Asia &Elimination &Epidemiology &Mapping &Surveillance Bill Brieger | 19 Jul 2018
Pilot Mapping, Real Time Reporting and Responding in High Risk Malaria Areas of Viet Nam
 Viet Nam is among the Asia-Pacific countries focusing on eliminating malaria. Mapping helps target malaria interventions. Nguyen Xuan Thang and colleagues (James O’Donnell, Vashti Irani, Leanna Surrao, Ricardo Ataide, Josh Tram, An Le, Sara Canavati, Tran Thanh Duong, Tran Quoc Tuy, Gary Dahl, Gerard Kelly, Jack Richards, Ngo Duc Thang) presented their pilot mapping efforts at the Malaria World Congress in Melbourne recently and below share their experiences with us.
Viet Nam is among the Asia-Pacific countries focusing on eliminating malaria. Mapping helps target malaria interventions. Nguyen Xuan Thang and colleagues (James O’Donnell, Vashti Irani, Leanna Surrao, Ricardo Ataide, Josh Tram, An Le, Sara Canavati, Tran Thanh Duong, Tran Quoc Tuy, Gary Dahl, Gerard Kelly, Jack Richards, Ngo Duc Thang) presented their pilot mapping efforts at the Malaria World Congress in Melbourne recently and below share their experiences with us.
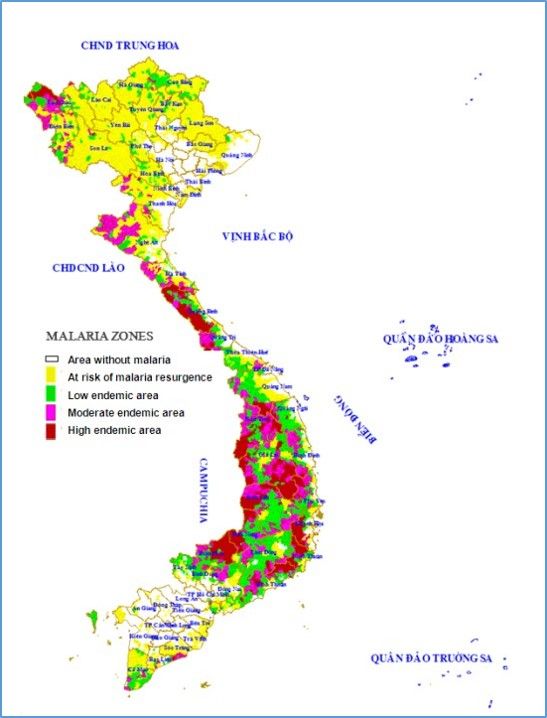
Viet Nam is focused on eliminating malaria by 2030. Viet Nam saw a 73% reduction in cases between 2013 and 2017 (NIMPE data), yet border provinces still have a high burden of malaria. However, some provinces still have a high burden of malaria. To achieve malaria elimination, it is essential to deploy targeted interventions in these locations.
 Spatial Decision Support Systems (SDSS) can be used by National Malaria programs to integrate geographic elements in the management of malaria cases and facilitate targeted malaria interventions in these high-risk settings.
Spatial Decision Support Systems (SDSS) can be used by National Malaria programs to integrate geographic elements in the management of malaria cases and facilitate targeted malaria interventions in these high-risk settings.
The objective of this work was to pilot a SDSS system for Binh Phuoc and Dak Nong Provinces in Viet Nam to facilitate ongoing surveillance and targeted malaria, as part of the Regional Artemisinin-resistance Initiative (RAI). This objective was achieved by:
-

Collecting data with cell phones
Collecting baseline GIS data at household level and environmental characteristics associated with the area;
- Establishing a routine data collection system that will be reported by mobile medical staff by mobile phone;
- Integrating this data to form a spatial decision support system (SDSS);
- Using the SDSS system for direct reporting to malaria control programs that provided strategic solutions for the prevention of disease spread and the elimination of malaria


Sample cell phone data screens
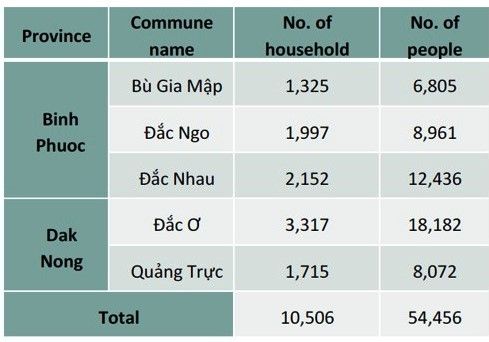
In Phase 1, a household and mapping survey was conducted in collaboration with commune, district and village health workers. Epicollect5 software was used on smartphones with GPS functionality to record mapping information (latitude and longitude) and general information on household members. During Phase 1, 10,506 households were surveyed and data was aggregated in a custom Geographic Information System (GIS) database.
 The majority of the surveyed individuals were of the Kinh ethnicity (19,282; 35.4%), followed by M’Nong (4,669; 8.6%) and Mong (3,359; 6.2%). Data related to malaria among mobile populations were included in the GIS as a means to identify and describe groups at high risk for malaria e.g. forest-goers. The survey data were reviewed, cleaned and matched using the ID numbers, then aggregated with relevant administrative boundary data and linked on ArcGIS 10.2 software. This database is located in a custom GIS system and can be visualized as a spatial transmission model to support appropriate decision-making
The majority of the surveyed individuals were of the Kinh ethnicity (19,282; 35.4%), followed by M’Nong (4,669; 8.6%) and Mong (3,359; 6.2%). Data related to malaria among mobile populations were included in the GIS as a means to identify and describe groups at high risk for malaria e.g. forest-goers. The survey data were reviewed, cleaned and matched using the ID numbers, then aggregated with relevant administrative boundary data and linked on ArcGIS 10.2 software. This database is located in a custom GIS system and can be visualized as a spatial transmission model to support appropriate decision-making

Dots representing households
Phase 2 focused on ongoing surveillance with rapid case reporting and responses. Malaria cases diagnosed at public and local health facilities were entered into the system by Commune Health Officials. Village Health Workers were immediately notified and went to the patient’s home to undertake case investigation including further household mapping and active case detection activities. The Viet Nam National Institute of Malariology was also notified, and organized local officials to carry out an investigation into the sources of transmission (i.e. ‘hotspots’) and to implement timely interventions.
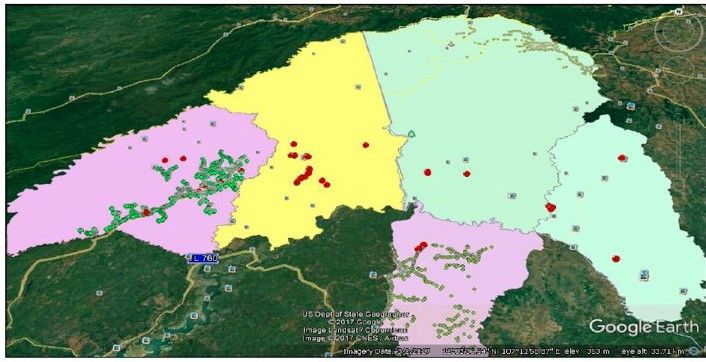
Dots representing cases
When the cases were identified, Village Health Workers went to the patient’s home to undertake operational procedures including geographic exploration, household mapping to identify the location and to identify the list of affected households. They also collected this data on EpiCollect5. Collated information on cases, transmission point, zoning of the target villages allowed for early detection of malaria outbreaks. The National Institute of Malariology can also issue guidelines when the hotspots are identified and when disease outbreaks occur
 These activities are ongoing. In conclusion, a custom GIS database was developed using a household survey in Binh Phuoc and Dak Nong province of Viet Nam. Malaria cases were mapped to identify hotspots of malaria transmission and enable further active case detection and targeted interventions. This established GIS database aims to support routine case notification and to enhance the role of surveillance for active case detection and responses to achieve malaria elimination.
These activities are ongoing. In conclusion, a custom GIS database was developed using a household survey in Binh Phuoc and Dak Nong province of Viet Nam. Malaria cases were mapped to identify hotspots of malaria transmission and enable further active case detection and targeted interventions. This established GIS database aims to support routine case notification and to enhance the role of surveillance for active case detection and responses to achieve malaria elimination.
The authors are affiliated with the National Institute of Malariology, Parasitology, Entomology (NIMPE), Viet Nam; Burnet Institute, Australia; and Health Poverty Action, UK. Contact: xuanthang.nimpe@gmail.com
Agriculture &Development &Epidemiology &Food Security &Integrated Vector Management &ITNs Bill Brieger | 25 May 2018
Agriculture and Promotion of Food Security Can Affect Malaria Transmission
The link between malaria and food security in a global context has been made. The influence of malaria on food security was examined. Now the connection between agriculture practices/food security and malaria is pursued below.
 A common complaint with programs that distribute insecticide-treated bednets to prevent malaria is that the nets may be used for other purposes that the intended effort to prevent infected mosquitoes from biting people. All informants interviewed for a study in Western Zambia reported that ITNs are regularly used for fishing and the misuse is widespread. Unsustainable fishing practices, drought and population pressure were mentioned as reasons for fishery decline. The implication was that the use of free ITNs for fishing at least saved the population money in a time of declining fortunes.
A common complaint with programs that distribute insecticide-treated bednets to prevent malaria is that the nets may be used for other purposes that the intended effort to prevent infected mosquitoes from biting people. All informants interviewed for a study in Western Zambia reported that ITNs are regularly used for fishing and the misuse is widespread. Unsustainable fishing practices, drought and population pressure were mentioned as reasons for fishery decline. The implication was that the use of free ITNs for fishing at least saved the population money in a time of declining fortunes.
A broader review of the ITNs for fishing issue was done through contacting expert witnesses across Africa. Mosquito net fishing (MNF) was found to be a broadly pan-tropical activity, particularly prevalent in sub-Saharan Africa. The authors found that, “Perceived drivers of MNF were closely related to poverty, revealing potentially complex and arguably detrimental livelihood and food security implications.”
 The mosquito breeding potential of dams cuts across Africa with the number of dams located in malarious areas projected to increase according to Kibret and colleagues. This is because “The population at risk of malaria around existing dams and associated reservoirs, is estimated to increase from 15 million in 2010 to 21-23 million in the 2020s, 25-26 million in the 2050s and 28-29 million in the 2080s.” In addition, areas with dams but without malaria transmission at present, will likely transition to regions of unstable transmission due to climate change.
The mosquito breeding potential of dams cuts across Africa with the number of dams located in malarious areas projected to increase according to Kibret and colleagues. This is because “The population at risk of malaria around existing dams and associated reservoirs, is estimated to increase from 15 million in 2010 to 21-23 million in the 2020s, 25-26 million in the 2050s and 28-29 million in the 2080s.” In addition, areas with dams but without malaria transmission at present, will likely transition to regions of unstable transmission due to climate change.
Likewise, a study in Ethiopia starts with the assertion that, “Dams are important to ensure food security and promote economic development in sub-Saharan Africa,” and then stresses the importance of understanding the consequences of these projects. The researchers found that “the mean monthly malaria incidence and anopheline larval density was generally higher in the dam villages than in the non-dam villages” in all the three dam settings studied. So while dams can increase agricultural production, the authors concluded that, “the presence of dams intensifies malaria transmission in lowland and midland ecological settings.”
 Hydro-agricultural projects include dams and irrigation. Human bait mosquito captures volunteers in hydro-agricultural and river bank sites in Cameroon Akono et al. found that mosquito biting rates were higher in hydro-agricultural sites of less urbanized and urban settings than in natural river banks sites. An additional implication is that urban farming, an important component of food security, may influence mosquito and malaria prevalence.
Hydro-agricultural projects include dams and irrigation. Human bait mosquito captures volunteers in hydro-agricultural and river bank sites in Cameroon Akono et al. found that mosquito biting rates were higher in hydro-agricultural sites of less urbanized and urban settings than in natural river banks sites. An additional implication is that urban farming, an important component of food security, may influence mosquito and malaria prevalence.
Stoler and colleagues pursued this question of urban agriculture. The odds of self-reported malaria are significantly higher for women in Accra, Ghana who are living within 1 km of urban agriculture compared with all women living near an irrigation source, the association disappearing beyond this critical distance. Likewise in Kumasi, Afrane et al. learned that “adult and larval mosquito abundance and larval survival were high in the irrigated fields in the irrigated (urban) vegetable farm. This therefore, contributed significantly to adult mosquito populations and hence malaria transmission in the city.”
Even agricultural practices in smaller subsistence farms can foster malaria mosquito breeding. Practices found in southwest Nigeria include collection of pools of water in the farms for soaking cassava tubers, digging of trenches, irrigation of farms, and the presence of fish ponds.
Communities can perceive how agricultural practices may contribute to malaria. In Tanzania a fair number of rural respondents associated growing of rice with malaria. They also noted that the need to sleep on their farms at times meant they could not benefit from the mosquito nets hanging back in their house, some hours walk away. The idea of rice cultivation and malaria was tested in central Kenya. Mwangangi and co-researchers found that, “Rice fields and associated canals were the most productive habitat types,” for malaria mosquito breeding. Overall, Mboera et al. found, “evidence that malaria transmission risk varies even between neighbouring villages and is influenced by agro-ecosystems.”
Although we can establish the two-way link or intersection between malaria and food security, we can see that recommended joint or integrated programming may not always be optimal at various levels from the nation to the community. Greater collaboration between health and agricultural ministries and agencies is needed, supported by national policies that see malaria and food production as part of overall national development goals.
CHW &Diagnosis &Elimination &Epidemiology Bill Brieger | 01 Apr 2018
Improving the efficacy of reactive screen-and-treat for malaria elimination in southern Zambia
Global Health Day 2018 sponsored by the Johns Hopkins University Center for Global Health featured a poster presentation by several colleagues on Improving the efficacy of reactive screen-and-treat for malaria elimination in southern Zambia. Fiona Bhondoekhan, William Moss, Timothy Shields, Douglas Norris, Kelly Searle, Jennifer Stevenson, Harry Hamapumba, Mukuma Lubinda and Japhet Matoba (Southern Africa International Centers of Excellence in Malaria Research, the JHU Bloomberg School of Public Health, and the Macha Research Trust, Zambia) share their findings below.
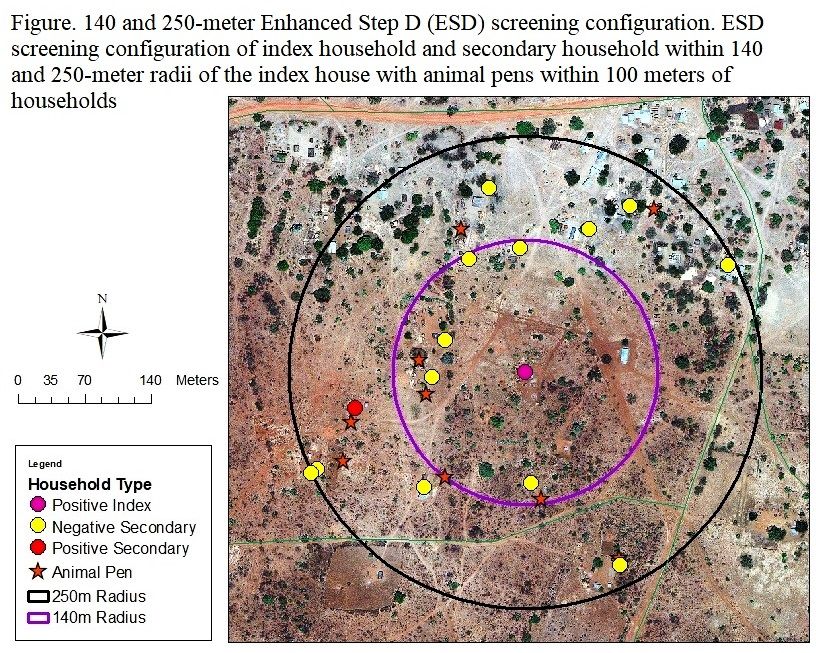 Background: Malaria screen-and-treat (called Step D in Zambia) is a reactive case detection strategy in which cases detected at a health center trigger community health workers (CHWs) to screen for secondary malaria cases within a 140-meter radius of the index case household using PfHRP2 rapid diagnostic tests (RDTs). Few studies evaluated whether an evidence-based strategy using environmental features that characterize the immediate surroundings of a household, can improve the efficiency of secondary case identification.
Background: Malaria screen-and-treat (called Step D in Zambia) is a reactive case detection strategy in which cases detected at a health center trigger community health workers (CHWs) to screen for secondary malaria cases within a 140-meter radius of the index case household using PfHRP2 rapid diagnostic tests (RDTs). Few studies evaluated whether an evidence-based strategy using environmental features that characterize the immediate surroundings of a household, can improve the efficiency of secondary case identification.
Objective: This study utilized the Step D and extended the screening radius to 250-meters (termed Enhanced Step D or ESD) to assess which local environmental variables can guide CHWs to identify secondary cases more efficiently. As Zambia works toward eliminating malaria, more refined and targeted case detection strategies are required to find the untreated malaria cases that could serve as potentially asymptomatic sources of infection. This study can help guide and plan reactive case detection strategies in Zambia that allow community health workers/field teams to employ an evidence-based strategy to find malaria-positive secondary households situated near index case houses more efficiently.
 Methods: Demographic information, malaria diagnosis, bed-net use and ownership, cooking energy source, and household floor material were obtained from surveys. Households were stratified into malaria positive and negative secondary households using RDT and qPCR results. ArcGIS was used to generate the following local environmental variables: screening radius (140 vs. 250-meters), number of animal pens within 100-meters, distance to nearest animal pen, distance and elevation difference between index and secondary houses, as well as the following large scale environmental variables: distance to main road and nearest stream category. Generalized estimating equations (GEE) estimated the cross-sectional effect for the difference in odds of a positive vs. negative secondary household for each predictor. For the secondary analysis GEE with the same model specifications was used to estimate the cross-sectional difference in odds of a positive vs. negative household for each environmental predictor. Model fit was evaluated with the Hosmer-Lemeshow goodness of fit test and significance was evaluated as a p-value of 0.05. Statistical analyses were carried out using STATA 14.2.
Methods: Demographic information, malaria diagnosis, bed-net use and ownership, cooking energy source, and household floor material were obtained from surveys. Households were stratified into malaria positive and negative secondary households using RDT and qPCR results. ArcGIS was used to generate the following local environmental variables: screening radius (140 vs. 250-meters), number of animal pens within 100-meters, distance to nearest animal pen, distance and elevation difference between index and secondary houses, as well as the following large scale environmental variables: distance to main road and nearest stream category. Generalized estimating equations (GEE) estimated the cross-sectional effect for the difference in odds of a positive vs. negative secondary household for each predictor. For the secondary analysis GEE with the same model specifications was used to estimate the cross-sectional difference in odds of a positive vs. negative household for each environmental predictor. Model fit was evaluated with the Hosmer-Lemeshow goodness of fit test and significance was evaluated as a p-value of 0.05. Statistical analyses were carried out using STATA 14.2.
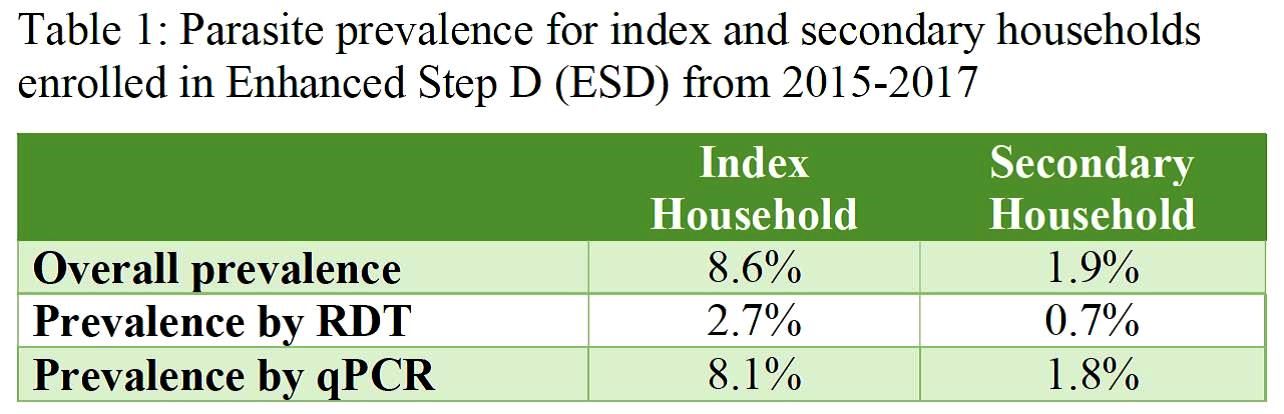
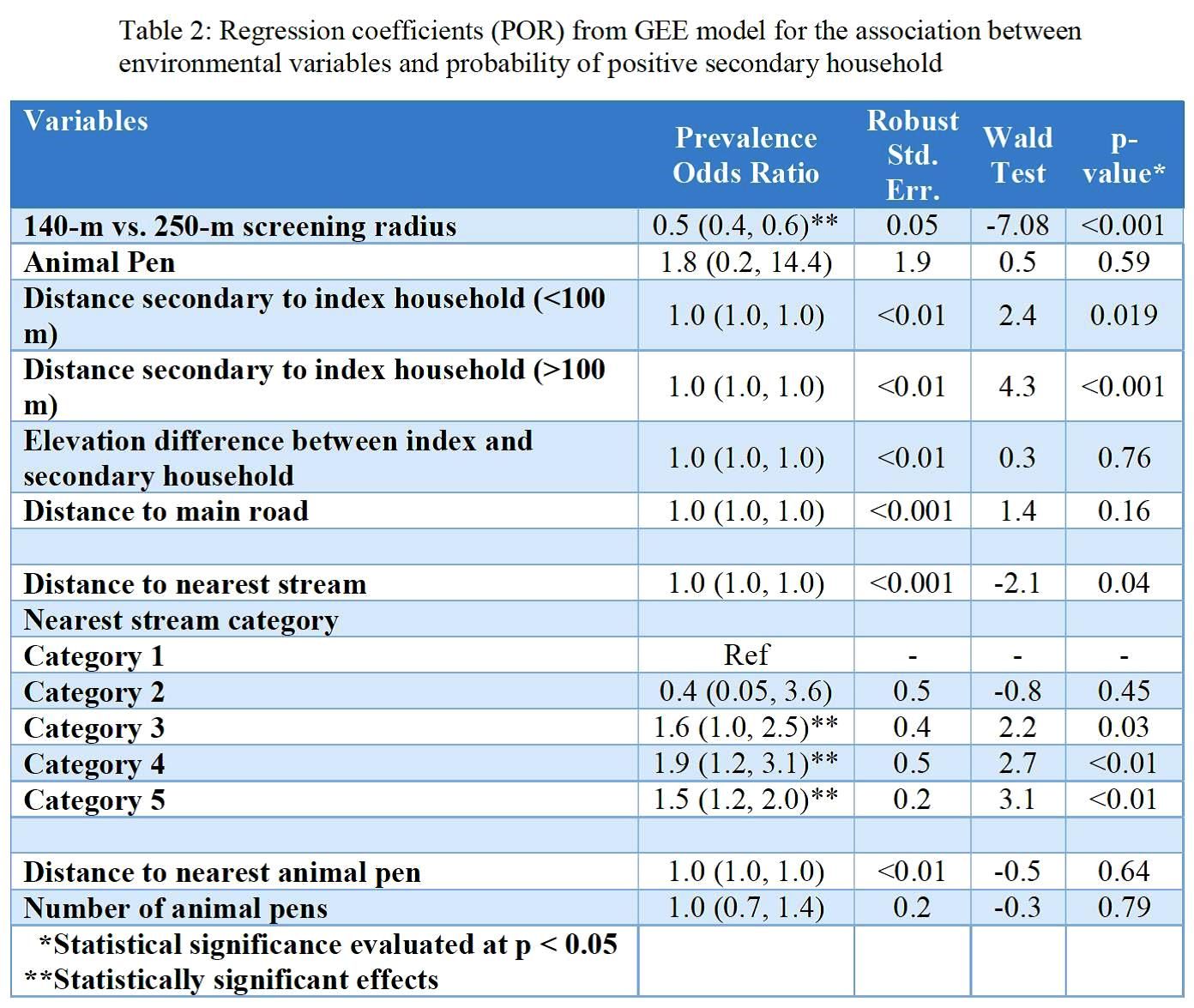 Results: Screening within the index households yielded an overall parasite prevalence of 8.6%, which was higher by qPCR (8.1%) than RDT (2.7%) as seen in Table 1. Secondary households had an overall parasite prevalence of 1.9% with similar differences by test used. Key results from regression analysis seen in Table 2 include a difference in prevalence according to screening radius as well as by proximity to the nearest stream. Secondary analysis produced similar results but showed statistically significant higher odds for households where animal pens were present.
Results: Screening within the index households yielded an overall parasite prevalence of 8.6%, which was higher by qPCR (8.1%) than RDT (2.7%) as seen in Table 1. Secondary households had an overall parasite prevalence of 1.9% with similar differences by test used. Key results from regression analysis seen in Table 2 include a difference in prevalence according to screening radius as well as by proximity to the nearest stream. Secondary analysis produced similar results but showed statistically significant higher odds for households where animal pens were present.
Conclusion: Screening for secondary households within low-transmission setting in Zambia could be optimized by using both local-scale indicators such as the presence of animal pens and large-scale indicators such as streams as environmental guiding tools.
Acknowledgements: This research was supported in part the Bloomberg Philanthropies and the Johns Hopkins Malaria Research Institute, and the NIH-sponsored Southern and Central Africa ICEMR 2U19AI089680.

Advocacy &Borders &Children &Conflict &Costs &Epidemiology &Funding &Human Resources &Leadership &Monitoring &Mortality &NTDs &Partnership &Surveillance Bill Brieger | 03 Feb 2018
African Leaders Malaria Alliance Recognizes Country Achievements, Adds NTDs to its Scorecard
 The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
 For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
The scorecard will now “report progress for the 47 NTD-affected countries in sub-Saharan Africa in their strategies to treat and prevent the five most common NTDs: lymphatic filariasis, onchocerciasis, schistosomiasis, soil-transmitted helminths and trachoma. By adding NTDs to the scorecard, African leaders are making a public commitment to hold themselves accountable for progress on these diseases.”
 In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
The combination is based on the logic that NTDs and malaria are both diseases of poverty. Malaria and several NTDs are also vector-borne. Also community platforms are a foundation for delivering needed drugs and supplies to tackle these diseases. Ultimately the decision shows that Heads of State are holding themselves accountable for progress in eliminating these diseases.
 At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
 The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
H.E . Dr. Barnabas Sibusiso Dlamini, the Prime Minister of the Kingdom of Swaziland, whose King and Head of State is the current chair of ALMA, warned all endemic countries that, “When we take our eyes off malaria, the cost for our countries is huge. Yet if we increase our efforts to control and eventually eliminate malaria, the yield we get from it is tremendous. It is time that we dig deep into our pockets and provide malaria programmes with the needed resources.”
 Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
IRIN concludes that, “For now, the biggest challenge for Zambia will be closing the gap in its malaria elimination strategy, which will cost around $160 million a year and is currently only about 50 percent funded – two thirds from international donors and one third from the Zambian government. Privately, international donors say the government must spend more money on its malaria programme if it is to succeed.” Cross-border transmission adds to the problem.
Internal strife is another challenge to malaria success. “The recent nurses’ strike which lasted for five months may have cost Kenya a continental award in reducing the prevalence of malaria during the 30th African Union Summit in Ethiopia on Sunday.” John Muchangi in the Star also noted that, “However, Kenya lost momentum last year and a major malaria outbreak during the prolonged nurses’ strike killed more than 30 people within two weeks in October.”
 Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Fortunately ALMA is equipped with the monitoring and advocacy tools to ensure that its members recognize and respond to such challenges. The Scorecards will keep the fight against the infectious diseases of poverty on track.
Case Management &Epidemiology &Malaria in Pregnancy Bill Brieger | 09 Dec 2017
Prof Lateef A Salako, 1935-2017, Malaria Champion
 Professor Lateef Akinola Salako was an accomplished leader in malaria and health research in Nigeria whose contributions to the University of Ibadan and the Nigeria Institute for Medical Research (among others) advanced the health of the nation, the region and the world. His scientific research and his over 140 scientific publications spanned five decades.
Professor Lateef Akinola Salako was an accomplished leader in malaria and health research in Nigeria whose contributions to the University of Ibadan and the Nigeria Institute for Medical Research (among others) advanced the health of the nation, the region and the world. His scientific research and his over 140 scientific publications spanned five decades.
His research not only added to knowledge but also served as a mentoring tool to junior colleagues. Some of his vast areas of interest in malaria ranged from malaria epidemiology, to testing the efficacy of malaria drugs to tackling the problem of malaria in pregnancy. He led a team from three research sites in Nigeria that documented care seeking for children with malaria the acceptability of pre-packaged malaria and pneumonia drugs for children that could be used for community case management. Prof Salako was also involved in malaria vaccine trials and urban malaria studies.
As recent as 2013 Prof Lateef Salako, formerly of NIMR said: “It is true there is a reduction in the rate of malaria cases in the country, but to stamp out this epidemic there is the urgent need for a synergy between researchers, the government, ministries, departments and agencies and involved in malaria control. That will enable coordinated activities that will produce quicker results than what obtains at the moment.”
At least one website has been set up where people can express their condolences. As one person wrote, “Professor Lateef Salako was an exceptional student, graduating with distinction from medical school; an unforgettable teacher, speaking as a beneficiary of his tutelage; an exemplary scholar, mentoring many others; an accomplished scientist, making indelible contributions to knowledge. May his legacy endure.”
Readers are also welcome to add their own comments here about Prof Salako’s contribution to malaria and tropical health.
Emergency &Epidemiology &Social/Cultural &Surveillance Bill Brieger | 17 Aug 2017
The Forest through the Trees: Themes in Social Production of Health
Recently Professor Ayodele S Jegede of the Faculty of Social Sciences, delivered the 419th Inaugural Lecture at the University of Ibadan, Ibadan, Nigeria, during the 2016/2017 academic session. Below Prof. Jegede shares an abstract of his lecture.

Prof Ayodele S Jegede
Knowledge of individual actor’s behaviour is a reflection of the society as tree to the forest. As forest produces large quantities of oxygen and takes in carbon dioxide, society produces the needed resources for human beings to survive through culture. This inter-dependence between man and the environment is summarised by the Yoruba adage which says: “irorun igi ni irorun eye” (meaning: a bird’s peace depends on the peace enjoyed by the tree which harbours it).
Nigeria, a country with a population of about 187 million and a life expectancy of 53 years, 54% of the populace are living below the poverty line with limited access to health care services physically and economically. Although universal health coverage is vital to the achievement of the Sustainable Development Goals (SDGs) cultural perception of disease aside from loss of economic and low purchasing power makes people to attribute their illnesses to spiritual cause and therefore seek alternative health care services. This influences resistance to public health interventions in some African communities resulting in suspicion and distrust between health educators and the public.

Strengthening Health Information Systems
For instance, response to childhood immunizable diseases, mental illness, malaria and HIV/AIDS reported in this lecture was driven by how people define the diseases. Their response did result in delay in seeking modern health care until alternative care sources proved ineffective. This confirms W.I. Thomas (1929: 572) postulation that, “If men define situations as real, they are real in their consequences”.
Our stakeholders’ engagement interventions strategies strengthened by knowledge of how people construct their life, socially and culturally, proved to be a potent vaccine for preventing strain relationship between health workers and clients. Since society consists of individuals who constitute the stakeholders conducting health researches as well as management of epidemics and treatment during epidemics and disease episodes require appropriate ethical behaviours.
This suggests that adequate knowledge of the society is inevitable since a tree does not make a forest which confirms Marx Weber’s Action Theory postulation that an act does not become social unless it involves two or more persons. It is, therefore, that government should establish National Disease Observatory System (NDOS) to document diseases by type, location and related local practices for training health care professionals, clinical practice and emergencies preparedness.
Note also that the lecture was featured in the New Nigerian Newspaper with an emphasis on establishing a national disease observatory. The Nigerian Tribune also featured the lecture stressing the importance of disease emergency preparedness.
Climate &Community &Development &Epidemiology &Malaria in Pregnancy &Mosquitoes &Surveillance &Urban &Zoonoses Bill Brieger | 11 Jul 2017
Population Health: Malaria, Monkeys and Mosquitoes
 On World Population Day (July 11) one often thinks of family planning. A wider view was proposed by resolution 45/216 of December 1990, of the United Nations General Assembly which encouraged observance of “World Population Day to enhance awareness of population issues, including their relations to the environment and development.”
On World Population Day (July 11) one often thinks of family planning. A wider view was proposed by resolution 45/216 of December 1990, of the United Nations General Assembly which encouraged observance of “World Population Day to enhance awareness of population issues, including their relations to the environment and development.”
A relationship still exists between family planning and malaria via preventing pregnancies in malaria endemic areas where the disease leads to anemia, death, low birth weight and stillbirth. Other population issues such as migration/mobility, border movement, and conflict/displacement influence exposure of populations to malaria, NTDs and their risks. Environmental concerns such as land/forest degradation, occupational exposure, population expansion (even into areas where populations of monkeys, bats or other sources of zoonotic disease transmission live), and climate warming in areas without prior malaria transmission expose more populati ons to mosquitoes and malaria.
ons to mosquitoes and malaria.
Ultimately the goal of eliminating malaria needs a population based focus. The recent WHO malaria elimination strategic guidance encourages examination of factors in defined population units that influence transmission or control.
Today public health advocates are using the term population health more. The University of Wisconsin Department of Population Health Sciences in its blog explained that “Population health is defined as the health outcomes of a group of individuals, including the distribution of such outcomes within the group.” World Population Day is a good time to consider how the transmission or prevention of malaria, or even neglected tropical diseases, is distributed in our countries, and which groups and communities within that population are most vulnerable.
World Population Day has room to consider many issues related to the health of populations whether it be reproductive health, communicable diseases or chronic diseases as well as the services to address these concerns.
Epidemiology &IPTp &ITNs &Malaria in Pregnancy &Morbidity &Treatment Bill Brieger | 26 Jun 2017
Burundi: when will citizens see real protection from malaria?
Preliminary findings from Burundi’s 2015-16 DHS have been made available. The country has a long way to go to meet targets for basic control of malaria.
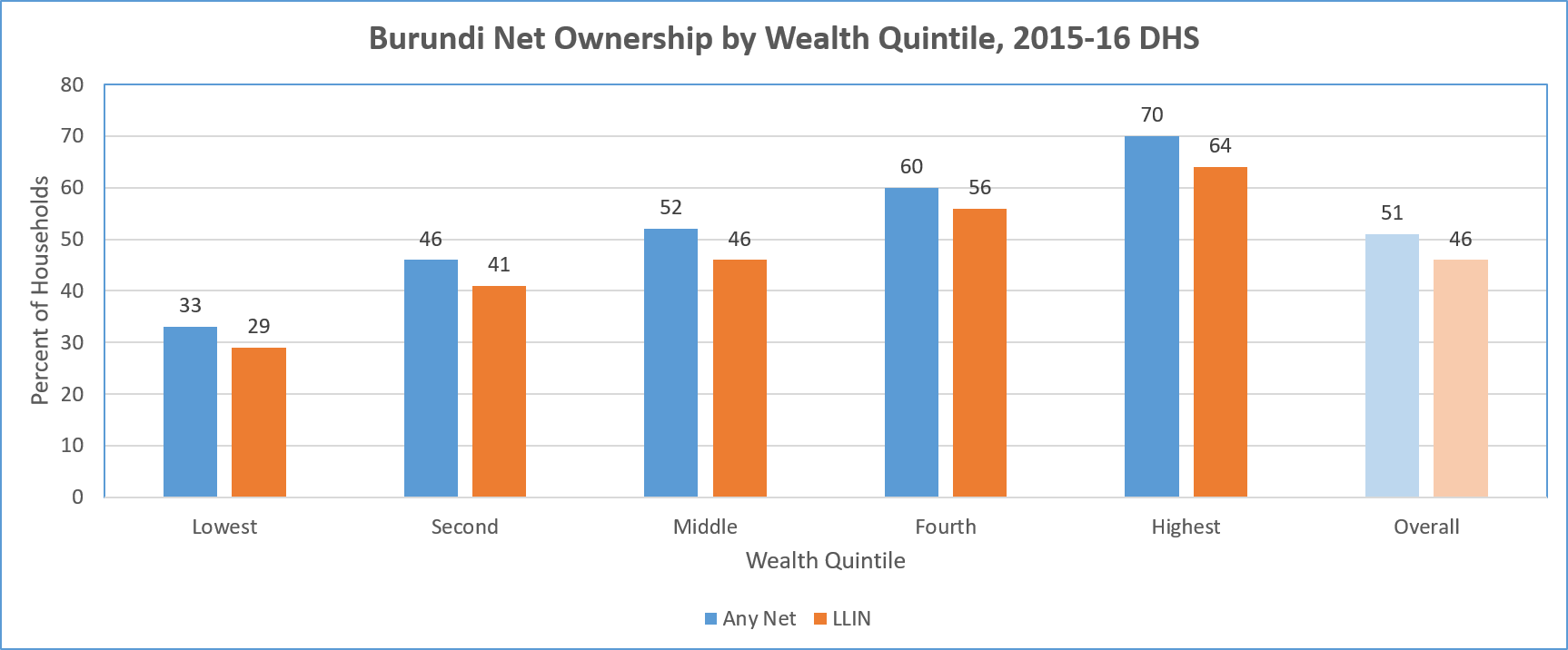 LLIN availability by household is an overall disappointing 32%. Ironically there is greater coverage of households in in urban areas (50%) than rural (30%). There is also great variation among the provinces with 52% coverage in Bujumbura metropolitan but only 19% in Canzuko. The overall average is less than one treated net per household.
LLIN availability by household is an overall disappointing 32%. Ironically there is greater coverage of households in in urban areas (50%) than rural (30%). There is also great variation among the provinces with 52% coverage in Bujumbura metropolitan but only 19% in Canzuko. The overall average is less than one treated net per household.
A major concern is equity. The chart above shows a steep gradation from 19% coverage among the lowest fifth of the wealth quintile, up to 48% in the highest. Even in households that have at least one net, only 17% of of people slept under a net the night before the survey.
In terms of use by those traditionally defined as vulnerable, the DHS shows only 40% of children below 5 years of age overall slept under a treated net the night prior to the survey. Even in households that own at least one net, 78% of these children slept under one.
A similar pattern is seen for treated net use by pregnant women. Overall 44% slept under a treated net, and 84% did so in households that owned at least one treated net. The internal household dynamics of net use where one is available does appear to favor these two groups.
Overall coverage of Intermittent Preventive Treatment for pregnant women is very low. Less than 30% of pregnant women received even the first dose of SP. This decreased to 21% for two doses and 13% for three. In contrast to net coverage, more rural women (31%) received the first dose of IPTp than urban ones (19%).
 Nearly 40% of children below five years of age were found to have had a fever in the two weeks preceding the survey. Among those care was sought for only two-thirds. Eleven percent of those with fever received an artemisinin-based combination therapy drug. The report did not mention whether these children had received any testing prior to treatment, so appropriateness of treatment cannot be judged. Prevalence testing of the children in the sample found 38% with parasitemia. Therefore one might assume that more children should have received ACTs.
Nearly 40% of children below five years of age were found to have had a fever in the two weeks preceding the survey. Among those care was sought for only two-thirds. Eleven percent of those with fever received an artemisinin-based combination therapy drug. The report did not mention whether these children had received any testing prior to treatment, so appropriateness of treatment cannot be judged. Prevalence testing of the children in the sample found 38% with parasitemia. Therefore one might assume that more children should have received ACTs.
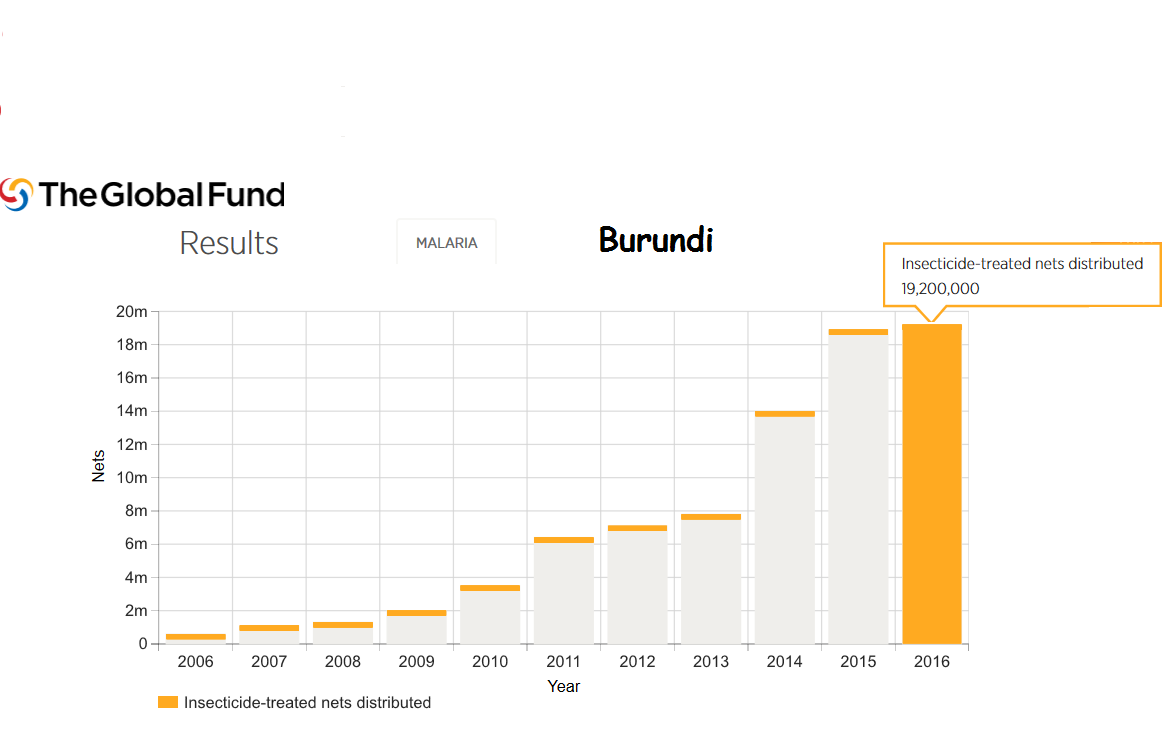
Burundi still faces major political and social challenges. Even so Burundi is the recipient of malaria support from the Global Fund. For example 18 million LLINs were distributed in 2015 and 19 million in 2016.
Much work is needed to bring Burundi even close to universal coverage of malaria interventions. In today’s climate of questionable donor commitment, it is hoped that regional partners may play a role since malaria knows no boundaries.
Blood Borne &Epidemiology Bill Brieger | 14 Jun 2017
Donate Blood, Not Malaria
 June 14th is World Blood Donor Day. This year’s theme stresses the importance of donating now before a disaster strikes. This requires good storage facilities (and strong systems) in countries where disasters may occur, which may not always be the case. We know that blood donation facilities are concerned about testing for infectious diseases like HIV and Hepatitis C. What of malaria?
June 14th is World Blood Donor Day. This year’s theme stresses the importance of donating now before a disaster strikes. This requires good storage facilities (and strong systems) in countries where disasters may occur, which may not always be the case. We know that blood donation facilities are concerned about testing for infectious diseases like HIV and Hepatitis C. What of malaria?
Studies have found that when people return to a non-endemic setting from malaria endemic countries, “Semi-immune individuals are more likely to transmit malaria as they may be asymptomatic” and serological data, not just circumstantial epidemiological information are also needed that if transmission through blood donations are to be prevented. There is also concern about the longevity of malaria infection depending on the species of Plasmodium in different parts of the world.
In endemic countries malaria antibodies can be present in basically all of asymptomatic adult blood donors. Unfortunately currently available screening assays appear unsuitable to minimize transfusion malaria.
Researchers in Brazil reported that, “The real-time PCR with TaqMan probes enabled the identification of P. vivax in a high proportion of clinically healthy donors, highlighting the potential risk for transfusion-transmitted malaria. Additionally, this molecular diagnostic tool can be adopted as a new laboratory screening method in haemotherapy centres, especially in malaria-endemic areas.”
Knowing the seasonal prevalence of malaria among blood donors in Bamako, Kouriba et al. suggest “A prevention strategy of transfusion malaria based on the combination of selection of blood donors through the medical interview, promoting a voluntary low-risk blood donation and screening all blood bags intended to be transfused” to vulnerable groups.
So while we recognize the life saving importance of adequate blood donations and supplies for transfusion, we also stress the importance of blood safety and expand our horizons to the possibility that malaria may be one of the potential problems shared with blood.
Elimination &Epidemiology &Funding &IPTp &ITNs &Procurement Supply Management &Treatment Bill Brieger | 20 May 2017
Ghana – spotlight on malaria indicators
 The Demographic and Health Surveys has released a brief on key indicators from the Ghana Malaria Indicator Survey of 2016. While much of the malaria community is discussing the elimination framework and processes, the reality is that many high burden countries are still trying to scale up basic interventions to achieve universal coverage.
The Demographic and Health Surveys has released a brief on key indicators from the Ghana Malaria Indicator Survey of 2016. While much of the malaria community is discussing the elimination framework and processes, the reality is that many high burden countries are still trying to scale up basic interventions to achieve universal coverage.
The overall prevalence across the country in children aged 6-59 months at the time of the survey was 27% using Rapid Diagnostic test and 20% using microscopy. Among children reporting fever in the previous two weeks care/advice was sought for only 72%. Although only only 30% received some sort of blood based diagnostic test, 61% of the febrile children were given the antimalarial artemisinin-based combination therapy drugs.
 Children are still being treated without the benefit of parasitological testing, a key procedure highlighted in WHO case management guidelines. Presumptive treatment for malaria without testing means that a child could inappropriately receive antimalarial drugs and die of another underlying febrile illness. Appropriate testing and adherence to test results is one of the main areas of focus of Ghana’s grants from the US President’s Malaria Initiative. Improved testing is also an important element in Ghana’s current Global Fund support. Clearly more value for money is needed from these inputs.
Children are still being treated without the benefit of parasitological testing, a key procedure highlighted in WHO case management guidelines. Presumptive treatment for malaria without testing means that a child could inappropriately receive antimalarial drugs and die of another underlying febrile illness. Appropriate testing and adherence to test results is one of the main areas of focus of Ghana’s grants from the US President’s Malaria Initiative. Improved testing is also an important element in Ghana’s current Global Fund support. Clearly more value for money is needed from these inputs.
Preventive measures as documented in the MIS fare somewhat better., but at present only 73% of households own an insecticide treated bednet. When considering the recommended 1 net for every 2 household members, the indicator drops to 50%. Concerning the typical ‘vulnerable’ populations, we see that only 52% of children below the age of 5 years slept under an ITN the night before the survey; only 50% of pregnant women did likewise.
 Malaria prevention in pregnancy results reflect the fact that Ghana has promoted at least three IPTp doses for around ten years. Most pregnant women (78% ) had received the previously recommended minimum of two doses, and now 60% have received at least three doses.
Malaria prevention in pregnancy results reflect the fact that Ghana has promoted at least three IPTp doses for around ten years. Most pregnant women (78% ) had received the previously recommended minimum of two doses, and now 60% have received at least three doses.
One of the important issues stressed in WHO’s new malaria elimination framework is stratifying the country by prevalence to the lowest level possible in order to plan appropriate interventions. Fortunately the Ghana 217 MIS key indicator brief does stratify prevalence and intervention coverage by region. Prevalence through RDT testing ranges from nearly 5% in the urbanized greater Accra area to 44% in the Central Region. Interestingly ITN use is nearly 20% higher in Central than greater Accra.
Hopefully future planning in Ghana will build on this stratification. Better mobilization of donor, national and private sector resources will address likely issues of stock-outs and increase the likelihood of universal coverage of basic interventions that is needed to move the country along the road to malaria elimination.