CHW &Community &IPTi &ITNs &Malaria in Pregnancy &Treatment Bill Brieger | 01 Nov 2015 10:38 am
Community Directed Interventions to Enhance PHC and MCH
William Brieger of the Department of International Health, JHU Bloomberg School of Public Health, delivered the keynote address to the Community Based Primary Health Care Working Group at the 2015 American Public Health Association in Chicago. The focus was on Community Directed Interventions (CDI) as a way to enhance implementation of primary health care and maternal and child health. Some excerpt from the talk follow.
 The origins of the CDI Approach are based in Onchocerciasis Control and the implementation research done by the Tropical Disease Research (TDR) Program of WHO and collaborating agencies to help establish the foundational guidance of the African Program for Onchocerciasis Control in 1995. Since then we have seen an expansion of CDI into other health issues
The origins of the CDI Approach are based in Onchocerciasis Control and the implementation research done by the Tropical Disease Research (TDR) Program of WHO and collaborating agencies to help establish the foundational guidance of the African Program for Onchocerciasis Control in 1995. Since then we have seen an expansion of CDI into other health issues
We should start discussion with an understanding of ‘community’ which Rifkin et al. (1988) defined as a group of people living in the same defined area sharing basic values, organization, and interests. White (1982) proposed that community is an informally organized social entity which is characterized by a sense of identity. Manderson et al. (1992) in their work for TDR defined community as a population which is geographically focused but which also exists as a discrete social entity, with a local collective identity and corporate purpose.
Communities are people sharing values and institutions. Community is based on locality (geographic), interdependent social groups, interpersonal relationships expressed through social networks and built on s culture that includes values, norms, and attachments to the community as a whole as well as to its parts. Prior to developing any community intervention we must understand the boundaries, composition and structure of a community from the perspectives of its own members, as their local knowledge and participation are central to success.
 Community Systems Strengthening has been taken up by the Global Fund in order to enhance coverage of various health interventions such as HIV drugs and bednets to prevent malaria. Community systems are community?led structures and mechanisms used by communities through which community members and community based organizations and groups interact, coordinate and deliver their responses to the challenges and needs affecting their communities. Many community systems are small?scale and/or informal. Others are more extensive – they may be networked between several organizations and involve various sub?systems. For example, a large care and support system may have distinct sub?systems for comprehensive home?based care, providing nutritional support, counselling, advocacy, legal support, and referrals for access to services and follow?up.
Community Systems Strengthening has been taken up by the Global Fund in order to enhance coverage of various health interventions such as HIV drugs and bednets to prevent malaria. Community systems are community?led structures and mechanisms used by communities through which community members and community based organizations and groups interact, coordinate and deliver their responses to the challenges and needs affecting their communities. Many community systems are small?scale and/or informal. Others are more extensive – they may be networked between several organizations and involve various sub?systems. For example, a large care and support system may have distinct sub?systems for comprehensive home?based care, providing nutritional support, counselling, advocacy, legal support, and referrals for access to services and follow?up.
Efficacy, Social Control and Cohesion are important characteristics of communities that enable them to take on project and solve problems. Collective Efficacy is a perceived ability to work together. Social control provides evidence that communities are able to enforce their norms. Cohesion describes social interaction that brings people together. A strong sense of identity and a sense of belonging describe communities that can get things done. These characteristics lead to community competency to collaborate effectively in identifying the problems/needs of the community, achieve a working consensus on goals and priorities, agree on ways and means to implement the agreed-upon goals, and collaborate effectively in the required actions.
 It is important to distinguish between Community Based Intervention (CBI) and Community Directed Intervention. CBI takes place in the community but a Health/Development agency exercises authority over decisions on project design and implementation. Project activities (e.g., service delivery dates and procedures) are designed by the agency. Activities simply happen in the community.
It is important to distinguish between Community Based Intervention (CBI) and Community Directed Intervention. CBI takes place in the community but a Health/Development agency exercises authority over decisions on project design and implementation. Project activities (e.g., service delivery dates and procedures) are designed by the agency. Activities simply happen in the community.
With CDI the community exercises authority over decisions and decides on acceptable method to implement projects. This ensures sensitivity to local decision-making structures and social life. Activities happen both in and by the community; the community is in control.
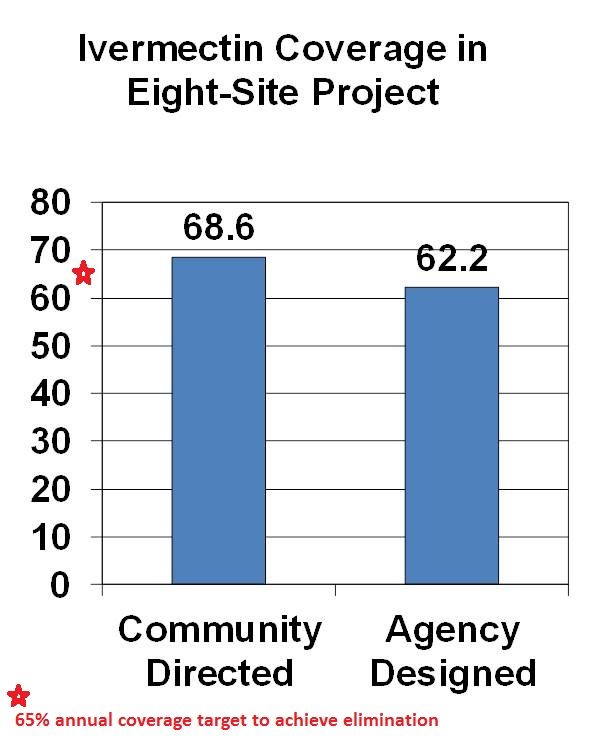
CDI was pioneered for Onchocerciasis (River Blindness) Control as community directed treatment with ivermectin (CDTI). When communities are in charge, coverage is better than when ivermectin distribution is centrally organized by a health agency. The original 1995 CDI field testing showed better ivermectin coverage when the community was in charge of distribution. Since the beginning of CDTI, over 200,000 villages in 18 African countries have been distributing ivermectin annually through their own efforts. Lessons learned over the years are that CDI works best when 1) the smallest level of an organized community is the basis of action (e.g. a hamlet, a clan/kin group) and 2) communities are encouraged to choose as many CDDs as they think they need to get the job done. This means that the community is in charge, not individual volunteers who can be replaced anytime the community finds the need.
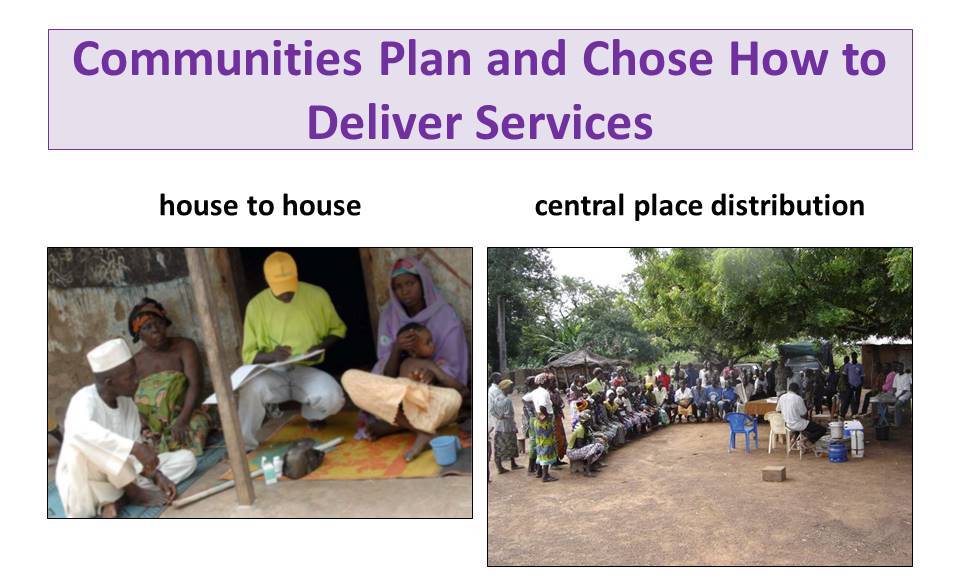
With CDI for onchocerciasis or any other health program, Communities plan and chose how to deliver services. This may be house-to-house, central place distribution or a combination. Health workers provide training and supervision to volunteer village health workers called community directed distributors (CDDs).
 TDR observed that CDI naturally expanded to include other services wanted by the community such as immunization, community development, water and sanitation, agriculture and forestry, HIV-AIDS, family planning, guinea worm, Vitamin A. TDR and APOC then decided that CDI with other service components should be systematically tested. The project sites added in a systematic manner other interventions to existing CDTI programs including home management of malaria, ITN distribution & promotion, TB DOTS, Vitamin A in addition to continued ivermectin distribution. These services varied in complexity and communities responded by dividing the work among several different volunteers.
TDR observed that CDI naturally expanded to include other services wanted by the community such as immunization, community development, water and sanitation, agriculture and forestry, HIV-AIDS, family planning, guinea worm, Vitamin A. TDR and APOC then decided that CDI with other service components should be systematically tested. The project sites added in a systematic manner other interventions to existing CDTI programs including home management of malaria, ITN distribution & promotion, TB DOTS, Vitamin A in addition to continued ivermectin distribution. These services varied in complexity and communities responded by dividing the work among several different volunteers.
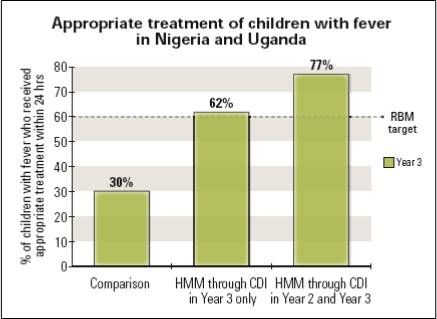 Coverage of interventions like malaria case management, ITN promotion and Vitamin A distribution was higher in the intervention areas compared to the delivery of these services through the routine health system. TB DOTS presented the only challenge because of the social stigma associated with the disease. The study concluded that CDI can effectively incorporate high impact, evidence based interventions while at the same time maintaining and increasing ivermectin coverage. Since CDI does not rely on one volunteer but whole community effort, the problem of overburdening on community health worker did not arise. Other incterventions ould benefit from CDI such as Misoprostol, Intermittent Preventive Treatment, Deworming, Oral Rehydration solution, Zinc, Cotrimoxazole, Amoxicillin, Soap for handwashing and WaterGuard treatment kits.
Coverage of interventions like malaria case management, ITN promotion and Vitamin A distribution was higher in the intervention areas compared to the delivery of these services through the routine health system. TB DOTS presented the only challenge because of the social stigma associated with the disease. The study concluded that CDI can effectively incorporate high impact, evidence based interventions while at the same time maintaining and increasing ivermectin coverage. Since CDI does not rely on one volunteer but whole community effort, the problem of overburdening on community health worker did not arise. Other incterventions ould benefit from CDI such as Misoprostol, Intermittent Preventive Treatment, Deworming, Oral Rehydration solution, Zinc, Cotrimoxazole, Amoxicillin, Soap for handwashing and WaterGuard treatment kits.
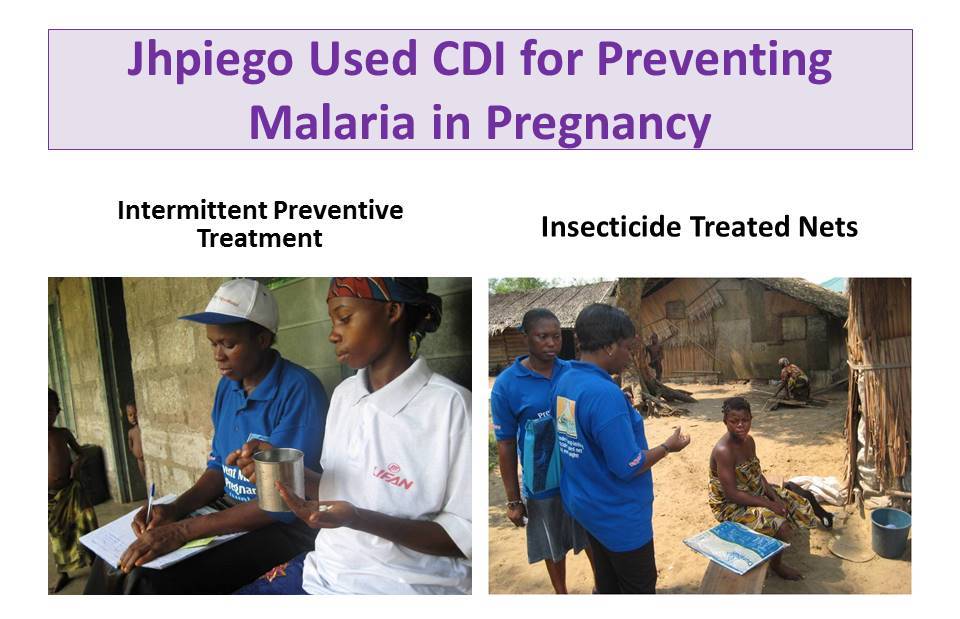 Jhpiego an NGO affiliate of the Johns Hopkins University used CDI to deliver malaria in pregnancy (MIP) prevention services in Nigeria including Intermittent Preventive Treatment and Insecticide Treated Nets. Contrary to fears that CDI would detract from antenatal care attendance, the work of CDDs actually ensured that ANC attendance increased over time. Through CDI IPTp coverage increased compared to control communities and more pregnant women slept under ITNs regularly.
Jhpiego an NGO affiliate of the Johns Hopkins University used CDI to deliver malaria in pregnancy (MIP) prevention services in Nigeria including Intermittent Preventive Treatment and Insecticide Treated Nets. Contrary to fears that CDI would detract from antenatal care attendance, the work of CDDs actually ensured that ANC attendance increased over time. Through CDI IPTp coverage increased compared to control communities and more pregnant women slept under ITNs regularly.
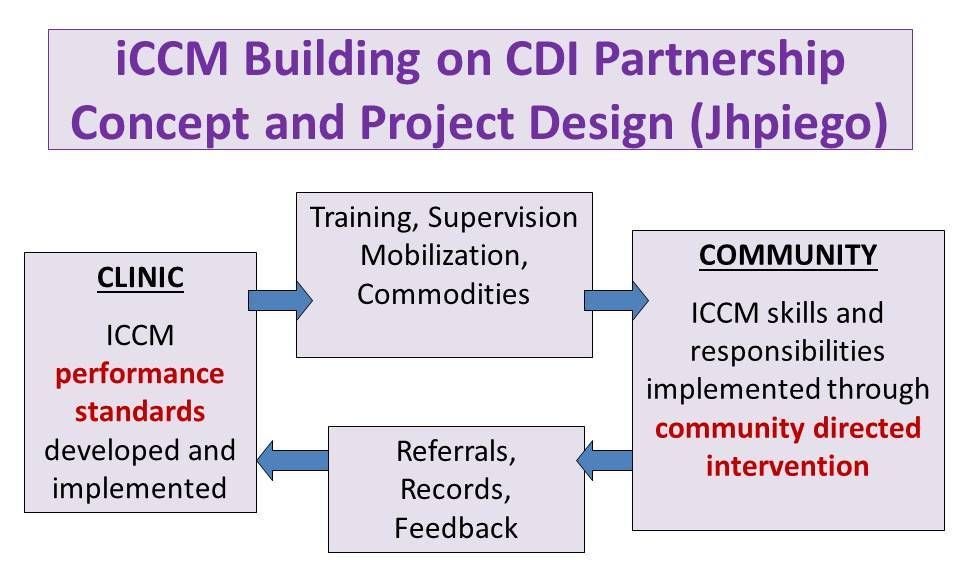 Jhpiego next expanded CDI for MIP into integrated Community Case Management (iCCM), thus taking community case management beyond community based care. Giving communities responsibility for organizing and managing their services using the CDI approach meant greater access to services whenever people need them. Using the CDI approach to iCCM CDDs reached 7,504 clients who presented signs and symptoms of malaria. CDDs successfully conducted malaria diagnosis using the rapid diagnostic test (RDT) kits. Overall, 47.8% tested positive while 52.2% tested negative. CDDs adhered to guidelines and all the 3,587 clients with positive RDT results received appropriate anti-malarial medicines. As appropriate 21.0% were treated for diarrhoea, 11.0% for pneumonia (of whom 68.0% were referred to the health facility)
Jhpiego next expanded CDI for MIP into integrated Community Case Management (iCCM), thus taking community case management beyond community based care. Giving communities responsibility for organizing and managing their services using the CDI approach meant greater access to services whenever people need them. Using the CDI approach to iCCM CDDs reached 7,504 clients who presented signs and symptoms of malaria. CDDs successfully conducted malaria diagnosis using the rapid diagnostic test (RDT) kits. Overall, 47.8% tested positive while 52.2% tested negative. CDDs adhered to guidelines and all the 3,587 clients with positive RDT results received appropriate anti-malarial medicines. As appropriate 21.0% were treated for diarrhoea, 11.0% for pneumonia (of whom 68.0% were referred to the health facility)
 A Supervisory Checklist and Performance Standards were developed and used for Assessing CDD performance. The results were discussed at monthly CDD meetings at their nearest health facilities. This led to further improvements in History taking, Examination, Conducting RDTs for Malaria and Illness Management.
A Supervisory Checklist and Performance Standards were developed and used for Assessing CDD performance. The results were discussed at monthly CDD meetings at their nearest health facilities. This led to further improvements in History taking, Examination, Conducting RDTs for Malaria and Illness Management.
TDR has done further scoping to learn if CDI would be acceptable by health workers and community members in Urban, Nomadic and Underserved Rural Communities. CDI was favorable received. In conclusion we have learned over the years that CDI can involve women, families and communities in meeting their own health needs.