewpoints on LLIN efficacy and use, with a focus on understanding why employers may hold unfavorable views and what it would take to overturn them.
In the future it will be necessary to move beyond the occupational considerations specific to mining and agro-industrial operations and consider how the work has changed the environment into a malaria habitat and the non-traditional work hours that may create more significant Anopheles mosquito exposures. PSMP should gather specific information on lifestyle, housing, and work environments during future visits with employers so that companies that have the most to gain through LLIN distribution are identified and targeted.
Asia &ITNs &Treatment Bill Brieger | 29 Mar 2017
Myanmar – update on malaria indicators
 Myanmar is one of the countries at the epicenter of the developing resistance of malaria parasites to artemisinin based drugs. This means there is a strong need for prompt, appropriate and thorough diagnosis and treatment of febrile illnesses and malaria as well as the regular use of effective malaria preventive technologies. The 2015-16 Demographic and Health Survey for the country is thus a timely source of information to improve malaria interventions. Highlights from the DHS follow.
Myanmar is one of the countries at the epicenter of the developing resistance of malaria parasites to artemisinin based drugs. This means there is a strong need for prompt, appropriate and thorough diagnosis and treatment of febrile illnesses and malaria as well as the regular use of effective malaria preventive technologies. The 2015-16 Demographic and Health Survey for the country is thus a timely source of information to improve malaria interventions. Highlights from the DHS follow.
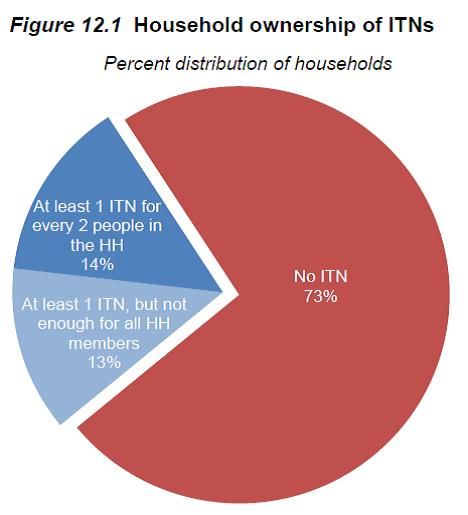
The first major concern is both lack of insecticide treated nets as well as low use of those available as the pie chart from the DHS makes clear. Ironically 97% of households have some kind of net, but 73% do not have an insecticide treated one. Although the Global Fund has supported distribution of 4.3 million ITNs in the country, there are over 56 million people living there. The US President’s Malaria Initiative has procured nearly 900,000 ITNs for the country. 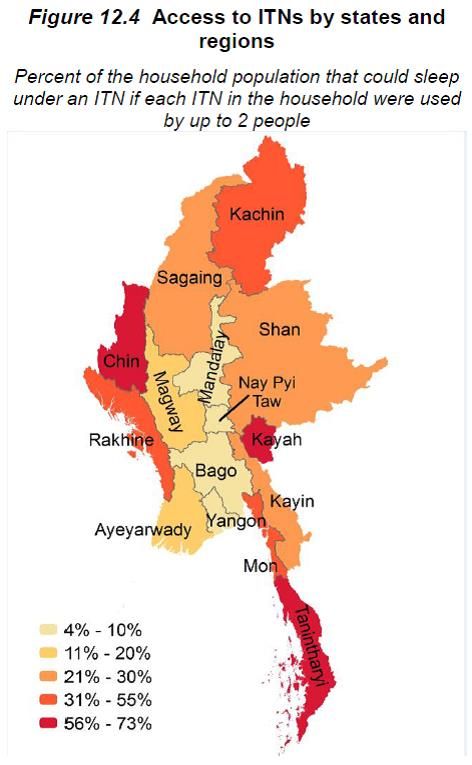 Although low across all economic strata, the lowest wealth quintile have the highest ITN possession (35%).
Although low across all economic strata, the lowest wealth quintile have the highest ITN possession (35%).
The 2013 concept note submitted by Myanmar to Global Fund under the new funding mechanism identifies many of the challenges: “Factors that may cause inequity to services for treatment and prevention: There are several population groups, which are poorly served by the health system and malaria services such as those living in remote border areas, migrant populations, forest workers and miners where malaria transmission is intense. Many of them are internal and external migrants who usually have limited access to malaria prevention and control. Major factors include distance from health facilities and poor awareness of malaria and its prevention.”
 Key strategies in the Global Fund Concept Note do address quality malaria diagnostics and appropriate treatment. Unfortunately DHS results do not yet show the impact of improved diagnosis and treatment. “Overall, 16% of children under age 5 had a fever in the 2 weeks before the survey. Advice or treatment was sought for 65% of these children with recent fever, and 3% had blood taken from a finger or heel, presumably for diagnostic testing.” A variety of public and private sources were used to seek fever treatment, but “Only
Key strategies in the Global Fund Concept Note do address quality malaria diagnostics and appropriate treatment. Unfortunately DHS results do not yet show the impact of improved diagnosis and treatment. “Overall, 16% of children under age 5 had a fever in the 2 weeks before the survey. Advice or treatment was sought for 65% of these children with recent fever, and 3% had blood taken from a finger or heel, presumably for diagnostic testing.” A variety of public and private sources were used to seek fever treatment, but “Only  1% of children received antimalarial drugs for treatment of fever in the 2 weeks preceding the survey.”
1% of children received antimalarial drugs for treatment of fever in the 2 weeks preceding the survey.”
In addition to formal donors, there are coalitions and consortia who provide encouragement, technical assistance, advocacy and capacity building for eliminating malaria in the Asia-Pacific region. While the country needs to take stronger leadership in malaria elimination, all groups need to come together and strengthen the malaria interventions in Myanmar as these have implications for eliminating the disease in the region as a whole.
IPTp &ITNs &Malaria in Pregnancy Bill Brieger | 27 Jan 2017
Malaria in Pregnancy Progress in Nigeria – the 2015 Malaria Indicator Survey
With an eye toward the future Nigeria’s National Malaria Control Program also refers to itself as the National Malaria Elimination Program (NMEP). Given that Nigeria has the highest burden of malaria in Africa, along with around one-quarter of sub-Saharan Africa’s population, the elimination goal will take a lot of work.
 Recently the 2015 Malaria Information Survey (MIS) for Nigeria was released and gives a perspective on how far we have some and how far we need to go. We will focus on malaria in pregnancy (MIP) interventions today.
Recently the 2015 Malaria Information Survey (MIS) for Nigeria was released and gives a perspective on how far we have some and how far we need to go. We will focus on malaria in pregnancy (MIP) interventions today.
Intermittent Preventive Treatment for pregnant women (IPTp) using sulfadoxine-pyrimethamine (SP) remains the key MIP intervention due to the high and stable malaria transmission that still persists. There is always a challenge in delivering health interventions that require multiple contacts, and IPTp is not exception. The difficulty in achieving two doses when that was policy was clear. Now that WHO recommends monthly dosing from the second trimester forward (giving the possibility of 3, 4 or more doses), the service delivery challenge is heightened.
We can see in the attached graph from the MIS report that while there is progress, it remains well below the 2010 Roll back malaria Target of 80%. Part of the problem resides in the fact that the 2013 DHS showed only 61% of pregnant women attended even one antenatal care visit while 51% attended four or more.
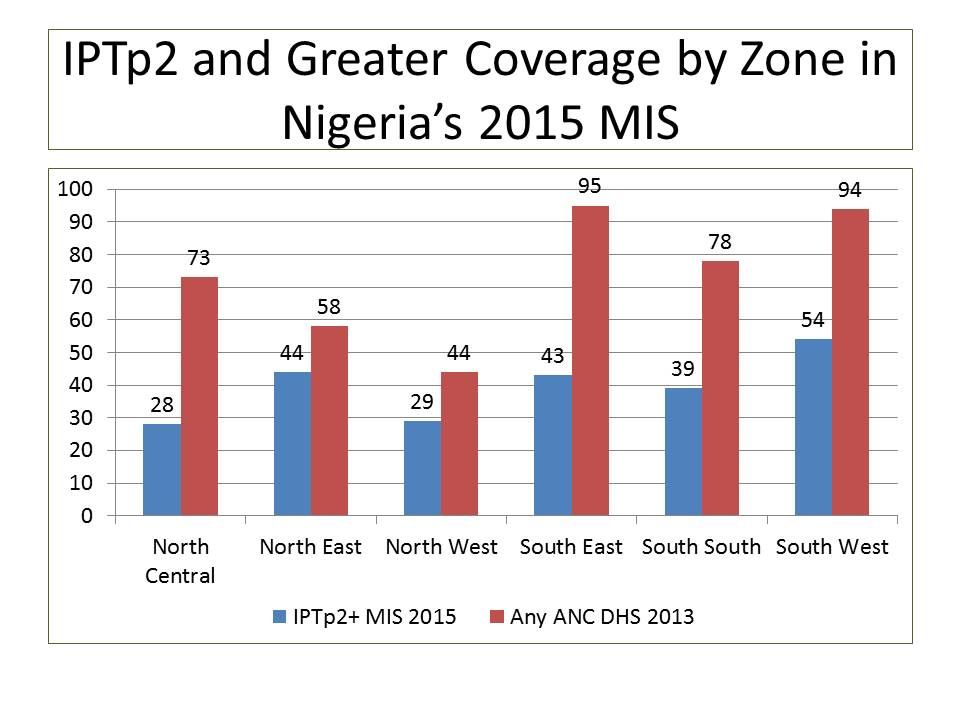 The second lesson of the graph is missed opportunities. There is a gap between IPTp1 coverage of 37% and at least one ANC visit of 61%. Granted, 18% of women made their first visit in the first trimester when SP is not given, but not all of those stopped ANC then. The next evidence of missed opportunities is the gap between IPTp1 and IPTp2, almost a quarter of women who started IPTp did not get a second dose. We cannot say that the women’s own attendance gaps account for all the missed opportunities; some are likely due to health systems weaknesses such as stock-outs and health staff attention.
The second lesson of the graph is missed opportunities. There is a gap between IPTp1 coverage of 37% and at least one ANC visit of 61%. Granted, 18% of women made their first visit in the first trimester when SP is not given, but not all of those stopped ANC then. The next evidence of missed opportunities is the gap between IPTp1 and IPTp2, almost a quarter of women who started IPTp did not get a second dose. We cannot say that the women’s own attendance gaps account for all the missed opportunities; some are likely due to health systems weaknesses such as stock-outs and health staff attention.
Key demographic factors are linked to receiving two or more IPTp doses. Only 30% or rural women received two or more compared to 50% of urban. There was a steady progression from 21% of the poorest women to 55% of those in the highest wealth quintile. A second chart also shows variation by section of the country. These access gaps are why we have advocated for supplementary distribution of IPTp through trained community health workers.
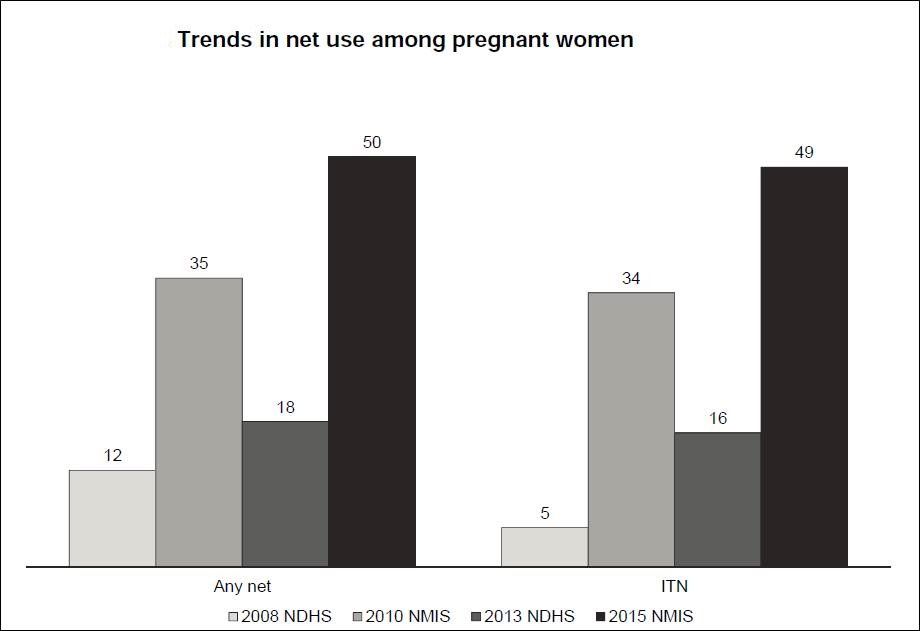 Use of insecticide treated bed nets by pregnant women shows a similar increase over time. The dip in 2013 probably related to fact that mass campaigns had occurred between 2009 and 2011 and thus by the time of the survey some nets had become damaged and abandoned. A major challenge in achieving net coverage is NOT relying on periodic distribution campaigns only, but ensuring regular and reliable supplies during routine services such as antenatal care. This again is a health systems problem that must be solved.
Use of insecticide treated bed nets by pregnant women shows a similar increase over time. The dip in 2013 probably related to fact that mass campaigns had occurred between 2009 and 2011 and thus by the time of the survey some nets had become damaged and abandoned. A major challenge in achieving net coverage is NOT relying on periodic distribution campaigns only, but ensuring regular and reliable supplies during routine services such as antenatal care. This again is a health systems problem that must be solved.
Net access is not only a health systems issue, bit may be factor of internal household dynamics. Even when the household possesses nets, only 63% of pregnant women therein slept under one the night before the survey. Community education needs strengthening – more than just telling people what to do but involving them is solving the problems of net use.
So as mentioned earlier, progress is being made, but more effort is needed. We are especially concerned because of the precariousness of global financial support for disease control. Nigeria needs to strategize how it can meet its own needs in protecting pregnant women and their unborn children from malaria, disability and death.
IPTp &ITNs &Malaria in Pregnancy Bill Brieger | 08 Nov 2016
Malaria Excerpts from WHO’s New Antenatal Care Recommendations
 Many years ago WHO formulated guidance for encouraging 4 Focused Antenatal Care (FANC) that addressed the reality that 1) ANC attendance schedules were not standardized, 2) service package elements were not clearly laid out, and 3) women found it difficult to attend ANC as many times as some countries recommended. The New York Times reported that WHO now recommends 8 ANC visits in large part because greater action is needed in light of the fact that …
Many years ago WHO formulated guidance for encouraging 4 Focused Antenatal Care (FANC) that addressed the reality that 1) ANC attendance schedules were not standardized, 2) service package elements were not clearly laid out, and 3) women found it difficult to attend ANC as many times as some countries recommended. The New York Times reported that WHO now recommends 8 ANC visits in large part because greater action is needed in light of the fact that …
“About 300,000 women die in pregnancy or childbirth each year, the agency said, and more than six million babies die in the womb, during birth or within their first month. Many of those deaths can by prevented through simple interventions.”
The new recommendations number 49 and strongly consider the roles of all health workers from auxiliaries to doctors – stressing task shifting to ensure that women have access to life saving services. Below are extracted some of the aspects that relate to malaria.
- In areas with endemic infections that may cause anaemia through blood loss, increased red cell destruction or decreased red cell production, such as malaria and hookworm, measures to prevent, diagnose and treat these infections should be implemented.
- Malaria prevention: intermittent preventive treatment in pregnancy (IPTp): In malaria-endemic areas in Africa, intermittent preventive treatment with sulfadoxine-pyrimethamine (IPTp-SP) is recommended for all pregnant women. Dosing should start in the second trimester, and doses should be given at least one month apart, with the objective of ensuring that at least three doses are received.
The above recommendation has been, “Integrated from the WHO publication Guidelines for the treatment of malaria (2015), which also states: ‘WHO recommends that, in areas of moderate-to-high malaria transmission of Africa, IPTp-SP be given to all pregnant women at each scheduled ANC visit, starting as early as possible in the second trimester, provided that the doses of SP are given at least 1 month apart. WHO recommends a package of
interventions for preventing malaria during pregnancy, which includes promotion and use of insecticide-treated nets, as well as IPTp-SP’. To ensure that pregnant women in endemic areas start IPTp-SP as early as possible in the second trimester, policy-makers should ensure health system contact with women at 13 weeks of gestation.”
 Task shifting components of antenatal care delivery: Task shifting the distribution of recommended nutritional supplements and intermittent preventive treatment in pregnancy (IPTp) for malaria prevention to a broad range of cadres, including auxiliary
Task shifting components of antenatal care delivery: Task shifting the distribution of recommended nutritional supplements and intermittent preventive treatment in pregnancy (IPTp) for malaria prevention to a broad range of cadres, including auxiliary
nurses, nurses, midwives and doctors is recommended.

Readers should download the full set of recommendations for more details on the above. We do offer a challenge. Since the 4-visit FANC processes, that was adopted in part because of the difficulty in getting pregnant women to attend ANC many times, is still not fully achieved (see graph), we must now strengthen community involvement, mobilization and education to double that target to 8 visits. Efforts must focus on women, men, elders and even youth. Health workers also need education and motivation to adopt a client-friendly attitude to make this new schedule work.
Integrated Vector Management &ITNs &Ivermectin &NTDs Bill Brieger | 11 Oct 2016
Malaria, Lymphatic Filariasis and Insecticide-treated Nets

?
Throughout Africa one of the main vectors that carry Lymphatic Filariasis (LF) is the Anopheles mosquito, which also carries the malaria parasite. The Carter Center has been promoting use of insecticide treated nets (ITNs) for many years as part of its LF control efforts, but others may not have gotten the message.
The global community is targeting LF for elimination in 2020. The primary strategy is mass drug administration annually with ivermectin and albendazole. The plan is that up to seven annual rounds of drug distribution in endemic communities where 90% of population coverage is achieved is necessary to stop LF transmission. The Carter Center explains that distribution of long-lasting insecticidal bed nets (LLINs) protects pregnant women and children who cannot take drug treatment.
The LF strategy often builds on and integrates with onchocerciasis control efforts where these diseases overlap. The community directed treatment with ivermectin (CDTI) model pioneered by the African Program for Onchocerciasis Control (APOC), wherein communities or villages plan together the distribution process including selecting their own community directed distributors (CDDs). This model has also been used to distribute ITNs.
 A second component of the LF strategy is morbidity management which focuses on enhanced personal hygiene or cleaning of the parts of the body that experience lymphedema. Another aspect uses surgery to address some of the worst effects, hydrocele. While this component does not ‘control’ LF, it is a necessary effort to reduce suffering and the negative stigma from the disease.
A second component of the LF strategy is morbidity management which focuses on enhanced personal hygiene or cleaning of the parts of the body that experience lymphedema. Another aspect uses surgery to address some of the worst effects, hydrocele. While this component does not ‘control’ LF, it is a necessary effort to reduce suffering and the negative stigma from the disease.
To judge whether transmission has stopped and elimination has been achieved Transmission Assessment Surveys (TAS) are conducted with rapid diagnostic tests on young children after at least 5 years of MDA in a community. Specifically WHO recommends an implementation unit must have completed five effective rounds of annual MDA defined as achieving rates of drug coverage exceeding 65% in the total population.
For example the Carter Center in Support of the Nigerian Federal Ministry of Health worked in Plateau and Nasarawa States through community health education, delivery of long lasting insecticide-treated nets (LLINs) and 33 million drug treatments for lymphatic filariasis and river blindness between 2000 and 2011. “In 2012, it was confirmed (through TAS) that lymphatic filariasis transmission had stopped. Post-treatment surveillance is currently underway to assure that the parasite is not reintroduced into the area.”
Another component of the assessment process is yet to be fully realized. That is the testing of mosquitoes for the presence of microfilariae. This indirectly implies an important role in preventing human-vector contact as would be achieved through the use of ITNs as well as indoor residual spray (IRS).
Vector control can benefit more than one disease. Integrated vector management is seen as a key tool to prevent reintroduction of LF in areas where anopheles mosquitoes carry the disease and where ITN campaigns are successful.
Ultimately the key to benefiting from the disease control synergies provided by insecticide-treated nets is an understanding what if any effect nets have on transmission. This poses a challenge in terms of separating it from the effect of MDAs as well as the fact that MDAs are time-limited. As MDAs are still underway in many places it is incumbent on program managers to monitor and evaluate the impact of all activities, treatment and vector control, over the next decade to determine the success of eliminating LF and hopefully malaria, too.
IPTp &ITNs &Morbidity &Treatment Bill Brieger | 22 Jun 2016
Tanzania – Malaria Indicators Low, Still Need Work
Success in the war against malaria is not guaranteed. Two articles to that effect have appeared The Citizen of Dar es Salaam following presentation of findings from the most recent (2015-16) Tanzania Demographic and Health Survey (DHS)/Malaria Indicator Survey (MIS).
 On Tuesday (21 June 2016) the news story noted the increase in malaria prevalence among children below the age of 5 years, which was attributed to “the decline in the use of mosquito nets and low distribution of nets to households.” Then in a Wednesday (22 June 2016) Editorial, the paper noted that this “backtracking” is a “worrisome situation, for malaria is a problem that puts such a heavy burden on the government and the country’s economy.”
On Tuesday (21 June 2016) the news story noted the increase in malaria prevalence among children below the age of 5 years, which was attributed to “the decline in the use of mosquito nets and low distribution of nets to households.” Then in a Wednesday (22 June 2016) Editorial, the paper noted that this “backtracking” is a “worrisome situation, for malaria is a problem that puts such a heavy burden on the government and the country’s economy.”
 A look at the preliminary DHS does confirm the concerns about insecticide treated nets (ITNs). After nearly 10 years of progress, reported ITN availability in households declined. This was reflected in a drop in reported use by children below 5 years of age as well as pregnant women. It should be noted that targets set in 2000 in the Roll Back Malaria Abuja Declaration had been 80% by the year 2010, and those had almost been achieved in 2012, but the fall to around 50% in 2015-16 is discouraging.
A look at the preliminary DHS does confirm the concerns about insecticide treated nets (ITNs). After nearly 10 years of progress, reported ITN availability in households declined. This was reflected in a drop in reported use by children below 5 years of age as well as pregnant women. It should be noted that targets set in 2000 in the Roll Back Malaria Abuja Declaration had been 80% by the year 2010, and those had almost been achieved in 2012, but the fall to around 50% in 2015-16 is discouraging.
Another preventive measure has also faced difficulty. Pregnant women should receive doses of Sulfadoxine-pyrimethamine (SP) as part intermittent preventive treatment (IPT) during antenatal care (ANC). Until 2012 the recommendation was two contacts, but the World Health Organization has raised this to three or more depending on the number of times a woman attends ANC. So far IPT has not reached 40% or half of the Abuja target.
 This low IPT coverage is ironic since most women attend ANC at least once in Tanzania. At present only 68% of women who had been pregnant received the first dose of IPT even though 98% registered for ANC. Granted that some may have registered in their first trimester when they would not yet be eligible for IPT, but the gap is quite large and signals missed opportunities, which are often caused by stock-outs. Even though the proportion of women attending up to ANC visits could be better, these attendances should produce better delivery of the 3rd IPT dose.
This low IPT coverage is ironic since most women attend ANC at least once in Tanzania. At present only 68% of women who had been pregnant received the first dose of IPT even though 98% registered for ANC. Granted that some may have registered in their first trimester when they would not yet be eligible for IPT, but the gap is quite large and signals missed opportunities, which are often caused by stock-outs. Even though the proportion of women attending up to ANC visits could be better, these attendances should produce better delivery of the 3rd IPT dose.
 Malaria can also be controlled through prompt and appropriate treatment. While testing and treatment of children with appropriate artemisinin-based combination therapy (ACT) has increased, this are is still problematic. In particular, while WHO recommends that all cases of fever should be tested, less than a third received a test (rapid diagnostic test – RDT or microscopy). Testing helps distinguish malaria from other fevers, and ACTs should not be given unless malaria is confirmed. We can see that more ACTs are provided than the number who were tested, so treatment based solely on signs and symptoms is still the norm. Again there is need to explore the availability of both RDTs and ACTs as factors that have made these targets difficult to achieve.
Malaria can also be controlled through prompt and appropriate treatment. While testing and treatment of children with appropriate artemisinin-based combination therapy (ACT) has increased, this are is still problematic. In particular, while WHO recommends that all cases of fever should be tested, less than a third received a test (rapid diagnostic test – RDT or microscopy). Testing helps distinguish malaria from other fevers, and ACTs should not be given unless malaria is confirmed. We can see that more ACTs are provided than the number who were tested, so treatment based solely on signs and symptoms is still the norm. Again there is need to explore the availability of both RDTs and ACTs as factors that have made these targets difficult to achieve.
Tanzania continues to receive support from the Global Fund and the US President’s Malaria Initiative, among other partners. It is incumbent on all partners, global and national, to use these results as a wake up call to to plan for better delivery of malaria services and thus a reduction of both the economic and health burden of malaria in Tanzania.
IPTp &ITNs &Malaria in Pregnancy Bill Brieger | 21 Jun 2016
Kenya – the long road to controlling malaria in pregnancy
Augustine Ngindu, the Technical Advisor for Malaria in Kenya’s Maternal and Child Survival Program (USAID, Jhpiego) shares with us the steps and processes in building a national response to controlling malaria in pregnancy (MIP) in Kenya.
Recently Stephanie Dellicour and colleagues wrote about the challenges in the delivery of interventions to prevent malaria in pregnancy in Kenya in Malaria Journal. They examined MIP services in Nyanza Province of western Kenya between February and May 2010. At that time they found that, “… delivery of IPTp (intermittent preventive treatment in pregnancy) and ITNs (insecticide treated nets) through ANC (antenatal care) was ineffective and more so for higher-level facilities. This illustrates missed opportunities and provider level bottlenecks to the scale up and use of interventions to control malaria in pregnancy delivered through ANC.”
 Since that time the National Malaria Control Program (NMCP) has made efforts to address these problems by building on the national malaria strategy (NMS) 2009-2017 that recommend provision of IPTp only in high malaria transmission areas based on strong epidemiological evidence. In 2010 NMCP revised the national guidelines on diagnosis, treatment and prevention of malaria in line with the NMS 2009-2017. Then in 2011 NMCP in collaboration with Jhpiego developed simplified MIP guidelines on provision of IPTp in line with the national guidelines (each pregnant woman to receive at least 2 IPTp doses starting from 16 weeks of pregnancy at 4 weeks interval). Also in 2011 Maternal and Child health care workers in all 14 high malaria transmission areas were trained on provision of MIP using the simplified guidelines.
Since that time the National Malaria Control Program (NMCP) has made efforts to address these problems by building on the national malaria strategy (NMS) 2009-2017 that recommend provision of IPTp only in high malaria transmission areas based on strong epidemiological evidence. In 2010 NMCP revised the national guidelines on diagnosis, treatment and prevention of malaria in line with the NMS 2009-2017. Then in 2011 NMCP in collaboration with Jhpiego developed simplified MIP guidelines on provision of IPTp in line with the national guidelines (each pregnant woman to receive at least 2 IPTp doses starting from 16 weeks of pregnancy at 4 weeks interval). Also in 2011 Maternal and Child health care workers in all 14 high malaria transmission areas were trained on provision of MIP using the simplified guidelines.
 In 2012 health facility in-charges in the same high transmission areas were trained on MIP quality performance improvement. Then in 2013 promotion of early start of IPTp in the second trimester through sensitization of pregnant women was started in two out of the 14 malaria endemic counties. This resulted in increased IPTp2 coverage from 25% as reported in the kenya Malaria Indicator Survey) (KMIS 2010) to 63% (US-CDC survey 2013).
In 2012 health facility in-charges in the same high transmission areas were trained on MIP quality performance improvement. Then in 2013 promotion of early start of IPTp in the second trimester through sensitization of pregnant women was started in two out of the 14 malaria endemic counties. This resulted in increased IPTp2 coverage from 25% as reported in the kenya Malaria Indicator Survey) (KMIS 2010) to 63% (US-CDC survey 2013).
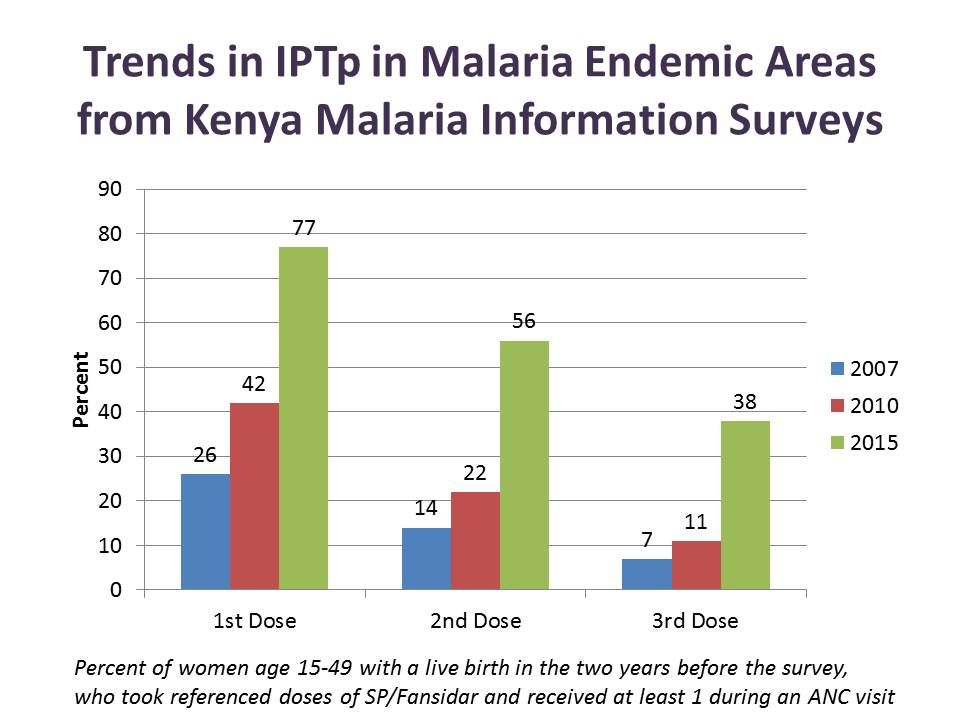
From 2014 to date the practice of sensitizing pregnant women using community health workers/volunteers has been replicated in other counties. IPTp2 coverage has increased from known 25% (KMIS 2010) to 56% (KMIS 2015) in the malaria endemic counties. Likewise use of ITNs by pregnant women increased from 50% in 2010 to 79% in 2015.
Although IPTp coverage is still below national target, the lost opportunities are being addressed. Kenya is still confronting multiple challenges including SP stock-out and devolution of health services to county governments but is set on making progress and saving mothers’ lives.
ITNs &Mosquitoes &Private Sector Bill Brieger | 03 Jun 2016
Manufacturing Mosquito Nets ‘At Home’
The technology of insecticide treated nets (ITNs) to prevent malaria has been around for over three decades. ITNs have evolved from a process of semi-annual soaking and impregnating nets with a safe insecticide at the household or community level to long lasting insecticide-treated nets (LLINs) where the insecticide is integrated into the nets during the manufacturing process. The challenge has always been guaranteeing enough currently treated nets to cover the population and impede malaria transmission.
 Recently Rwanda announced its intentions to establish LLIN manufacturing in-country. The Ministry of Trade and Industry has begun screening of bidders. The government’s main rationale for this move is projected the need for a large and continuous supply of LLINs in the country through 2020, “making it a prudent to set up a production plant in the country.” When this information was shared with our malaria/tropical health update mailing list a number of readers expressed interest and hope that their own governments would follow suit. This post provides some background for readers to consider.
Recently Rwanda announced its intentions to establish LLIN manufacturing in-country. The Ministry of Trade and Industry has begun screening of bidders. The government’s main rationale for this move is projected the need for a large and continuous supply of LLINs in the country through 2020, “making it a prudent to set up a production plant in the country.” When this information was shared with our malaria/tropical health update mailing list a number of readers expressed interest and hope that their own governments would follow suit. This post provides some background for readers to consider.
The idea of locally made mosquito nets is not new. MacCormack and Snow documented that, “95% of people were already sleeping under locally-made  nets,” in The Gambia in the 1980s. Likewise in Burkina Faso it was common to find nets made from imported materials or local cotton that were sewn by local tailors.
nets,” in The Gambia in the 1980s. Likewise in Burkina Faso it was common to find nets made from imported materials or local cotton that were sewn by local tailors.
The idea of drawing on the combination of local or regional textile and chemical industries to produce an ITN kit containing both net and approved insecticide for home/community soaking was tested in several countries by the USAID sponsored NetMark project between 1999–2009. Although the project made ITNs available at reduced prices and resulted in gains in awareness, ownership, and use of nets, “none of the countries reached the ambitious Abuja targets.”
 Even at reduced prices the ITNs made available through this commercial sector approach were still more expensive than most families could afford. In addition partway through the project the emphasis shifted from local products to imported LLiNs leaving a leaving a very bitter taste, particularly in Nigeria with its large industrial sector, in mouths of the textile and chemical partners who during malaria partners meetings at the time expressed a sense of betrayal.
Even at reduced prices the ITNs made available through this commercial sector approach were still more expensive than most families could afford. In addition partway through the project the emphasis shifted from local products to imported LLiNs leaving a leaving a very bitter taste, particularly in Nigeria with its large industrial sector, in mouths of the textile and chemical partners who during malaria partners meetings at the time expressed a sense of betrayal.
 Talk arose in Nigeria about the potential for starting LLIN production in the country, but no one stepped forward with funding or technical assistance. In the meantime, on the other side of the continent, A to Z Textiles of Tanzania entered into a partnership and by 2003 LLINs were being produced in Arusha. Sumitomo Chemical provided a royalty-free technology license to the company for its Olyset LLINs. “By 2010, Olyset Net production capacity (at A to Z) reached 30 million LLINs per year, creating 8,000 jobs; more than half of the global Olyset Net output and an outstanding contribution to the local economy.”
Talk arose in Nigeria about the potential for starting LLIN production in the country, but no one stepped forward with funding or technical assistance. In the meantime, on the other side of the continent, A to Z Textiles of Tanzania entered into a partnership and by 2003 LLINs were being produced in Arusha. Sumitomo Chemical provided a royalty-free technology license to the company for its Olyset LLINs. “By 2010, Olyset Net production capacity (at A to Z) reached 30 million LLINs per year, creating 8,000 jobs; more than half of the global Olyset Net output and an outstanding contribution to the local economy.”
Over the years A to Z Textiles were hard pressed, just like the few other LLIN manufacturers, to meet global demand. Over the period, the focus changed from protecting young children and pregnant women to universal coverage of the population. Also research and actual use found that the lifespan of an LLIN was not the 5 years as initially projected, but more like two. These factors meant that supply could rarely meet demand for regular replacement nets. No wonder Rwanda wants its own LLIN factory!
 In addition to supply issues, does local availability of LLINs make a difference in fighting malaria? Regular studies by the Demographic and Health Survey group of USAID in Tanzania found that ITN use increased over time by children below five years of age. The most recent survey still shows that the 2010 Abuja target of 80% was not met (let alone a target of universal coverage), but the findings hint at the importance of having locally available LLINs.
In addition to supply issues, does local availability of LLINs make a difference in fighting malaria? Regular studies by the Demographic and Health Survey group of USAID in Tanzania found that ITN use increased over time by children below five years of age. The most recent survey still shows that the 2010 Abuja target of 80% was not met (let alone a target of universal coverage), but the findings hint at the importance of having locally available LLINs.
Let’s wish Rwanda success in establishing its LLIN manufacturing capacity. For colleagues in Nigeria and elsewhere who have expressed interest in this issue, your advocacy work is just beginning.
Communication &IPTp &ITNs &Treatment Bill Brieger | 04 Nov 2015
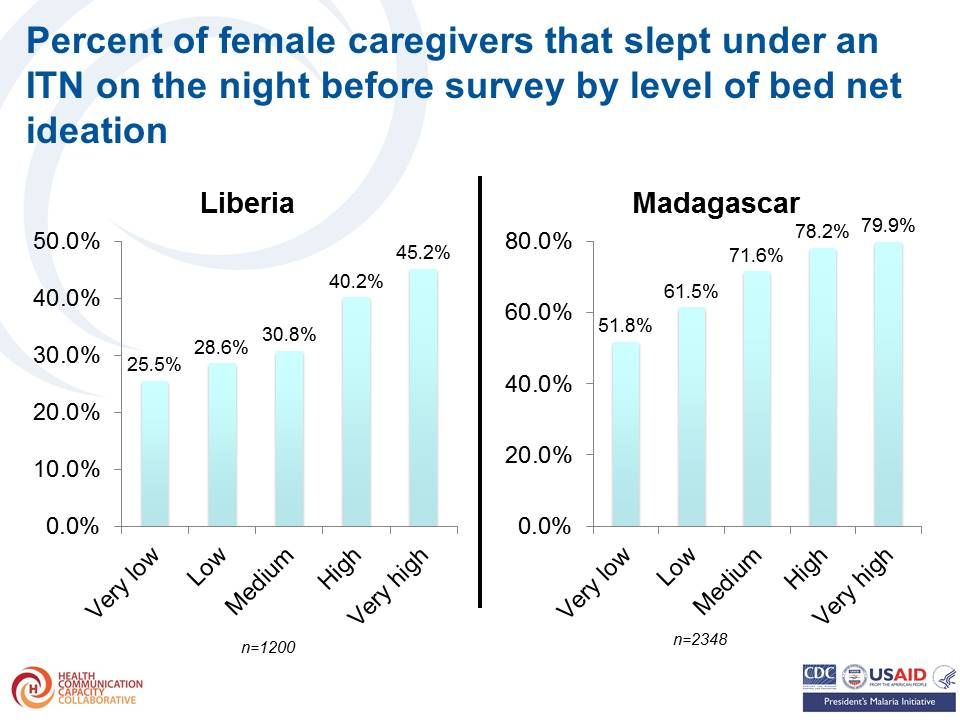
An Ideation Model: Attitudes, Beliefs and Practices Relevant to Malaria Prevention and Treatment in Madagascar and Liberia
Stella Babalola, Nan Lewicky, Grace Awantang, Michael Toso, Hannah Koenker, Arsene Ratsimbasoa, Monique Vololona of the Johns Hopkins Center for Communication Programs and the Division for Malaria Control, Madagascar Presented findings on how local perceptions help predict uptake of malaria interventions at the 143rd American Public Health Association Annual Meeting, October 31 – November 4, 2015, in Chicago. Their presentation on Liberia and Madagascar is summarized below.
While Liberia has an average malaria parasitemia prevalence of 28%, malaria is considerable less common in Madagascar and varies by region and altitude. This difference provides an interesting opportunity to observe similarities and contrasts in community perceptions of the disease.
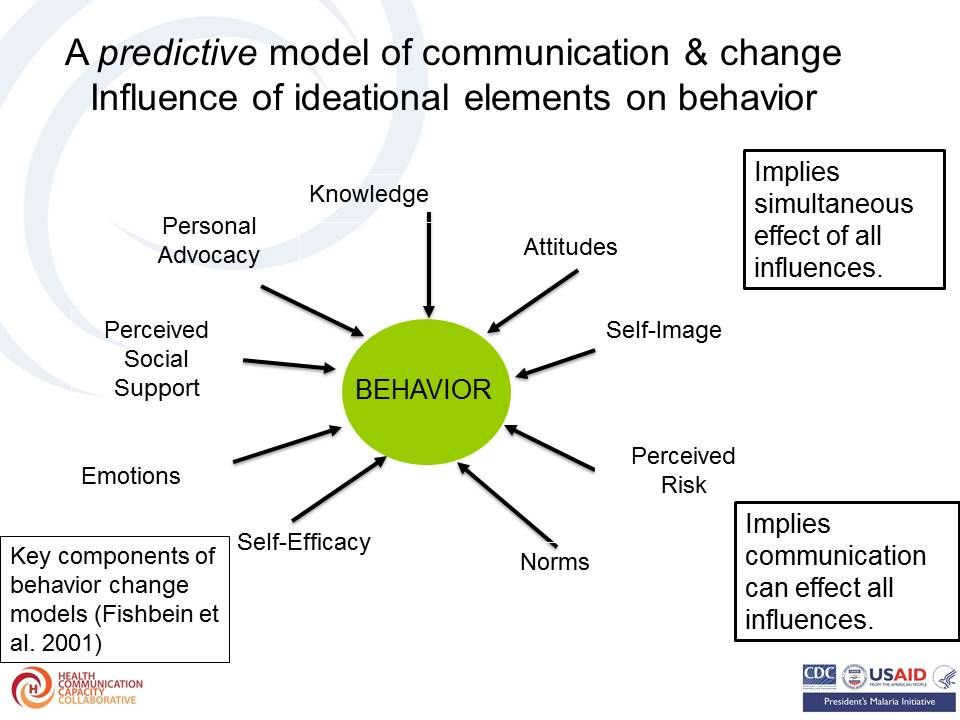
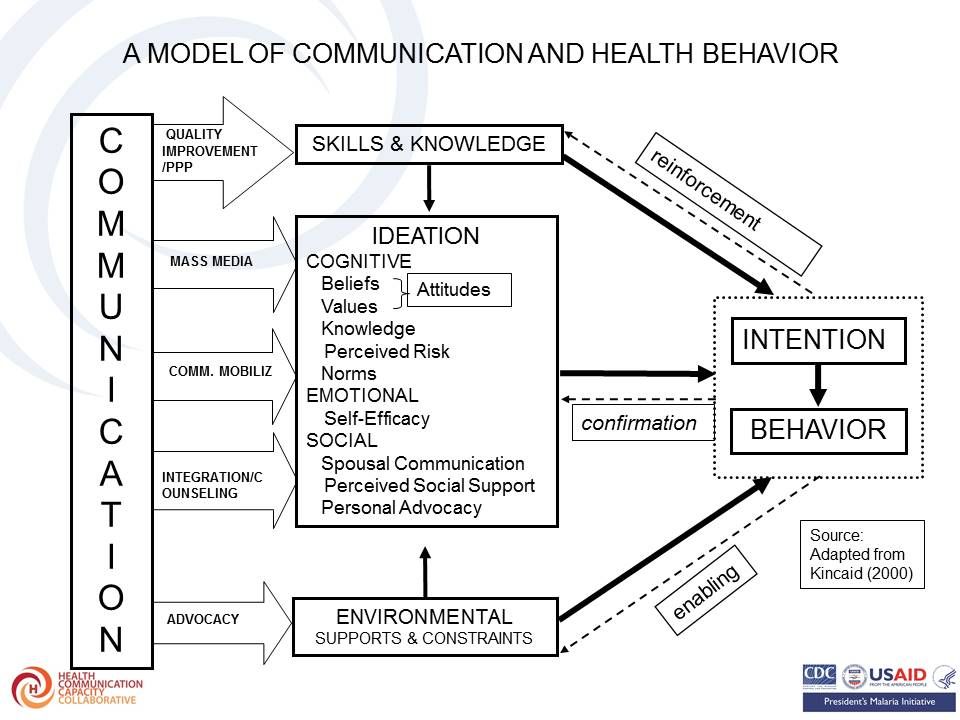 Theoretical basis of the research is based on the Ideation model which has been described as follows and as seen in the attached figures:
Theoretical basis of the research is based on the Ideation model which has been described as follows and as seen in the attached figures:
- “New ways of thinking and the diffusion of those ways of thinking by means of exposure to mass media and social interactions in local, culturally homogeneous communities” – Kincaid, 2000
- “views and ideas that people hold individually” – van de Kaa 1996
 The ideation model has successfully predicted current use of a contraceptive method as well as accessing childhood immunization. The team took up the challenge to learn whether this model would be applicable to malaria interventions.
The ideation model has successfully predicted current use of a contraceptive method as well as accessing childhood immunization. The team took up the challenge to learn whether this model would be applicable to malaria interventions.
Malaria-related ideation was proposed to consist of: Malaria knowledge (cause, symptom, prevention); Perceived susceptibility to malaria; Perceived severity of malaria; Perceived self-efficacy to prevent malaria; and Social interactions about malaria. These may lead to uptake of malaria interventions.
 Items for measuring bed net ideation could include – knowing where to procure a bed net, Willingness to pay for bed net, Having a positive attitudes towards bed net (derived from ten attitudinal statements), Perceived response-efficacy of bed nets, Perceived self-efficacy for procuring and using bed nets, Participation in household decisions about bed nets, Descriptive norm about bed net use and Social interactions about bed net use.
Items for measuring bed net ideation could include – knowing where to procure a bed net, Willingness to pay for bed net, Having a positive attitudes towards bed net (derived from ten attitudinal statements), Perceived response-efficacy of bed nets, Perceived self-efficacy for procuring and using bed nets, Participation in household decisions about bed nets, Descriptive norm about bed net use and Social interactions about bed net use.
Percent of female caregivers that slept under an ITN on the night before survey increased by level (score) of bed net ideation as seen in the graph. Results (odds ratio) of logistic regression of sleeping under an ITN on bed net ideation and other covariates showed a similar trend.
 Intermittent Preventive Treatment of Malaria in Pregnancy ideation measures included the following:
Intermittent Preventive Treatment of Malaria in Pregnancy ideation measures included the following:
- Knows name of the drug for malaria prevention during pregnancy
- Knows the timing of first dose of IPTp
- Has positive attitudes towards ANC and IPTp (derived from four attitudinal statements)
- Perceived response-efficacy of IPTp
- Woman participates in decisions about own health
- Social interactions about malaria and pregnancy
- Descriptive norm about ANC visits
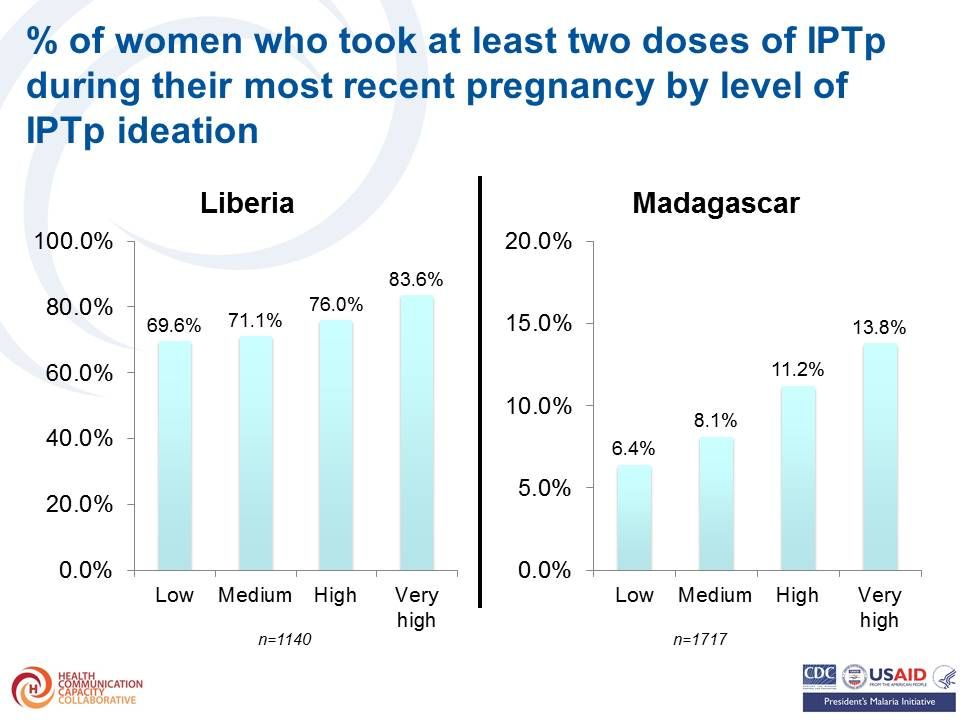 The percent of women who took at least two doses of IPTp during their most recent pregnancy also increased by level of IPTp ideation Likewise the results (odds ratio) of logistic regression of obtaining at least two doses of IPTp on IPTp ideation and other covariates were highest among those with highest levels of ideation.
The percent of women who took at least two doses of IPTp during their most recent pregnancy also increased by level of IPTp ideation Likewise the results (odds ratio) of logistic regression of obtaining at least two doses of IPTp on IPTp ideation and other covariates were highest among those with highest levels of ideation.
Items for measuring case management ideation included –
- Perceived response efficacy of malaria diagnostic test
- Perceived self-efficacy for detecting uncomplicated malaria
- Perceived self-efficacy for detecting severe malaria
- Descriptive norm about prompt treatment of malaria in children
- Social interactions about malaria treatment
- Participation in household decisions about child health
- Positive attitudes towards appropriate malaria treatment
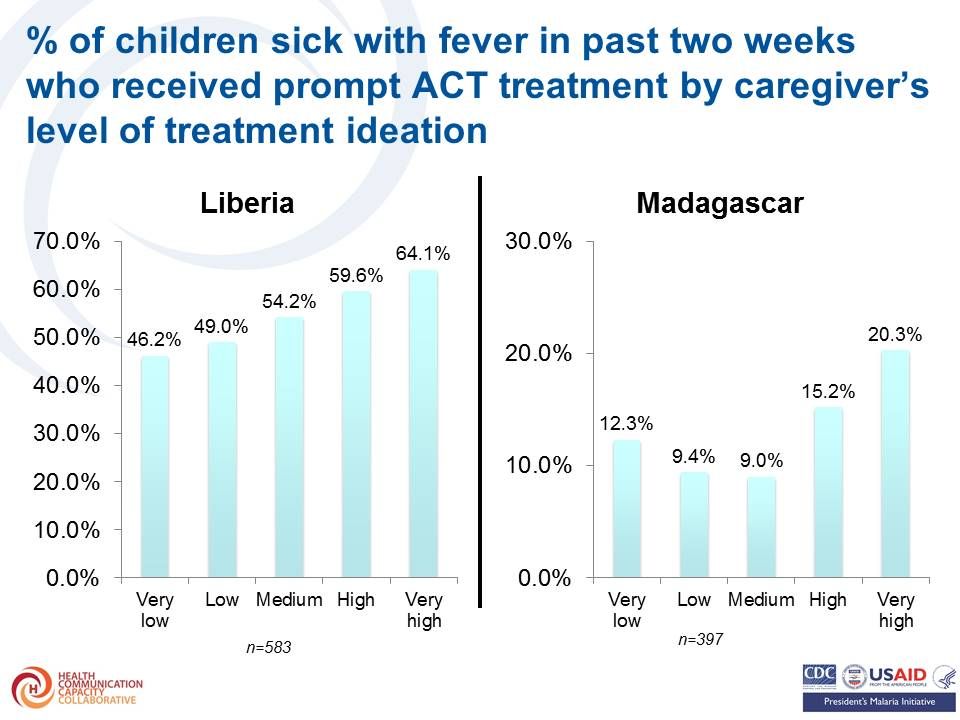 Again the percent of children sick with fever in past two weeks who received prompt ACT treatment by caregiver’s increased with increasing level of treatment ideation. As before the results (odds ratio) of logistic regression of prompt ACT treatment on caregiver’s treatment ideation and other covariates shows highest levels of ideation were associated with greated treatment seeking.
Again the percent of children sick with fever in past two weeks who received prompt ACT treatment by caregiver’s increased with increasing level of treatment ideation. As before the results (odds ratio) of logistic regression of prompt ACT treatment on caregiver’s treatment ideation and other covariates shows highest levels of ideation were associated with greated treatment seeking.
The team concluded that the same ideation model with demonstrated validity for family planning, child immunization, WASH and other health behaviors is relevant for malaria prevention and treatment. Strategically designed messages and interventions addressing ideational variables can help foster adoption of health-protective malaria prevention and treatment behaviors.
The authors acknowledge The US President’s Malaria Initiative (PMI) for technical guidance on the implementation of the surveys and The Ministry of Health and Social Welfare in Liberia and the Ministry of Health in Madagascar for their collaboration on the surveys.
CHW &Community &IPTi &ITNs &Malaria in Pregnancy &Treatment Bill Brieger | 01 Nov 2015
Community Directed Interventions to Enhance PHC and MCH
William Brieger of the Department of International Health, JHU Bloomberg School of Public Health, delivered the keynote address to the Community Based Primary Health Care Working Group at the 2015 American Public Health Association in Chicago. The focus was on Community Directed Interventions (CDI) as a way to enhance implementation of primary health care and maternal and child health. Some excerpt from the talk follow.
 The origins of the CDI Approach are based in Onchocerciasis Control and the implementation research done by the Tropical Disease Research (TDR) Program of WHO and collaborating agencies to help establish the foundational guidance of the African Program for Onchocerciasis Control in 1995. Since then we have seen an expansion of CDI into other health issues
The origins of the CDI Approach are based in Onchocerciasis Control and the implementation research done by the Tropical Disease Research (TDR) Program of WHO and collaborating agencies to help establish the foundational guidance of the African Program for Onchocerciasis Control in 1995. Since then we have seen an expansion of CDI into other health issues
We should start discussion with an understanding of ‘community’ which Rifkin et al. (1988) defined as a group of people living in the same defined area sharing basic values, organization, and interests. White (1982) proposed that community is an informally organized social entity which is characterized by a sense of identity. Manderson et al. (1992) in their work for TDR defined community as a population which is geographically focused but which also exists as a discrete social entity, with a local collective identity and corporate purpose.
Communities are people sharing values and institutions. Community is based on locality (geographic), interdependent social groups, interpersonal relationships expressed through social networks and built on s culture that includes values, norms, and attachments to the community as a whole as well as to its parts. Prior to developing any community intervention we must understand the boundaries, composition and structure of a community from the perspectives of its own members, as their local knowledge and participation are central to success.
 Community Systems Strengthening has been taken up by the Global Fund in order to enhance coverage of various health interventions such as HIV drugs and bednets to prevent malaria. Community systems are community?led structures and mechanisms used by communities through which community members and community based organizations and groups interact, coordinate and deliver their responses to the challenges and needs affecting their communities. Many community systems are small?scale and/or informal. Others are more extensive – they may be networked between several organizations and involve various sub?systems. For example, a large care and support system may have distinct sub?systems for comprehensive home?based care, providing nutritional support, counselling, advocacy, legal support, and referrals for access to services and follow?up.
Community Systems Strengthening has been taken up by the Global Fund in order to enhance coverage of various health interventions such as HIV drugs and bednets to prevent malaria. Community systems are community?led structures and mechanisms used by communities through which community members and community based organizations and groups interact, coordinate and deliver their responses to the challenges and needs affecting their communities. Many community systems are small?scale and/or informal. Others are more extensive – they may be networked between several organizations and involve various sub?systems. For example, a large care and support system may have distinct sub?systems for comprehensive home?based care, providing nutritional support, counselling, advocacy, legal support, and referrals for access to services and follow?up.
Efficacy, Social Control and Cohesion are important characteristics of communities that enable them to take on project and solve problems. Collective Efficacy is a perceived ability to work together. Social control provides evidence that communities are able to enforce their norms. Cohesion describes social interaction that brings people together. A strong sense of identity and a sense of belonging describe communities that can get things done. These characteristics lead to community competency to collaborate effectively in identifying the problems/needs of the community, achieve a working consensus on goals and priorities, agree on ways and means to implement the agreed-upon goals, and collaborate effectively in the required actions.
 It is important to distinguish between Community Based Intervention (CBI) and Community Directed Intervention. CBI takes place in the community but a Health/Development agency exercises authority over decisions on project design and implementation. Project activities (e.g., service delivery dates and procedures) are designed by the agency. Activities simply happen in the community.
It is important to distinguish between Community Based Intervention (CBI) and Community Directed Intervention. CBI takes place in the community but a Health/Development agency exercises authority over decisions on project design and implementation. Project activities (e.g., service delivery dates and procedures) are designed by the agency. Activities simply happen in the community.
With CDI the community exercises authority over decisions and decides on acceptable method to implement projects. This ensures sensitivity to local decision-making structures and social life. Activities happen both in and by the community; the community is in control.
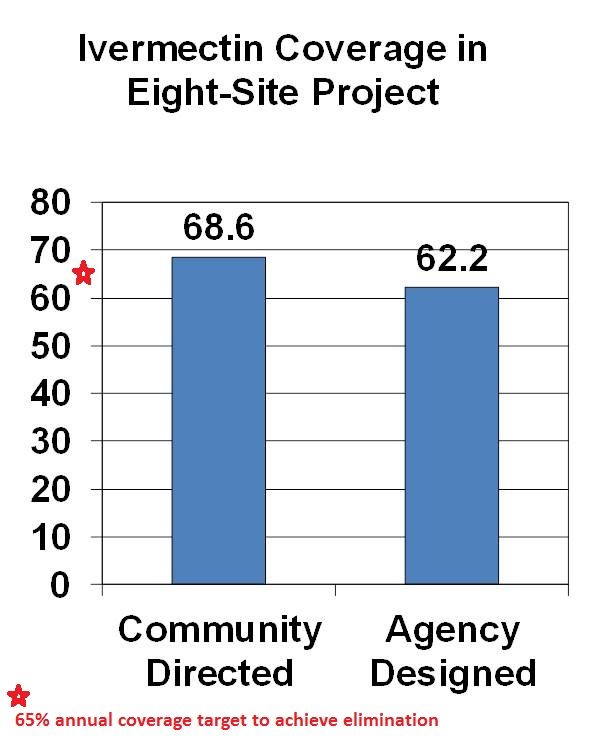
CDI was pioneered for Onchocerciasis (River Blindness) Control as community directed treatment with ivermectin (CDTI). When communities are in charge, coverage is better than when ivermectin distribution is centrally organized by a health agency. The original 1995 CDI field testing showed better ivermectin coverage when the community was in charge of distribution. Since the beginning of CDTI, over 200,000 villages in 18 African countries have been distributing ivermectin annually through their own efforts. Lessons learned over the years are that CDI works best when 1) the smallest level of an organized community is the basis of action (e.g. a hamlet, a clan/kin group) and 2) communities are encouraged to choose as many CDDs as they think they need to get the job done. This means that the community is in charge, not individual volunteers who can be replaced anytime the community finds the need.
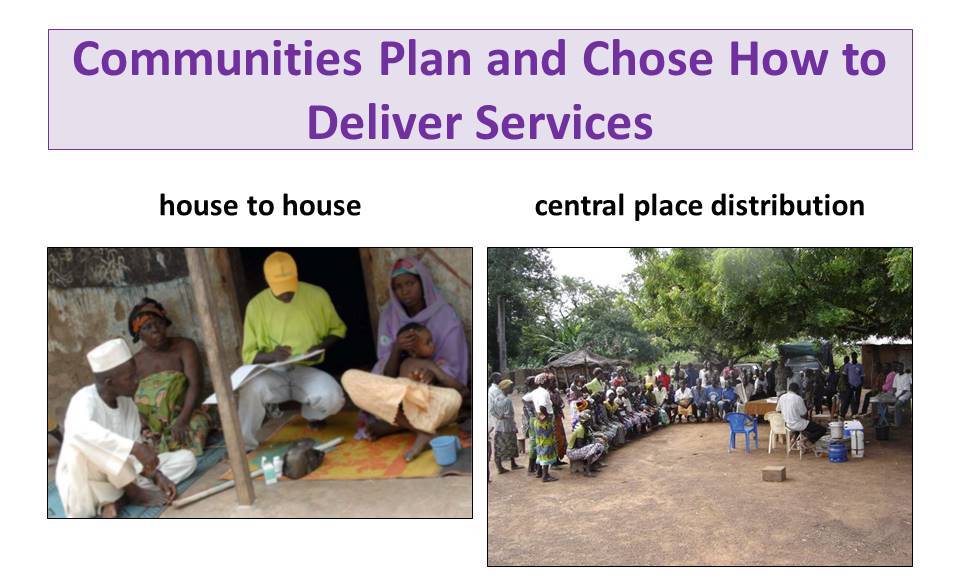
With CDI for onchocerciasis or any other health program, Communities plan and chose how to deliver services. This may be house-to-house, central place distribution or a combination. Health workers provide training and supervision to volunteer village health workers called community directed distributors (CDDs).
 TDR observed that CDI naturally expanded to include other services wanted by the community such as immunization, community development, water and sanitation, agriculture and forestry, HIV-AIDS, family planning, guinea worm, Vitamin A. TDR and APOC then decided that CDI with other service components should be systematically tested. The project sites added in a systematic manner other interventions to existing CDTI programs including home management of malaria, ITN distribution & promotion, TB DOTS, Vitamin A in addition to continued ivermectin distribution. These services varied in complexity and communities responded by dividing the work among several different volunteers.
TDR observed that CDI naturally expanded to include other services wanted by the community such as immunization, community development, water and sanitation, agriculture and forestry, HIV-AIDS, family planning, guinea worm, Vitamin A. TDR and APOC then decided that CDI with other service components should be systematically tested. The project sites added in a systematic manner other interventions to existing CDTI programs including home management of malaria, ITN distribution & promotion, TB DOTS, Vitamin A in addition to continued ivermectin distribution. These services varied in complexity and communities responded by dividing the work among several different volunteers.
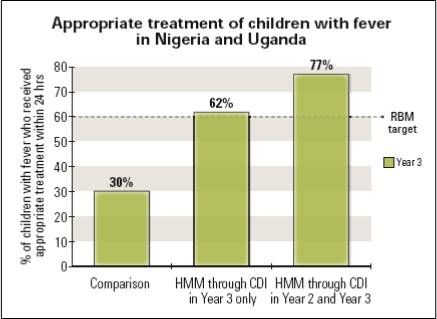 Coverage of interventions like malaria case management, ITN promotion and Vitamin A distribution was higher in the intervention areas compared to the delivery of these services through the routine health system. TB DOTS presented the only challenge because of the social stigma associated with the disease. The study concluded that CDI can effectively incorporate high impact, evidence based interventions while at the same time maintaining and increasing ivermectin coverage. Since CDI does not rely on one volunteer but whole community effort, the problem of overburdening on community health worker did not arise. Other incterventions ould benefit from CDI such as Misoprostol, Intermittent Preventive Treatment, Deworming, Oral Rehydration solution, Zinc, Cotrimoxazole, Amoxicillin, Soap for handwashing and WaterGuard treatment kits.
Coverage of interventions like malaria case management, ITN promotion and Vitamin A distribution was higher in the intervention areas compared to the delivery of these services through the routine health system. TB DOTS presented the only challenge because of the social stigma associated with the disease. The study concluded that CDI can effectively incorporate high impact, evidence based interventions while at the same time maintaining and increasing ivermectin coverage. Since CDI does not rely on one volunteer but whole community effort, the problem of overburdening on community health worker did not arise. Other incterventions ould benefit from CDI such as Misoprostol, Intermittent Preventive Treatment, Deworming, Oral Rehydration solution, Zinc, Cotrimoxazole, Amoxicillin, Soap for handwashing and WaterGuard treatment kits.
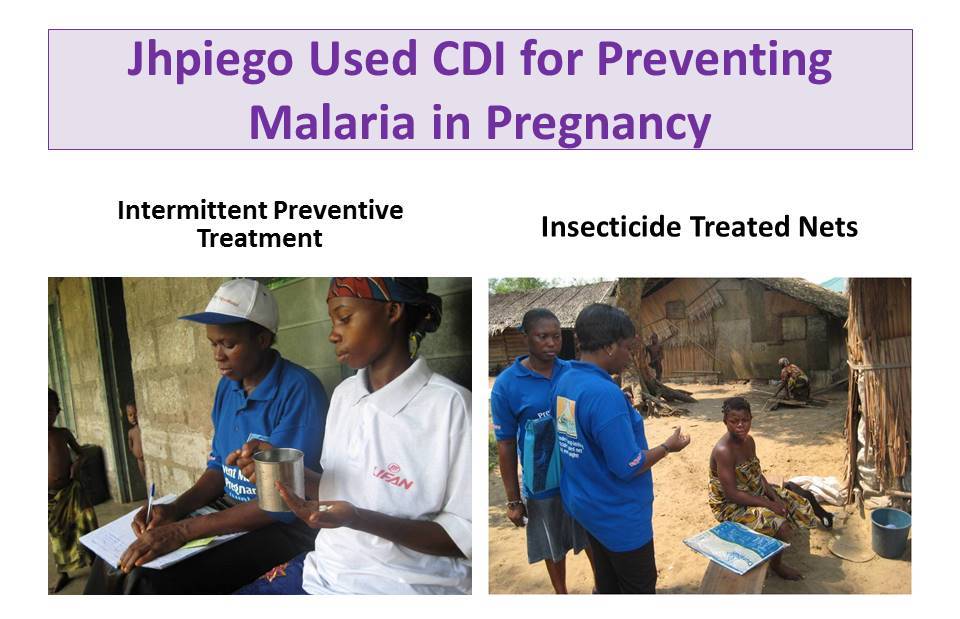 Jhpiego an NGO affiliate of the Johns Hopkins University used CDI to deliver malaria in pregnancy (MIP) prevention services in Nigeria including Intermittent Preventive Treatment and Insecticide Treated Nets. Contrary to fears that CDI would detract from antenatal care attendance, the work of CDDs actually ensured that ANC attendance increased over time. Through CDI IPTp coverage increased compared to control communities and more pregnant women slept under ITNs regularly.
Jhpiego an NGO affiliate of the Johns Hopkins University used CDI to deliver malaria in pregnancy (MIP) prevention services in Nigeria including Intermittent Preventive Treatment and Insecticide Treated Nets. Contrary to fears that CDI would detract from antenatal care attendance, the work of CDDs actually ensured that ANC attendance increased over time. Through CDI IPTp coverage increased compared to control communities and more pregnant women slept under ITNs regularly.
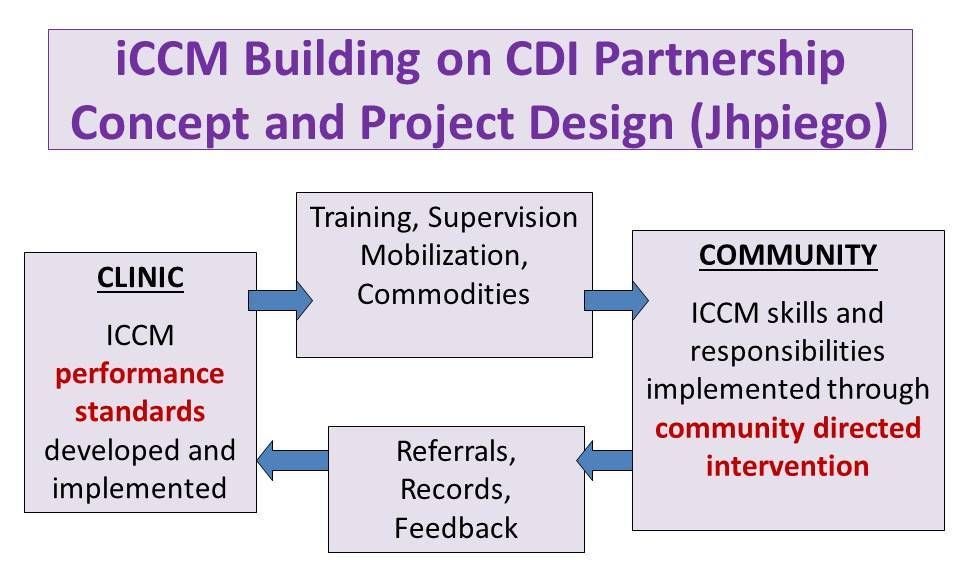 Jhpiego next expanded CDI for MIP into integrated Community Case Management (iCCM), thus taking community case management beyond community based care. Giving communities responsibility for organizing and managing their services using the CDI approach meant greater access to services whenever people need them. Using the CDI approach to iCCM CDDs reached 7,504 clients who presented signs and symptoms of malaria. CDDs successfully conducted malaria diagnosis using the rapid diagnostic test (RDT) kits. Overall, 47.8% tested positive while 52.2% tested negative. CDDs adhered to guidelines and all the 3,587 clients with positive RDT results received appropriate anti-malarial medicines. As appropriate 21.0% were treated for diarrhoea, 11.0% for pneumonia (of whom 68.0% were referred to the health facility)
Jhpiego next expanded CDI for MIP into integrated Community Case Management (iCCM), thus taking community case management beyond community based care. Giving communities responsibility for organizing and managing their services using the CDI approach meant greater access to services whenever people need them. Using the CDI approach to iCCM CDDs reached 7,504 clients who presented signs and symptoms of malaria. CDDs successfully conducted malaria diagnosis using the rapid diagnostic test (RDT) kits. Overall, 47.8% tested positive while 52.2% tested negative. CDDs adhered to guidelines and all the 3,587 clients with positive RDT results received appropriate anti-malarial medicines. As appropriate 21.0% were treated for diarrhoea, 11.0% for pneumonia (of whom 68.0% were referred to the health facility)
 A Supervisory Checklist and Performance Standards were developed and used for Assessing CDD performance. The results were discussed at monthly CDD meetings at their nearest health facilities. This led to further improvements in History taking, Examination, Conducting RDTs for Malaria and Illness Management.
A Supervisory Checklist and Performance Standards were developed and used for Assessing CDD performance. The results were discussed at monthly CDD meetings at their nearest health facilities. This led to further improvements in History taking, Examination, Conducting RDTs for Malaria and Illness Management.
TDR has done further scoping to learn if CDI would be acceptable by health workers and community members in Urban, Nomadic and Underserved Rural Communities. CDI was favorable received. In conclusion we have learned over the years that CDI can involve women, families and communities in meeting their own health needs.