Children &Indoor Residual Spraying &IPTp &ITNs &Malaria in Pregnancy Bill Brieger | 23 Feb 2020
Preventing Malaria in Mozambique: the 2018 Malaria Indicator Survey Summarized
 The Demographic and Health Survey Program has recently released the 2018 Malaria Indicator Survey for Mozambique. Below is a summary of some of the key findings. These focus on access and use of insecticide-treated nets, intermittent preventive treatment in pregnancy and case management
The Demographic and Health Survey Program has recently released the 2018 Malaria Indicator Survey for Mozambique. Below is a summary of some of the key findings. These focus on access and use of insecticide-treated nets, intermittent preventive treatment in pregnancy and case management
While “82% of Mozambican households have at least one ITN, and half have at least one ITN for each two people,” these achievements do not reach universal coverage targets. That said, the ownership of at least one net by a household did increase from 51% in 2011 to the recent 82%. Likewise 23% of households met the universal coverage target of one net per two people in a household in 2011 compared to 51% in 2018. The pace of progress may appear good, but this must be seen in light of lack of growth in donor funding and greater calls for countries to assume more financial responsibility for disease control.
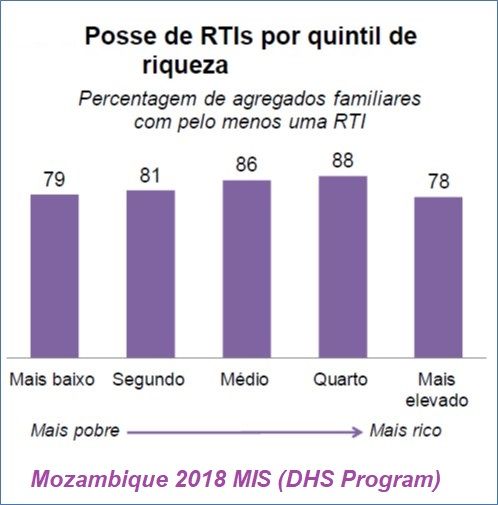 Of interest is the fact that net ownership is spread somewhat evenly over the economic class quintiles. Ideally we would want to see better ownership figures for the lower quintiles.
Of interest is the fact that net ownership is spread somewhat evenly over the economic class quintiles. Ideally we would want to see better ownership figures for the lower quintiles.
Households obtained their nets from three major sources. “Most ITNs (87%) were obtained in mass distribution campaigns, 4% in prenatal consultations (PNC) and 6% are purchased in stores or markets.” While the proportion getting their nets through PNC may roughly reflect the proportion of the population who are pregnant at a given time, the survey is not specifically a snapshot of this population in real time. Thus, one could question whether distribution of ITNs through routine health services is fully functioning.
Since it was noted that only half of households have the ideal number of ITNs to reach universal coverage of their members, it is not surprising that only, “69% of the population of households’ family members have access to an ITN. This means that 7 in every 10 people could sleep under an ITN if each ITN in a household were used by a maximum of two people.” On the positive side, this represents an approximate doubling of use of ITNs since 2011.
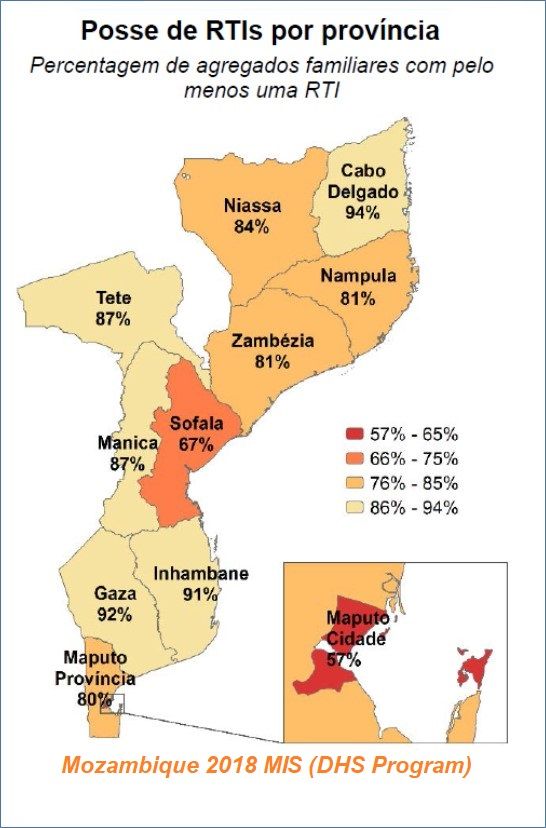 The survey further notes that those segments of the population traditionally viewed as “vulnerable” fared a bit better: “73% of children under 5 years and 76% of pregnant women slept under an ITN the night before investigation.” This too, represents a doubling from 2011. There is also geographical variation where it appears that the more rural provinces have higher rates of use.
The survey further notes that those segments of the population traditionally viewed as “vulnerable” fared a bit better: “73% of children under 5 years and 76% of pregnant women slept under an ITN the night before investigation.” This too, represents a doubling from 2011. There is also geographical variation where it appears that the more rural provinces have higher rates of use.
It would appear that IRS is not a major component of malaria control. Household coverage with indoor residual spray “decreased from 19% in 2011 to 11% in 2015, and then increased to 16% in 2018.” Urban coverage (23%) of IRS in the twelve months prior to the survey is twice as high as the percentage in rural areas (12%).
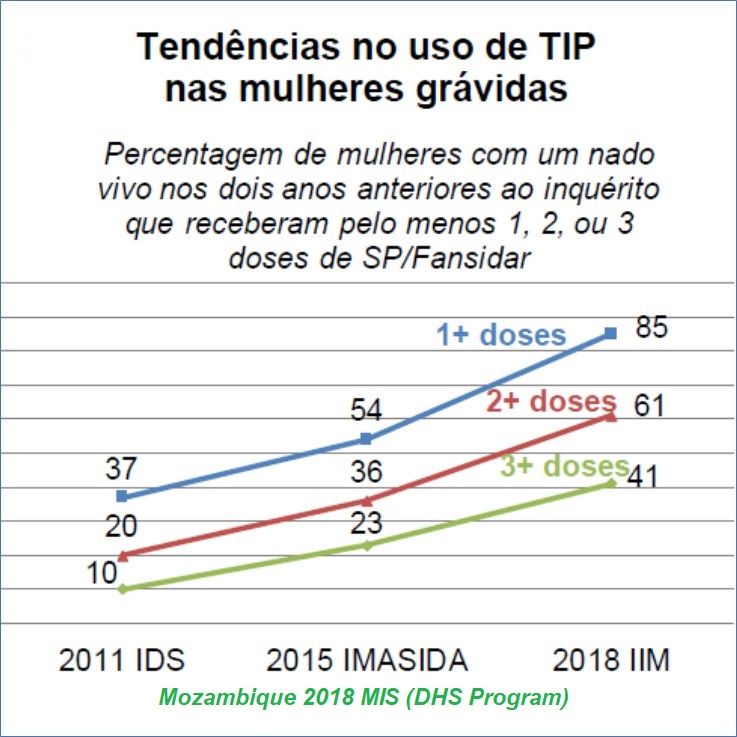 Although still not meeting targets, Mozambique has seen major progress in providing IPTp for pregnant women. Over the period from 2011 to 2018 the proportion of pregnant women receiving even one dose rose from 37% to 85%. Since WHO has set targets for at least 3 monthly doses from the 13th week of pregnancy, Mozambique’s coverage of the third dose increased from 10% to 41% with wide variation among provinces.
Although still not meeting targets, Mozambique has seen major progress in providing IPTp for pregnant women. Over the period from 2011 to 2018 the proportion of pregnant women receiving even one dose rose from 37% to 85%. Since WHO has set targets for at least 3 monthly doses from the 13th week of pregnancy, Mozambique’s coverage of the third dose increased from 10% to 41% with wide variation among provinces.
UNICEF shared data from 2015 to show that 51% of pregnant women in Mozambique attended 4 PNC/ANC visits, implying that there are missed opportunities for achieving at least 3 doses of IPTp. Also, since more women are now getting the first dose of IPTp, hopefully more can also get an ITN at PNC.
These national surveys (MIS, DHS) are invaluable for assessing progress and planning what interventions need to be strengthened where and among whom. They also show that progress is slow, reinforcing global concerns that malaria elimination will still be a challenge by 2050.
Case Management &Diagnosis &IPTp &ITNs &Quality of Services Bill Brieger | 26 Nov 2019
Use of Malaria Service and Data Quality Improvement in Mwanza Tanzania
 Emmanuel Lesilwa, Goodluck Tesha, Jasmine Chadewa, Agnes Kosia, Zahra Mkomwa, Bayoum Awadhi, Gaudiosa Tibaijuka, Rita Noronha, Dunstan Bishanga, Lusekelo Njonge, Frank Chacky, Abdallah Lusasi, Ally Mohamed, Chonge Kitojo, and Erik Reaves presented a poster entitled “Use of Malaria Service and Data Quality Improvement (MSDQI) Tool in Cascaded Supervision Approach Improved Quality of Malaria Services – Experience from Mwanza, Tanzania” at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings are shared below.
Emmanuel Lesilwa, Goodluck Tesha, Jasmine Chadewa, Agnes Kosia, Zahra Mkomwa, Bayoum Awadhi, Gaudiosa Tibaijuka, Rita Noronha, Dunstan Bishanga, Lusekelo Njonge, Frank Chacky, Abdallah Lusasi, Ally Mohamed, Chonge Kitojo, and Erik Reaves presented a poster entitled “Use of Malaria Service and Data Quality Improvement (MSDQI) Tool in Cascaded Supervision Approach Improved Quality of Malaria Services – Experience from Mwanza, Tanzania” at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings are shared below.
 Inadequate quality of malaria service and data has been one of the problems in Mwanza region due to high malaria prevalence, inadequate knowledge of supervisors and standardized supervision tool. In 2017, NMCP and stakeholders developed malaria services and data quality improvement (MSDQI) tool to guide supervisors. The tool comprises of seven modules addressing performance of Malaria Case Management with indicators weighted against a standard score. Any facility scoring below 50% of the overall score is deemed poorly performing, 50%-75% moderate and above 75% good performance.
Inadequate quality of malaria service and data has been one of the problems in Mwanza region due to high malaria prevalence, inadequate knowledge of supervisors and standardized supervision tool. In 2017, NMCP and stakeholders developed malaria services and data quality improvement (MSDQI) tool to guide supervisors. The tool comprises of seven modules addressing performance of Malaria Case Management with indicators weighted against a standard score. Any facility scoring below 50% of the overall score is deemed poorly performing, 50%-75% moderate and above 75% good performance.
 What is Malaria Service and Data Quality Improvement (MSDQI)? It is a checklist to guide supportive supervision teams in evaluating the quality of malaria services at the health facility level. MSDQI helps with the:-
What is Malaria Service and Data Quality Improvement (MSDQI)? It is a checklist to guide supportive supervision teams in evaluating the quality of malaria services at the health facility level. MSDQI helps with the:-
- Monitoring and evaluation
- Facility-based malaria performance indicators
- Provision of timely, accurate information and data for decision-making at district, regional, and national levels
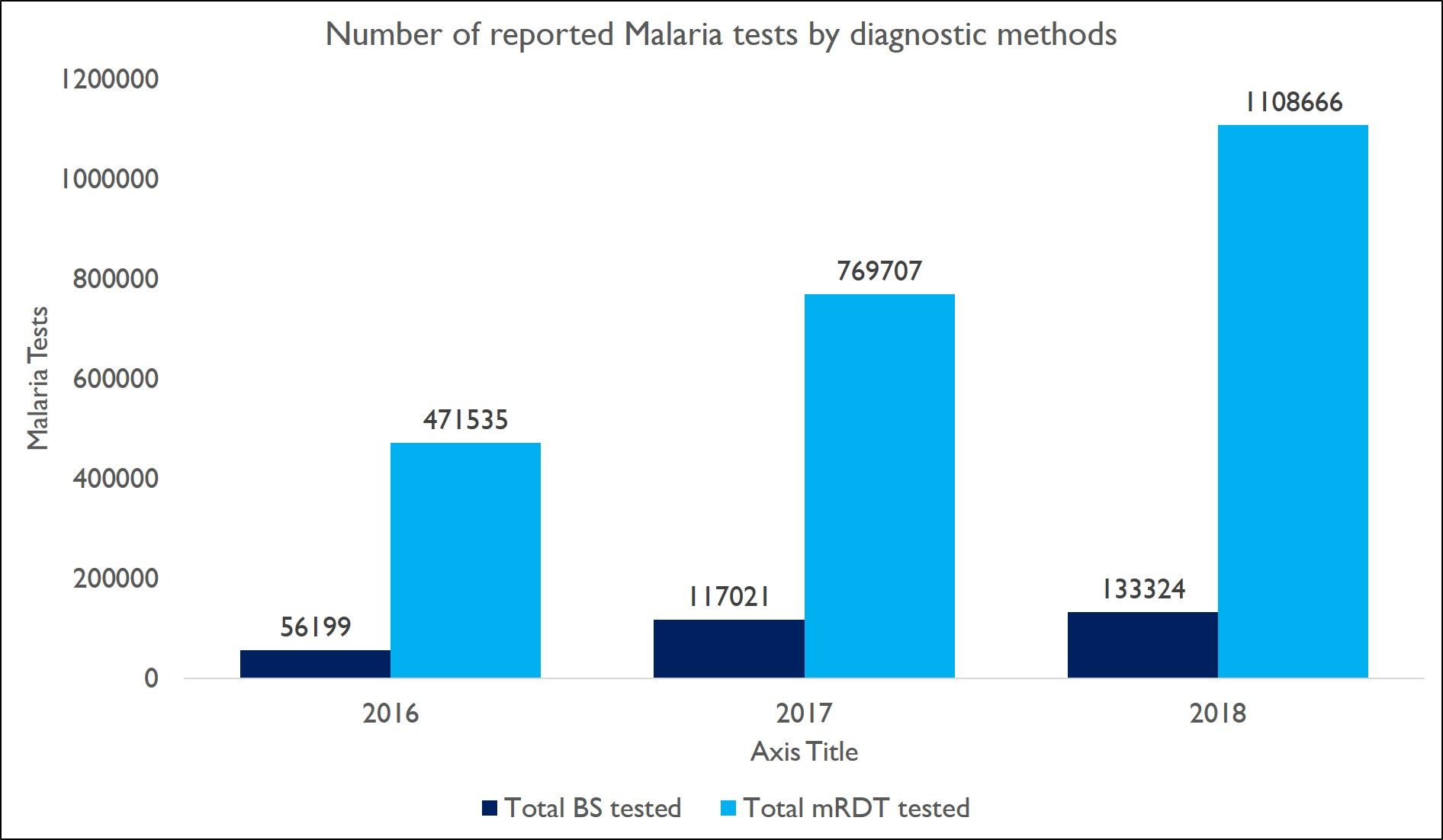
 In the attached graphs we present the Number of malaria test among OPD cases and the Number of malaria test among OPD cases which increased from 527,734 in 2016 to 1,241,990 in 2018 in Mwanza region. This resulted to the decrease of patients treated without malaria confirmatory test.
In the attached graphs we present the Number of malaria test among OPD cases and the Number of malaria test among OPD cases which increased from 527,734 in 2016 to 1,241,990 in 2018 in Mwanza region. This resulted to the decrease of patients treated without malaria confirmatory test.
 After intervention with MSDQI, there was a Decline in proportion of malaria cases clinically diagnosed and treated in Mwanza Regions reduced from 6.5% cases in 2016 to 0.1% cases in 2018
After intervention with MSDQI, there was a Decline in proportion of malaria cases clinically diagnosed and treated in Mwanza Regions reduced from 6.5% cases in 2016 to 0.1% cases in 2018
Good progress in IPTp2 and IPTp3 Coverage in Mwanza region was also 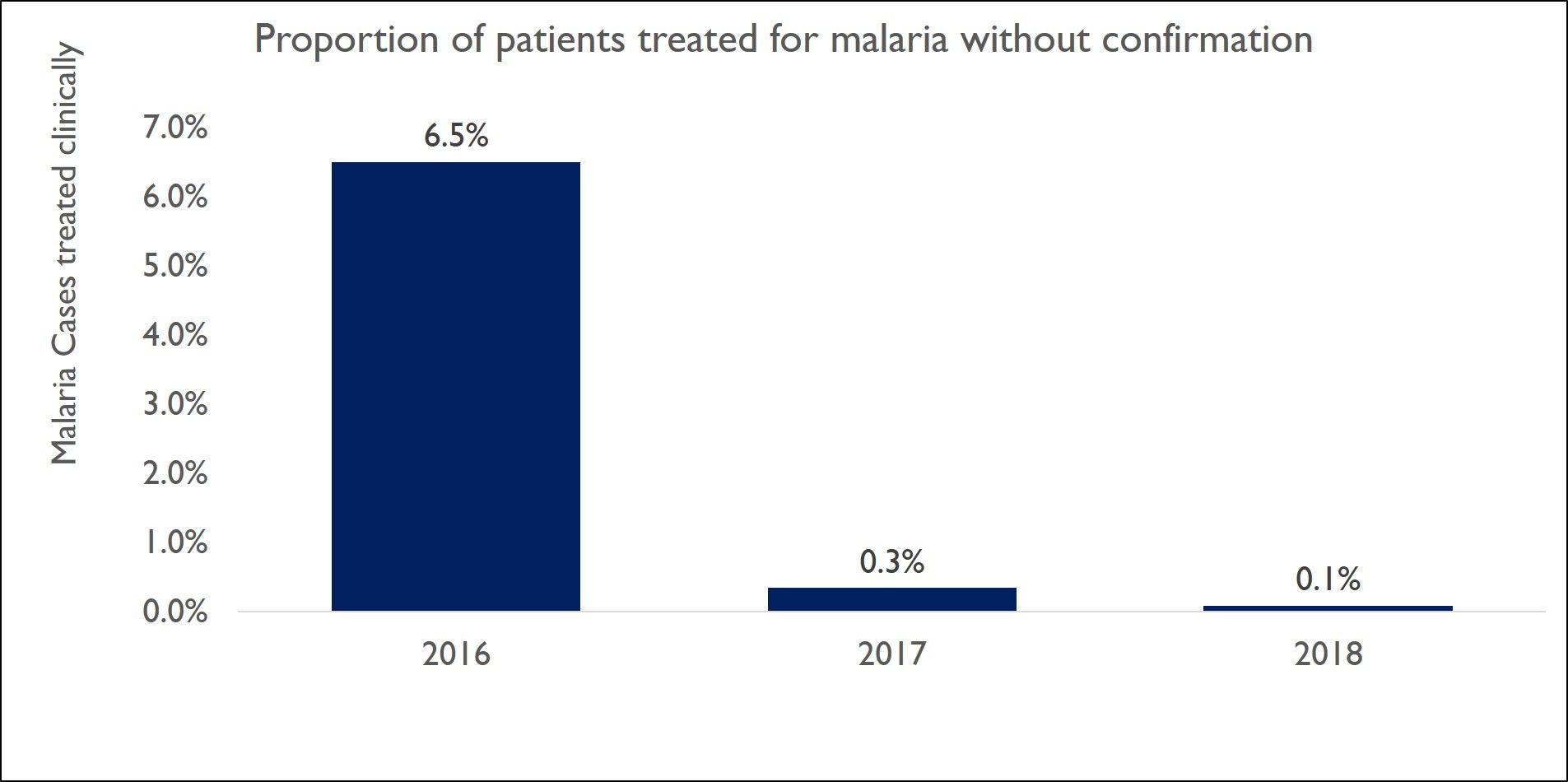 documented. IPTp2 increased from 37.6% in 2016 to 72.3%, while PITp3 increased from 1.2% in 2016 to 48.5% in 2018.
documented. IPTp2 increased from 37.6% in 2016 to 72.3%, while PITp3 increased from 1.2% in 2016 to 48.5% in 2018.
There was Increased coverage of LLINs in pregnant women and infants.
Increased coverage of LLINs in Pregnant women went from 4.9% 2016 to 75.6% in 2018. Likewise that for Infants increased from 2.9% 2016 to 65% in 2018.
 Several Lessons were Learned. Cascaded supervision approaches contribute to improved quality of malaria service provision and hence improved malaria indicators. The Way forward is to Continue using cascaded supervisors to improve quality of data and malaria services through MSDQI
Several Lessons were Learned. Cascaded supervision approaches contribute to improved quality of malaria service provision and hence improved malaria indicators. The Way forward is to Continue using cascaded supervisors to improve quality of data and malaria services through MSDQI
 *Affiliation: : USAID Boresha Afya Lake and Western Zone – PATH; USAID Boresha Afya Lake and Western Zone –Jhpiego; National Malaria Control Programme-Tanzania Ministry of Health, Community Development, Gender, Elderly and Children, Tanzania; US President’s Malaria Initiative-United States Agency for International Development
*Affiliation: : USAID Boresha Afya Lake and Western Zone – PATH; USAID Boresha Afya Lake and Western Zone –Jhpiego; National Malaria Control Programme-Tanzania Ministry of Health, Community Development, Gender, Elderly and Children, Tanzania; US President’s Malaria Initiative-United States Agency for International Development
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of the USAID Boresha Afya and do not necessarily reflect the views of USAID or the United States government
Borders &Diagnosis &Ebola &Elimination &Integrated Vector Management &ITNs &Mosquitoes &NTDs &Snakebite &Trachoma &Urban Bill Brieger | 04 Aug 2019
Tropical Health Update 2019-08-04: Ebola, Malaria Vectors, Snakebite and Trachoma
In the past week urban transmission in Goma, a city of at least 2 million inhabitants in eastern Democratic republic of Congo, was documented as a gold miner came home and infected his wife and child. To get a grip on the spread of the disease, DRC is considering another vaccine, not without some controversy. WHO provides detailed guidance on all aspects of response. On the malaria front we have learned more about malaria vectors, natural immunity and reactive case detection.
Ebola Challenges: Vaccines, Urban Transmission
 The current Ebola vaccine being deployed to over 150,000 people in North Kivu and Ituri Provinces was itself an experimental intervention during 2016 when it was first used in the largest ever outbreak located in West Africa. BBC reports that, “World Health Organization (WHO) data show the Merck vaccine has a 97.5% efficacy rate for those who are immunised, compared to those who are not.”
The current Ebola vaccine being deployed to over 150,000 people in North Kivu and Ituri Provinces was itself an experimental intervention during 2016 when it was first used in the largest ever outbreak located in West Africa. BBC reports that, “World Health Organization (WHO) data show the Merck vaccine has a 97.5% efficacy rate for those who are immunised, compared to those who are not.”
The proposed addition of a Johnson and Johnson vaccine would be in that same experimental phase if introduced in DRC now. It has been proven safe as well as effective in other primates. The challenge is that even though the Merck vaccine supplies are near 500,000, this is not enough to cover the potential needs in an area with over 10 million people, although Merck is still producing more. At present, BBC says, “Those pushing for the use of the new Johnson & Johnson vaccine, had proposed using it to create a protective wall, vaccinating people outside the outbreak zone.” In addition, the new national response team is concerned that “Only about 50% of cases of Ebola in the Democratic Republic of Congo are being identified.”
Finally, there is the issue of community mistrust of government workers and challenging logistics. “There are also concerns that the new vaccine – which requires two injections 56 days apart – may be difficult to administer in a region where the population is highly mobile, and insecurity is rife.”
If efforts at vaccination are needed soon in Goma, up to 2 million doses might be needed. Reuters reports that, “Congolese authorities were racing to contain an Ebola epidemic on Thursday, after a gold miner with a large family contaminated several people in the east’s main city of Goma before dying of the hemorrhagic fever.” Readers may recall that the West Africa outbreak of 2014-16 in Guinea, Sierra Leone and Liberia accelerated greatly after infected people went to major cities in search of help.
The miner is the second ‘imported case into Goma, which borders Rwanda, but because his family lives there, he has already infected his wife and one of his 10 children. Contacts are being traced and monitored, but this urban and border threat is one of the factors that led WHO to finally declare the current outbreak a public health emergency.
Malaria
As we move toward malaria elimination Reactive Case Detection (RCD) has been proposed as an integral part of these efforts with the hopes that is can be conceived of as a way of gradually decreasing transmission, according to an article in Malaria Journal. In fact, the value of RCD may be limited as follows:
- RCD alone can eliminate malaria in only a very limited range of settings, where transmission potential is very low
- In other settings, it is likely to reduce disease burden and help maintain the disease-free state in the face of imported infections
Another article looks at “natural exposure to gametocytes that can result in the development of immunity against the gametocyte by the host as well as genetic diversity in the gametocyte.” The researchers learned that there can be variations in immune response depending on season and geography. This information is helpful in planning malaria elimination interventions.
On the vector front a baseline susceptibility testing was conducted in 16 countries in sub-Saharan Africa for neonicotinoids. “The target site of neonicotinoids represents a novel mode of action for vector control, meaning that cross-resistance through existing mechanisms is less likely.” The findings will help in the preparation for rollout of clothianidin formulations as part of national IRS rotation strategies by PMI and other partners.
 Researchers also called on us to learn more about malaria vectors in other parts of the world. In order to eliminate Plasmodium falciparum from the Caribbean and Central America program planners should consider local vector characteristics such as An. albimanus. They found that, “House-screening and repellent IRS are potentially highly effective against An. albimanus if people are indoors during the evening.”
Researchers also called on us to learn more about malaria vectors in other parts of the world. In order to eliminate Plasmodium falciparum from the Caribbean and Central America program planners should consider local vector characteristics such as An. albimanus. They found that, “House-screening and repellent IRS are potentially highly effective against An. albimanus if people are indoors during the evening.”
Vectors are also of concern on the edges of malaria transmission, particularly in South Africa, one of the ‘elimination eight’ countries of the Southern Africa Development Community. Researchers examined the, “potential role of Anopheles parensis and other Anopheles species in residual malaria transmission, using sentinel surveillance sites in the uMkhanyakude District of northern KwaZulu-Natal Province.” They found Anopheles parensis is a potential but minimal vector of malaria in South Africa “owing to its strong zoophilic tendency.” On the other hand, An. arabiensis was found to be the major vector responsible for residual malaria transmission in South Africa. Since these mosquitoes were found in outdoor-placed resting traps, interventions are needed to control outdoor-resting of vector populations.
NTDs of Concern
During the week, the member states of the African Union renewed their commitment to fight and permanently eliminate Neglected Tropical Diseases. Africa.com reported that, “Achievements to date include 1 billion people treated against at least one NTD and 37 countries have completed the removal of at least one NTD.”
Although some reports have discounted the idea of trachoma in Namibia, there may be reason to re-examine the situation. On Twitter Anthony Solomon notes that Namibia needs #trachoma prevalence surveys. A just-completed joint Ministry of Health & Social Services/@WHO mission found active trachoma & trichiasis in Zambezi & Kunene Regions.
 The Times of India draws attention to snakebite. It says that “Under-reported and inadequately treated, fatalities in India are estimated at close to 50,000 a year, the world’s highest.”
The Times of India draws attention to snakebite. It says that “Under-reported and inadequately treated, fatalities in India are estimated at close to 50,000 a year, the world’s highest.”
Overall we can see that the concept of ‘neglect’ has several uses. There is neglect if half of Ebola cases are undetected. There is neglect if we do not understand malaria vectors in low transmission areas. Finally, there is neglect if we do not conduct up-to-date disease surveys to determine whether a disease is present or not. Elimination of tropical diseases is challenging when key processes are neglected.
Conflict &Diagnosis &Ebola &ITNs &Mosquitoes &Plasmodium/Parasite &Resistance &Vaccine Bill Brieger | 29 Jul 2019
Tropical Health Update 2019-07-28: Ebola and Malaria Crises
This posting focuses on Malaria and Ebola, both of which have been the recent focus of some disturbing news. The malaria community has been disturbed by the clear documentation of resistance to drugs in Southeast Asia. Those working to contain Ebola in the northeast of the Democratic Republic of Congo saw a change in political leadership even in light of continued violence and potential cross-border spread.
Malaria Drug Resistance
Several sources reported on studies in the Lancet Infectious Diseases concerning the spread of Multidrug-Resistant Malaria in Southeast Asia. Reuters explained that by sing genomic surveillance, researchers concurred that “strains of malaria resistant to two key anti-malarial medicines are becoming more dominant” and “spread aggressively, replacing local malaria parasites,” becoming the dominant strains in Vietnam, Laos and northeastern Thailand.”
 The focus was on “the first-line treatment for malaria in many parts of Asia in the last decade has been a combination of dihydroartemisinin and piperaquine, also known as DHA-PPQ,” and resistance had begun to spread in Cambodia between 2007 and 2013. Authors of the study noted that while, “”Other drugs may be effective at the moment, but the situation is extremely fragile, and this study highlights that urgent action is needed.” They further warned of an 9impending Global Health Emergency.
The focus was on “the first-line treatment for malaria in many parts of Asia in the last decade has been a combination of dihydroartemisinin and piperaquine, also known as DHA-PPQ,” and resistance had begun to spread in Cambodia between 2007 and 2013. Authors of the study noted that while, “”Other drugs may be effective at the moment, but the situation is extremely fragile, and this study highlights that urgent action is needed.” They further warned of an 9impending Global Health Emergency.
NPR notes that “Malaria drugs are failing at an “alarming” rate in Southeast Asia” and provided some historical context about malaria drug resistance arising in this region since the middle of the 20th century. “Somehow antimalarial drug resistance always starts in that part of the world,” says Arjen Dondorp, who leads malaria research at the Mahidol Oxford Tropical Medicine Research Unit in Bangkok and who was a lead author of the report about the randomized trial. Ironically, “one reason could have something to do with the relatively low levels of malaria there. When resistant parasites emerge, they are not competing against a dominant nonresistant strain of malaria and are possibly able to spread easier.
When we are talking about monitoring resistance in low resource and logistically and politically challenging areas, we need to think of appropriate diagnostic tools at the molecular level. Researchers in Guinea-Bissau conducted a proof of concept study and used malaria rapid diagnostic tests applied for parallel sequencing for surveillance of molecular markers. While they noted that, “Factors such as RDT storage prior to DNA extraction and parasitaemia of the infection are likely to have an effect on whether or not parasite DNA can be successfully analysed … obtaining the necessary data from used RDTs, despite suboptimal output, becomes a feasible, affordable and hence a justifiable method.”
A Look at Insecticide Treated Nets
On a positive note, Voice of America provides more details on the insecticide treated net (ITN) monitoring tool developed called “SmartNet” by Dr Krezanoski in collaboration with the Consortium for Affordable Medical Technologies in Uganda. The net uses strips of conductive fabric to detect when it’s in use. Dr. Krezanoski was happy to find that people given the net used it no differently that if they were not being observed. The test nets made it clear who what using and not using this valuable health investment and when it was in use. Such fine tuning will be deployed to design interventions to educate net users based on their real-life use patterns.
Another important net issue is local beliefs that may influence use. We can find out when people use nets, but we also need to determine why. In Tanzania, researchers found that people think mosquitoes that bite in the early evening when people are outside relaxing are harmless. As one community member said, “I only fear those that bite after midnight. We’ve always been told that malaria is spread by mosquitoes that bite after midnight.”
Even if people do use their ITNs correctly, we still need to worry about insecticide resistance. A study in Afghanistan reported that, “Resistance to different groups of insecticides in the field populations of An. stephensi from Kunar, Laghman and Nangarhar Provinces of Afghanistan is caused by a range of metabolic and site insensitivity mechanisms.” The authors conclude that vector control programs need to be better prepared to implement insecticide resistance management strategies.
Ebola Crisis Becomes (More) Political
Headlines such as “Congo health minister resigns over response to Ebola crisis” confronted the global health community this week. this happened after the DRC’s relatively new president took control of the response. The President set up a new government office to oversee the response to an outbreak outside of the Ministry of Health which was managing the current outbreak and the previous ones. The new board was set up without the knowledge of the Minister who was traveling to the effected provinces at the time.
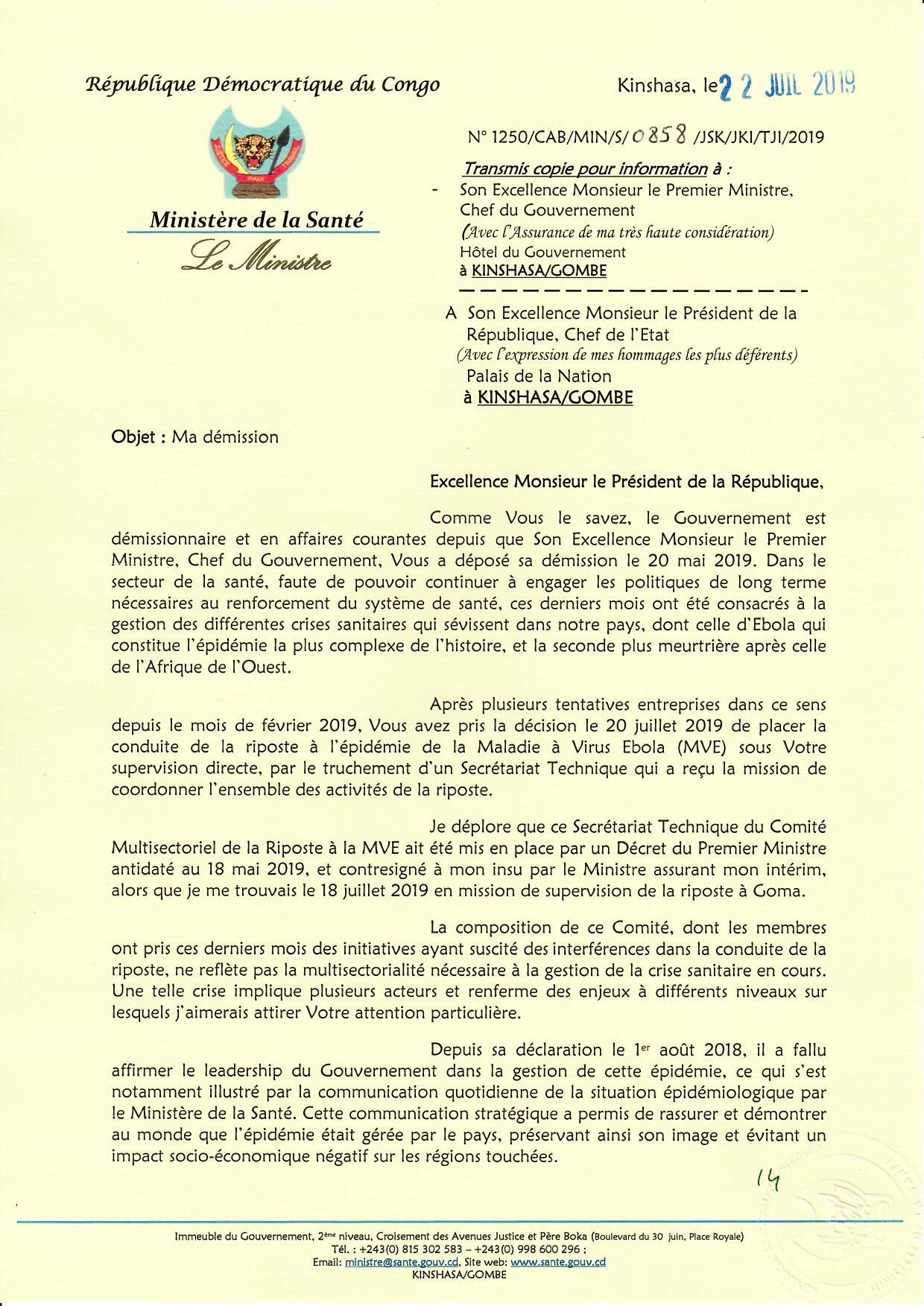 The former Minister, Dr Oly Ilunga stated on Twitter that, “Suite à la décision de la @Presidence_RDC. de gérer à son niveau l’épidémie d’#Ebola, j’ai remis ma démission en tant que Ministre de la Santé ce lundi. Ce fut un honneur de pouvoir mettre mon expertise au service de notre Nation pendant ces 2 années importantes de notre Histoire. (Following the decision of the @Presidence_RDC to manage the # Ebola outbreak, I resigned as Minister of Health on Monday. It was an honor to be able to put my expertise at the service of our Nation during these two important years of our History.)
The former Minister, Dr Oly Ilunga stated on Twitter that, “Suite à la décision de la @Presidence_RDC. de gérer à son niveau l’épidémie d’#Ebola, j’ai remis ma démission en tant que Ministre de la Santé ce lundi. Ce fut un honneur de pouvoir mettre mon expertise au service de notre Nation pendant ces 2 années importantes de notre Histoire. (Following the decision of the @Presidence_RDC to manage the # Ebola outbreak, I resigned as Minister of Health on Monday. It was an honor to be able to put my expertise at the service of our Nation during these two important years of our History.)
 The former Minister also warned that the “Multisectoral Ebola Response Committee would interfere with the ongoing activities of national and international health workers on the ground in North Kivu and Ituri provinces.” Part of the issue may likely have been “pressure to approve a new vaccine in addition to one that has already been used to protect more than 171,000 people.” People had warned about the potential confusion to the public as well as ethical issues if a second vaccine was used, especially one that did not have the strong accumulated evidence from both the current outbreak as well as the previous one in West Africa.
The former Minister also warned that the “Multisectoral Ebola Response Committee would interfere with the ongoing activities of national and international health workers on the ground in North Kivu and Ituri provinces.” Part of the issue may likely have been “pressure to approve a new vaccine in addition to one that has already been used to protect more than 171,000 people.” People had warned about the potential confusion to the public as well as ethical issues if a second vaccine was used, especially one that did not have the strong accumulated evidence from both the current outbreak as well as the previous one in West Africa.
One might have thought that this would be a time when stability was needed since “The WHO earlier this month declared the outbreak a Public Health Emergency of International Concern, a rare step meant to highlight the urgency of the moment that has been used only four times before.” In addition, “the World Bank said it would release $300 million from a special fund set aside for crises like viral outbreaks to help cover the cost of the response.”
Unfortunately one of the msain impediments to successful Ebola control, violence in the region, continues. CIDRAP stated that. “the Allied Democratic Forces (ADF), a rebel group, attacked two villages near Beni, killing 12 people who live in the heart of the Democratic Republic of the Congo’s (DRC’s) ongoing Ebola outbreak. The terrorists killed nine in Eringeti and three in Oicha, according to Reuters. ADF has not publicly pledged allegiance to the Islamic state (ISIL), but that hasn’t stopped ISIL from claiming responsibility for the attacks.” It will take more than a change of structure in Kinshasa to deal with the realities on the ground.
 CIDRAP also observed that since the resignation of the Health Minister, “DRC officials have provided no update on the outbreak, including statistics on the number of deaths, health workers infected, or suspected cases.” The last was seen on 21 July 2019.
CIDRAP also observed that since the resignation of the Health Minister, “DRC officials have provided no update on the outbreak, including statistics on the number of deaths, health workers infected, or suspected cases.” The last was seen on 21 July 2019.
ReliefWeb reports that, “Adding to the peril, the Ebola-affected provinces share borders with Rwanda and Uganda, with frequent cross-border movement for personal travel and trade, increasing the chance that the virus could spread beyond the DRC. There have already been isolated cases of Ebola reported outside of the outbreak zone.”
These are troubling times when parasites and mosquitoes are becoming more resistant to our interventions and when governments and communities are resistant to a clear and stable path to disease containment and control.
Agriculture &Borders &Ebola &Essential Medicines &Integrated Vector Management &ITNs &Larvicide &Mosquitoes &Schistosomiasis &Severe Malaria &Vaccine &Vector Control Bill Brieger | 15 Jul 2019
The Weekly Tropical Health News 2019-07-13
In the past week more attention was drawn to the apparently never-ending year-long Ebola outbreak in the northeast of the Democratic Republic of the Congo. Regarding other diseases, there is new information on the RTS,S malaria vaccine, river prawns have been found to play a biological control role in schistosomiasis, and an update from the World Health Organization on essential medicines and diagnostics. New malaria vector control technologies are discussed.
Second Largest Ebola Outbreak One Year On
Ronald A. Klain and Daniel Lucey in the Washington Post observed raised concern that, “the disease has since crossed one border (into Uganda) and continues to spread. In the absence of a trajectory toward extinguishing the outbreak, the opposite path — severe escalation — remains possible. The risk of the disease moving into nearby Goma, Congo — a city of 1 million residents with an international airport.”
They added their voices to a growing number of experts who are watching this second biggest Ebola outbreak in history and note that, “As the case count approaches 2,500 with no end in sight, it is time for the WHO to declare the outbreak a public health emergency of international concern — a ‘PHEIC’ — to raise the level of global alarm and signal to nations, particularly the United States, that they must ramp up their response.” They call for three actions: 1) improved security for health workers in the region, 2) stepped up community engagement and 3) extended health care beyond Ebola treatment. The inability to adequately respond to malaria, diarrheal diseases and maternal health not only threated life directly, but also threated community trust, putting health workers’ lives at risk.
Olivia Acland, a freelance journalist based in DRC, reporting for the New Humanitarian describes the insecurity and the recent “wave of militia attacks in the Democratic Republic of Congo’s northeastern Ituri province has left hundreds dead and roughly 300,000 displaced in recent weeks, triggering a new humanitarian crisis in a region.” Specifically, “Ituri, a fertile region rich in gold deposits, has been an epicentre of conflict in Congo for decades. Between 1999 and 2003, around 60,000 people were killed here, as a power struggle between rebel groups escalated into ethnic violence,” related to traditional tensions between Hema cattle herders and Lendu farmers with roots in Belgian colonization.
Updates from the DRC Ministry of Health report on average 11 new Ebola cases per day in the past week. So far over 160,000 people have been vaccinated, and yet the spread continues. The Ministry also describes new protocol contains three vaccinations strategies that can be used depending on the environment in which confirmed cases are found including:
- Classic Ring: The classic strategy of vaccinating contacts of confirmed cases and contact contacts.
- Enlarged ring: It is also possible to vaccinate all inhabitants of houses within 5 meters around the outbreak of a confirmed case.
- Geographical Ring: In an area where team safety can not be guaranteed, they can vaccinate an entire village or neighborhood.
Malaria Vaccines, Essential Drugs and New Vector Control Technologies
Halidou Tinto and colleagues enrolled two age groups of children in a 3-year extension of the RTS,S/AS01 vaccine efficacy trial: 1739 older children (aged 5–7 years) and 1345 younger children (aged 3–5 years). During extension, they reported 66 severe malaria cases. Overall they found that, “severe malaria incidence was low in all groups, with no evidence of rebound in RTS,S/AS01 recipients, despite an increased incidence of clinical malaria in older children who received RTS,S/AS01 compared with the comparator group in Nanoro. No safety signal was identified,” as seen in The Lancet.
WHO has updated the global guidance on medicines and diagnostic tests to address health challenges, prioritize highly effective therapeutics, and improve affordable access. Section 6.5.3 presents antimalarial medicines including curative treatment (14 medicines) for both vivax and falciparum and including tablets and injectables. Prophylaxis includes 6 medicines including those for IPTp and SMC. The latest guidance can be downloaded at WHO.
Paul Krezanoski reports on a new technology to monitor bednet use and tried it out in Ugandan households. As a result. “Remote bednet use monitors can provide novel insights into how bednets are used in practice, helping identify both households at risk of malaria due to poor adherence and also potentially novel targets for improving malaria prevention.
In another novel technological approach to vector control, Humphrey Mazigo and co-researchers tested malaria mosquito control in rice paddy farms using biolarvicide mixed with fertilizer in Tanzanian semi-field experiments. The intervention sections (with biolarvicide) had lowest mean mosquito larvae abundance compared to control block and did not affect the rice production/harvest.
Prawns to the Rescue in Senegal Fighting Schistosomiasis and Poverty
Anne Gulland reported how Christopher M. Hoover et al. discovered how prawns could be the key to fighting poverty and schistosomiasis, a debilitating tropical disease. They found that farming the African river prawn could fight the disease and improve the lives of local people, because the African river prawn is a ‘voracious’ predator of the freshwater snail, which is a carrier of schistosomiasis.
The researchers in Senegal said that, “market analysis in Senegal had shown there was significant interest among restaurant owners and farmers in introducing prawns to the diet.” The prawn could also for the basis of aquaculture in rice paddies and remove the threat of schistosomiasis from the rice workers.
—- Thank you for reading this week’s summary. These weekly abstractings have replaced our occasional mailings on tropical health issues due to fees introduced by those maintaining the listserve website. Also continue to check the Tropical Health Twitter feed, which you can see running on this page.
Borders &Diagnosis &Elimination &Environment &Gender &Health Education &Health Workers &Indoor Residual Spraying &IRS &ITNs &Mosquitoes &Plasmodium/Parasite &Vector Control Bill Brieger | 07 Jul 2019
The Weekly Tropical Health News 2019-07-06: Eliminating Malaria in Low Transmission Settings
This week started with articles that drew attention to the challenges of malaria in low transmission areas and with low density infections. Malaria Journal has provided several insightful articles toward this end.
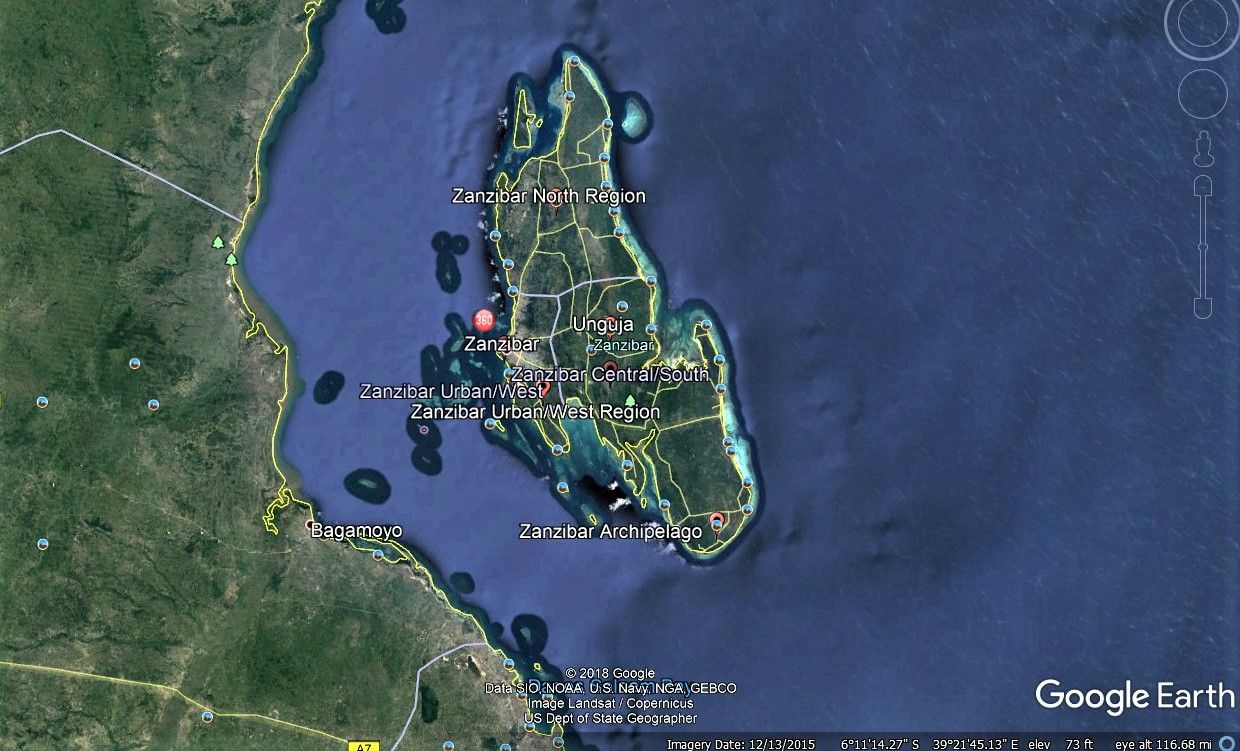 Being an island has certainly helped Zanzibar make progress toward malaria elimination as witness the fact that malaria prevalence has remained below 1% for the past decade. Not only does Zanzibar still face threats of infection from the mainland, it may also experience an upsurge locally if residual transmission and the role of human behavior and community actions are not well understood. April Monroe et al. conducted in-depth interviews with community members and local leaders across six sites on Unguja, Zanzibar as well as semi-structured community observations of night-time activities and special events to learn more.
Being an island has certainly helped Zanzibar make progress toward malaria elimination as witness the fact that malaria prevalence has remained below 1% for the past decade. Not only does Zanzibar still face threats of infection from the mainland, it may also experience an upsurge locally if residual transmission and the role of human behavior and community actions are not well understood. April Monroe et al. conducted in-depth interviews with community members and local leaders across six sites on Unguja, Zanzibar as well as semi-structured community observations of night-time activities and special events to learn more.
While there was high reported ITN use, there were also times when people were exposed t mosquitoes while being outdoors during biting times. This could be around the house, or at special night events like such as weddings, funerals, and religious ceremonies. Men spent more time outdoors than women. Clearly appropriate interventions and needed and should be promoted in culturally appropriate ways in order to further reduce and eventually eliminate transmission.
Angela Early and colleagues presented findings on a diagnostic process of deep sequencing for understanding the dynamics and complexity of Plasmodium infections, but stress that knowing the lower limit of detection is challenging. They present “a new amplicon analysis tool, the Parallel Amplicon Sequencing Error Correction (PASEC) pipeline, is used to evaluate the performance of amplicon sequencing on low-density Plasmodium DNA samples.”
The authors learned that, “four state-of-the-art tools resolved known haplotype mixtures with similar sensitivity and precision.” They also cautioned that, “Samples with very low parasitemia and very low read count have higher false positive rates and call for read count thresholds that are higher than current default recommendations.” Better understanding of the genetic mix of plasmodium infections as countries move toward low transmission and elimination is crucial for selecting appropriate interventions and evaluating their outcomes.
 Hannah Edwards and co-researchers examined conditions for malaria transmission along the Thailand-Myanmar border in areas approaching malaria elimination. While prevalence may be less than 1%, residual transmission still occurs. Transmission occurs not only around residences but in the forests where people work. The researchers therefore looked at the behavior of both humans and insects. Overall, they found that, “Community members frequently stayed overnight at subsistence farm huts or in the forest. Entomological collections showed higher biting rates of primary vectors in forested farm hut sites and in a more forested village setting compared to a village with clustered housing and better infrastructure.”
Hannah Edwards and co-researchers examined conditions for malaria transmission along the Thailand-Myanmar border in areas approaching malaria elimination. While prevalence may be less than 1%, residual transmission still occurs. Transmission occurs not only around residences but in the forests where people work. The researchers therefore looked at the behavior of both humans and insects. Overall, they found that, “Community members frequently stayed overnight at subsistence farm huts or in the forest. Entomological collections showed higher biting rates of primary vectors in forested farm hut sites and in a more forested village setting compared to a village with clustered housing and better infrastructure.”
While mosquitoes preferred to bite inside huts, their threat was magnified by those who did not use long lasting insecticide-treated nets (LLINs). While out in the farms and forests, people tended to wake early and increase their likelihood of being bitten. The authors discuss the challenges of dual residences in terms of LLIN ownership and even concerning the potential access to indoor residual spraying. The definition for universal net coverage needs to expand from one net per two people to include adequate nets wherever people are located.
 The Amazonian area of Brazil is another area working toward malaria elimination, in particular, Plasmodium vivax. Felipe Leão Gomes Murta et al. also looked at the human side of the equation and identified misperceptions by both community members and health workers that could inhibit elimination efforts. They found, “many myths regarding malaria transmission and treatment that may hinder the sensitization of the population of this region in relation to the use of current control tools and elimination strategies, such as mass drug administration (MDA),” and LLINs.
The Amazonian area of Brazil is another area working toward malaria elimination, in particular, Plasmodium vivax. Felipe Leão Gomes Murta et al. also looked at the human side of the equation and identified misperceptions by both community members and health workers that could inhibit elimination efforts. They found, “many myths regarding malaria transmission and treatment that may hinder the sensitization of the population of this region in relation to the use of current control tools and elimination strategies, such as mass drug administration (MDA),” and LLINs.
Problematic perceptions included mention by both groups that the use of insecticide-treated nets, may cause skin irritations and allergies. Both community members and health professionals said malaria is “an impossible disease to eliminate because it is intrinsically associated with forest landscapes.” They concluded that such perceptions can be a barrier to control and elimination.
Efforts to eliminate malaria from low transmission settings are an essential to the overall global goals. These four articles tell us that close attention to and better understanding of humans, parasites and mosquitoes is still needed to achieve these goals.
Children &Equity &IPTp &ITNs &Nigeria &Treatment Bill Brieger | 02 Jul 2019
Nigeria’s 2018 Demographic and Health Survey: Malaria Situation
 The Demographic and Health Survey for 2018 in Nigeria has released preliminary findings. These cover insecticide Treated Nets (ITNs), Intermittent Preventive Treatment of malaria in pregnancy (IPTp), and treatment of children with Artemisinin-Based Combination Therapy (ACT).
The Demographic and Health Survey for 2018 in Nigeria has released preliminary findings. These cover insecticide Treated Nets (ITNs), Intermittent Preventive Treatment of malaria in pregnancy (IPTp), and treatment of children with Artemisinin-Based Combination Therapy (ACT).
The key findings have been converted into graphs. We can see that ITN ownership by a household (HH) is greater in rural areas, but overall reaches only a national average of 60% of households having at least one net. People may recall that the 2010 target by the Roll Back malaria Partnership was 80% for all key indicators with the hope that by attaining and then maintaining 80% coverage or more, malaria incidence would drop and elimination would be on the horizon.
Nigeria is not among WHO’s Elimination by 2020 (E2020) countries, and it is not clear when transmission will move i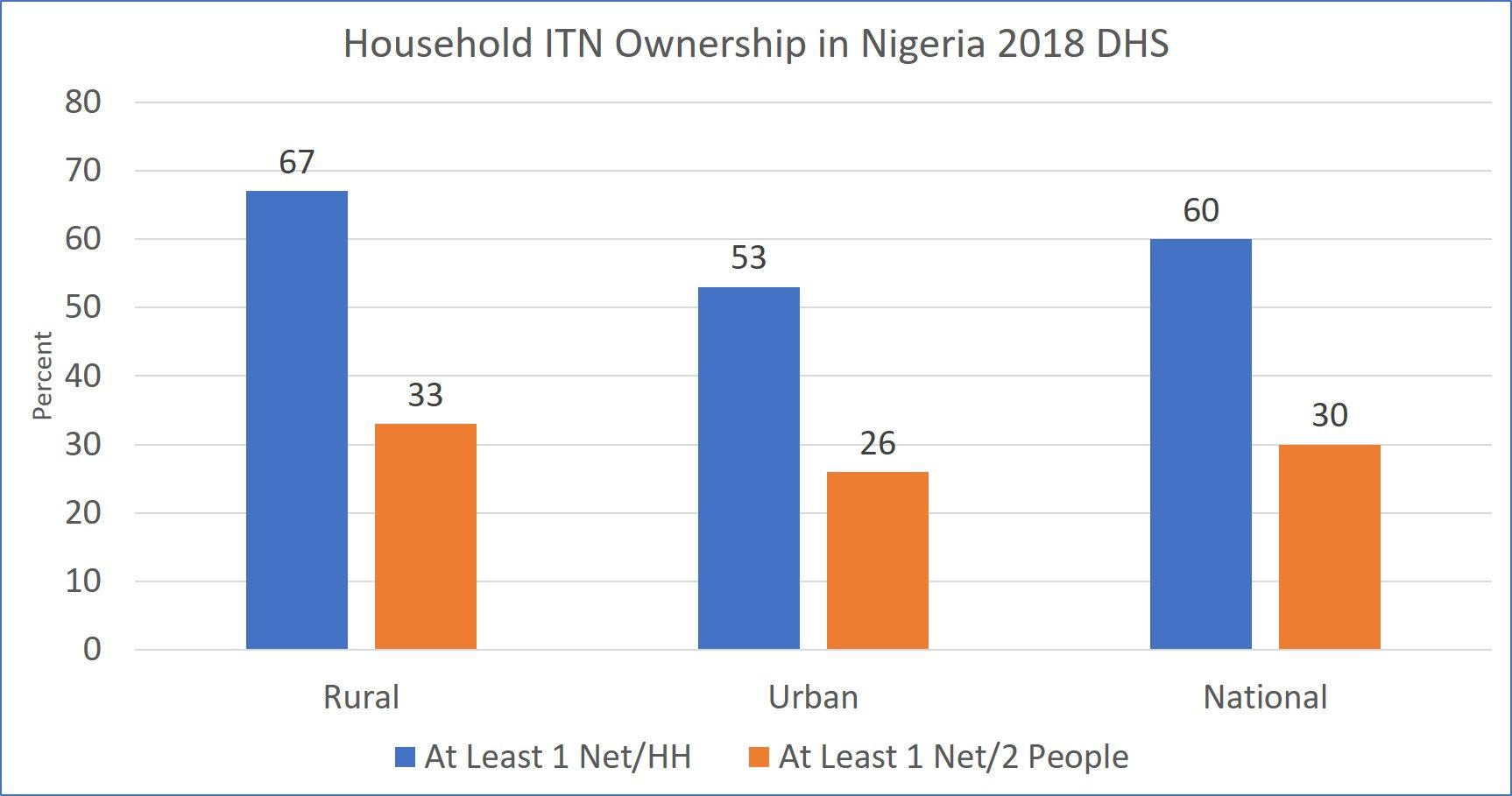 n that direction when key interventions are still not reaching targets. This is due also to the fact that 60% of households covered does not mean that residents are protected. In fact only 30% meet the goal of universal net coverage with at least one net for every two household members.
n that direction when key interventions are still not reaching targets. This is due also to the fact that 60% of households covered does not mean that residents are protected. In fact only 30% meet the goal of universal net coverage with at least one net for every two household members.
On the positive side, comparison of household net ownership and we alth status appears to favor the poorer households. 72% of the poorest households have at least one net compared to 48% of the highest income quintile. Unfortunately the gap between rich and poor narrows when it comes to the target of 1 net for 2 people.
alth status appears to favor the poorer households. 72% of the poorest households have at least one net compared to 48% of the highest income quintile. Unfortunately the gap between rich and poor narrows when it comes to the target of 1 net for 2 people.
Although these days we stress universal coverage of all household members, DHS still collects data on what are often termed ‘vulnerable’ groups, children below the age of 5 years and pregnant women. Just over half of each group slept under an ITN the night before the survey. It is obvious that access plays a role, so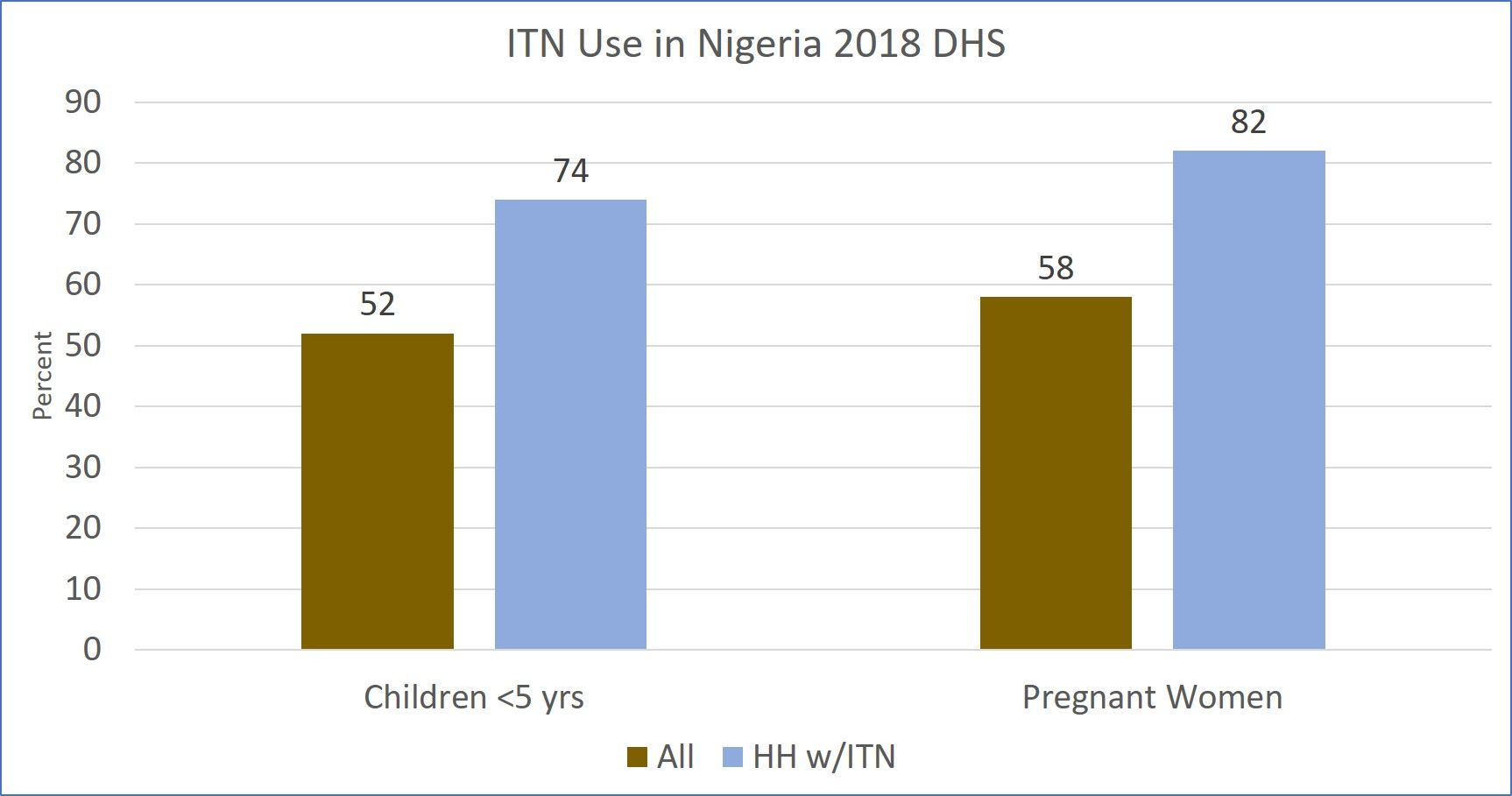 in those households that actually own at least one net 74% of children and 82% of pregnant women slept under an ITN. These figures might even be higher if the target of 1 net per two people were met.
in those households that actually own at least one net 74% of children and 82% of pregnant women slept under an ITN. These figures might even be higher if the target of 1 net per two people were met.
Nigeria is a huge and diverse country in terms of geography, epidemiology and ethncity. The country has 6 regions that are used for planning and analysis pur poses. The map attached shows that there are major regional variations in households owning at least one net and households having at least one net for every 2 people residing there.
poses. The map attached shows that there are major regional variations in households owning at least one net and households having at least one net for every 2 people residing there.
There is better coverage of at least one net per household in the northern zones than the southern, with the Northwest achieving 86% and then 42% for covering two people with one net. When it comes to that latter measure, the remaining 5 regions are all in the 20% level, meaning that for most of the country, there is a long way to go to achieve universal net coverage.
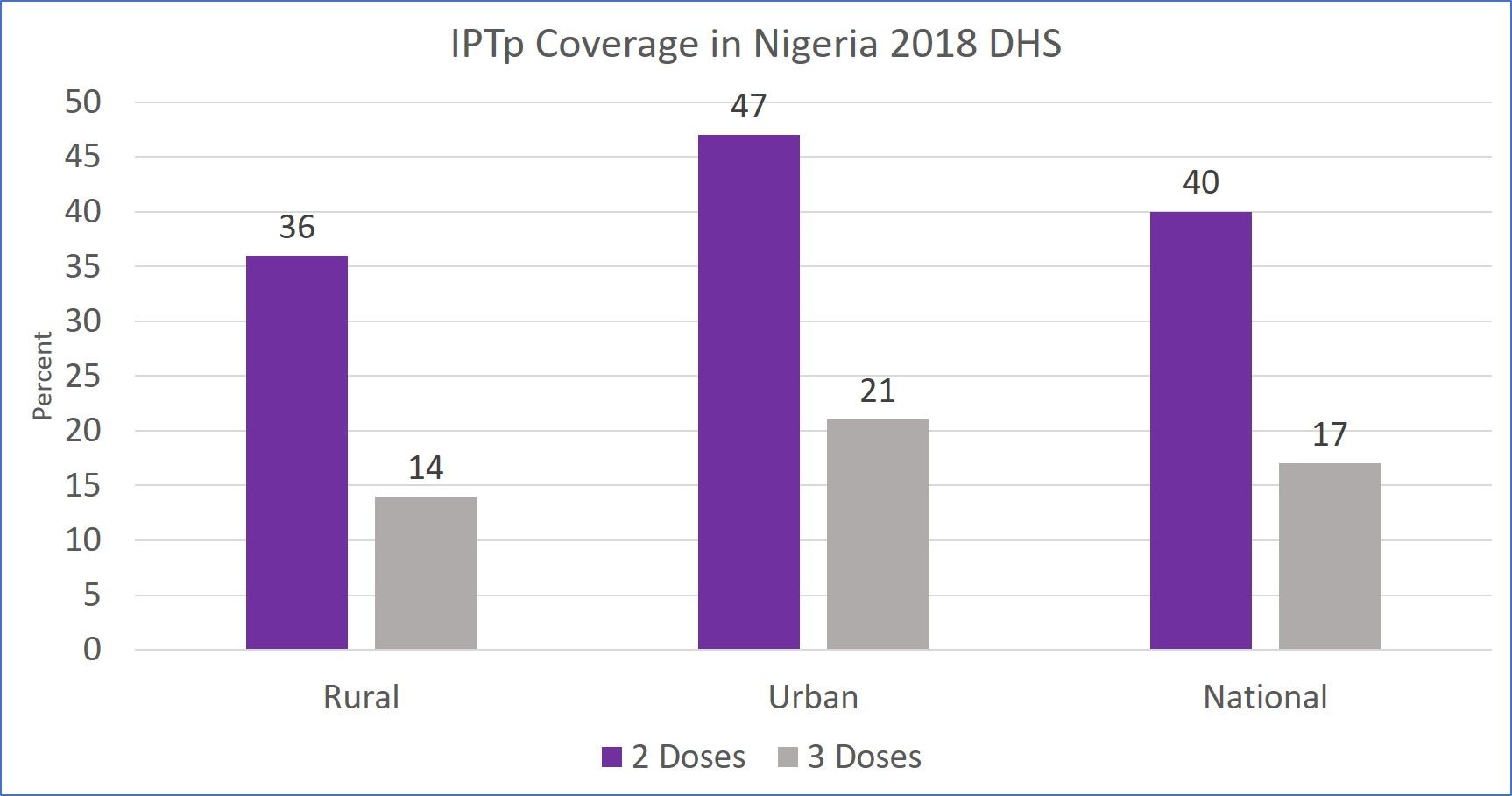 Intermittent preventive treatment of pregnant women with sulphadoxine-pyrimethamine (SP) has been a long standing intervention to protect women and their unborn children from the devastating effects of malaria. For at least six years now, WHO has recommended that pregnant women take three or more monthly doses of IPTp from the 13th week of pregnancy, onward.
Intermittent preventive treatment of pregnant women with sulphadoxine-pyrimethamine (SP) has been a long standing intervention to protect women and their unborn children from the devastating effects of malaria. For at least six years now, WHO has recommended that pregnant women take three or more monthly doses of IPTp from the 13th week of pregnancy, onward.
A challenge to getting IPTp is contact with antenatal care services, and only 67% of women who delivered a child in the 5 year preceding the survey attended ANC even once. Not surprisingly, only 40% of those pregnant women received two doses of IPTp and only 17% got three doses.
Finally, only 28% of children with fever in the two weeks prior to the survey took ACT, although we are not certain about the proportion who had been tested. It is difficult to interpret this finding since we do not know what proportion of those with fever might have been tested and found to harbor malaria parasites. ACTs should only be given to those with positive parasitological tests.
DHS and its sister survey, the Malaria Indicator Survey are performed at approximately three-year intervals. These data sources are valuable for evaluating past interventions and planning new. Clearly some serious planning is needed to address the shortfalls in malaria intervention coverage and save more lives.
Asymptomatic &Burden &Dengue &Diagnosis &Ebola &Elimination &Epidemiology &Health Systems &ITNs &MDA &Mosquitoes &NTDs &Schistosomiasis &Schools &Vector Control &Zoonoses Bill Brieger | 30 Jun 2019
The Weekly Tropical Health News 2019-06-29
Below we highlight some of the news we have shared on our Facebook Tropical Health Group page during the past week.
Polio Persists
If all it took to eradicate a disease was a well proven drug, vaccine or technology, we would not be still reporting on polio, measles and guinea worm, to name a few. In the past week Afghanistan reported 2 wild poliovirus type 1 (WPV1) cases, and Pakistan had 3 WPV1 cases. Circulating vaccine-derived poliovirus type 2 (cVDPV2) was reported in Nigeria (1), DRC (4) and Ethiopia (3) from healthy community contacts.
Continued Ebola Challenges
In the seven days from Saturday to Friday (June 28) there were 71 newly confirmed Ebola Cases and 56 deaths reported by the Democratic Republic of Congo’s Ministry of Health. As Ebola cases continue to pile up in the Democratic Republic of the Congo (DRC), with 12 more confirmed Thursday and 7 more Friday, a USAID official said four major donors have jump-started a new strategic plan for coordinating response efforts. To underscore the heavy toll the outbreak has caused, among its 2,284 cases, as noted on the World Health Organization Ebola dashboard today, are 125 infected healthcare workers, including 2 new ones, DRC officials said.
Pacific Standard explained the differences in Ebola outbreaks between DRC today and the West Africa outbreak of 2014-16. On the positive side are new drugs used in organized trials for the current outbreak. The most important factor is safe, effective vaccine that has been tested in 2014-16, but is now a standard intervention in the DRC. While both Liberia and Sierra Leone had health systems and political weaknesses as post-conflict countries, DRC’s North Kivu and Ituri provinces are currently a war zone, effectively so for the past generation. Ebola treatment centers and response teams are being attacked. There are even cultural complications, a refusal to believe that Ebola exists. So even with widespread availability of improved technologies, teams may not be able to reach those in need.
To further complicate matters in the DRC, Doctors Without Borders (MSF) “highlighted ‘unprecedented’ multiple crises in the outbreak region in northeastern DRC. Ebola is coursing through a region that is also seeing the forced migration of thousands of people fleeing regional violence and is dealing with another epidemic. Moussa Ousman, MSF head of mission in the DRC, said, ‘This time we are seeing not only mass displacement due to violence but also a rapidly spreading measles outbreak and an Ebola epidemic that shows no signs of slowing down, all at the same time.’”
NIPAH and Bats
Like Ebola, NIPAH is zoonotic, and also involves bats, but the viruses differ. CDC explains that, “Nipah virus (NiV) is a member of the family Paramyxoviridae, genus Henipavirus. NiV was initially isolated and identified in 1999 during an outbreak of encephalitis and respiratory illness among pig farmers and people with close contact with pigs in Malaysia and Singapore. Its name originated from Sungai Nipah, a village in the Malaysian Peninsula where pig farmers became ill with encephalitis.
A recent human outbreak in southern India has been followed up with a study of local bats. In a report shared by ProMED, out of 36 Pteropus species bats tested for Nipah, 12 (33%) were found to be positive for anti-Nipah bat IgG antibodies. Unlike Ebola there are currently no experimental drugs or vaccines.
Climate Change and Dengue
Climate change is expected to heighten the threat of many neglected tropical diseases, especially arboviral infections. For example, the New York Times reports that increases in the geographical spread of dengue fever. Annually “there are 100 million cases of dengue infections severe enough to cause symptoms, which may include fever, debilitating joint pain and internal bleeding,” and an estimated 10,000 deaths. Dengue is transmitted by Aedes mosquitoes that also spread Zika and chikungunya. A study, published Monday in the journal Nature Microbiology, found that in a warming world there is a strong likelihood for significant expansion of dengue in the southeastern United States, coastal areas of China and Japan, as well as to inland regions of Australia. “Globally, the study estimated that more than two billion additional people could be at risk for dengue in 2080 compared with 2015 under a warming scenario.”
Schistosomiasis – MDA Is Not Enough, and Neither Are Supplementary Interventions
Schistosomiasis is one of the five neglected tropical diseases (NTDs) that are being controlled and potentially eliminated through mass drug administration (MDA) of preventive chemotherapy (PCT), in this case praziquantel. In The Lancet Knopp et al. reported that biannual MDA substantially reduced Schistosomiasis haematobium prevalence and infection intensity but was insufficient to interrupt transmission in Zanzibar. In addition, neither supplementary snail control or behaviour change activities did not significantly boost the effect of MDA. Most MDA programs focus on school aged children, and so other groups in the community who have regular water contact would not be reached. Water and sanitation activities also have limitations. This raises the question about whether control is acceptable for public health, or if there needs to be a broader intervention to reach elimination?
Trachoma on the Way to Elimination
Speaking of elimination, WHO has announced major “sustained progress” on trachoma efforts. “The number of people at risk of trachoma – the world’s leading infectious cause of blindness – has fallen from 1.5 billion in 2002 to just over 142 million in 2019, a reduction of 91%.” Trachoma is another NTD that uses the MDA strategy.
The news about NTDs from Dengue to Schistosomiasis to Trachoma is complicated and demonstrates that putting diseases together in a category does not result in an easy choice of strategies. Do we control or eliminate or simply manage illness? Can our health systems handle the needs for disease elimination? Is the public ready to get on board?
Malaria Updates
And concerning being complicated, malaria this week again shows many facets of challenges ranging from how to recognize and deal with asymptomatic infection to preventing reintroduction of the disease once elimination has been achieved. Several reports this week showed the particular needs for malaria intervention ranging from high burden areas to low transmission verging on elimination to preventing re-introduction in areas declared free from the disease.
In South West, Nigeria Dokunmu et al. studied 535 individuals aged from 6 months were screened during the epidemiological survey evaluating asymptomatic transmission. Parasite prevalence was determined by histidine-rich protein II rapid detection kit (RDT) in healthy individuals. They found that, “malaria parasites were detected by RDT in 204 (38.1%) individuals. Asymptomatic infection was detected in 117 (57.3%) and symptomatic malaria confirmed in 87 individuals (42.6%).
Overall, detectable malaria by RDT was significantly higher in individuals with symptoms (87 of 197/44.2%), than asymptomatic persons (117 of 338/34.6%)., p = 0.02. In a sub-set of 75 isolates, 18(24%) and 14 (18.6%) individuals had Pfmdr1 86Y and 1246Y mutations. Presence of mutations on Pfmdr1 did not differ by group. It would be useful for future study to look at the effect of interventions such as bednet coverage. While Southwest Nigeria is a high burden area, the problem of asymptomatic malaria will become an even bigger challenge as prevalence reduces and elimination is in sight.
Sri Lanka provides a completely different challenge from high burden areas. There has been no local transmission of malaria in Sri Lanka for 6 years following elimination of the disease in 2012. Karunasena et al. report the first case of introduced vivax malaria in the country by diagnosing malaria based on microscopy and rapid diagnostic tests. “The imported vivax malaria case was detected in a foreign migrant followed by a Plasmodium vivax infection in a Sri Lankan national who visited the residence of the former. The link between the two cases was established by tracing the occurrence of events and by demonstrating genetic identity between the parasite isolates. Effective surveillance was conducted, and a prompt response was mounted by the Anti Malaria Campaign. No further transmission occurred as a result.”
Bangladesh has few but focused areas of malaria transmission and hopes to achieve elimination of local transmission by 2030. A particular group for targeting interventions is the population of slash and burn cultivators in the Rangamati District. Respondents in this area had general knowledge about malaria transmission and modes of prevention and treatment was good according to Saha and the other authors. “However, there were some gaps regarding knowledge about specific aspects of malaria transmission and in particular about the increased risk associated with their occupation. Despite a much-reduced incidence of malaria in the study area, the respondents perceived the disease as life-threatening and knew that it needs rapid attention from a health worker. Moreover, the specific services offered by the local community health workers for malaria diagnosis and treatment were highly appreciated. Finally, the use of insecticide-treated mosquito nets (ITN) was considered as important and this intervention was uniformly stated as the main malaria prevention method.”
Kenya offers some lessons about low transmission areas but also areas where transmission may increase due to climate change. A matched case–control study undertaken in the Western Kenya highlands. Essendi et al. recruited clinical malaria cases from health facilities and matched to asymptomatic individuals from the community who served as controls in order to identify epidemiological risk factors for clinical malaria infection in the highlands of Western Kenya.
“A greater percentage of people in the control group without malaria (64.6%) used insecticide-treated bed nets (ITNs) compared to the families of malaria cases (48.3%). Low income was the most important factor associated with higher malaria infections (adj. OR 4.70). Houses with open eaves was an important malaria risk factor (adj OR 1.72).” Other socio-demographic factors were examined. The authors stress the need to use local malaria epidemiology to more effectively targeted use of malaria control measures.
The key lesson arising from the forgoing studies and news is that disease control needs strong global partnerships but also local community investment and adaptation of strategies to community characteristics and culture.
ITNs &Universal Coverage &Vector Control &Zero Malaria Bill Brieger | 25 Apr 2019
Zero Malaria Starts with Universal Coverage: Part 1 Nets
WHO says, “Malaria elimination and universal health coverage go hand in hand,” at a special event during the 72st World Health Assembly. To achieve zero malaria, the goal of involving everyone from the policy maker to the community member must have a focus on achieving universal health coverage (UHC) of all malaria interventions ranging from insecticide treated bednets (ITNs) to appropriate provision of malaria diagnostics and medicines. Many of the studies to date have focused on ITNs, which include long-lasting insecticide treated nets (LLINs), but nationwide monitoring through the Demographic and Health Surveys (DHS), the Malaria Indicator Surveys (MIS) and the Multi-Indicator Cluster Surveys (MICS).
UNICEF’s website provides a data repository that includes the most recent DHS, MIS and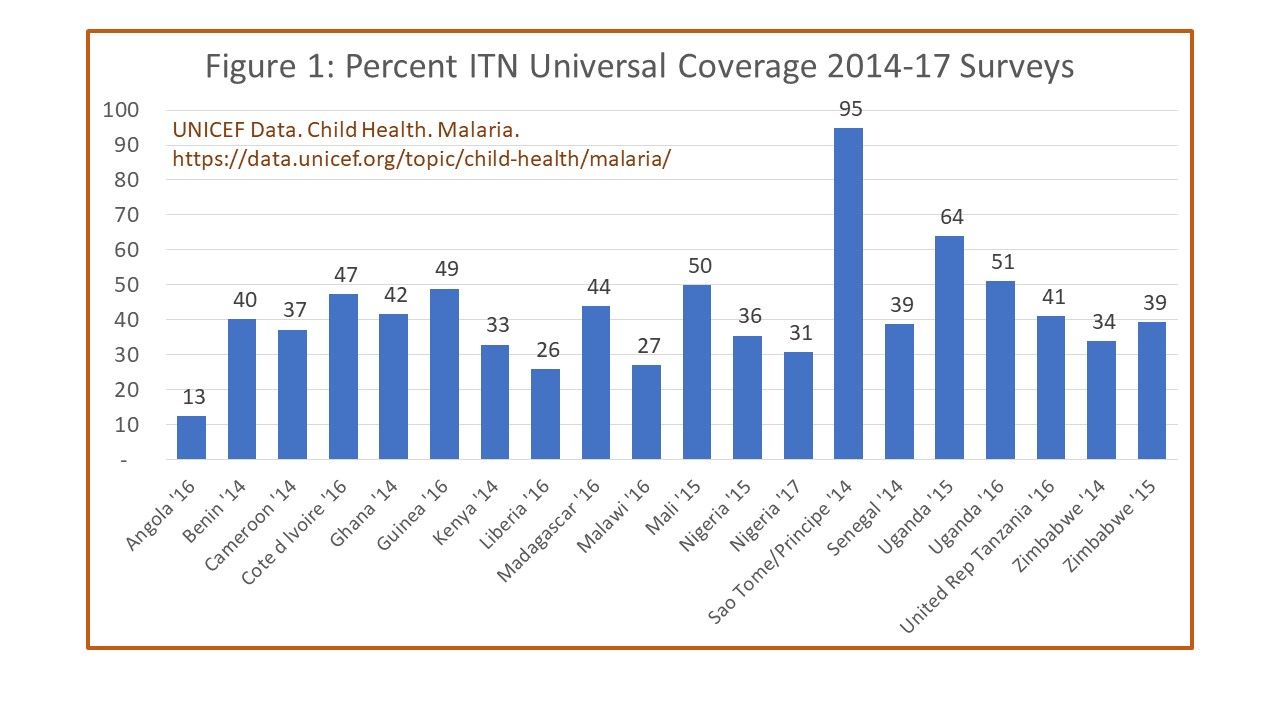 MICS survey data per country between 2014 and 2017. For the indicator of one ITN per to people in a household, shows Angola at only 13%, most countries for which recent data are available reached between 40-50%. Only two achieved above 60% on a point-in-time survey, Uganda at 62% and Sao Tome and Principe at 95%. The website shows information that where there were multiple surveys in a country during the period, there were variations, sometimes quite wide, over the years. Aside from the fact that the surveys may have had slightly different procedures, the problem remains of achieving and sustaining UHC for ITNs.
MICS survey data per country between 2014 and 2017. For the indicator of one ITN per to people in a household, shows Angola at only 13%, most countries for which recent data are available reached between 40-50%. Only two achieved above 60% on a point-in-time survey, Uganda at 62% and Sao Tome and Principe at 95%. The website shows information that where there were multiple surveys in a country during the period, there were variations, sometimes quite wide, over the years. Aside from the fact that the surveys may have had slightly different procedures, the problem remains of achieving and sustaining UHC for ITNs.
Another factor that affects maintaining UHC for ITNs, assuming the target can be met is the durability of nets. The physical integrity as well as the insecticide efficacy can decline over time. Intact nets may lose their insecticide through improper washing and drying, yet still prevent mosquito bites to the individual sleeping under them. Nets with holes may still maintain a minimal level of effective insecticide and may not fully prevent bites but ultimately kill the mosquito that flies through. Researchers in Senegal have been grappling with these challenges.
 Program managers must themselves grapple with whether such compromised nets count toward universal coverage as well as how often to conduct net replacement campaigns. A report from community surveys in Uganda during 2017 found that, “Long-lasting insecticidal net ownership and coverage have reduced markedly in Uganda since the last net distribution campaign in 2013/14.” UHC for ITNs is always a moving target.
Program managers must themselves grapple with whether such compromised nets count toward universal coverage as well as how often to conduct net replacement campaigns. A report from community surveys in Uganda during 2017 found that, “Long-lasting insecticidal net ownership and coverage have reduced markedly in Uganda since the last net distribution campaign in 2013/14.” UHC for ITNs is always a moving target.
A frequently unaddressed issue in seeking to improve ITN coverage is whether it makes a difference in malaria disease. A study in Malawi reported that although ITNs per household increased from 1.1 in 2012 to 1.4 in 2014, the prevalence of malaria in children increased over the period from 28% to 32%. The authors surmised that factors such as insecticide resistance, irregular ITN use and inadequate coordinated use of other malaria control interventions may have influenced the results. This shows that UHC for ITNs cannot be viewed in isolation.
This brings up the issue of the role of the many different vector control measures available. Researchers in Côte d’ Ivoire examined the use of eave nets and window screening. At present eave nets are mainly deployed in research contexts but use of window and door screening and netting are a commercially available interventions that households employ on their own. One wonders then whether UHC should focus on how the household and the people therein are protected by any malaria vector intervention.
 Here the discussion should focus on the question raised by colleagues in the USAID/PMI Vectorworks Project. WHO declared a goal of universal ITN coverage in 2009 using the target f one ITN/LLIN for every two household members. Vectorworks found that a decade on only one instance of a country briefly achieving 80% of this UHC net target, whereas no others reached above 60%. In fact, the bigger the household, the less chance there was of meeting the two people for one ITN target. Just because people live in a household that has the requisite number of nets, does not guarantee the actual target for sleeping under a net can be achieved because of practical or cultural realities in a household. Neither the minimal indicator of having at least one net in a household, or the ideal or ‘perfect’ indicator of UHC are satisfactory for judging population protection.
Here the discussion should focus on the question raised by colleagues in the USAID/PMI Vectorworks Project. WHO declared a goal of universal ITN coverage in 2009 using the target f one ITN/LLIN for every two household members. Vectorworks found that a decade on only one instance of a country briefly achieving 80% of this UHC net target, whereas no others reached above 60%. In fact, the bigger the household, the less chance there was of meeting the two people for one ITN target. Just because people live in a household that has the requisite number of nets, does not guarantee the actual target for sleeping under a net can be achieved because of practical or cultural realities in a household. Neither the minimal indicator of having at least one net in a household, or the ideal or ‘perfect’ indicator of UHC are satisfactory for judging population protection.
The Vectorworks team suggests that, “Population ITN access indicator is a far better indicator of ‘universal coverage’ because it is based on individual people,” and can be compared to, “The proportion of the population that used an ITN the previous night, which enables detailed analysis of specific behavioral gaps nationally as well as among population subgroups.” Population access to ITNs therefore, provides a batter basis for more realistic policies and strategies.
We have seen that defining as well as achieving universal coverage of malaria interventions is a challenging prospect. For example, do we base our monitoring on households or populations? Do we have the funds and technical capacity to implement and sustain the level of coverage required to have an impact on malaria transmission and move toward elimination? Are we able to introduce new, complimentary and appropriate interventions as a country moves closer to elimination?
A useful perspective would be determination if households and individuals even benefit from any part of the malaria package, even if everyone does not have access and utilize all components. This may be why zero malaria has to start with each person living in endemic areas.
Equity &ITNs Bill Brieger | 28 Feb 2019
Equity in Malaria Programming, the example of bednets
The WHO defines Equity as “the absence of avoidable, unfair, or remediable differences among groups of people, whether those groups are defined socially, economically, demographically or geographically or by other means of stratification. ‘Health equity’ or ‘equity in health’ implies that ideally everyone should have a fair opportunity to attain their full health potential and that no one should be disadvantaged from achieving this potential.”
WHO goes on to say that, “Countries and programs need to disaggregate selected health indicators by key stratifiers including demographic characteristics (gender, age), place of residence (urban/rural, subnational), socioeconomic status (wealth, education), as well as other characteristics (migrant/minority status etc.).”
 Writing for the Tropical Disease Research Program, H. Kristian Heggenhougen, Veronica Hackethal, and Pramila Vivek in the publication, The behavioural and social aspects of malaria and its control, say that …
Writing for the Tropical Disease Research Program, H. Kristian Heggenhougen, Veronica Hackethal, and Pramila Vivek in the publication, The behavioural and social aspects of malaria and its control, say that …
“What must now be clear is our conviction that any review of factors for world-wide malaria control must give specific attention to issues of socio-economic inequity and disease epidemiology.” Malaria is not an equal opportunity killer, but disproportionately affects certain segments of the population. Heggenhougen et al. continue that, “while we argue for a focused attack on malaria, we cannot avoid noting that without attention to these larger matters – inequity and marginalization – any improvement in health, including malaria, may be short-lived.”
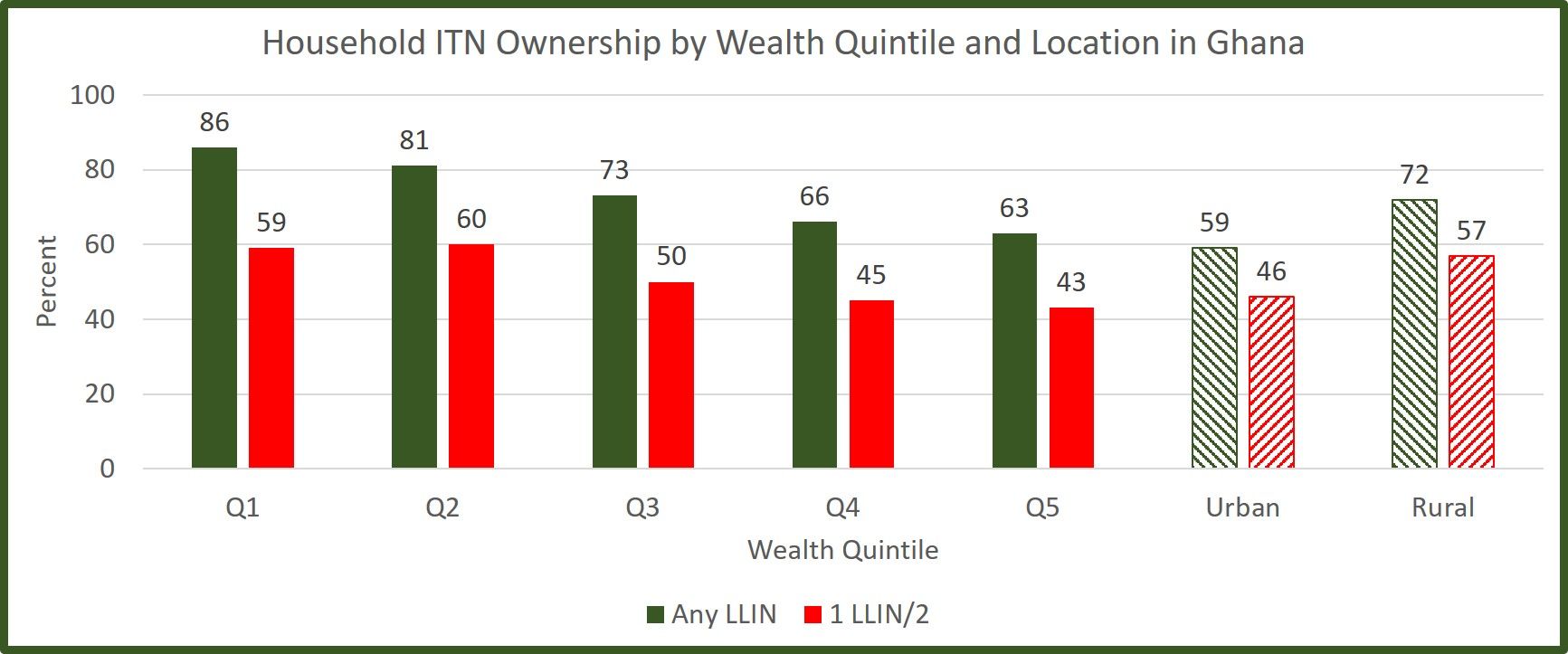 The Demographic and Health Survey (DHS) and its Malaria Indicator Survey (MIS) provide an important snapshot on equity issues in the rollout and coverage of major malaria. In particular, we look at the issue of long lasting insecticide-treated nets in two countries, Ghana (2016 MIS) and Liberia (2016 MIS), to demonstrate how equity issues can be seen. Two three measures are considered, wealth quintile, location (urban/rural) and gender/sex.
The Demographic and Health Survey (DHS) and its Malaria Indicator Survey (MIS) provide an important snapshot on equity issues in the rollout and coverage of major malaria. In particular, we look at the issue of long lasting insecticide-treated nets in two countries, Ghana (2016 MIS) and Liberia (2016 MIS), to demonstrate how equity issues can be seen. Two three measures are considered, wealth quintile, location (urban/rural) and gender/sex.
 In Ghana we see that having at least one net for the household is more common in lower income groups. These groups are more vulnerable. Although not specifically shown in the MIS, one might assume that people in the higher income groups have better quality housing that provides less opportunity for mosquito entry. Likewise households in rural areas, where anopheles are more likely to breed, have a higher proportion of nets. So while nets are not ‘equally distributed by these characteristics, they are more favorably available in those households that may be more vulnerable to malaria.
In Ghana we see that having at least one net for the household is more common in lower income groups. These groups are more vulnerable. Although not specifically shown in the MIS, one might assume that people in the higher income groups have better quality housing that provides less opportunity for mosquito entry. Likewise households in rural areas, where anopheles are more likely to breed, have a higher proportion of nets. So while nets are not ‘equally distributed by these characteristics, they are more favorably available in those households that may be more vulnerable to malaria.
When we look at the indicator of universal coverage where it is expected that there should be one net for every two household members, the proportion meeting that goal is much lower than simply having a net in the household for all groups. That said the pattern of higher proportions among rural and lower income groups remains. Within households, the Ghana MIS a nearly equal proportion of female (43%) and male (41%) had slept under a net the night prior to the survey.
 Overall, Liberia has much lower LLIN coverage than Ghana. The pattern for location is similar to that of Ghana, but for wealth, the poorest group (Q1) have lower coverage that wealth quintile groups 2-4. Also as in Ghana the Female (40%) and male (38%) are very similar.
Overall, Liberia has much lower LLIN coverage than Ghana. The pattern for location is similar to that of Ghana, but for wealth, the poorest group (Q1) have lower coverage that wealth quintile groups 2-4. Also as in Ghana the Female (40%) and male (38%) are very similar.
We encourage readers to review the recent MIS and/or DHS reports from the countries where they work and look for differences in net availability as well as uptake of other malaria control interventions to determine the level of equity in intervention access and use, but also as one sees in Liberia, take action to ensure that strategies are in place to reach the poorest and most vulnerable segment of society.