Case Management &CHW &IPTp &ITNs Bill Brieger | 14 Apr 2018
Community Health Volunteers Contribute to Improved Malaria Prevention and Management in Kribi, Cameroon
Kodjo Morgah, Eric Tchinda, and Naibei Mbaïbardoum of Jhpiego (a Johns Hopkins University Affiliate) in Cameroon are presenting a poster at the Multilateral Initiative for Malaria Conference in Dakar this week. Their findings, seen below, show how community health volunteers can contribute to improving the quality of malaria control services in Chad and Cameroon.

CHV Lilian Kubeh preparing to administer a rapid diagnostic test. Photo by Karen Kasmauski.
Project objectives focused overall on contributing to the reduction of malaria-related morbidity and mortality in Cameroon and Chad. It also aimed to strengthen community-based interventions through the use of community health volunteers (CHVs) to manage simple cases of malaria and conduct awareness-raising activities. The geographic scope of the project was Kribi District in the south of Cameroon. Thirty-two health facilities are supported by Jhpiego. Kribi District has an estimated population of 134,876.
Reports from the National Malaria Control Program show that malaria is the leading cause of morbidity in Cameroon—an estimated 1,500,000 cases occur each year. In 2016, it was the leading reason for medical consultations (23.6% of all medical consultations) and hospitalizations (46% of all hospitalizations). Among children under 5 years of age, malaria accounted for 41% of all medical consultations and 55% of all hospitalizations. Malaria is also a leading cause of mortality. In 2016, Cameroon had 2,639 deaths caused by malaria—12% of all deaths across all age groups and 28% of all deaths among children under 5 years of age were attributed to malaria.
 Project intervention strategies target the four levels of the health system. The CHV intervention was mobilized to support the strategy at the community level as seen in the attached diagram. In 2012 and 2014, 38 CHVs were selected by the community and received training to support areas in the district more than 10 km from a health center. (Note: 10 km was the measurement tool used to determine the geographic scope of each CHV for this project.) An initial donation of medications, data collection tools, and small equipment was made available to CHVs using funding from ExxonMobil Foundation. An evaluation of the training intervention was conducted by an external consultant in April 2016.
Project intervention strategies target the four levels of the health system. The CHV intervention was mobilized to support the strategy at the community level as seen in the attached diagram. In 2012 and 2014, 38 CHVs were selected by the community and received training to support areas in the district more than 10 km from a health center. (Note: 10 km was the measurement tool used to determine the geographic scope of each CHV for this project.) An initial donation of medications, data collection tools, and small equipment was made available to CHVs using funding from ExxonMobil Foundation. An evaluation of the training intervention was conducted by an external consultant in April 2016.

CHV Daniel Ze conducting an individual educational session on IPTp. Photo by Karen Kasmauski.
CHVs conduct outreach activities in their communities—via home visits and community education sessions—to provide health education on malaria transmission and prevention, use of long-lasting insecticidal nets, the importance of intermittent preventive treatment in pregnancy (IPTp), and the importance of promptly seeking medical care for suspected cases of malaria. CHVs also support national health campaigns and health promotion events, including World Malaria Day. In Cameroon, where CHVs are also able to test and treat patients, they administer rapid diagnostic tests (RDTs) and treat cases of uncomplicated malaria.
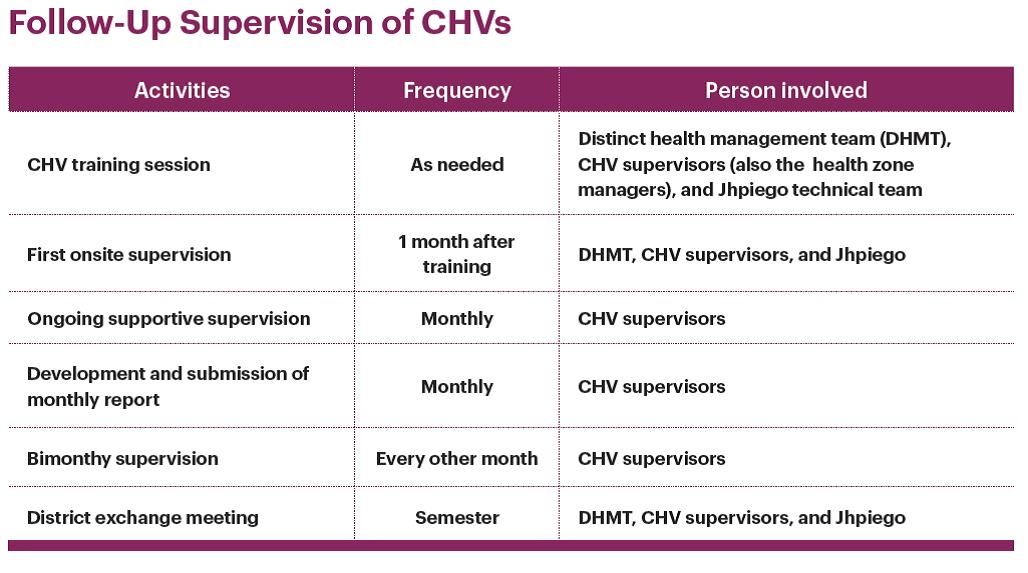 Motivation of CHVs included ongoing training and technical updates, regular replenishment of materials, CHVs are recognized and respected community leaders, provision of per diem and transport costs, and continued advocacy targeting district officials to provide CHV stipends to ensure sustainability. Attached are details of the supervisory activities that provided continual technical support to the CHVs to ensure that they retain knowledge and skills to carry out their activities and track their data.
Motivation of CHVs included ongoing training and technical updates, regular replenishment of materials, CHVs are recognized and respected community leaders, provision of per diem and transport costs, and continued advocacy targeting district officials to provide CHV stipends to ensure sustainability. Attached are details of the supervisory activities that provided continual technical support to the CHVs to ensure that they retain knowledge and skills to carry out their activities and track their data.
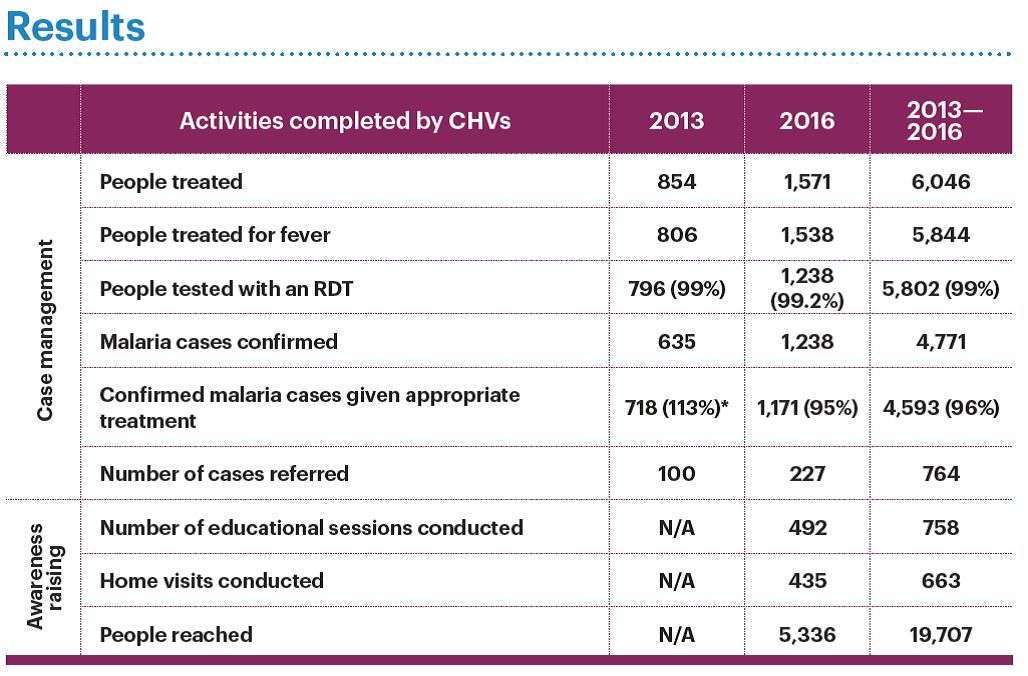 Between 2013 and 2016 CHVs in these communities were able to reach nearly 20,000 people with a variety of malaria services as seen in the attached table. The project paid close attention to data quality, which was reviewed with the CHVs on a regular basis, resulting in improved data quality. CHVs improved the accessibility of malaria prevention and care services for communities living in remote areas. Results from April 2016 external evaluation show these results. Knowledge of malaria prevention is significantly higher in households that did not receive CHV support (p = 0.001). Use of long-lasting insecticide-treated nets is higher in households that benefitted from CHV support (88%) than in households that did not benefit from CHV support (73%) (p = 0.023). There was an increase in the delivery of IPTp2, from 60% in 2012 to 70% in 2016.
Between 2013 and 2016 CHVs in these communities were able to reach nearly 20,000 people with a variety of malaria services as seen in the attached table. The project paid close attention to data quality, which was reviewed with the CHVs on a regular basis, resulting in improved data quality. CHVs improved the accessibility of malaria prevention and care services for communities living in remote areas. Results from April 2016 external evaluation show these results. Knowledge of malaria prevention is significantly higher in households that did not receive CHV support (p = 0.001). Use of long-lasting insecticide-treated nets is higher in households that benefitted from CHV support (88%) than in households that did not benefit from CHV support (73%) (p = 0.023). There was an increase in the delivery of IPTp2, from 60% in 2012 to 70% in 2016.
In conclusion CHVs have increased their communities’ access to health centers through referrals, health education on malaria prevention, IPTp, and treatment for simple and severe cases of malaria. Regular supervision of CHVs by their supervisors (the health zone managers) is essential to maintaining and strengthening CHV performance and motivation. Continuing advocacy efforts with local authorities is necessary to ensure that CHV activities are sustainable. The project team aims to establish a mechanism to improve documentation of its activities to better measure the impact on indicators at the community, facility, and district levels, and provide evidence for advocacy to sustain these efforts.
Diagnosis &Health Systems &IPTp &ITNs &Universal Coverage Bill Brieger | 31 Mar 2018
Universal Health Coverage – Where is Malaria?
 Universal Health Coverage (UHC) is the theme of the 2018 World Health Day on April 7th. The concept was applied to malaria in 2009 regarding the provision of long lasting insecticide-treated nets (LLINs aka ITNs) with the definition of universal meaning one net for every two persons in a household. Up until that time coverage targets for malaria interventions set at the 2000 Abuja Declaration had focused on achieving by the year 2010, 80% of people (particularly pregnant women and children below the age of 5 years) sleeping under ITNs, 80% of children receiving appropriate malaria treatment with artemisinin-based combination therapy (ACTs) within 24 hours of onset of illness and 80% of pregnant women receiving two doses of Intermittent Preventive Treatment (IPTp) for malaria as part of antenatal care (ANC).
Universal Health Coverage (UHC) is the theme of the 2018 World Health Day on April 7th. The concept was applied to malaria in 2009 regarding the provision of long lasting insecticide-treated nets (LLINs aka ITNs) with the definition of universal meaning one net for every two persons in a household. Up until that time coverage targets for malaria interventions set at the 2000 Abuja Declaration had focused on achieving by the year 2010, 80% of people (particularly pregnant women and children below the age of 5 years) sleeping under ITNs, 80% of children receiving appropriate malaria treatment with artemisinin-based combination therapy (ACTs) within 24 hours of onset of illness and 80% of pregnant women receiving two doses of Intermittent Preventive Treatment (IPTp) for malaria as part of antenatal care (ANC).
 Definitions have evolved since the Abuja Declaration. The target for ITNs was extended to all household members (thus universal). The ACT target was modified to require treatment based on parasitological testing (microscopy or rapid diagnostic tests). IPTp targets were extended to achieving monthly dosing from the 13th week of pregnancy, which depending on the point in pregnancy when a women entered the ANC system could be 3, 4 or more doses. In addition to these changes, the US President’s malaria Initiative upped the Abuja targets from 80% to 85% in the countries where it supported national malaria programs.
Definitions have evolved since the Abuja Declaration. The target for ITNs was extended to all household members (thus universal). The ACT target was modified to require treatment based on parasitological testing (microscopy or rapid diagnostic tests). IPTp targets were extended to achieving monthly dosing from the 13th week of pregnancy, which depending on the point in pregnancy when a women entered the ANC system could be 3, 4 or more doses. In addition to these changes, the US President’s malaria Initiative upped the Abuja targets from 80% to 85% in the countries where it supported national malaria programs.
We are eight years past 2010. It had been assumed that if scale up to 80% had been achieved by then and sustained for five or more years, malaria deaths would come close to zero and elimination of the disease would be in sight. National surveys have shown that reaching these targets has not been simple.
 The example of ITNs is a good place to start, as is Nigeria with the highest burden of malaria. The attached chart shows findings from the Demographic and Health or Malaria Information Surveys in 2010, 2013 and 2015. Whether one measures universal coverage by the house possessing at least one net per two residents or by the proportion who actually use/sleep under the nets, we can see that UHC for this intervention is difficult to achieve. Even when households possess nets, not everyone sleeps under them either because of adequacy of nets, preferred sleeping arrangements, internal household power structure or other factors.
The example of ITNs is a good place to start, as is Nigeria with the highest burden of malaria. The attached chart shows findings from the Demographic and Health or Malaria Information Surveys in 2010, 2013 and 2015. Whether one measures universal coverage by the house possessing at least one net per two residents or by the proportion who actually use/sleep under the nets, we can see that UHC for this intervention is difficult to achieve. Even when households possess nets, not everyone sleeps under them either because of adequacy of nets, preferred sleeping arrangements, internal household power structure or other factors.
In 2015 the majority of nets that existed in households were obtained through campaigns (77%), 14% were acquired from the health services, and 7% were purchased. These systems are not keeping up with the need.
 Four endemic countries reported a malaria Information Survey in 2016, Liberia, Ghana, Madagascar, and Sierra Leone. The chart shows that they too have had difficulty in achieving universal coverage of malaria interventions. Of note the chart only includes whether appropriate malaria parasitological diagnosis was done on children who had fever in the preceding two weeks. Data on provision of ACTs is based on fever, not test results, so there is no way to know whether it was appropriate. Generally 20-30% more febrile children received ACTs than were tested.
Four endemic countries reported a malaria Information Survey in 2016, Liberia, Ghana, Madagascar, and Sierra Leone. The chart shows that they too have had difficulty in achieving universal coverage of malaria interventions. Of note the chart only includes whether appropriate malaria parasitological diagnosis was done on children who had fever in the preceding two weeks. Data on provision of ACTs is based on fever, not test results, so there is no way to know whether it was appropriate. Generally 20-30% more febrile children received ACTs than were tested.
 All three malaria interventions, ACTs, Diagnostics and ITNs, require contact with the health system (including community health workers). If malaria services are indicative of other health interventions, then universal coverage including seeking interventions, getting them and ultimately using them is still a distant goal. To achieve universal coverage there also needs to be universal commitment by countries, donors and technical partners.
All three malaria interventions, ACTs, Diagnostics and ITNs, require contact with the health system (including community health workers). If malaria services are indicative of other health interventions, then universal coverage including seeking interventions, getting them and ultimately using them is still a distant goal. To achieve universal coverage there also needs to be universal commitment by countries, donors and technical partners.
CHW &Community &Equity &Health Workers &ITNs Bill Brieger | 12 Mar 2018
Malaria by the numbers: are the statistics real or are they a barrier to community involvement?
 George Mwinnyaa grew up in a small village in Ghana, West Africa. “I witnessed the death of several people including my siblings and my father. I became a health volunteer and later a community health worker.” George presented at the Johns Hopkins University TEDx event on 10 March 2018. Below are excerpts from that talk focused on his experiences in malaria interventions in Ghana and reflects on numbers found in public health interventions and questions what these numbers really mean to community members on the ground. George is currently an MHS student studying infectious disease epidemiology at the JHU Bloomberg School of Public Health.
George Mwinnyaa grew up in a small village in Ghana, West Africa. “I witnessed the death of several people including my siblings and my father. I became a health volunteer and later a community health worker.” George presented at the Johns Hopkins University TEDx event on 10 March 2018. Below are excerpts from that talk focused on his experiences in malaria interventions in Ghana and reflects on numbers found in public health interventions and questions what these numbers really mean to community members on the ground. George is currently an MHS student studying infectious disease epidemiology at the JHU Bloomberg School of Public Health.
——-
 I have always been very skeptical with numbers, particularly numbers that indicate program accomplishments from the developing world. Whenever I see numbers reporting a problem such as the mortality relating to malaria, Pneumonia, or diarrheal diseases- it puzzles me because these are all diseases that have received great attention, and there have been many interventions implemented. Yet these problems still exist, and the question is why?
I have always been very skeptical with numbers, particularly numbers that indicate program accomplishments from the developing world. Whenever I see numbers reporting a problem such as the mortality relating to malaria, Pneumonia, or diarrheal diseases- it puzzles me because these are all diseases that have received great attention, and there have been many interventions implemented. Yet these problems still exist, and the question is why?
Today malaria is still among the top causes of infant mortality in many African countries, including Ghana, yet we have mosquito nets, coils, sprays, long sleeved shirts that have been circulating in the country for years……and sometimes I wonder: why?
Total funding for malaria prevention and control was 2.7 billion dollars in 2016. Between 2014-2016, 582 million nets were distributed, of which 505 million were distributed in Africa, yet the number of malaria cases increased from 211 million in 2015 to 216 million in 2016 (WHO-malaria fact sheet, 2017).
I was once a supervisor for the distribution of long-lasting insecticide treated nets in rural communities. The numbers driven world saw big numbers that showed that many pregnant women were not sleeping under mosquito nets and so the solution to solve the malaria problem was to give them mosquito nets.
 First, they started out by selling the nets and people would not buy them, then they offered them free to pregnant women and that did not change anything, next they distributed to families in a household and that did not change anything, and finally they implemented what is known as the hanging of long lasting insecticide treated bed nets.
First, they started out by selling the nets and people would not buy them, then they offered them free to pregnant women and that did not change anything, next they distributed to families in a household and that did not change anything, and finally they implemented what is known as the hanging of long lasting insecticide treated bed nets.
This time we went into a house with a hammer, nails and ropes, and families showed us their bedroom and we hung the net for them. And yet malaria still rules. What happened with the free bed nets is now widely reported across different countries in Africa.
What do the numbers we measure mean to the people they represent?
 As an example, there was a man in a small fishing village with seven children. His biggest worry was how to get food for his family. So the world of numbers develops numbers-based interventions, numbers-driven solutions. Reporters found months after the family received the mosquito nets that no one in the family slept under the mosquito nets; instead the man had sown the nets together and used them for fishing to feed his family.
As an example, there was a man in a small fishing village with seven children. His biggest worry was how to get food for his family. So the world of numbers develops numbers-based interventions, numbers-driven solutions. Reporters found months after the family received the mosquito nets that no one in the family slept under the mosquito nets; instead the man had sown the nets together and used them for fishing to feed his family.
Frustrations abound on both ends of the system, for public health agents and community members. Numbers act as the barrier between the two ends of the “system”, and our goal must be to break the barrier. The numbers that drive interventions can be meaningless to the community people they represent unless we engage the community and learn how our interventions can really help them.
Case Management &Community &ITNs &Training Bill Brieger | 15 Nov 2017
Community Based Intervention in Malaria Training in Myanmar
 Nu Nu Khin of Jhpiego who is working on the US PMI “Defeat Malaria Project” led by URC shares observations on the workshop being held in Yangon with national and regional/state malaria program staff to plan how to strengthen malaria interventions at the community level. The workshop has adapted Jhpiego’s Community Directed Intervention training package to the local setting.
Nu Nu Khin of Jhpiego who is working on the US PMI “Defeat Malaria Project” led by URC shares observations on the workshop being held in Yangon with national and regional/state malaria program staff to plan how to strengthen malaria interventions at the community level. The workshop has adapted Jhpiego’s Community Directed Intervention training package to the local setting.
 Yesterday’s opening speech was being hailed as a significant milestone to give Community-Based Intervention (CBI) training teams the knowledge, skills, and attitudes they need to effectively provide quality malaria services and quality malaria information.
Yesterday’s opening speech was being hailed as a significant milestone to give Community-Based Intervention (CBI) training teams the knowledge, skills, and attitudes they need to effectively provide quality malaria services and quality malaria information.
 This core team is going to train the critical groups of community-level implementers including CBI focal persons and malaria volunteers at the community level.
This core team is going to train the critical groups of community-level implementers including CBI focal persons and malaria volunteers at the community level.
We embarked this important step yesterday with the collaboration of Johns Hopkins University, Myanmar Ministry of Health and Sports, and World Health Organization Myanmar.
 Participants will be developing action plans to apply the community approach to malaria efforts in townships and villages in three high transmission Rakhine State, Kayin State and Tanintharyi Region.
Participants will be developing action plans to apply the community approach to malaria efforts in townships and villages in three high transmission Rakhine State, Kayin State and Tanintharyi Region.
Economics &ITNs &Mosquitoes &Vector Control Bill Brieger | 25 Oct 2017
Mis-Use of Insecticide Treated Nets May Actually Be Rational
People have sometimes question whether insecticide treated nets (ITNs) provided for free are valued by the recipients. Although this is not usually a specific question in surveys, researchers found in a review of 14 national household surveys that free nets received through a campaign were six times more likely to be given away than nets obtained through other avenues such as routine health care or purchased from shops.
 Giving nets away to other potential users, not hanging nets or not sleeping under nets at least imply that the nets could potentially be used for their intended purpose. What concerns many is that nets may be used for unintended and inappropriate reasons. Often the evidence is anecdotal, but photos from Nigeria and Burkina Faso shown here document cases where nets were found to cover kiosks, make football goalposts, protect vegetable seedlings and fence in livestock.
Giving nets away to other potential users, not hanging nets or not sleeping under nets at least imply that the nets could potentially be used for their intended purpose. What concerns many is that nets may be used for unintended and inappropriate reasons. Often the evidence is anecdotal, but photos from Nigeria and Burkina Faso shown here document cases where nets were found to cover kiosks, make football goalposts, protect vegetable seedlings and fence in livestock.
Newspapers tend to quote horrified health or academic staff when reporting this, such as this statement from Mozambique, “The nets go straight out of the bag into the sea.” The Times said that net misuse squandered money and lives when they observed that “Malaria nets distributed by the Global Fund have ended up being used for fishing, protecting livestock and to make wedding dresses.”
 Two years ago the New York Times reported that, “Across Africa, from the mud flats of Nigeria to the coral reefs off Mozambique, mosquito-net fishing is a growing problem, an unintended consequence of one of the biggest and most celebrated public health campaigns in recent years.”5 Not only were people not being protected from malaria, but the pesticide in these ‘fishing nets’ was causing environmental damage. The article explains that the problem of such misuse may be small, but that survey respondents are very unlikely to admit to alternative uses to interviewers.
Two years ago the New York Times reported that, “Across Africa, from the mud flats of Nigeria to the coral reefs off Mozambique, mosquito-net fishing is a growing problem, an unintended consequence of one of the biggest and most celebrated public health campaigns in recent years.”5 Not only were people not being protected from malaria, but the pesticide in these ‘fishing nets’ was causing environmental damage. The article explains that the problem of such misuse may be small, but that survey respondents are very unlikely to admit to alternative uses to interviewers.
Similarly El Pais website featured an article on malaria in Angola this year with a striking lead photo of children fishing in the marshes near their village in Cubal with a LLIN. A video from the New York Times frames this problem in a stark choice: sleep under the nets to prevent malaria or them it to catch fish and prevent starvation.[v]
 More recently, researchers who examined net use data from Kenya and Vanuatu found that alternative LLIN use is likely to emerge in impoverished populations where these practices had economic benefits like alternative ITN uses sewing bednets together to create larger fishing nets, drying fish on nets spread along the beach, seedling crop protection, and granary protection. The authors raise the question whether such uses are in fact rational from the perspective of poor people.
More recently, researchers who examined net use data from Kenya and Vanuatu found that alternative LLIN use is likely to emerge in impoverished populations where these practices had economic benefits like alternative ITN uses sewing bednets together to create larger fishing nets, drying fish on nets spread along the beach, seedling crop protection, and granary protection. The authors raise the question whether such uses are in fact rational from the perspective of poor people.
An important fact is that not all ovserved ‘mis-use’ of nets is really inappropriate use. A qualitative study in the Kilifi area of coastal Kenya demonstrated local ‘recycling’ of old ineffective nets. The researchers clearly found that in rural, peri-urban and urban settings people adopted innovative and beneficial ways of re-using old, expired nets, and those that were damaged beyond repair. Fencing for livestock, seedlings and crops were the most common uses in this predominantly agricultural area. Other domestic uses were well/water container covers, window screens, and braiding into rope that could be used for making chairs, beds and clotheslines. Recreational uses such as making footballs, football goals and children’s swings were reported
What we have learned here is that we should not jump to conclusions when we observe a LLIN that is set up for another purpose than protecting people from mosquito bites. Alternative uses of newly acquired nets do occur and may seem economically rational to poor communities. At the same time we must ensure that mass campaigns pay more attention to community involvement, culturally appropriate health education and onsite follow-up, especially the involvement of community health workers. Until such time as feasible safe disposal of ‘retired’ nets can be established, it would be good to work with communities to help them repurpose those nets that no longer can protect people from malaria.
IPTp &ITNs &Malaria in Pregnancy &Treatment Bill Brieger | 10 Jul 2017
Liberia’s Fight against Malaria Continues
Liberia was making steady progress against malaria in the years after the civil war. Despite the devastation of Ebola, the health authorities have continued to push against malaria. The DHS Program has released key findings from the 2016 Malaria Information Survey. We have compared those against the 2011 MIS, and while there is progress, much work needs to be done in this highly endemic area – not just in fighting malaria, but in rebuilding health systems damaged by war and Ebola.
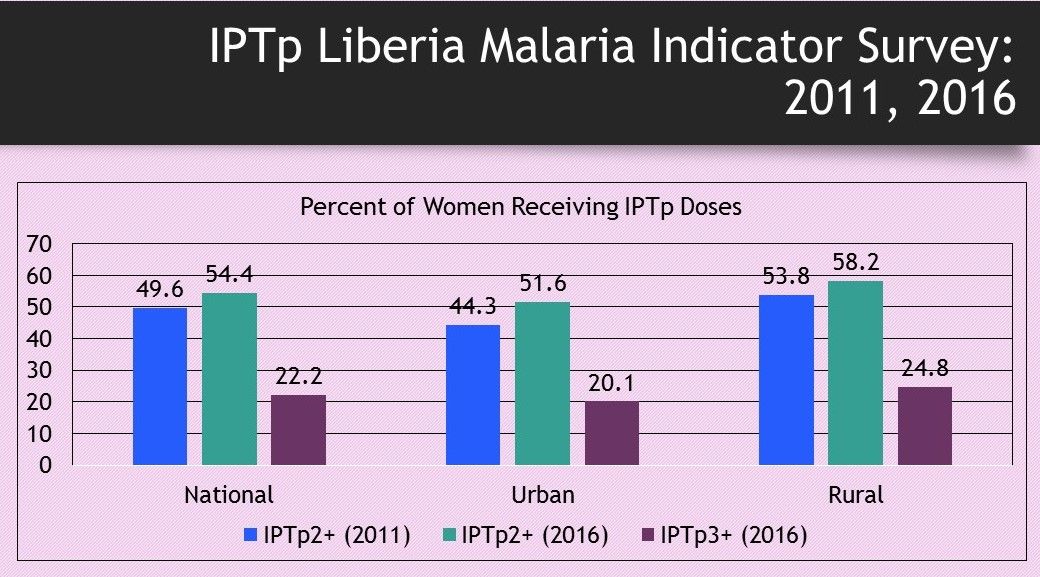 Targets for Intermittent Preventive Treatment in pregnancy of malaria have risen from at least 2 doses in 2011 to three or more when the 2016 data were collected. While the IPTp2+ doses have increased by a little less than 5%, the challenge of IPTp3 and greater has become quite evident. It is interesting that coverage of IPTp is slightly better in rural areas, but there is still a long way to go to protect pregnant Liberian women.
Targets for Intermittent Preventive Treatment in pregnancy of malaria have risen from at least 2 doses in 2011 to three or more when the 2016 data were collected. While the IPTp2+ doses have increased by a little less than 5%, the challenge of IPTp3 and greater has become quite evident. It is interesting that coverage of IPTp is slightly better in rural areas, but there is still a long way to go to protect pregnant Liberian women.
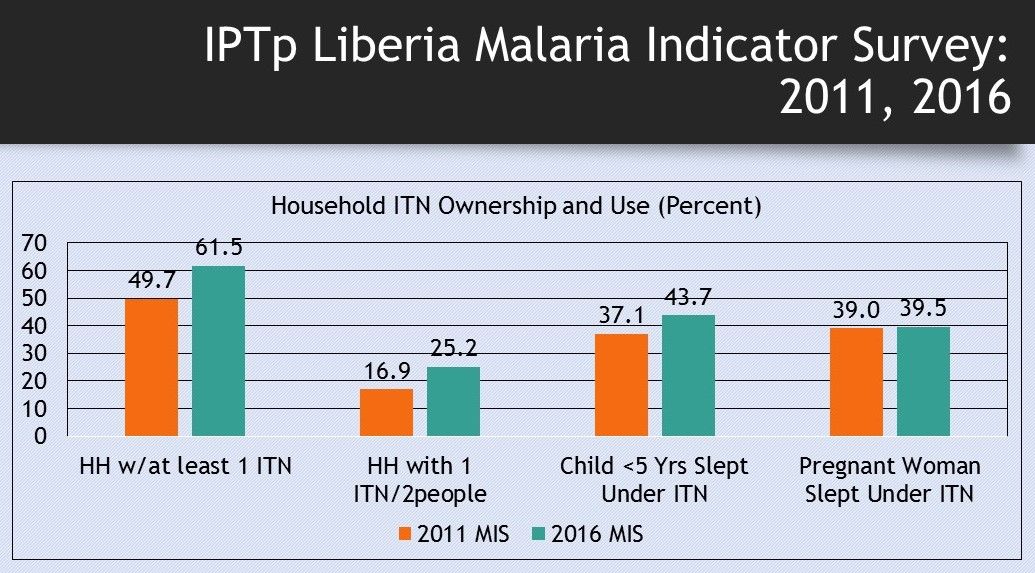 The situation with access to and use of insecticide treated nets has also improved over the 5-year period, but still remains well below the targets of universal coverage. Even though nearly two-thirds of households have at least one ITN, only a quarter have enough nets to reach the goal of one net for every two people. Net use by children below the age of 5 years is better than that of pregnant women, though in both cases less that half of these vulnerable populations are covered. Nets are particularly important for pregnant women who cannot take IPTp in the first trimester.
The situation with access to and use of insecticide treated nets has also improved over the 5-year period, but still remains well below the targets of universal coverage. Even though nearly two-thirds of households have at least one ITN, only a quarter have enough nets to reach the goal of one net for every two people. Net use by children below the age of 5 years is better than that of pregnant women, though in both cases less that half of these vulnerable populations are covered. Nets are particularly important for pregnant women who cannot take IPTp in the first trimester.
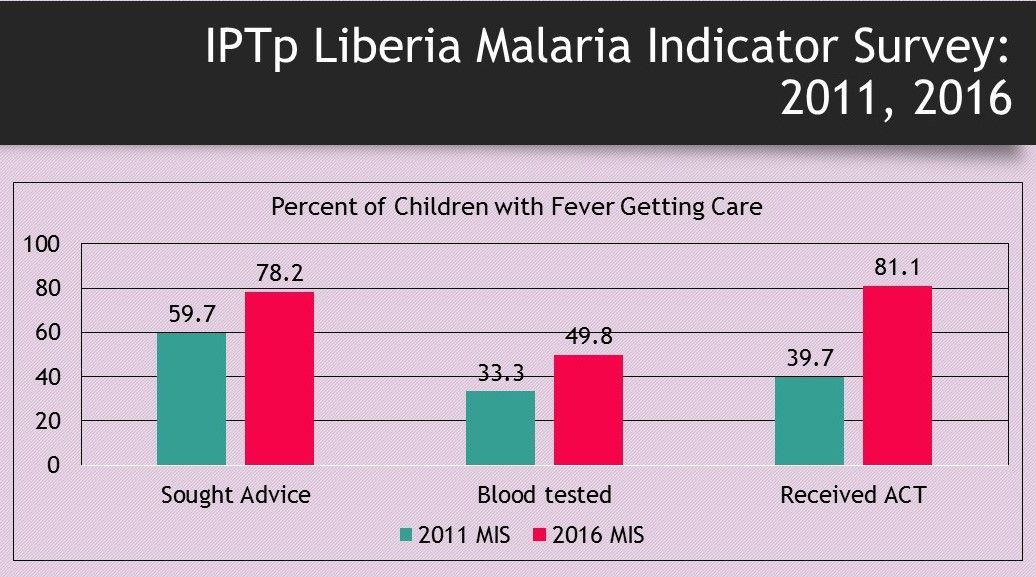 Care for febrile children also has improved, but questions remain about appropriate care due to the nature of the questioning processes in the MIS. Seeking advice increased by 20% as did getting blood tests (RDT or microscopy) once care is sought. Double the number of febrile children received artemisinin-based combination therapy in 2016 compared to 2011, but since the rate of testing is low, we do not know if they were being appropriately treated – given ACT only is tests were positive.
Care for febrile children also has improved, but questions remain about appropriate care due to the nature of the questioning processes in the MIS. Seeking advice increased by 20% as did getting blood tests (RDT or microscopy) once care is sought. Double the number of febrile children received artemisinin-based combination therapy in 2016 compared to 2011, but since the rate of testing is low, we do not know if they were being appropriately treated – given ACT only is tests were positive.
Liberia does receive support from donors such as the Global Fund and the US President’s Malaria Initiative. These and other partners need to strategize with the Liberian Ministry of Health and other local partners (NGOs, Businesses, etc.) in order to mobilize the support to put Liberia more squarely on the road to malaria elimination.
Epidemiology &IPTp &ITNs &Malaria in Pregnancy &Morbidity &Treatment Bill Brieger | 26 Jun 2017
Burundi: when will citizens see real protection from malaria?
Preliminary findings from Burundi’s 2015-16 DHS have been made available. The country has a long way to go to meet targets for basic control of malaria.
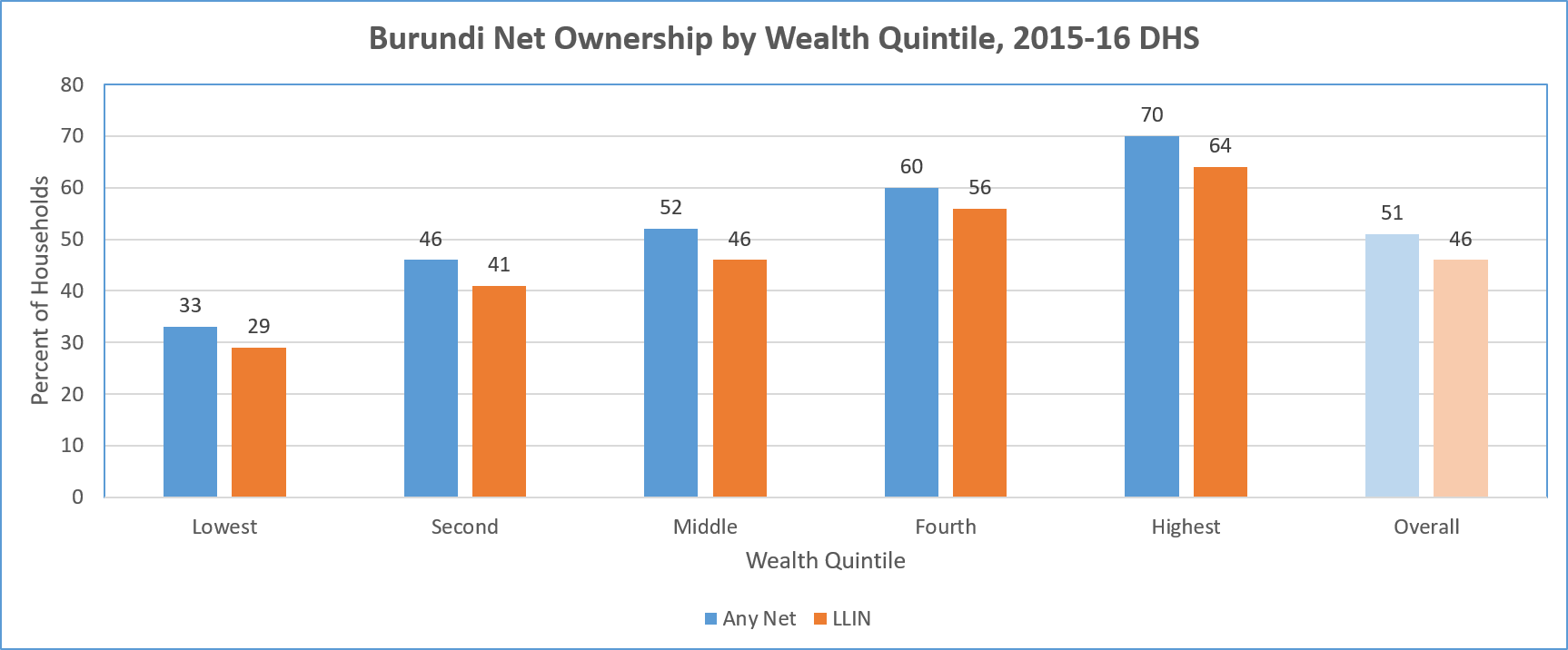 LLIN availability by household is an overall disappointing 32%. Ironically there is greater coverage of households in in urban areas (50%) than rural (30%). There is also great variation among the provinces with 52% coverage in Bujumbura metropolitan but only 19% in Canzuko. The overall average is less than one treated net per household.
LLIN availability by household is an overall disappointing 32%. Ironically there is greater coverage of households in in urban areas (50%) than rural (30%). There is also great variation among the provinces with 52% coverage in Bujumbura metropolitan but only 19% in Canzuko. The overall average is less than one treated net per household.
A major concern is equity. The chart above shows a steep gradation from 19% coverage among the lowest fifth of the wealth quintile, up to 48% in the highest. Even in households that have at least one net, only 17% of of people slept under a net the night before the survey.
In terms of use by those traditionally defined as vulnerable, the DHS shows only 40% of children below 5 years of age overall slept under a treated net the night prior to the survey. Even in households that own at least one net, 78% of these children slept under one.
A similar pattern is seen for treated net use by pregnant women. Overall 44% slept under a treated net, and 84% did so in households that owned at least one treated net. The internal household dynamics of net use where one is available does appear to favor these two groups.
Overall coverage of Intermittent Preventive Treatment for pregnant women is very low. Less than 30% of pregnant women received even the first dose of SP. This decreased to 21% for two doses and 13% for three. In contrast to net coverage, more rural women (31%) received the first dose of IPTp than urban ones (19%).
 Nearly 40% of children below five years of age were found to have had a fever in the two weeks preceding the survey. Among those care was sought for only two-thirds. Eleven percent of those with fever received an artemisinin-based combination therapy drug. The report did not mention whether these children had received any testing prior to treatment, so appropriateness of treatment cannot be judged. Prevalence testing of the children in the sample found 38% with parasitemia. Therefore one might assume that more children should have received ACTs.
Nearly 40% of children below five years of age were found to have had a fever in the two weeks preceding the survey. Among those care was sought for only two-thirds. Eleven percent of those with fever received an artemisinin-based combination therapy drug. The report did not mention whether these children had received any testing prior to treatment, so appropriateness of treatment cannot be judged. Prevalence testing of the children in the sample found 38% with parasitemia. Therefore one might assume that more children should have received ACTs.
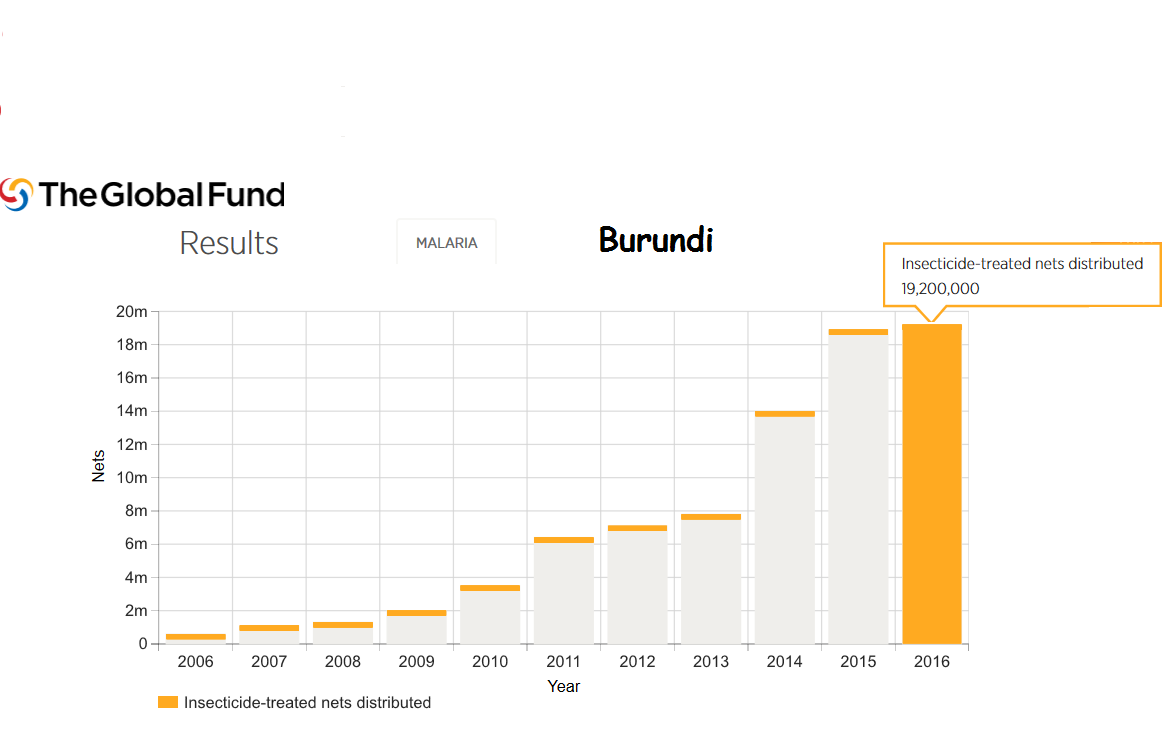
Burundi still faces major political and social challenges. Even so Burundi is the recipient of malaria support from the Global Fund. For example 18 million LLINs were distributed in 2015 and 19 million in 2016.
Much work is needed to bring Burundi even close to universal coverage of malaria interventions. In today’s climate of questionable donor commitment, it is hoped that regional partners may play a role since malaria knows no boundaries.
Elimination &Epidemiology &Funding &IPTp &ITNs &Procurement Supply Management &Treatment Bill Brieger | 20 May 2017
Ghana – spotlight on malaria indicators
 The Demographic and Health Surveys has released a brief on key indicators from the Ghana Malaria Indicator Survey of 2016. While much of the malaria community is discussing the elimination framework and processes, the reality is that many high burden countries are still trying to scale up basic interventions to achieve universal coverage.
The Demographic and Health Surveys has released a brief on key indicators from the Ghana Malaria Indicator Survey of 2016. While much of the malaria community is discussing the elimination framework and processes, the reality is that many high burden countries are still trying to scale up basic interventions to achieve universal coverage.
The overall prevalence across the country in children aged 6-59 months at the time of the survey was 27% using Rapid Diagnostic test and 20% using microscopy. Among children reporting fever in the previous two weeks care/advice was sought for only 72%. Although only only 30% received some sort of blood based diagnostic test, 61% of the febrile children were given the antimalarial artemisinin-based combination therapy drugs.
 Children are still being treated without the benefit of parasitological testing, a key procedure highlighted in WHO case management guidelines. Presumptive treatment for malaria without testing means that a child could inappropriately receive antimalarial drugs and die of another underlying febrile illness. Appropriate testing and adherence to test results is one of the main areas of focus of Ghana’s grants from the US President’s Malaria Initiative. Improved testing is also an important element in Ghana’s current Global Fund support. Clearly more value for money is needed from these inputs.
Children are still being treated without the benefit of parasitological testing, a key procedure highlighted in WHO case management guidelines. Presumptive treatment for malaria without testing means that a child could inappropriately receive antimalarial drugs and die of another underlying febrile illness. Appropriate testing and adherence to test results is one of the main areas of focus of Ghana’s grants from the US President’s Malaria Initiative. Improved testing is also an important element in Ghana’s current Global Fund support. Clearly more value for money is needed from these inputs.
Preventive measures as documented in the MIS fare somewhat better., but at present only 73% of households own an insecticide treated bednet. When considering the recommended 1 net for every 2 household members, the indicator drops to 50%. Concerning the typical ‘vulnerable’ populations, we see that only 52% of children below the age of 5 years slept under an ITN the night before the survey; only 50% of pregnant women did likewise.
 Malaria prevention in pregnancy results reflect the fact that Ghana has promoted at least three IPTp doses for around ten years. Most pregnant women (78% ) had received the previously recommended minimum of two doses, and now 60% have received at least three doses.
Malaria prevention in pregnancy results reflect the fact that Ghana has promoted at least three IPTp doses for around ten years. Most pregnant women (78% ) had received the previously recommended minimum of two doses, and now 60% have received at least three doses.
One of the important issues stressed in WHO’s new malaria elimination framework is stratifying the country by prevalence to the lowest level possible in order to plan appropriate interventions. Fortunately the Ghana 217 MIS key indicator brief does stratify prevalence and intervention coverage by region. Prevalence through RDT testing ranges from nearly 5% in the urbanized greater Accra area to 44% in the Central Region. Interestingly ITN use is nearly 20% higher in Central than greater Accra.
Hopefully future planning in Ghana will build on this stratification. Better mobilization of donor, national and private sector resources will address likely issues of stock-outs and increase the likelihood of universal coverage of basic interventions that is needed to move the country along the road to malaria elimination.
ITNs Bill Brieger | 29 Apr 2017
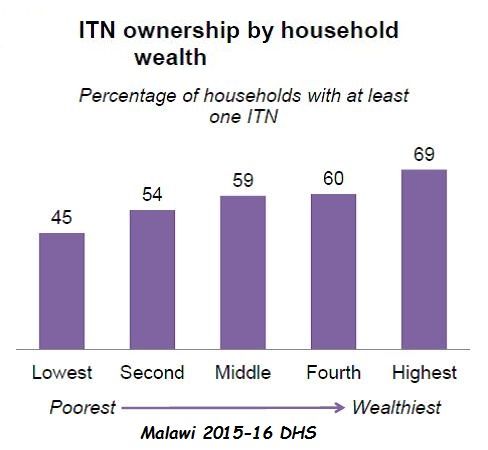
Insecticide Treated Nets in Malawi: Lessons from the 2015-16 Demographic and Health Survey
In 2000 the Abuja Declaration set a target of 80% coverage for people in endemic countries owning AND sleeping under nets by the year 2010. The United Nations came along in 2009 and upped the ante making the target “Universal Coverage.” Such targets were assumed to help countries meet the 2015 Millennium Development Goals for reducing malaria morbidity and mortality. So what happens when these dates pass and countries still have neither achieved nor maintained ITN coverage?
 An example of the remaining challenges can be seen in the 2015-16 malaria section of the Malawi Demographic and Health Survey. The MDHS notes that while household ownership of nets increased from 27% in 2004 to 57% in 2010, it did not change between 2010 and 2015-16. This is despite efforts by the Ministry of health, The US President’s Malaria Initiative and the Global Fund, not to mention peer pressure from the members of the Southern African Development Community who are pushing a malaria elimination agenda.
An example of the remaining challenges can be seen in the 2015-16 malaria section of the Malawi Demographic and Health Survey. The MDHS notes that while household ownership of nets increased from 27% in 2004 to 57% in 2010, it did not change between 2010 and 2015-16. This is despite efforts by the Ministry of health, The US President’s Malaria Initiative and the Global Fund, not to mention peer pressure from the members of the Southern African Development Community who are pushing a malaria elimination agenda.
Even though the actual availability of nets in the households did not increase recently, use or those available improved slightly. The MDHS explains that, “The ITN use among children under age 5 has increased over the years, from 15% in 2004 to 39% in 2010, and 43% in 2015-16. Among pregnant women, ITN use increased from 15% in 2004 to 35% in 2010, and 44% in 2015-16.” This shows some improvement in health education activities, but people cannot use the net that is not available.
Where do the nets come from? Among the nets found in surveyed households newly a third (32%) were acquired through a mass distribution campaign. Nearly half (47%) were acquired through a routine clinic visit such as antenatal care, child birth, immunization clinic and other clinic visits. The remainder were bought from shops or other places. This shows a good mix of distribution strategies. It is therefore, the volume of nets made available that is of concern, possibly more than the process, but further analysis by the national malaria program should examine all of these avenues to ensure efficiency.
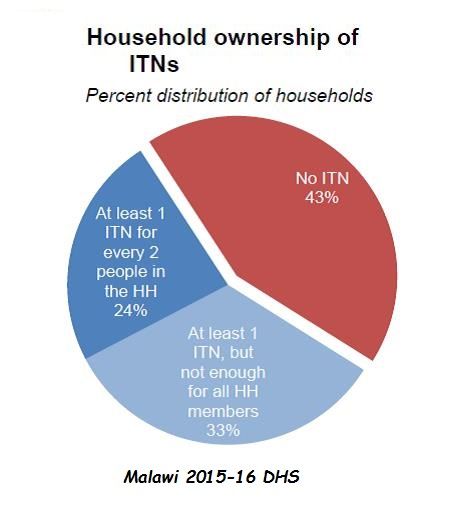
 An irony appears in the pie chart on net availability in households. While 43% did not have any nets, another 33% did not have enough nets to meet coverage targets of one net per two people. This again poses serious access issues. Thus, it is not surprising that 13% of people who in theory have access to nets did not sleep under them.
An irony appears in the pie chart on net availability in households. While 43% did not have any nets, another 33% did not have enough nets to meet coverage targets of one net per two people. This again poses serious access issues. Thus, it is not surprising that 13% of people who in theory have access to nets did not sleep under them.
Several other challenges were documented. Only 45% of the poorest segment of the population lived in households with nets, compared to 69% of the wealthiest. Similarly rural populations were less likely to sleep under ITNs (32%) than urban (42%). It would appear that more attention to equity in ITN programs is needed. Interestingly, urban households are more likely to purchase their nets from shops and markets than rural dwellers.
Good news is that the US President’s Malaria Initiative plans to help maintain coverage of pregnant women and children in the coming year through the procurement and distribution of ITNs through routine service channels with 1.2 million ITNs. In addition the Global Fund reports that over 7.7 million ITNs were distributed in Malawi in 2016 with it’s support. Maybe these efforts will reflect in the next iteration of the DHS or MIS, but fluctuations in ITN availability do impact on disease transmission, and concerns about equity will remain.
The DHS and its sister survey, the Malaria Information Surveys are crucial tools for identifying challenges and planning ways to improve coverage of malaria interventions. Hopefully Malawi will be able to use this information to save lives.
Community &ITNs &Urban Bill Brieger | 19 Apr 2017
Challenges and Recommendations in Distribution of LLINs in Urban Contexts
by Brooke Farrenkopf

With the malaria team made up of public health nurses and an infectious disease specialist in Kumasi
I participated in a study on urban distribution of long lasting insecticide treated bednets (LLINs) as part of the USAID/PMI VectorWorks Project of the Johns Hopkins University Center for Communication Programs aided by a JHU Global Health Field Placement Scholarship. I conducted qualitative interviews to support a programmatic study on the challenges associated with mass distributions in urban contexts and helped develop report recommendations for developing the guidelines for future campaigns in urban areas. I am sharing my findings here.
As noted VectorWorks is funded by the US President’s Malaria Initiative and works to improve access to long-lasting insecticide treated nets (LLINs) in 12 countries in Asia and Africa. VectorWorks Ghana, through collaboration with the National Malaria Control Program (NMCP) and partners, supports the following distribution campaigns:
- School-based distribution, occurring every May for grades 2 and 6
- Continuous facility-based distribution at ANC and EPI visits
- Point mass distribution campaigns, occurring every 3 years
 In Kumasi, Takoradi, and Tamale, a point mass distribution campaign had already occurred. The campaign in Accra occurred while I was in Ghana, and I was able to visit the distribution sites and the health facilities where a portion of the LLINs were stored. Here, I was able to see some of the logistical challenges associated with the urban context.
In Kumasi, Takoradi, and Tamale, a point mass distribution campaign had already occurred. The campaign in Accra occurred while I was in Ghana, and I was able to visit the distribution sites and the health facilities where a portion of the LLINs were stored. Here, I was able to see some of the logistical challenges associated with the urban context.
I was also able to see the solutions put in place by the local malaria teams. One solution to improve program delivery was the development of a coupon coding system. As each community member attended the distribution site to receive a LLIN, Ghana Health Service (GHS) staff had to match their registration coupon with the coded coupon in the book. The coding system organized the coupons and identified members who had not attended distribution.
Mass distribution campaigns are the most effective method to rapidly increase long-lasting insecticidal net (LLIN) coverage. Mass distribution in urban areas with characteristically large and heterogeneous populations of high population density comes with higher costs and difficult logistics. Many inhabitants are not indigenous to the area and are of varied religious, occupational, and socioeconomic backgrounds. Urban areas commonly have large mobile working class populations that are difficult to access. These characteristics are unique to urban areas and introduces the need for improved guidelines in urban areas.

VectorWorks Ghana Team
To date, the National malaria Control Program (NMCP) guidelines for point mass distribution in Ghana have made no distinction between urban and rural areas and have therefore not addressed these differences. This study intended to provide information to refine these guidelines.
Most interviews were conducted in hospitals and health facilities where the members of the malaria teams were located. The interviews were conducted in-person in the four largest metropolitan areas in Ghana: Kumasi, Greater Accra, Takoradi, and Tamale. I helped develop and follow a question guide that covered each phase of the distribution focusing on the challenges, solutions, and recommendations associated with each phase of distribution.
Most common challenges with implementation in urban communities:
- Reaching community members during registration
- Completing registration within the period of days provided and the volunteers allocated, because the population was too dense to reach all of the households and many community members were not at home during registration
- Beneficiary dissatisfaction with universal health coverage definition of sufficient LLIN coverage {one net per two people in each household}
Most common recommendations for future distributions:
- Greater inclusion of sub-metro teams in development of the micro plan
- Increase the resources to recruit and remunerate more volunteers and supervisors to enable more distribution sites, help control crowds, and allow fewer days for each phase
- Intensify social mobilization and allow sub-metros to help develop this plan to utilize local resources, especially to improve understanding of universal health coverage definition of one net per two people and to inform about logistics
- Increase the number of registration days
- Conduct a utilization study to understand coverage of LLIN use and barriers to consistent use.
I was able to speak with public health nurses, malaria experts, and district health directors, and hear their insight on how to improve future campaigns. My favorite anecdotes included examples of how teams developed innovative solutions to improve campaign efficiency or strategically access hard to reach populations.
The observations and recommendations by the respondents themselves should guide future LLIN campaigns in urban settings in Ghana.
References
- VectorWorks (2017) Johns Hopkins center for Communication Programs. http://ccp.jhu.edu/projects/malaria-vector-control/
- de Beyl CZ, Koenker H, Acosta A, Onyefunafoa EO, Adegbe E, McCartney-Melstad A, Killian A (2016) Multi-country comparison of delivery strategues for mass campaigns to achieve universal coverage with insecticide-treated nets: what works best? Malaria Journal, 15(1): 1.
- Stakeholder Review of Experiences in urban Long-Lasting Insecticidal Net (LLIN) campaign distributions (2012). Malaria Consortium Africa.