Capacity Building &Case Management &Funding &Health Systems &IPTp &ITNs &Leadership Bill Brieger | 09 Feb 2019
Guinea: The Challenge of Malaria Control in a Post-Ebola Context
The preliminary 2018 Demographic and Health Survey (DHS) data have been released for Guinea (Conakry). Since the last DHS in 2012, Guinea and its neighbors experienced the largest Ebola outbreak in history, an event that damaged already weak health systems.
 The previous DHS showed very weak malaria indicators. Only 47% of households had at least one ITN, which averages to 0.8 ITNs per person (compared to the universal coverage of 2.0). Among vulnerable groups only 26% of children below the age of 5 years slept under an ITN, as did 28% of pregnant women. Very few, 18%, pregnant women got two doses of IPTp, and only 5% of febrile children received ACTs (testing was not reported then).
The previous DHS showed very weak malaria indicators. Only 47% of households had at least one ITN, which averages to 0.8 ITNs per person (compared to the universal coverage of 2.0). Among vulnerable groups only 26% of children below the age of 5 years slept under an ITN, as did 28% of pregnant women. Very few, 18%, pregnant women got two doses of IPTp, and only 5% of febrile children received ACTs (testing was not reported then).
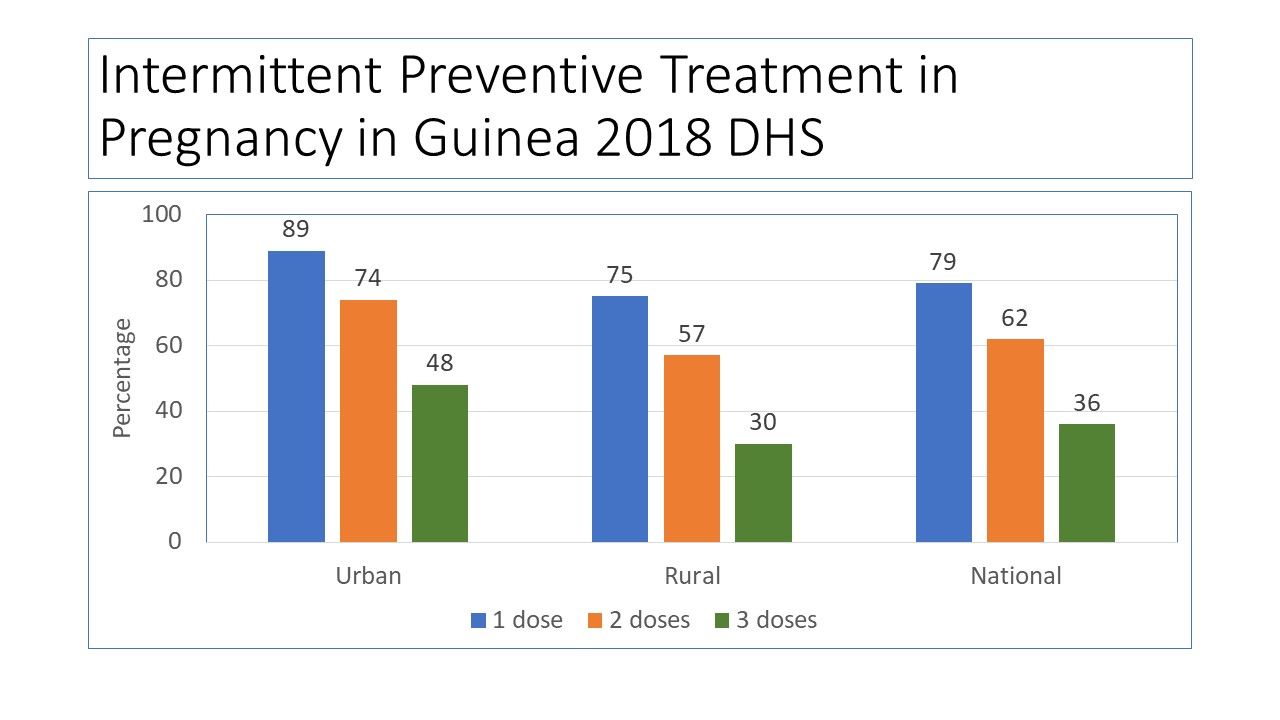
 Not much has changed concerning ITN coverage as reported in 2018. Slight improvements are seen in IPTp (which now requires 3 or more doses) and malaria testing and treatment for children. Ironically none of the indicators has passed the original 2006 Roll Back Malaria target of 60%, let alone 80% for 2010 and not of course the drive for universal coverage.
Not much has changed concerning ITN coverage as reported in 2018. Slight improvements are seen in IPTp (which now requires 3 or more doses) and malaria testing and treatment for children. Ironically none of the indicators has passed the original 2006 Roll Back Malaria target of 60%, let alone 80% for 2010 and not of course the drive for universal coverage.
 DHS has released a preliminary report for 2018 and the malaria component is summarized in the charts posted here. The national coverage for ITNs is 44%, slightly lower than 2012, but the average per household member is slightly higher at 1.1. Again, these numbers do not mark significant progress. Looking at wealth and ITN ownership there is a slight benefit in terms of equity in net possession among those with lower income, but this must be seen in the overall context of very low basic coverage.
DHS has released a preliminary report for 2018 and the malaria component is summarized in the charts posted here. The national coverage for ITNs is 44%, slightly lower than 2012, but the average per household member is slightly higher at 1.1. Again, these numbers do not mark significant progress. Looking at wealth and ITN ownership there is a slight benefit in terms of equity in net possession among those with lower income, but this must be seen in the overall context of very low basic coverage.
 Having a net in the household and using it are different challenges as seen in the reports of sleeping under the net on the night prior to the survey among children under 5 years of age and pregnant women. The sad finding is that even in households that own a net, the coverage of these two groups remains very low. This is reflected in the low net per person ratio nationally (1.1).
Having a net in the household and using it are different challenges as seen in the reports of sleeping under the net on the night prior to the survey among children under 5 years of age and pregnant women. The sad finding is that even in households that own a net, the coverage of these two groups remains very low. This is reflected in the low net per person ratio nationally (1.1).
 One would almost wonder if malaria is a neglected disease in Guinea. The reality is that since 2003, Guinea has received around $172 million US dollars in malaria project funding from the Global Fund. Its most recent annual funding from the US President’s Malaria Initiative (PMI) is around $14 million. Of that PMI funding 24% was designated for nets and related activities, while 52% was to be spent on medicines, diagnostics and pharmaceutical management. These investments include systems strengthening and capacity building in addition to commodities.
One would almost wonder if malaria is a neglected disease in Guinea. The reality is that since 2003, Guinea has received around $172 million US dollars in malaria project funding from the Global Fund. Its most recent annual funding from the US President’s Malaria Initiative (PMI) is around $14 million. Of that PMI funding 24% was designated for nets and related activities, while 52% was to be spent on medicines, diagnostics and pharmaceutical management. These investments include systems strengthening and capacity building in addition to commodities.
PMI provides the needed context: “Since the country was declared Ebola-free in in June of 2016, Guinea continues to make positive advances towards building a strong health system in line with the health recovery plan. The government continues to mobilize internal and external resources for rolling out the health system recovery plan, but much remains to be done if this plan is to yield the intended results.” Areas in particular need of strengthening within the National Malaria Control Program include coordination, health information systems, leadership, supervision and logistics.
Three years have passed since the last Ebola case in Guinea. Hopefully the country can stave off another outbreak and at the same time strengthen its health system. Guinea may not yet be targeted for malaria elimination, but until systems are strengthened, the resources going into malaria control will not be able to push malaria indicators toward saving more lives.
Burden &Funding &Health Education &Health Systems &Invest in Malaria Control &ITNs &Management Bill Brieger | 19 Nov 2018
Malaria funding may never be enough, but better program management should be possible
 The World Malaria Report shows that malaria cases are up, and even though there are fewer reported cases in 2017 than 2010, the number is greater than 2016. So once again high burden countries are being targeted. Today this focus is on “High Burden to High Impact”, but in 2012-13 it was the “Malaria Situation Room” that also focused on 10 high burden countries.
The World Malaria Report shows that malaria cases are up, and even though there are fewer reported cases in 2017 than 2010, the number is greater than 2016. So once again high burden countries are being targeted. Today this focus is on “High Burden to High Impact”, but in 2012-13 it was the “Malaria Situation Room” that also focused on 10 high burden countries.
Progress was being made up to around 2015-16, it then started to reverse. The challenge was not just funding. As the WHO Director General noted in the foreword to the 2018 World Malaria Report (WMR), “Importantly, ‘High burden to high impact’ calls for increased funding, with an emphasis on domestic funding for malaria, and better targeting of resources. The latter is especially pertinent because many people who could have benefited from malaria interventions missed out because of health system inefficiencies.”
 Over the years there have never been enough pledged funds to fully achieve targets, but as funding has never reached desired levels, attention is now being drawn more and more to the source of that funding (more emphasis on domestic/endemic countries) and especially how the health system functions to use the funds that are made available. In 1998 during one of the early meetings establishing the Roll Back Malaria Partnership, a speaker stressed that malaria control could not succeed without concomitant health systems strengthening and reform. That 20-year-old thought was prescient for today’s dilemma.
Over the years there have never been enough pledged funds to fully achieve targets, but as funding has never reached desired levels, attention is now being drawn more and more to the source of that funding (more emphasis on domestic/endemic countries) and especially how the health system functions to use the funds that are made available. In 1998 during one of the early meetings establishing the Roll Back Malaria Partnership, a speaker stressed that malaria control could not succeed without concomitant health systems strengthening and reform. That 20-year-old thought was prescient for today’s dilemma.
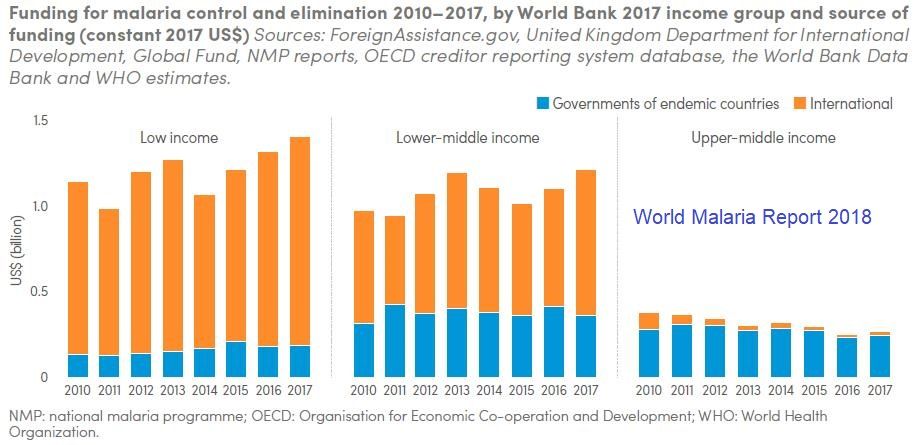
First, what is the funding situation? As outlined in the World Malaria Report …
- In 2017, an estimated US$ 3.1 billion was invested in malaria control and elimination efforts globally by governments of malaria endemic countries and international partners – an amount slighter higher than the figure reported for 2016.
- Governments of endemic countries contributed 28% of total funding (US$ 900 million) in 2017, a figure unchanged from 2016.
- Funding for malaria has remained relatively stable since 2010
- To reach the Global Technical Strategy 2030 targets, it is estimated that annual malaria funding will need to increase to at least US$ 6.6 billion per year by 2020
 The question remains – does investment lead to results. The WMR shows, for example, that “Between 2015 and 2017, a total of 624 million insecticide-treated mosquito nets (ITNs/LLINs), were reported by manufacturers as having been delivered globally. This represents a substantial increase over the previous period 2012–2014, when 465 million ITNs were delivered globally”.
The question remains – does investment lead to results. The WMR shows, for example, that “Between 2015 and 2017, a total of 624 million insecticide-treated mosquito nets (ITNs/LLINs), were reported by manufacturers as having been delivered globally. This represents a substantial increase over the previous period 2012–2014, when 465 million ITNs were delivered globally”.
At the same time the report states that, “Households with at least one ITN for every two people doubled to 40% between 2010 and 2017. However, this figure represents only a modest increase over the past 3 years, and remains far from the target of universal coverage.” Is it simply a matter of funding to reach the other 60% of households, or are there serious management problems on the ground?
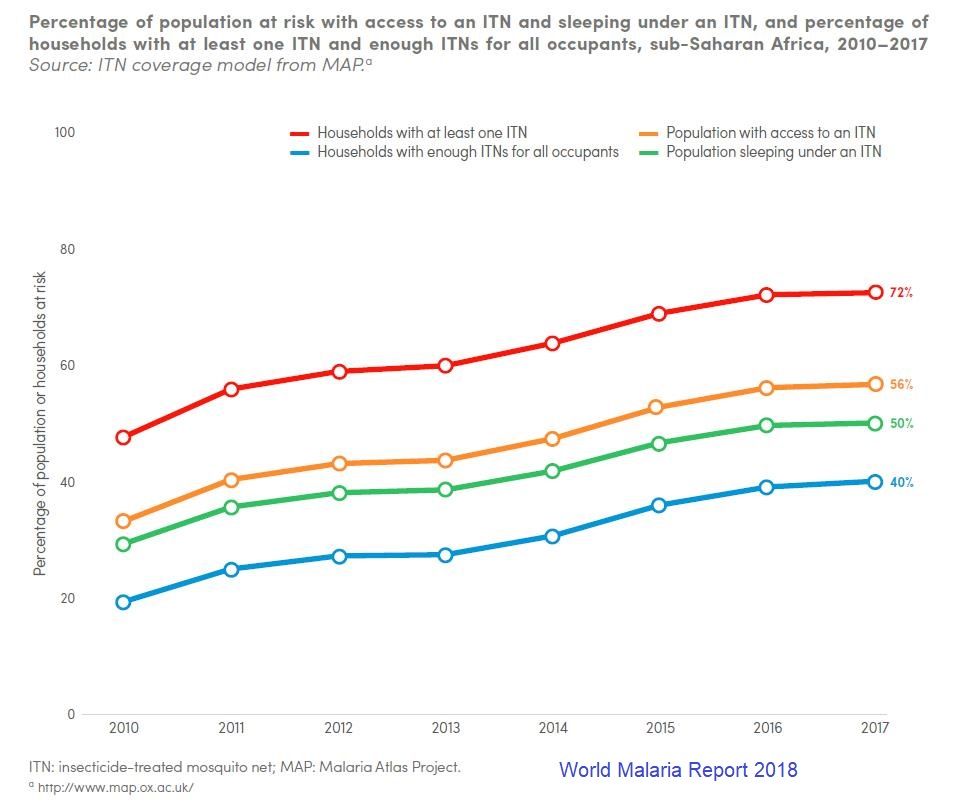 Then there is the issue of using nets. The WMR traces new ownership and use from 2010 to 2017, and we can see that overall the proportion of the population at risk who slept under a net increased from around 30% to 50%, but only 56% of those with access to a net were sleeping under them. This can be attributed in part but not completely to the adequacy of nets in a household.
Then there is the issue of using nets. The WMR traces new ownership and use from 2010 to 2017, and we can see that overall the proportion of the population at risk who slept under a net increased from around 30% to 50%, but only 56% of those with access to a net were sleeping under them. This can be attributed in part but not completely to the adequacy of nets in a household.
We should ask are enough nets getting to the right places, and also are efforts in place to promote their use. Behavior change efforts should be a major component of malaria program management. Even the so called biological challenges to malaria control have a human element. Monkey malaria transmission to people results from deforestation. Malaria parasite resistance to medicines comes from poor drug management on individual and systems levels.
The target year 2030 will be here before we know it. Will malaria still be here, or will countries and donors get serious about malaria financing AND program management?
Equity &IPTp &ITNs &Malaria in Pregnancy &Private Sector Bill Brieger | 18 Nov 2018
Tanzania: Slow Progress in Preventing Malaria
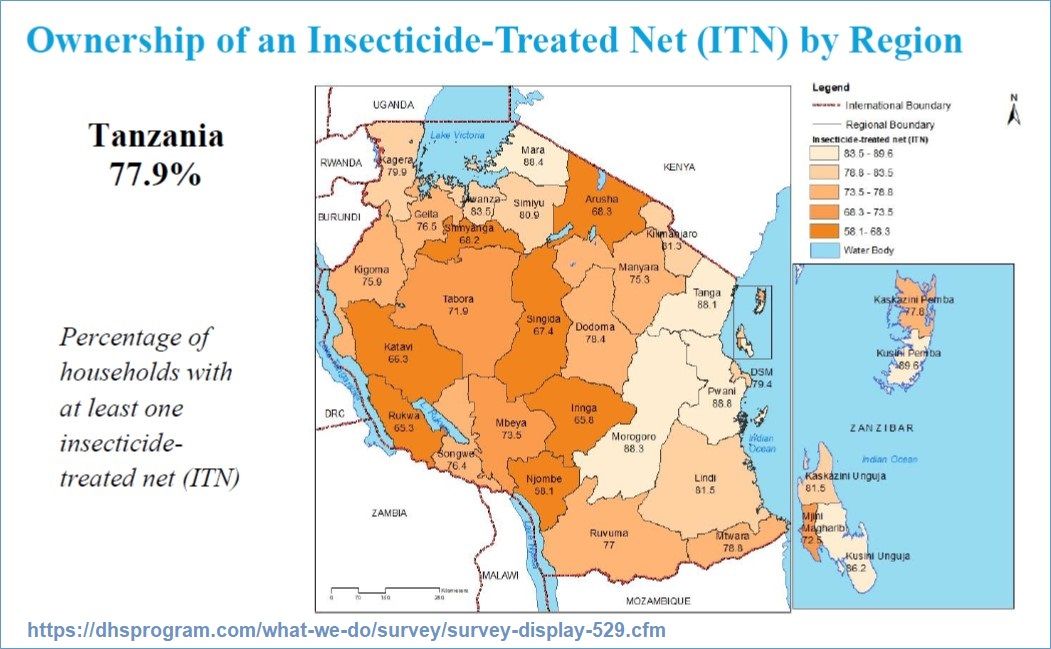
 The full 2017 Malaria Indicator Survey (MIS) results have been published for Tanzania providing an opportunity to look at the findings in more detail. Several important factors need highlighting since Tanzania is part of a regional block where some countries are activly considering malaria elimination – the E8 countries of the Southern Africa Development Community.
The full 2017 Malaria Indicator Survey (MIS) results have been published for Tanzania providing an opportunity to look at the findings in more detail. Several important factors need highlighting since Tanzania is part of a regional block where some countries are activly considering malaria elimination – the E8 countries of the Southern Africa Development Community.
So far Tanzania has come close to achieving a target of 80% of households owning insecticide treated nets (ITNs) with 78% on the mainland and 79% in Zanzibar. A closer look shows that there is still a ways to go to get to universal coverage or at least one net for every two persons in the household. With this indicator 45% of mainland and 42% of Zanzibar households have met the target, meaning that there are unprotected people in a majority of households across the country. This indicator experienced a drop from a 2011 “high” of 56%, a drop to 39% in 2015 and a slight recovery to 45% in 2017.
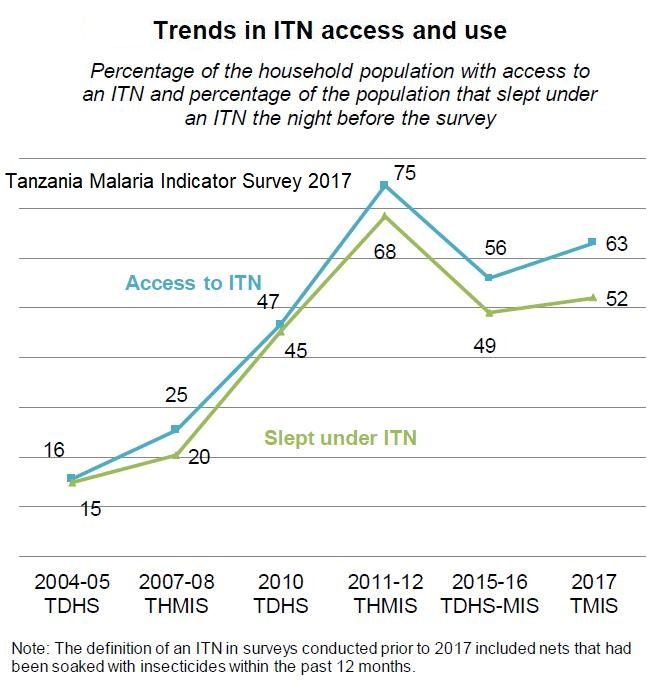
Even the universal coverage target requires that people actually sleep under the nets. What the MIS report shows is that although 63% of people had access to an ITN, only 52% reported sleeping under one the night before the survey.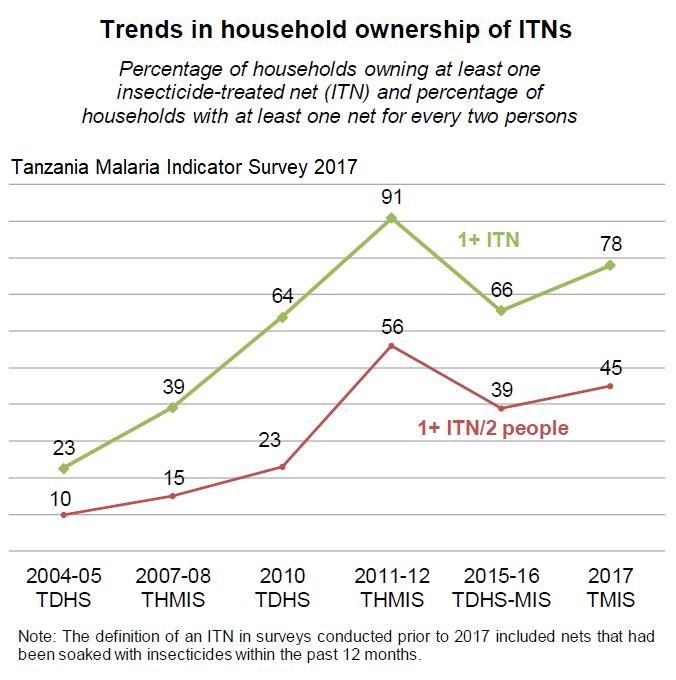
Equity remains an issue with 69% of households in the lowest wealth quintile owning at least one net compared to 81% and 83% in the middle and fourth quintiles. Although households in the highest quintile had 78% ownership, this group is more likely to live in better quality housing that prevents the ingress of most mosquitoes. Also residents in urban areas have an edge over rural counterparts in terms of net access.
 The report show that 55% of children under 5 years of age and 51% of pregnant women slept under an ITN. This is down from 72% and 75% respectively in 2011.
The report show that 55% of children under 5 years of age and 51% of pregnant women slept under an ITN. This is down from 72% and 75% respectively in 2011.
We learn that 90% of existing nets were obtained through some form of public sector campaign including mass distribution (62%), village coupons redeemable at health centers (15%), and school campaigns (4%). Only 5% were obtained through routine services (ANC, child immunization) 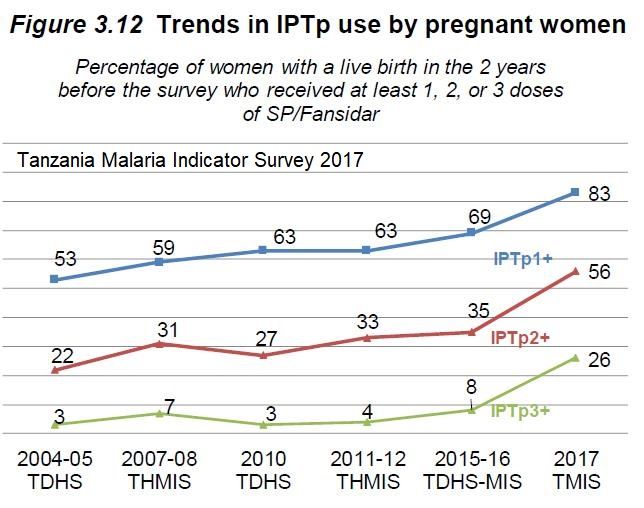 indicating that efforts to ‘keep up’ after mass campaigns need to be strengthened. The 10% of nets, whether treated or not, that were obtained in shops and markets cost the owner in the neighborhood of US$5.00.
indicating that efforts to ‘keep up’ after mass campaigns need to be strengthened. The 10% of nets, whether treated or not, that were obtained in shops and markets cost the owner in the neighborhood of US$5.00.
Uptake of doses of intermittent preventive treatment for malaria in pregnancy has slowly but steadily increased over the past 15 years and stood at 83% for one dose, 56% for two doses and 26% for three in this most recent MIS. With the current target being three or more doses needed for optimal protection, Tanzania still has a far long way to go, especially considering that accessing ITNs through ANC services is also low..
Case Management &Elimination &Epidemiology &Health Information &ITNs &Migration &Surveillance Bill Brieger | 20 Jul 2018
Establishing Mobile Outreach Teams (MOTs) for strengthening Active Case Detection with Mobile Populations in Vietnam 2016-2020
 Mobile migrant populations present a special challenge for malaria control and elimination efforts. Nguyen Ha Nam and colleagues* (Nguyen Xuan Thang, Gary Dahl, James O’Donnell, Vashti Irani, Sara Canavati, Jack Richards, Ngo Duc Thang, and Tran Thanh Duong) presented their study of this group at the recent Malaria World Congress. They are also sharing what they learned below.
Mobile migrant populations present a special challenge for malaria control and elimination efforts. Nguyen Ha Nam and colleagues* (Nguyen Xuan Thang, Gary Dahl, James O’Donnell, Vashti Irani, Sara Canavati, Jack Richards, Ngo Duc Thang, and Tran Thanh Duong) presented their study of this group at the recent Malaria World Congress. They are also sharing what they learned below.
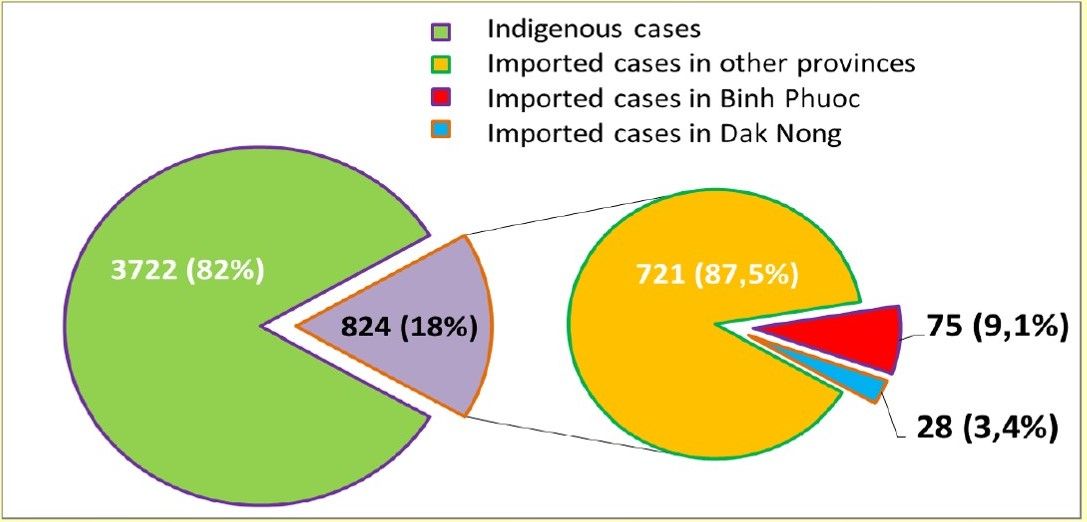
 Mobile Migrant Populations (MMPs) are a key population for containing the spread of malaria in the border areas between Cambodia and Vietnam. The number of imported cases in Viet Nam in 2017. 12,5% of such cases caught in Binh Phuoc and Dak Nong provinces and all of them came from Cambodia. The provinces bordering Cambodia and Vietnam have been had the highest malaria transmission intensity. This borders are frequented by MMPs who have proven difficult to target for surveillance and malaria control activities.
Mobile Migrant Populations (MMPs) are a key population for containing the spread of malaria in the border areas between Cambodia and Vietnam. The number of imported cases in Viet Nam in 2017. 12,5% of such cases caught in Binh Phuoc and Dak Nong provinces and all of them came from Cambodia. The provinces bordering Cambodia and Vietnam have been had the highest malaria transmission intensity. This borders are frequented by MMPs who have proven difficult to target for surveillance and malaria control activities.
 Mobile Outreach Teams (MOTs) provide a potential approach to target malaria elimination activities for MMPs who may not be strongly supported by the regular village-based and clinic-based health services. This work describes the implementation of MOTs in Binh Phuoc and Dak Nong Provinces, which are high-risk regions along the Viet Nam-Cambodia border. These activities were conducted as part of the Regional Artemisinin-resistance Initiative (RAI) in 2017. Each MOT was comprised of 2 Commune Health Staff and 1 Village Health Worker (VHW) from the village nearest to the outreach area.
Mobile Outreach Teams (MOTs) provide a potential approach to target malaria elimination activities for MMPs who may not be strongly supported by the regular village-based and clinic-based health services. This work describes the implementation of MOTs in Binh Phuoc and Dak Nong Provinces, which are high-risk regions along the Viet Nam-Cambodia border. These activities were conducted as part of the Regional Artemisinin-resistance Initiative (RAI) in 2017. Each MOT was comprised of 2 Commune Health Staff and 1 Village Health Worker (VHW) from the village nearest to the outreach area.
In the first phase of the pilot, 3 communes of 2 districts in Binh Phuoc and 2 communes of 1 district in Dak Nong with highest malaria cases reported from NIMPE are selected as targeted areas. The Objectives were to …
- Design/tailor Mobile Outreach Information Education and Communication/Behaviour change communication (BCC/ IEC) Toolkit
- Intensify case detection and quality management by increasing the coverage of diagnostics and treatment for hard to reach populations
- Strengthen outreach to high-risk and under-served populations through MOT scouting activities to locate unreached Mobile Communities and map their locations
- Link MMPs with health facilities and Village Health Workers
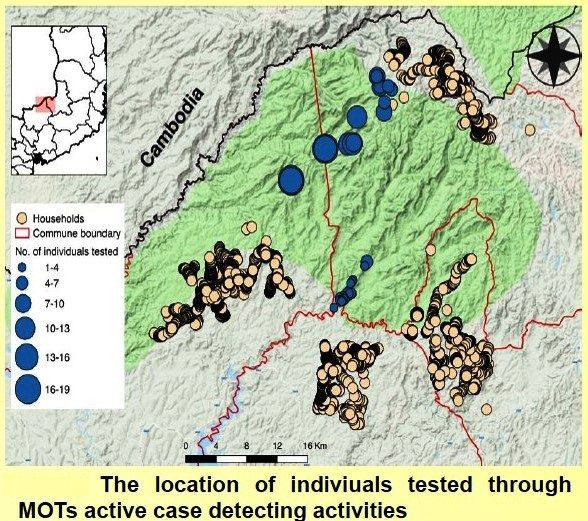 All MOT members were provided with smartphones and were trained on how to use the EpiCollect5 app to track malaria cases, record mapping information and upload real-time reports of these malaria cases. MOTs conducted 5-day outreach activities every month. These activities began with scouting out locations of the MMP communities.
All MOT members were provided with smartphones and were trained on how to use the EpiCollect5 app to track malaria cases, record mapping information and upload real-time reports of these malaria cases. MOTs conducted 5-day outreach activities every month. These activities began with scouting out locations of the MMP communities.
Once located, the MOTs geo-tagged the location of the community, conducted a short epidemiological survey on the community and screened for malaria using Rapid Diagnostic Tests and blood smear microscopy. Active malaria cases were provided with treatment according to the National guidelines, and Long Lasting Insecticidal Nets were distributed based on results of diagnosis and the survey.
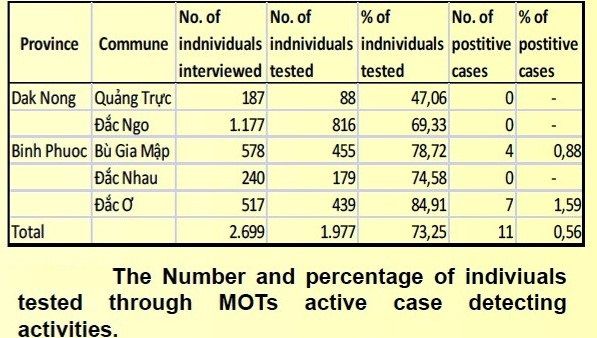 This action has led to increased diagnosis and treatment of hard to reach MMPs with increased access by those communities to malaria services. Improved understanding and increased use of malaria prevention practices hard to reach MMP communities/households. Mapped of previously unreached MMP Communities and unofficial border crossing points with malaria transmission hotspots and highly frequented crossing identified. The number of MMPs were monitored by MOTs were 2,699 accounting for 5.18% of the population in the project sites (2,699/52,095).
This action has led to increased diagnosis and treatment of hard to reach MMPs with increased access by those communities to malaria services. Improved understanding and increased use of malaria prevention practices hard to reach MMP communities/households. Mapped of previously unreached MMP Communities and unofficial border crossing points with malaria transmission hotspots and highly frequented crossing identified. The number of MMPs were monitored by MOTs were 2,699 accounting for 5.18% of the population in the project sites (2,699/52,095).
These screened MMPs were almost located along the border among project communes in Bu Gia Map National Forest where have a lot of unofficial border crossers, timber camp communities, and other revolving communities. 1,977 targeted people were tested for malaria. This number was achieved 73.25% of mobile migrant people (1,977/2,699). This work highlights how MOTs can target the previously unreached populations of MMPs to strengthen malaria surveillance and active case responses to reduce malaria transmission in Viet Nam.
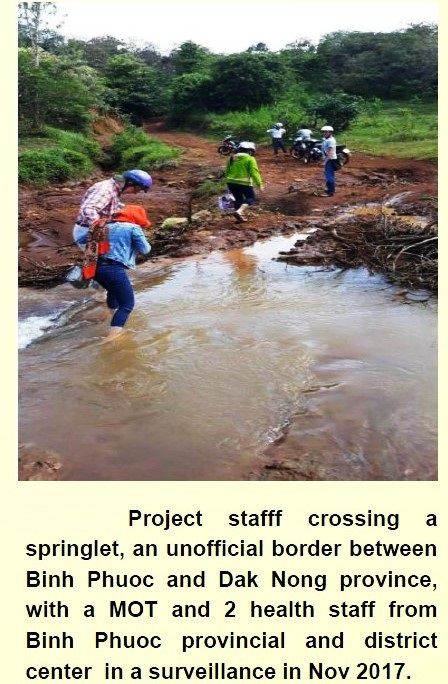 A system of real-time data collection of malaria cases from VHWs and MOTs using mobile phone uploads was established. Border screening and tracking hard to reach communities is a useful approach to implement to identify imported cases; however, it is labor-intensive, and misses subjects crossing at unofficial borders due to limited working time of MOTs (5 days a month).
A system of real-time data collection of malaria cases from VHWs and MOTs using mobile phone uploads was established. Border screening and tracking hard to reach communities is a useful approach to implement to identify imported cases; however, it is labor-intensive, and misses subjects crossing at unofficial borders due to limited working time of MOTs (5 days a month).
Positive cases in Binh Phuoc province are maintained for keeping track after receiving treatment due to no confirmed cases detected in targeted communes in Dak Ngo province, though these communes mainly have numerous transient timber camps moving in deep forests, and highly mobile border-crossers moving between regions and countries frequently. Future work will combine routine support from District health staff and expand the role of VHWs with motorbike provision for each MOT in order to not only to improve their quality outreach activities but also develop stronger Active Case Detection in the next phase of the project.
*Team members represent the National Institute of Malariology, Parasitology and Entomology, Hanoi, Viet Nam; Health Poverty Action, London, UK; and the Burnet Institute, Melbourne, Australia.
References
- Kheang ST, Lin MA, et al. Malaria Case Detection Among Mobile Populations and Migrant Workers in Myanmar: Comparison of 3 Service Delivery Approaches. 2018
- Shannon Takala-Harrison,a Christopher G. Jacob, et al. Independent Emergence of Artemisinin Resistance Mutations Among Plasmodium falciparum in Southeast Asia. 2014.
- Imwong M, Hien TT, et al. Spread of a single multidrug resistant malaria parasite lineage (PfPailin) to Vietnam. 2017.
- Richard J Maude,corresponding author Chea Nguon, et al. Spatial and temporal epidemiology of clinical malaria in Cambodia 2004–2013. 2014.
- Imwong M, Nguyen TN, et al.The epidemiology of subclinical malaria infections in South-East Asia: findings from cross-sectional surveys in Thailand–Myanmar border areas, Cambodia, and Vietnam. 2015.
- Hannah Edwards, Sara E. Canavati, et al. Novel Cross-Border Approaches to Optimise Identification of Asymptomatic and Artemisinin-Resistant Plasmodium Infection in Mobile Populations Crossing Cambodian Borders. 2015.
CHW &Community &ITNs &Ivermectin &Mapping &MDA &Seasonal Malaria Chemoprevention Bill Brieger | 04 Jul 2018
Mapping to Integrate Filariasis and Onchocerciasis Control with Malaria Interventions
 William R Brieger (wbriege1@jhu.edu) and Gilbert Burnham (gburnha1@jhu.edu) of The Johns Hopkins Bloomberg School of Public Health, Department of International Health presented ideas about mapping and integration of neglected tropical diseases and malaria interventions at the Malaria World Congress, Melbourne, Australia, July 2018
William R Brieger (wbriege1@jhu.edu) and Gilbert Burnham (gburnha1@jhu.edu) of The Johns Hopkins Bloomberg School of Public Health, Department of International Health presented ideas about mapping and integration of neglected tropical diseases and malaria interventions at the Malaria World Congress, Melbourne, Australia, July 2018
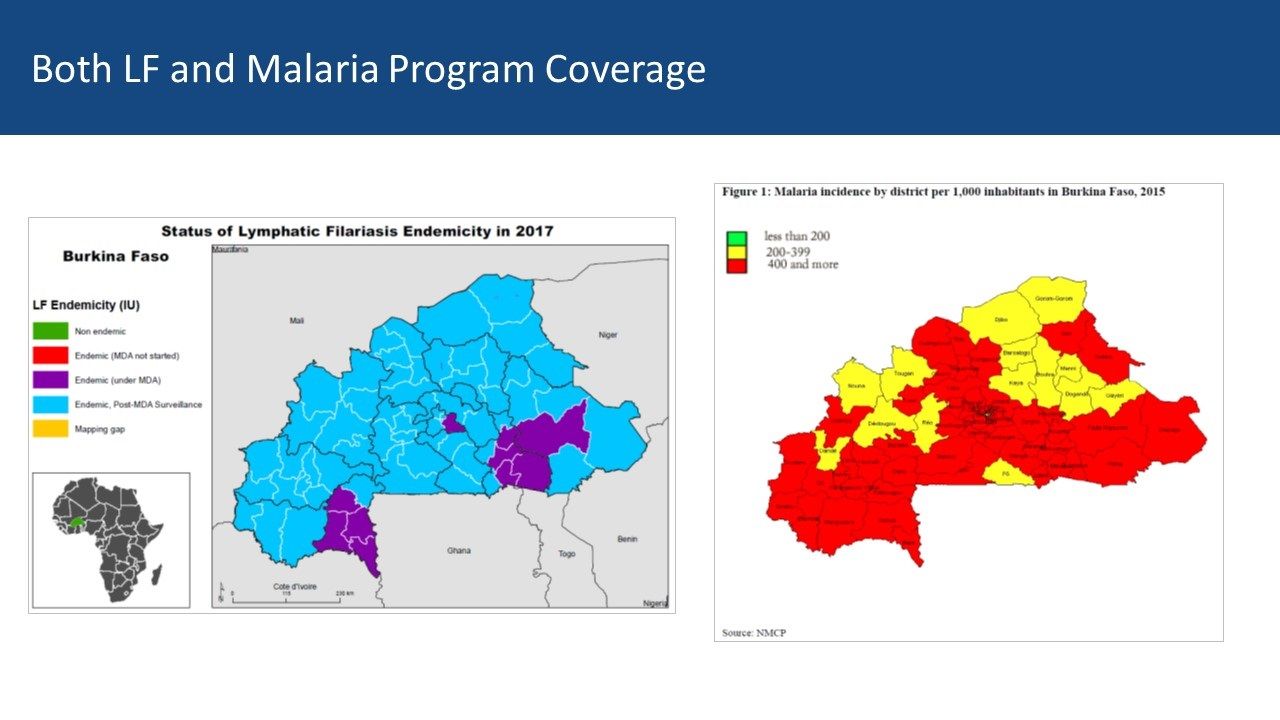
Overview: Lymphatic Filariasis (LF) and Malaria share a common vector in sub-Saharan Africa. Mass Drug Administration (MDA) is a strategy that is common to both diseases. Where the diseases overlap there is the potential opportunity to coordinate both vector control and MDA to achieve synergy in program results. The example of Burkina Faso, supplemented with information from Ghana, serves as an example of what could be integrated and what actually happens.
 Background: Thirty years ago then veterinary drug, ivermectin, was found effective in controlling neglected tropical diseases (NTDs), specifically two human filarial diseases: onchocerciasis and lymphatic filariasis (LF). The drug manufacturer donates 300 million treatments annually to eliminate both diseases. Since then, annual community based mass drug administration (MDA) efforts have resulted in millions of treatments in endemic countries and great progress has been made toward elimination of transmission. Through observation and experimentation, ivermectin was found to kill malaria carrying mosquitoes when they bite people who have taken ivermectin making it a useful tool for vector control.
Background: Thirty years ago then veterinary drug, ivermectin, was found effective in controlling neglected tropical diseases (NTDs), specifically two human filarial diseases: onchocerciasis and lymphatic filariasis (LF). The drug manufacturer donates 300 million treatments annually to eliminate both diseases. Since then, annual community based mass drug administration (MDA) efforts have resulted in millions of treatments in endemic countries and great progress has been made toward elimination of transmission. Through observation and experimentation, ivermectin was found to kill malaria carrying mosquitoes when they bite people who have taken ivermectin making it a useful tool for vector control.

CHWs in Burkina Faso demonstrating how to measure height to determine ivermectin dosage
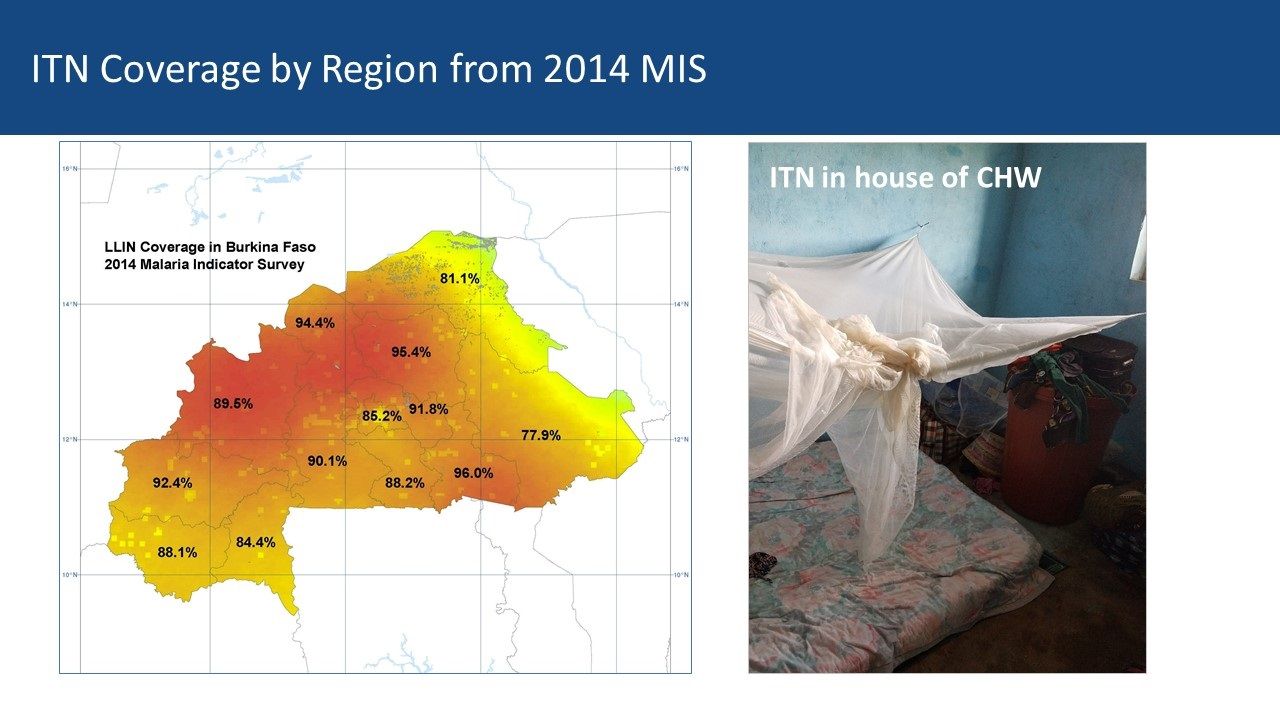
Community Health Workers’ Role: Current research is examining how dosing and timing of treatments may impact national malaria vector control efforts. Comparing maps between malaria and LF can be a starting point for adapting ivermectin MDAs for malaria vector control. Burkina Faso MDAs are operationalized by community health workers (CHWs) who are part of a national program that provides treatment for common illnesses and also conducts village level onchocerciasis and LF MDAs. Vector Control with Long Lasting Insecticide Treated Nets In most of rural Africa, malaria and lymphatic Filariasis are co-endemic and share the same anopheles mosquito vector.
However, that does not mean that there is a coordinated effort to plan distribution of LLINs despite the fact that the intervention meets the needs of both disease control efforts. The current NTD programs in Burkina Faso and Ghana focus on Preventive Chemotherapy (PCT) delivered through Mass Drug Administration (MDA). Vector Control is seen as essential in areas co-endemic with LF, Loa loa and Malaria – mapping helps identify priority areas for vector control.
 Vector Control by Chance: In Ghana, the NTD/LF elimination program was unaware of the LLIN coverage data available in the NMCP housed in an adjacent building. This illustrates the lack of collaboration between the two programs. Thus where — and if — vector control benefits the reduction of both diseases, it is often by chance where LF is concerned. The International NGO, The Carter Center, may be the only one that includes vector control as part of its programming for both malaria and LF in Nigeria. This practice should be replicated by other partners and country programs where possible.
Vector Control by Chance: In Ghana, the NTD/LF elimination program was unaware of the LLIN coverage data available in the NMCP housed in an adjacent building. This illustrates the lack of collaboration between the two programs. Thus where — and if — vector control benefits the reduction of both diseases, it is often by chance where LF is concerned. The International NGO, The Carter Center, may be the only one that includes vector control as part of its programming for both malaria and LF in Nigeria. This practice should be replicated by other partners and country programs where possible.
 Mass Drug Administration: MDA is the major strategy for control of five PCT diseases in the NTD program, and LF is one of those. Currently MDA anti-malarial drugs has been considered in limited situations in countries where there are areas that have very low transmission In the future countries may consider research that shows mosquitocidal effects of Onchocerciasis and LF MDAs with ivermectin. Otherwise for malaria, a special intervention called Seasonal Malaria Chemoprevention (SMC) is used in an MDA-like approach to reach young children in the African Sahel during high transmission months. In both cases, existing cadres of (usually volunteer) community health workers are the front line providers of MDA.
Mass Drug Administration: MDA is the major strategy for control of five PCT diseases in the NTD program, and LF is one of those. Currently MDA anti-malarial drugs has been considered in limited situations in countries where there are areas that have very low transmission In the future countries may consider research that shows mosquitocidal effects of Onchocerciasis and LF MDAs with ivermectin. Otherwise for malaria, a special intervention called Seasonal Malaria Chemoprevention (SMC) is used in an MDA-like approach to reach young children in the African Sahel during high transmission months. In both cases, existing cadres of (usually volunteer) community health workers are the front line providers of MDA.
Burkina Faso LF Map from ESPEN: Mapping shows 10 of 70 health districts are currently doing LF MDA, though all have done it. Thus CHWs in all districts are experienced in ivermectin MDA. The malaria map shows that two-thirds of districts have a malaria incidence of 400/1000 or more while 14 have lower incidence. There is an overlap between current LF MDA districts and higher incidence malaria districts Both LF and Malaria Program Coverage can be seen to overlap in [program maps.

Ghana CHWs explain how they conduct MDA
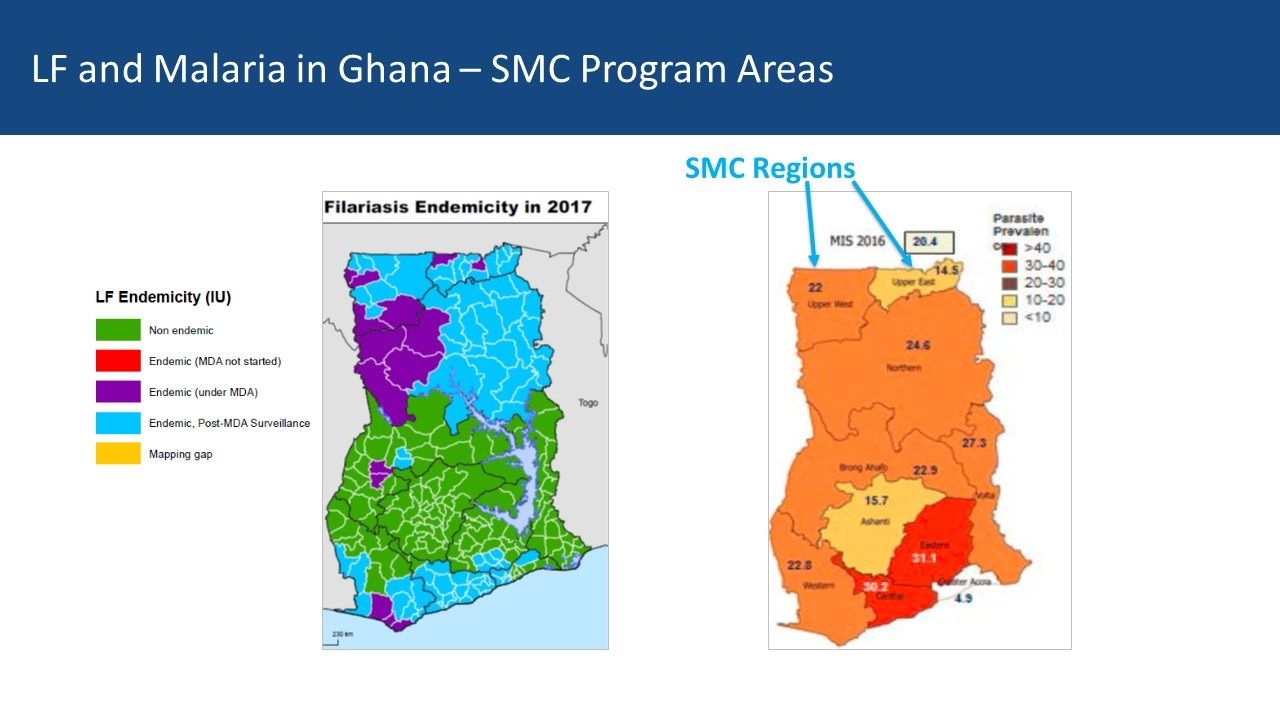
Ghana Experiences: Ghana provides a contrasting example. There five regions in central Ghana that are mostly non-endemic for LF but do have moderate malaria transmission In the south two regions with former LF MDA activity overlap with higher malaria endemicity While four northern regions have lower malaria parasite prevalence, they do have current and recent LF MDAs Community Directed Distributors work with LF MDA in Ghana
Conclusions: Malaria elimination will need a mix of strategies to be successful. Therefore, it is not too early for malaria and NTD program managers, as well as their respective donors, to begin comparing maps to identify possibilities for adapting ivermectin MDAs for malaria vector control. Even though one endemic disease is nearing control or elimination, the infrastructure put in place to accomplish this can be mobilized for other disease control efforts – as long as we map where interventions and resources have been targeted.
ITNs &Vector Control Bill Brieger | 26 Jun 2018
Tanzania Malaria Indicator Survey, ITNs and the View of the Press
 Take away messages by the Press sometimes need a bit of clarification. A recent report in The Citizen (Dar es Salaam) expressed that the author was ‘startled’ to mean from the recent Malaria Indicator Suvey (MIS/DHS 2017) that there is high malaria prevalence in regions that also have high insecticide treated bednet ownership and use, implying that nets might not be effective. Actually the preliminary Key Indicators Report showed the overlap between prevalence and nets but did not actually present statistical analysis comparing the two to show whether actual sleeping under the net is associated with prevalence one way or the other.
Take away messages by the Press sometimes need a bit of clarification. A recent report in The Citizen (Dar es Salaam) expressed that the author was ‘startled’ to mean from the recent Malaria Indicator Suvey (MIS/DHS 2017) that there is high malaria prevalence in regions that also have high insecticide treated bednet ownership and use, implying that nets might not be effective. Actually the preliminary Key Indicators Report showed the overlap between prevalence and nets but did not actually present statistical analysis comparing the two to show whether actual sleeping under the net is associated with prevalence one way or the other.
 The reporter quoted Dr William Kisinza, director and chief researcher at the Amani Research Centre of the National Institute for Medical Research as saying “This shows that mosquito bed-nets aren’t the only solution in addressing malaria in Tanzania,” and while this is true, it should not be construed as meaning nets don’t work. Any national malaria strategy uses ITNs in combination with other interventions to have a comprehensive program, including indoor residual spraying, which is also mentioned in the new article.
The reporter quoted Dr William Kisinza, director and chief researcher at the Amani Research Centre of the National Institute for Medical Research as saying “This shows that mosquito bed-nets aren’t the only solution in addressing malaria in Tanzania,” and while this is true, it should not be construed as meaning nets don’t work. Any national malaria strategy uses ITNs in combination with other interventions to have a comprehensive program, including indoor residual spraying, which is also mentioned in the new article.
Dr Kisinza was also quoted as saying, “In Kigoma and Mtwara, bed-nets are used in fishing. There’s a need for behavioural change, if the problem is to be effectively addressed.” This is a real problem but anecdotal. In order to make a clearer point it would be necessary to test the connection between net ownership and use and do a follow-up study to see if in fact those owning but not sleeping under the nets are practicing alternative net usage.
 Actually key findings from the preliminary MIS report include the fact that while 78% of households have one ITN, only 45% have at least one for every two people. Hence it is not surprising that only 55% of children under the age of 5 and 62% of pregnant women reported sleeping under a net. These are important service gaps that must be addressed. Certainly all countries need to monitor the effectiveness of nets and insecticide resistance.
Actually key findings from the preliminary MIS report include the fact that while 78% of households have one ITN, only 45% have at least one for every two people. Hence it is not surprising that only 55% of children under the age of 5 and 62% of pregnant women reported sleeping under a net. These are important service gaps that must be addressed. Certainly all countries need to monitor the effectiveness of nets and insecticide resistance.
Analysis of net use and malaria parasitaemia among the children can and should be presented to address the reporter’s questions as well as provide a clue to potential insecticide resistance.
Children &Equity &IPTp &ITNs &Monitoring Bill Brieger | 26 May 2018
Malawi Makes Progress and Plans to Defeat Malaria: Directions from the 2017 Malaria Indicator Survey
Malawi has conducted four Malaria Indicator Surveys (MIS), with the most recent being in 2017. Such surveys are crucial tools for [planning and evaluating efforts by national control programs and their partners. Dr. Dan Namarika, Secretary for Health, Ministry of Health in the preface to the 2017 Report sums up the context and progress best, and so first, we have reproduced his narrative below.
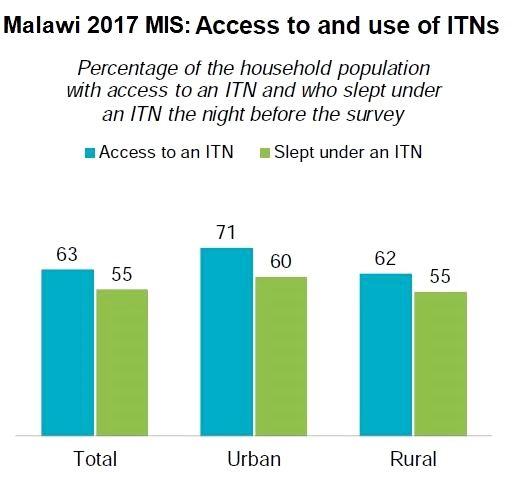
Then we look at the example of the insecticide treated net (ITN) data as a way to guide future planning. The MIS format itself has seen improvements with much better color graphics in addition to the traditional tables. Some of these are also shared herein.
 According to Dr Namarika, “Malaria is a major public health problem in Malawi where an estimated 4 million cases occur each year. Children under age 5 and pregnant women are most likely to have severe illness. The Ministry of Health, in collaboration with partners, has developed the Malawi Health Sector Strategic Plan 2017-2022, which articulates the priorities for health sector development in the next 6 years and prioritizes malaria. In line with that emphasis, the National Malaria Control Program has just finished the development of the National Malaria Strategic Plan 2017–2022 with the goal of scaling up malaria interventions to reduce morbidity and mortality by 50% in 2022.
According to Dr Namarika, “Malaria is a major public health problem in Malawi where an estimated 4 million cases occur each year. Children under age 5 and pregnant women are most likely to have severe illness. The Ministry of Health, in collaboration with partners, has developed the Malawi Health Sector Strategic Plan 2017-2022, which articulates the priorities for health sector development in the next 6 years and prioritizes malaria. In line with that emphasis, the National Malaria Control Program has just finished the development of the National Malaria Strategic Plan 2017–2022 with the goal of scaling up malaria interventions to reduce morbidity and mortality by 50% in 2022.
 “We strive for progress in achieving prompt, effective malaria treatment. We hope to improve access to early intervention and treatment by expanding village clinic services, using insecticide-treated nets, spraying inside residences, managing the environment, encouraging changes in social behaviour and communication, and preventing malaria in pregnancy. We have set for ourselves high targets for these interventions, and we are confident that we will achieve our strategic goals of halving the incidence of malaria and deaths, as well as reducing the prevalence of malaria and malaria-related anaemia.
“We strive for progress in achieving prompt, effective malaria treatment. We hope to improve access to early intervention and treatment by expanding village clinic services, using insecticide-treated nets, spraying inside residences, managing the environment, encouraging changes in social behaviour and communication, and preventing malaria in pregnancy. We have set for ourselves high targets for these interventions, and we are confident that we will achieve our strategic goals of halving the incidence of malaria and deaths, as well as reducing the prevalence of malaria and malaria-related anaemia.
“Surveys such as the current Malaria Indicator Survey (MIS) are essential measures of progress towards these goals. Without measurement, we can only guess about progress. The 2017 Malawi Malaria Indicator Survey (MMIS) is the country’s fourth nationally representative assessment of the coverage attained by key malaria interventions. Interventions are reported in combination with measures of malaria-related burden and anaemia prevalence testing among children under age 5.
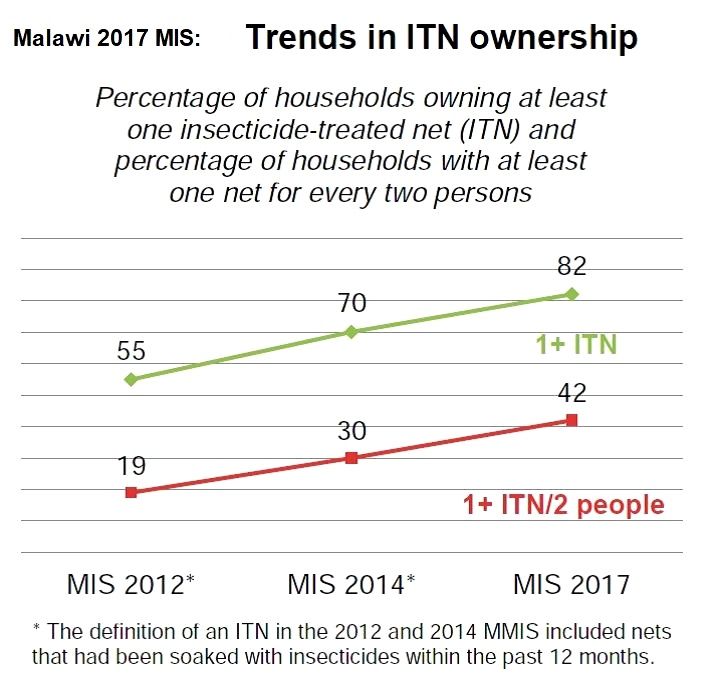
 “Overall, there has been considerable progress in scaling up interventions and controlling malaria. We noted a decline in malaria prevalence from 33% in 2014 to 24% in 2017. Insecticide-treated net (ITN) ownership has increased from 70% in 2014 to 82% in 2017.
“Overall, there has been considerable progress in scaling up interventions and controlling malaria. We noted a decline in malaria prevalence from 33% in 2014 to 24% in 2017. Insecticide-treated net (ITN) ownership has increased from 70% in 2014 to 82% in 2017.
“Results of the 2017 MIS also show improvement on use of intermittent preventive treatment during pregnancy (IPTp) by pregnant women age 15-49. Coverage has increased from 64% for two or more doses in 2014 to 77% in 2017. The percentage of women who took three or more doses of SP/Fansidar for prevention of malaria in pregnancy increased from 13% in 2014 to 43% in 2017.
 “In addition, numbers of children receiving a parasitological test and artemisinin-based combination therapy continue to increase.
“In addition, numbers of children receiving a parasitological test and artemisinin-based combination therapy continue to increase.
“These results represent the combined work of numerous partners contributing to the overall scale-up of malaria interventions. I would like to request that all partners make use of the information presented in this report as they implement projects to surmount the challenges depicted here.”
 According to PMI, “The 2017-2022 National Malaria Strategic Plan (MSP) builds on the successes achieved and lessons learned during implementation of previous strategic plans.” The example of ITN targets is illustrative and is included in the target, “At least 90% pf the population use one or more malaria preventative interventions.”
According to PMI, “The 2017-2022 National Malaria Strategic Plan (MSP) builds on the successes achieved and lessons learned during implementation of previous strategic plans.” The example of ITN targets is illustrative and is included in the target, “At least 90% pf the population use one or more malaria preventative interventions.”
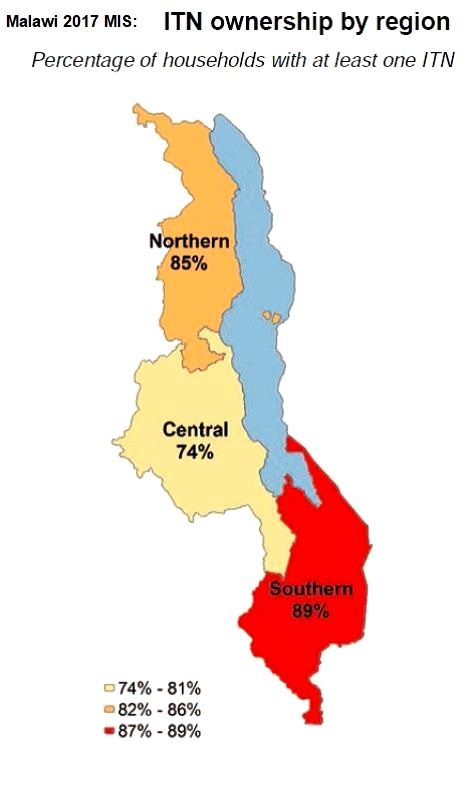
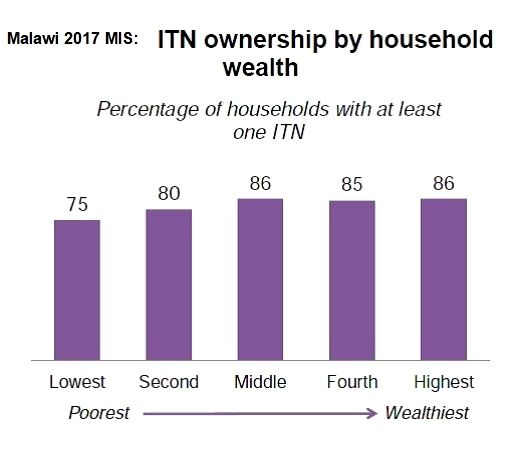
So in addition to showing progress with ITNs, the MIS 2017 report also points to gaps that require strengthened intervention. While there has been an increase of household net ownership we can see in the graph that the target for universal coverage of 1 net for 2 people still needs work. We can also see in the graphs that equity remains a challenge with a lower proportion of poorer households owning a net. In addition net ownership is lower in the Central Region of the Country.
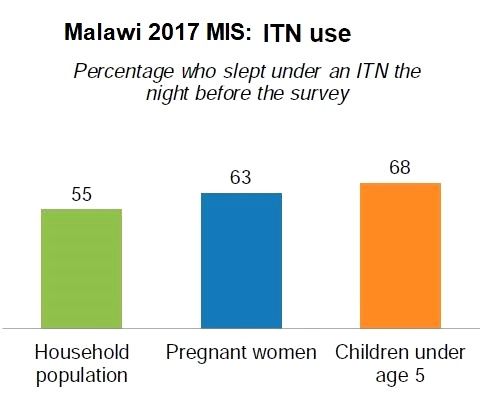 We learn from the graphs that having access to a net in the household does not guarantee that people will actually use or sleep under them. The tables show us that the traditionally defined ‘vulnerable groups’ like pregnant women (62.5%) and children below the age of 5 years (67.5%) were more likely to sleep under nets than household members in general (55.4%). The push towards universal coverage stresses that all household members contribute to the health, welfare and wealth of the family and should be protected from malaria.
We learn from the graphs that having access to a net in the household does not guarantee that people will actually use or sleep under them. The tables show us that the traditionally defined ‘vulnerable groups’ like pregnant women (62.5%) and children below the age of 5 years (67.5%) were more likely to sleep under nets than household members in general (55.4%). The push towards universal coverage stresses that all household members contribute to the health, welfare and wealth of the family and should be protected from malaria.
Now we should Return the comments by Dr Namarika on the value of having MIS data. All endemic countries need to ensure their malaria data are up-to-date to ensure they use this information to keep their strategic plans on track to defeat malaria.
Agriculture &Development &Epidemiology &Food Security &Integrated Vector Management &ITNs Bill Brieger | 25 May 2018
Agriculture and Promotion of Food Security Can Affect Malaria Transmission
The link between malaria and food security in a global context has been made. The influence of malaria on food security was examined. Now the connection between agriculture practices/food security and malaria is pursued below.
 A common complaint with programs that distribute insecticide-treated bednets to prevent malaria is that the nets may be used for other purposes that the intended effort to prevent infected mosquitoes from biting people. All informants interviewed for a study in Western Zambia reported that ITNs are regularly used for fishing and the misuse is widespread. Unsustainable fishing practices, drought and population pressure were mentioned as reasons for fishery decline. The implication was that the use of free ITNs for fishing at least saved the population money in a time of declining fortunes.
A common complaint with programs that distribute insecticide-treated bednets to prevent malaria is that the nets may be used for other purposes that the intended effort to prevent infected mosquitoes from biting people. All informants interviewed for a study in Western Zambia reported that ITNs are regularly used for fishing and the misuse is widespread. Unsustainable fishing practices, drought and population pressure were mentioned as reasons for fishery decline. The implication was that the use of free ITNs for fishing at least saved the population money in a time of declining fortunes.
A broader review of the ITNs for fishing issue was done through contacting expert witnesses across Africa. Mosquito net fishing (MNF) was found to be a broadly pan-tropical activity, particularly prevalent in sub-Saharan Africa. The authors found that, “Perceived drivers of MNF were closely related to poverty, revealing potentially complex and arguably detrimental livelihood and food security implications.”
 The mosquito breeding potential of dams cuts across Africa with the number of dams located in malarious areas projected to increase according to Kibret and colleagues. This is because “The population at risk of malaria around existing dams and associated reservoirs, is estimated to increase from 15 million in 2010 to 21-23 million in the 2020s, 25-26 million in the 2050s and 28-29 million in the 2080s.” In addition, areas with dams but without malaria transmission at present, will likely transition to regions of unstable transmission due to climate change.
The mosquito breeding potential of dams cuts across Africa with the number of dams located in malarious areas projected to increase according to Kibret and colleagues. This is because “The population at risk of malaria around existing dams and associated reservoirs, is estimated to increase from 15 million in 2010 to 21-23 million in the 2020s, 25-26 million in the 2050s and 28-29 million in the 2080s.” In addition, areas with dams but without malaria transmission at present, will likely transition to regions of unstable transmission due to climate change.
Likewise, a study in Ethiopia starts with the assertion that, “Dams are important to ensure food security and promote economic development in sub-Saharan Africa,” and then stresses the importance of understanding the consequences of these projects. The researchers found that “the mean monthly malaria incidence and anopheline larval density was generally higher in the dam villages than in the non-dam villages” in all the three dam settings studied. So while dams can increase agricultural production, the authors concluded that, “the presence of dams intensifies malaria transmission in lowland and midland ecological settings.”
 Hydro-agricultural projects include dams and irrigation. Human bait mosquito captures volunteers in hydro-agricultural and river bank sites in Cameroon Akono et al. found that mosquito biting rates were higher in hydro-agricultural sites of less urbanized and urban settings than in natural river banks sites. An additional implication is that urban farming, an important component of food security, may influence mosquito and malaria prevalence.
Hydro-agricultural projects include dams and irrigation. Human bait mosquito captures volunteers in hydro-agricultural and river bank sites in Cameroon Akono et al. found that mosquito biting rates were higher in hydro-agricultural sites of less urbanized and urban settings than in natural river banks sites. An additional implication is that urban farming, an important component of food security, may influence mosquito and malaria prevalence.
Stoler and colleagues pursued this question of urban agriculture. The odds of self-reported malaria are significantly higher for women in Accra, Ghana who are living within 1 km of urban agriculture compared with all women living near an irrigation source, the association disappearing beyond this critical distance. Likewise in Kumasi, Afrane et al. learned that “adult and larval mosquito abundance and larval survival were high in the irrigated fields in the irrigated (urban) vegetable farm. This therefore, contributed significantly to adult mosquito populations and hence malaria transmission in the city.”
Even agricultural practices in smaller subsistence farms can foster malaria mosquito breeding. Practices found in southwest Nigeria include collection of pools of water in the farms for soaking cassava tubers, digging of trenches, irrigation of farms, and the presence of fish ponds.
Communities can perceive how agricultural practices may contribute to malaria. In Tanzania a fair number of rural respondents associated growing of rice with malaria. They also noted that the need to sleep on their farms at times meant they could not benefit from the mosquito nets hanging back in their house, some hours walk away. The idea of rice cultivation and malaria was tested in central Kenya. Mwangangi and co-researchers found that, “Rice fields and associated canals were the most productive habitat types,” for malaria mosquito breeding. Overall, Mboera et al. found, “evidence that malaria transmission risk varies even between neighbouring villages and is influenced by agro-ecosystems.”
Although we can establish the two-way link or intersection between malaria and food security, we can see that recommended joint or integrated programming may not always be optimal at various levels from the nation to the community. Greater collaboration between health and agricultural ministries and agencies is needed, supported by national policies that see malaria and food production as part of overall national development goals.
Advocacy &Case Management &Community &IPTp &ITNs Bill Brieger | 30 Apr 2018
Burkina Faso Celebrated World Malaria Day with Pledges to Defeat Malaria
 Burkina Faso celebrated World Malaria Day with pledges to Defeat Malaria on 25th April 2018. Dr Ousman Badolo. Technical Director of Jhpiego’s USAID/PMI Supported Improving Malaria Care (IMC) Project describes below the event in the village of Kamboinsin, not far from the capital, Ouagadougou. Ibrahim Sawadogo from IMC provided the photographs.
Burkina Faso celebrated World Malaria Day with pledges to Defeat Malaria on 25th April 2018. Dr Ousman Badolo. Technical Director of Jhpiego’s USAID/PMI Supported Improving Malaria Care (IMC) Project describes below the event in the village of Kamboinsin, not far from the capital, Ouagadougou. Ibrahim Sawadogo from IMC provided the photographs.
The day started with a proclamation of malaria day from Burkina Faso’s President, Roch Marc Christian Kaboré, to his assembled cabinet and the press. The president recognized that malaria is still a major public health issue in the country, and while deaths are decreasing, the incidence of malaria is not. The President called for a greater commitment of resources by all partners to insure that malaria can be defeated in Burkina Faso by 2030.
 Kamboinsin village in Sig-Noghin Health District was the site of further observances organized by the National Malaria Control Program, later that afternoon. This district was chosen because of having among the highest incidence rates for malaria in the region. Many partners set up booths to share their work in malaria with partners and citizens of the district. Included were three research centers (Centre Muraz, CNRFP and IRD), and three USAID programs supported by the President’s Malaria Initiative in Burkina Faso (Procurement and Supply Management [PSM], IMC and VectorLink), among others.
Kamboinsin village in Sig-Noghin Health District was the site of further observances organized by the National Malaria Control Program, later that afternoon. This district was chosen because of having among the highest incidence rates for malaria in the region. Many partners set up booths to share their work in malaria with partners and citizens of the district. Included were three research centers (Centre Muraz, CNRFP and IRD), and three USAID programs supported by the President’s Malaria Initiative in Burkina Faso (Procurement and Supply Management [PSM], IMC and VectorLink), among others.
 During the program both the Minister for Health and the US Ambassador spoke. The Minister highlighted the main strategies that Burkina Faso is employing to reduce and eliminate malaria including regular use of insecticide treated nets (ITN), seasonal malaria chemoprevention, Intermittent Preventive Treatment in Pregnancy (IPTp), Prompt and Appropriate Case Management and other Vector Control Strategies.
During the program both the Minister for Health and the US Ambassador spoke. The Minister highlighted the main strategies that Burkina Faso is employing to reduce and eliminate malaria including regular use of insecticide treated nets (ITN), seasonal malaria chemoprevention, Intermittent Preventive Treatment in Pregnancy (IPTp), Prompt and Appropriate Case Management and other Vector Control Strategies.
The US Ambassador shared a real-life story of a pregnant woman who during her current pregnancy decided to register early for Antenatal Care (ANC) as encouraged by the IMC project. She was able to get several doses of IPTp as required as well as obtain an ITN on her first visit, unlike in her previous pregnancies.
 Entertainment was provided by the comedian Hypolythe Wangrawa (alias M’ba Bouanga) who presented a sketch involving his ‘son’ who was not encouraging his wife to attend ANC and receive malaria prevention services. M’ba Bouanga chastised the son and an actor playing a midwife explained to the family the value of attending ANC and preventing malaria. Singers Maria Bissongo, Miss Oueora and Aicha Junior provided the audience with a song that embodied a variety of malaria prevention and care messages.
Entertainment was provided by the comedian Hypolythe Wangrawa (alias M’ba Bouanga) who presented a sketch involving his ‘son’ who was not encouraging his wife to attend ANC and receive malaria prevention services. M’ba Bouanga chastised the son and an actor playing a midwife explained to the family the value of attending ANC and preventing malaria. Singers Maria Bissongo, Miss Oueora and Aicha Junior provided the audience with a song that embodied a variety of malaria prevention and care messages.
 A highlight of the occasion was recognition of high performing health districts in the country. They were judged on criteria including good management of malaria commodity stocks, reduced case fatality rates, use of diagnostic tests to confirm malaria before treatment and coverage of at least three doses of IPTp. Four districts were given awards, Titao, Thyou, Boussouma and Batie, while Charles de Gaul Pediatric Hospital was also recognized.
A highlight of the occasion was recognition of high performing health districts in the country. They were judged on criteria including good management of malaria commodity stocks, reduced case fatality rates, use of diagnostic tests to confirm malaria before treatment and coverage of at least three doses of IPTp. Four districts were given awards, Titao, Thyou, Boussouma and Batie, while Charles de Gaul Pediatric Hospital was also recognized.
One can watch a video of the proclamation by the President on the National Facebook page. More details of the events are found in the following media: Lefaso.net and Paalga Observer.
World Malaria Day in Burkina Faso demonstrated the political will and commitment to “defeat malaria.” More and more national resources will be needed to reach the endline in 2030.
Advocacy &Case Management &Children &CHW &Community &Elimination &Funding &iCCM &Invest in Malaria Control &IPTp &ITNs Bill Brieger | 25 Apr 2018
On World Malaria Day the realities of resurgence should energize the call to ‘Beat Malaria’
 Dr Pedro Alonso who directed the World Health Organization’s Global Malaria Program, has had several opportunities in the past two weeks to remind the global community that complacency on malaria control and elimination must not take hold as there are still over 400,000 deaths globally from malaria each year. At the Seventh Multilateral Initiative for Malaria Conference (MIM) in Dakar, Dr Alonso drew attention to the challenges revealed in the most recent World Malaria Report (WMR). While there have been decreases in deaths, there are places where the number of actual cases is increasing.
Dr Pedro Alonso who directed the World Health Organization’s Global Malaria Program, has had several opportunities in the past two weeks to remind the global community that complacency on malaria control and elimination must not take hold as there are still over 400,000 deaths globally from malaria each year. At the Seventh Multilateral Initiative for Malaria Conference (MIM) in Dakar, Dr Alonso drew attention to the challenges revealed in the most recent World Malaria Report (WMR). While there have been decreases in deaths, there are places where the number of actual cases is increasing.
 Around twenty years ago the course of malaria changed with the holding of the first MIM, also in Dakar and the establishment of the Roll Bank Malaria (RBM) Partnership. These were followed in short order by the Abuja Declaration that set targets for 2010 and embodied political in endemic countries, as well as major funding mechanisms such as the Global Fund to fight AIDS, TB and Malaria. This spurred what has been termed a ‘Golden Decade’ of increasing investment and intervention coverage, leading to decreasing malaria morbidity and mortality. The Millennium Development Goals provided additional impetus to reduce the toll of malaria by 2015.
Around twenty years ago the course of malaria changed with the holding of the first MIM, also in Dakar and the establishment of the Roll Bank Malaria (RBM) Partnership. These were followed in short order by the Abuja Declaration that set targets for 2010 and embodied political in endemic countries, as well as major funding mechanisms such as the Global Fund to fight AIDS, TB and Malaria. This spurred what has been termed a ‘Golden Decade’ of increasing investment and intervention coverage, leading to decreasing malaria morbidity and mortality. The Millennium Development Goals provided additional impetus to reduce the toll of malaria by 2015.
 On Facebook Live yesterday Dr Alonso talked about that ‘Golden Decade.’ There was a 60% decrease in mortality and a 40% decreases in malaria cases. But progress slowing down and we may be stalled at a crossroads. He noted that history show unless accelerate efforts, malaria will come back with a vengeance. Not only is renewed political leadership and funding, particularly from affected countries needed, but we also need new tools. Dr Alonso explained that the existing tools allowed 7m deaths be diverted in that golden decade, but these tools are not perfect. We are reaching limits on these tools such that we need R&D for tools to enable quantum leap forward. Even old tools like nets are threatened by insecticide resistance, and research on alternative safe insecticides is crucial.
On Facebook Live yesterday Dr Alonso talked about that ‘Golden Decade.’ There was a 60% decrease in mortality and a 40% decreases in malaria cases. But progress slowing down and we may be stalled at a crossroads. He noted that history show unless accelerate efforts, malaria will come back with a vengeance. Not only is renewed political leadership and funding, particularly from affected countries needed, but we also need new tools. Dr Alonso explained that the existing tools allowed 7m deaths be diverted in that golden decade, but these tools are not perfect. We are reaching limits on these tools such that we need R&D for tools to enable quantum leap forward. Even old tools like nets are threatened by insecticide resistance, and research on alternative safe insecticides is crucial.
 Dr Alonso at MIM pointed to the worrying fact that investment in malaria overall peaked in 2013. Investment by endemic countries themselves has remained stable throughout and never gone reached $1 billion despite advocacy and leadership groups like the Africa Leaders Malaria Alliance. The 2017 WMR shows that while 16 countries achieved a greater that 20% reduction in malaria cases, 25 saw a greater that 20% increase in cases. The outnumbering of decreasing countries by increasing was 4 to 8 in Africa, the region with the highest burden of the disease. Overall 24 African countries saw increases in cases between 2015 and 2016 versus 5 that saw a decrease. A review of the Demographic and Health and the Malaria Information Surveys in recent years show that most countries continue to have difficulty coming close to the Abuja 2010 targets for Insecticide treated net (ITN) use, prompt and appropriate malaria case management and intermittent preventive treatment of malaria in pregnancy (IPTp).
Dr Alonso at MIM pointed to the worrying fact that investment in malaria overall peaked in 2013. Investment by endemic countries themselves has remained stable throughout and never gone reached $1 billion despite advocacy and leadership groups like the Africa Leaders Malaria Alliance. The 2017 WMR shows that while 16 countries achieved a greater that 20% reduction in malaria cases, 25 saw a greater that 20% increase in cases. The outnumbering of decreasing countries by increasing was 4 to 8 in Africa, the region with the highest burden of the disease. Overall 24 African countries saw increases in cases between 2015 and 2016 versus 5 that saw a decrease. A review of the Demographic and Health and the Malaria Information Surveys in recent years show that most countries continue to have difficulty coming close to the Abuja 2010 targets for Insecticide treated net (ITN) use, prompt and appropriate malaria case management and intermittent preventive treatment of malaria in pregnancy (IPTp).
 The coverage gap is real. The WMR shows that while there have been small but steady increase in 3 doses of IPTp, coverage of the first dose has leveled off. Also while ownership of a net by households has increased, less than half of households have at least one net for every two residents.
The coverage gap is real. The WMR shows that while there have been small but steady increase in 3 doses of IPTp, coverage of the first dose has leveled off. Also while ownership of a net by households has increased, less than half of households have at least one net for every two residents.
In contrast a new form of IPT – seasonal malaria chemoprevention (SMC) for children in the Sahel countries has taken off with over 90% of children receiving at least one of the monthly doses during the high transmission season. Community case management is taking off as is increased use of rapid diagnostic testing. Increased access to care may explain how in spite of increased cases, deaths can be reduced. This situation could change rapidly if drug resistance spreads.
 While some international partners are stepping up, we are far short of the investment needed. The Gates Foundation is pledging more for research and development to address the need for new tools as mentioned by Dr Alonso. A big challenge is adequate funding to sustain the implementation of both existing tools and the new ones when they come online. Even in the context of a malaria elimination framework, WHO stresses the need to maintain appropriate levels of intervention with case management, ITNs and other measures regardless of the stage of elimination at which a country or sub-strata of a country is focused.
While some international partners are stepping up, we are far short of the investment needed. The Gates Foundation is pledging more for research and development to address the need for new tools as mentioned by Dr Alonso. A big challenge is adequate funding to sustain the implementation of both existing tools and the new ones when they come online. Even in the context of a malaria elimination framework, WHO stresses the need to maintain appropriate levels of intervention with case management, ITNs and other measures regardless of the stage of elimination at which a country or sub-strata of a country is focused.
Twenty years after the formation of RBM and 70 years after the foundation of WHO, the children, families and communities of endemic countries are certainly ready to beat malaria. The question is whether the national and global partners are equally ready.