Burden &Epidemiology Bill Brieger | 14 Nov 2016
The Challenge of Reducing Malaria in Angola – High Transmission Provinces
Below is an abstract of a poster presentation today at the American Society of tropical Medicine 65th Annual meeting in Atlanta. The presentation was prepared by Jhpiego’s Angola team including Jhony Juarez, Margarita Gurdian-Sandoval, Julio Bonillo, and William R. Brieger. Please join us at the Late-breaker’s session at noon.
CONTEXT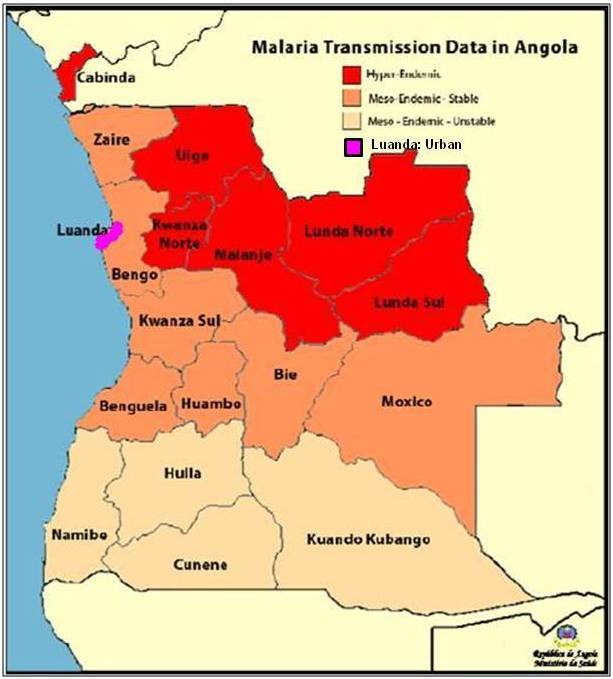
- Angola has three major belts of malaria transmission
- The north is high transmission and borders on the heavy burden country of the Democratic Republic of the Congo
- The mid-section of the country is meso-endemic
- The south is considered low endemic
- This low endemic area brings Angola into the Southern African Elimination 8 countries.
METHODS: Field visits were made to six northern high burden provinces. Health information system (HIS) data were collected from each provincial health department. Supplementary HIS information was collected from the national malaria control program
 FINDINGS: Data from the six high burden provinces reveal an overall upward trend in confirmed malaria. Cases from 2011, but with a jump of over 130,000 confirmed cases from 2014 to 2015. This occurred despite support from government and major malaria partners over the past decade. Overall cases in the country have risen from 2.73m in 2011 to 3.25m in 2015
FINDINGS: Data from the six high burden provinces reveal an overall upward trend in confirmed malaria. Cases from 2011, but with a jump of over 130,000 confirmed cases from 2014 to 2015. This occurred despite support from government and major malaria partners over the past decade. Overall cases in the country have risen from 2.73m in 2011 to 3.25m in 2015
NATIONAL MALARIA EFFORTS
- Between 2012 and 2015 2 million Long Lasting insecticide treated nets were distributed to a population of approximately 5 million in the 6 provinces
- This exceeded the desired 2 people per net ratio
 Intermittent preventive treatment in pregnancy reached only 59% of women registering for antenatal care in 2015
Intermittent preventive treatment in pregnancy reached only 59% of women registering for antenatal care in 2015- Only 44% and 18% of women received the second and third IPTp doses respectively.

CHALLENGES
- A dual challenge makes performance of malaria indicators difficult
- The Global Fund grant had expired for more than a year
- The oil-based economy also suffered from the major global drop in prices
THE WAY FORWARD
- Angola requires concerted efforts by government and partners to scale up malaria control interventions
- Universal coverage targets must be sustained if these high burden northern provinces are to begin seeing a decline in the disease
Announcement &Epidemiology &IPTp Bill Brieger | 04 Nov 2016
Malaria work of Jhpiego to be featured at ASTMH 65th Meeting
![]() The malaria work of Jhpiego will be featured in 8 posters and two symposia during the upcoming 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta from 13-17 November 2016. Below are titles of the posters and descriptions of the symposia along with session information that will help people find the presenters. We will share abstracts closer to the actual time of presentation. Follow the conference on twitter through #TropMed16.
The malaria work of Jhpiego will be featured in 8 posters and two symposia during the upcoming 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta from 13-17 November 2016. Below are titles of the posters and descriptions of the symposia along with session information that will help people find the presenters. We will share abstracts closer to the actual time of presentation. Follow the conference on twitter through #TropMed16.

Poster Presentations
- Collaborative efforts to improve prevention of malaria in pregnancy in Burkina
 Faso through use of IPTp-SP. Mathurin Dodo, Stanislas Paul Nebie, Ousmane Badolo, Thierry Ouedraogo Presentation No. 304 Poster Session A
Faso through use of IPTp-SP. Mathurin Dodo, Stanislas Paul Nebie, Ousmane Badolo, Thierry Ouedraogo Presentation No. 304 Poster Session A - The Improving Malaria Care (IMC) Project’s Contribution to follow up a Pilot to Use Rapid Diagnostic Tests (RDTs) at the Community Level in Burkina Faso. Ousmane Badolo, Stanislas P. Nebie, Moumouni Bonkoungou, Mathurin Dodo, Rachel Waxman, Danielle Burke, William Brieger Presentation No. 218 Poster Session A
- Building Capacity to accelerate IPTp uptake through the adoption of 2012 WHO IPTp guidance in Malawi. John Munthali Presentation No. 393 Poster Session A
- Rwanda Towards Malaria Pre-Elimination: Active case investigation in a low endemic district. Noella Umulisa, Angelique Mugirente, Veneranda Umubyeyi, Beata Mukarugwiro, Stephen Mutwiwa, Jean Pierre Habimana, Corrine Karema Presentation No. 310 Poster Session A
- The Challenge of Reducing Malaria in Angola. Jhony Juarez, Margarita Gurdian-Sandoval, Julio Bonillo, William R. Brieger Presentation No. LB-5113 Poster Session A
- Joint efforts, a key to success for the Malaria in Pregnancy Program in Luanda, Angola. Jhony Juarez, Adolfo Sampaio, William R. Brieger, and Domingos F. Gueve Presentation No. 982 Poster Session B
- Improving pregnancy outcomes: Alleviating stock-outs situation of sulfadoxine pyrimethamine in Bungoma, Kenya. Augustine M. Ngindu, Gathari G. Ndirangu, Waqo Ejersa, David O. Omoit, Mildred Mudany Presentation No. 815 Poster Session B
- Community health: Improving start of IPTp early in second trimester through promotion of MIP at the community level in Kenya. Augustine Ngindu Presentation No. LB-5383 Poster Session C
Symposia
- Global Call to Action to Increase Coverage of Intermittent Preventive Treatment in Pregnancy: Progress and Lessons Learned. Symposium 87 Tuesday, November 15, 2016 1:45 PM / 3:30 PM Sponsors: PMI and MCS
Description: The aim of the symposium is to review country progress in sub-Saharan Africa (SSA) in increasing intermittent preventative treatment in pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP). The symposium will expand the knowledge base among Ministries of Health, donors and partners who are working to increase IPTp-SP coverage to address malaria in pregnancy (MiP). In this symposium, speakers from WHO and the President’s Malaria Initiative will describe how they are prioritizing support to scale up MiP interventions including IPTp-SP across SSA. Burkina Faso, Malawi and Tanzania will present and discuss how they were able to dramatically scale up IPTp-SP through a health systems approach that addresses MiP from community to district to national level.
- Malaria Pre-Elimination: Ensuring Correct Care of Reproductive Age Women. Symposium 146 Wednesday, November 16, 2016 1:45 PM / 3:30 PM
Description: This symposium will present experiences from four countries – Mozambique, Sierra Leone, Brazil, and Dominican Republic; specifically, looking at how these countries have addressed pregnant women in their malaria pre-elimination strategies. Further the symposium will discuss the important ethical considerations that should be reviewed as countries contemplate standard diagnosis, notification and treatment vs. MDA. The lessons learned shared can be disseminated to guide other countries where these strategies are being considered.
Elimination &Epidemiology Bill Brieger | 26 Oct 2015
Readiness for Malaria Elimination: Using HMIS data to Map Malaria Test Positivity in Huambo Province, Angola
 Colleagues[1] from the Ministry of Health Angola, Jhpiego and the Johns Hopkins Bloomberg School of public Health are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Monday 26th October 2015. Please stop by Poster LB-5094 and discuss the results as presented in the Abstract below.
Colleagues[1] from the Ministry of Health Angola, Jhpiego and the Johns Hopkins Bloomberg School of public Health are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Monday 26th October 2015. Please stop by Poster LB-5094 and discuss the results as presented in the Abstract below.
Huambo Province in the south central highlands of Angola has a population of nearly 2 million, or 15% of the nation’s total. It is classified in the stable meso-endemic belt of the country, but is in the process of revising its malaria strategy to bring it closer to the pre-elimination phase on the pathway to malaria elimination. This means aiming to achieve 5% slide positivity rate for malaria parasites during the height of the transmission season (Novemb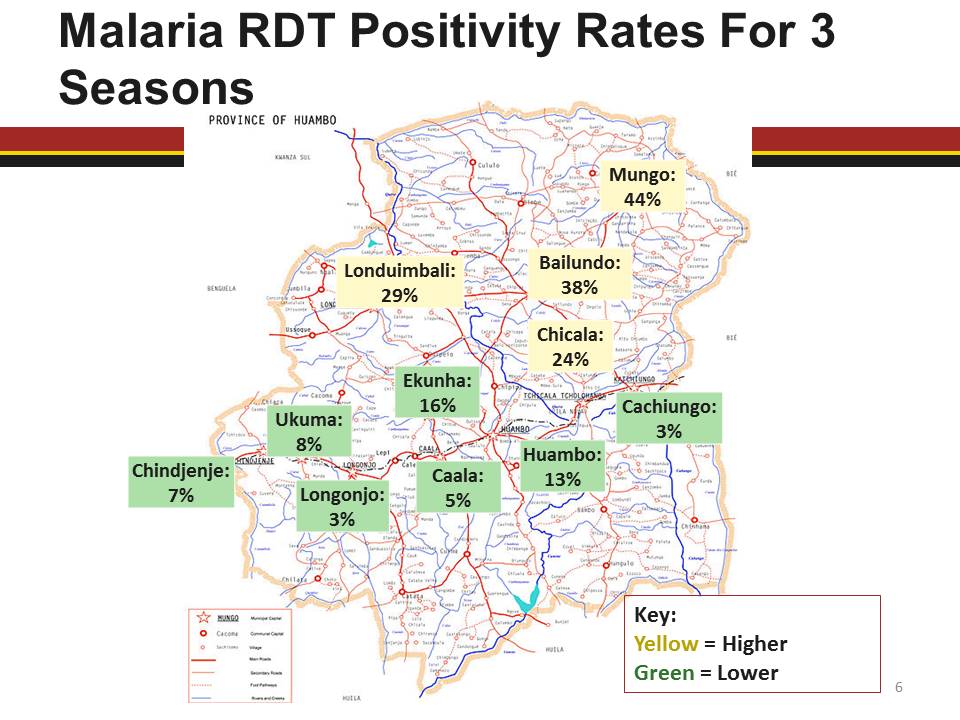 er to January).
er to January).
The health information system of the country reports information of positive and negative results of testing for suspected malaria cases from hospitals and clinics. The former use microscopy, while the latter rely on malaria rapid diagnostic tests (mRDTs). This information was analyzed for the past three high transmission periods and variations are reported herein among the 11 municipalities (districts) of the province.
The overall test positivity rates for all three seasons were 11% for microscopy and 25% for mRDTs among the 212,102 persons tested. The 4 municipalities in the northern part of the province ranged from 16-26% slide positivity and 24-44% mRDT positivity. The remaining municipalities in the south and central area ranged from 1-5% slide positivity and 3-16% mRDT positivity. Only one municipality achieved a positivity rate of <5% for both tests.
Moving forward, Huambo first intends to improve on the quality and coverage of malaria testing. The Ministry of Health will also focus on sustained control measures in the north, and begin more detailed mapping of malaria incidence in the central and southern municipalities to provide better targeting of interventions.
——-
[1] João Carlos F. Juliana, William R. Brieger, Jhony Juare3, Connie Lee, Clementino Sacanombo
Epidemiology &Malaria in Pregnancy Bill Brieger | 25 Oct 2015
Prevalence and Factors Associated with Malaria in Pregnancy in Rural Rwandan Health Facilities: A Cross-sectional Study
Colleagues[1] from the Rwanda Ministry of Health, Jhpiego and the Johns Hopkins Bloomberg School of public Health are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Monday 26th October 2015. Please stop by Poster 315 and discuss the results as presented in the Abstract below.
Malaria in pregnancy (MIP) is a serious health risk for the pregnant woman and fetus and associated 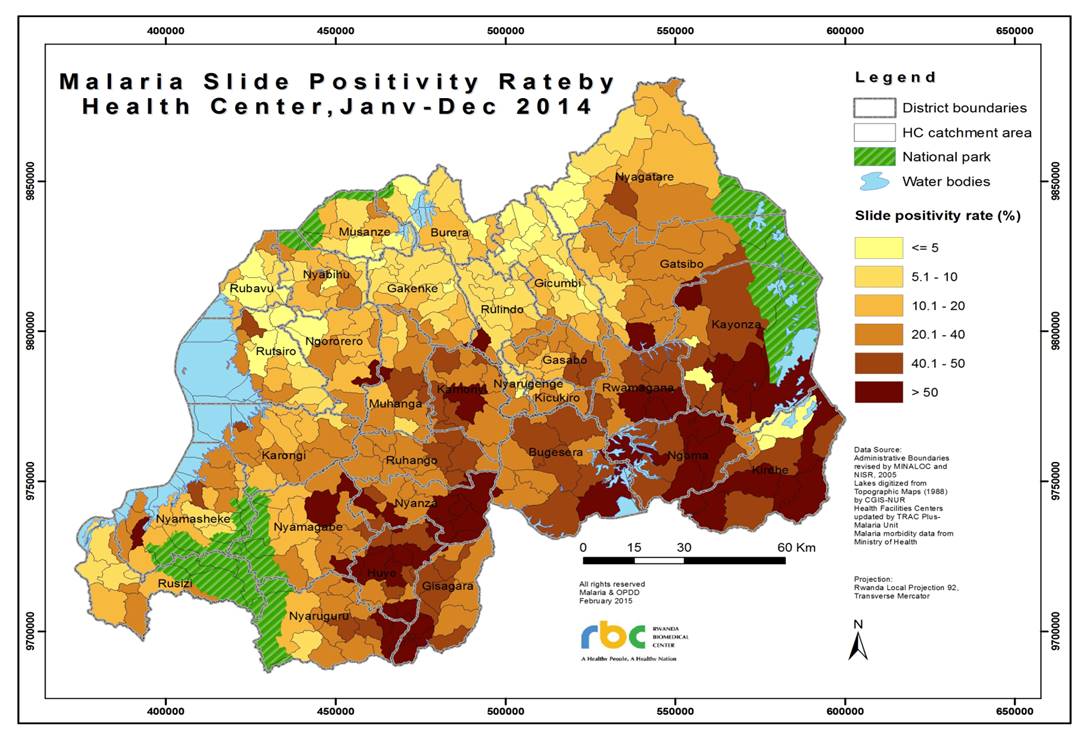 with mortality in the perinatal period. In Rwanda there has been no accurate national estimate of malaria prevalence among pregnant women. In 2011, a cross-sectional study of 6 districts in 3 malaria transmission zones (low, medium and high) in Rwanda was conducted to estimate the prevalence of peripheral parasitemia in pregnant women. Data were collected from consenting women presenting to antenatal clinics (ANC) for the first time in their current pregnancy including age, parity, gestation, ITN availability and use.
with mortality in the perinatal period. In Rwanda there has been no accurate national estimate of malaria prevalence among pregnant women. In 2011, a cross-sectional study of 6 districts in 3 malaria transmission zones (low, medium and high) in Rwanda was conducted to estimate the prevalence of peripheral parasitemia in pregnant women. Data were collected from consenting women presenting to antenatal clinics (ANC) for the first time in their current pregnancy including age, parity, gestation, ITN availability and use.
Blood was obtained for malaria testing using microscopy, rapid diagnosis tests and polymerase chain reaction (PCR). A total of 4,037 pregnant women were recruited with median age of 27 years, and 3,781 (93.7%) had usable PCR samples. The prevalence of MIP by PCR was 5.6%.
 Nearly 20% of women’s families did not have a net, and 8.7% of these tested positive compared to 4.9% of women whose family owned an ITN. For those who did not sleep under an ITN the previous night, 8.1% tested positive compared with 4.8% who slept under an ITN. Malaria prevalence by parity ranged from 5.5% (parity 0-1), to 5.4% (parity 2-3), and 6.5% (parity 4 or more). The two districts that bordered highly endemic countries had MIP prevalence rates of 10% and above. Those testing positive were treated according to national guidelines.
Nearly 20% of women’s families did not have a net, and 8.7% of these tested positive compared to 4.9% of women whose family owned an ITN. For those who did not sleep under an ITN the previous night, 8.1% tested positive compared with 4.8% who slept under an ITN. Malaria prevalence by parity ranged from 5.5% (parity 0-1), to 5.4% (parity 2-3), and 6.5% (parity 4 or more). The two districts that bordered highly endemic countries had MIP prevalence rates of 10% and above. Those testing positive were treated according to national guidelines.
Despite a significant decline of 86% in malaria prevalence in the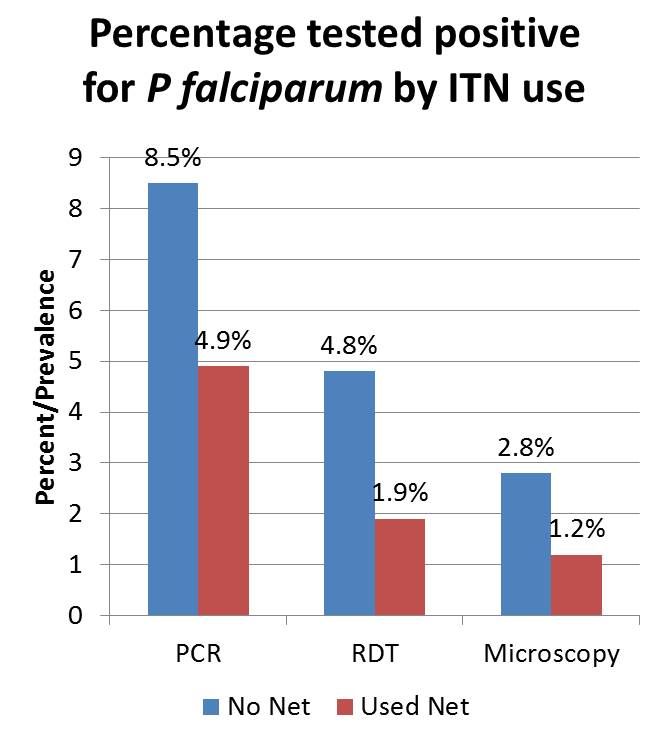 general population from 2005 to 2011, MIP prevalence remains high, especially in border districts. Our study also showed that ITN ownership and use among these pregnant women is below the national target. In order to address this gap, ITN distribution to achieve universal access, and educational campaign targeted at pregnant women on the use of ITN are recommended. Furthermore, early detection and treatment of MIP at ANC and regional collaboration to reduce cross-border malaria transmission should be prioritized.
general population from 2005 to 2011, MIP prevalence remains high, especially in border districts. Our study also showed that ITN ownership and use among these pregnant women is below the national target. In order to address this gap, ITN distribution to achieve universal access, and educational campaign targeted at pregnant women on the use of ITN are recommended. Furthermore, early detection and treatment of MIP at ANC and regional collaboration to reduce cross-border malaria transmission should be prioritized.
————————–
[1] Corine Karema, William R. Brieger, Irenee Umulisa, Aline Uwimana, Jeremie Zoungrana, Beata Mukarugwiro, Rachel Favero, Elaine Roman, Barbara Rawlins, Tharcisse Munyaneza, Fidele Ngabo, David Sullivan, Jean Baptiste Mazarati, Rukundo Alphonse, Agnes Binagwaho
Borders &Diagnosis &Epidemiology &ITNs Bill Brieger | 30 Sep 2015
Individual and Household Level Risk Factors Associated with Malaria in Mutasa District, Zimbabwe: a Serial Cross-Sectional Study
Mufaro Kanyangarara and her PhD thesis adviser, Luke Mullany of the Johns Hopkins Bloomberg School of Public Health Department of International Health, have been looking into the challenges of controlling and eventually eliminating malaria in a multi-country context in southern Africa. We are sharing abstracts from her pioneering work including the following which explores risk factors on the Zimbabwe-Mozambique order.
Background: Malaria constitutes a major public health problem in Zimbabwe, particularly in the north and east bordering Zambia and Mozambique. In Manicaland Province in eastern Zimbabwe, malaria transmission is seasonal and unstable. As a result of intensive scale up of malaria interventions, malaria control was successful in Manicaland Province. However, over the past decade, Manicaland Province has reported increased malaria transmission, and the resurgence of malaria in this region has been attributed to limited funding, drug resistance and insecticide resistance. One of the worst affected districts is Mutasa District. The aim of the study was to identify malaria risk factors at the individual and household levels to better understand what is driving factors associated with malaria and consequently enhance malaria control in eastern Zimbabwe.
north and east bordering Zambia and Mozambique. In Manicaland Province in eastern Zimbabwe, malaria transmission is seasonal and unstable. As a result of intensive scale up of malaria interventions, malaria control was successful in Manicaland Province. However, over the past decade, Manicaland Province has reported increased malaria transmission, and the resurgence of malaria in this region has been attributed to limited funding, drug resistance and insecticide resistance. One of the worst affected districts is Mutasa District. The aim of the study was to identify malaria risk factors at the individual and household levels to better understand what is driving factors associated with malaria and consequently enhance malaria control in eastern Zimbabwe.
Methods: Between October 2012 and September 2014, individual demographic data and household characteristics were collected from cross-sectional surveys of 1,116 individuals residing in 316 households in Mutasa District. Factors characterizing the surrounding environment were obtained from remote sensing data. Factors associated with malaria (measured by rapid diagnostic test [RDT]) were identified through univariate and multivariate multilevel logistic regression models.
Results: A total of 74 (6.4%) participants were RDT positive. Parasite prevalence differed by season (10.4% rainy and 2.9% dry, OR 4.52, 95% CI 2.11-9.69). Sleeping under a bednet showed a protective effect against malaria (OR 0.54, 95% CI 0.29-1.00) despite pyrethroid resistance. The household level risk factors protective against malaria were household density (OR 0.89, 95% CI 0.87-0.97) and increasing distance from the border with Mozambique (OR 0.86, 95% CI 0.76-0.97). Increased malaria risk was associated with recent indoor residual spraying (OR 2.30, 95% CI 1.16-4.56).
Conclusions: Malaria risk was concentrated in areas located at a lower household density and in closer proximity to the Mozambique border. Malaria control in these “high risk” areas may need to be enhanced. These findings underscore the need for strong cross-border malaria control initiatives to complement country specific interventions.
Environment &Epidemiology &Surveillance Bill Brieger | 19 Aug 2015
Beyond Garki baseline results released, highlighting changes in malaria environment
Ilya Jones shares with us the latest update on Malaria Consortium’s Beyond Garki project that seeks to understand changes in malaria epidemiology and recommend effective strategies to improve control efforts ……
 Over the last 15 years, increased global investment in fighting malaria has contributed substantially to reduction in the prevalence of the disease in endemic countries around the world. With the development of new technologies and innovative approaches to disease control, there is more hope than ever that malaria will be eliminated in places where it used to be a major public health threat.
Over the last 15 years, increased global investment in fighting malaria has contributed substantially to reduction in the prevalence of the disease in endemic countries around the world. With the development of new technologies and innovative approaches to disease control, there is more hope than ever that malaria will be eliminated in places where it used to be a major public health threat.
However, sustaining momentum requires a deep understanding of the changes in the frequency of the disease, determinants of transmission and impact of interventions in a changing environment. Understanding these changes is essential in order to tailor health interventions to be as effective as possible.
Malaria Consortium’s Beyond Garki project, funded by the UK government through the Programme Partnership Arrangement (PPA), seeks to understand changes in malaria epidemiology and recommend strategies to improve malaria control efforts. The project is named after the efforts of the World Health Organization and the government of Nigeria to study the epidemiology and control of malaria in Garki, Nigeria between 1969 and 1976. Beyond Garki began in Uganda and Ethiopia in 2012, with four survey rounds conducted to date. Additional studies were also carried out in Cambodia, and more studies are planned in Nigeria. Each survey tracks changes in malaria epidemiology over time and will ideally inform strategic decisions on the use of interventions.
The baseline results have been made available and will serve as a point of comparison for data obtained from subsequent survey rounds, which will be released in the autumn. However the results of the baseline survey are interesting in their own right. Some of the highlights are listed below:
- Low to moderate malaria transmission intensity was observed in all sites. In Ethiopia, P. vivax was found to be a predominant malaria species, probably due to decline in transmission over recent years.
- High coverage of insecticide treated nets (ITNs)was observed in three of four sites but it is still not at an ideal level.
- ITN use rates among household members that had access were generally quite high. The study
 also showed there is willingness to buy nets, at least in the Uganda sites.
also showed there is willingness to buy nets, at least in the Uganda sites. - In Uganda, a major vector of malaria, A. gambiae s.s., has developed resistance against pyrethroids.
- Most human-vector contact still occurs indoors. However, there is a tendency of early biting of A. funestus s.l. in one of the sites in Uganda. More information is needed to determine the biting and resting habits of vector species in both countries.
- The rate of malaria diagnosis using microscopy and rapid diagnostic tests (RDTs) has been strengthened in all sites. RDTs have been found to effectively predict negative malaria results, indicating that service providers should pay attention to other causes of fever when RDT negative results are reported for patients.
- The level of use of intermittent preventive treatment of pregnant women (IPTp) needs to be strengthened in Uganda.
 To learn more about the project, the methods used to collect data, the findings and the recommendations, check out the dedicated microsite for Beyond Garki here, or read the baseline report here.
To learn more about the project, the methods used to collect data, the findings and the recommendations, check out the dedicated microsite for Beyond Garki here, or read the baseline report here.
Epidemiology &Mapping &water Bill Brieger | 23 May 2014
Satellite Mapping, an important step toward malaria control and elimination in Nigeria
Omede Ogu of Nigeria’s Federal Ministry of Health reports on efforts to undertake mapping of malaria in the country as a basis for better planning of control and eventual elimination efforts.
 The National Malaria Elimination Program (NMEP) has been meeting with the team from the National Space Research and Development Agency (NASRDA). Progress on pilot malaria mapping in Niger State is being reviewed, though the study is yet to be concluded. NMEP is also looking at opportunities that exist to expand their initial mapping to cover the whole of the country. Discussions are underway on next steps and development of a road map or a framework for the study going forward.
The National Malaria Elimination Program (NMEP) has been meeting with the team from the National Space Research and Development Agency (NASRDA). Progress on pilot malaria mapping in Niger State is being reviewed, though the study is yet to be concluded. NMEP is also looking at opportunities that exist to expand their initial mapping to cover the whole of the country. Discussions are underway on next steps and development of a road map or a framework for the study going forward.
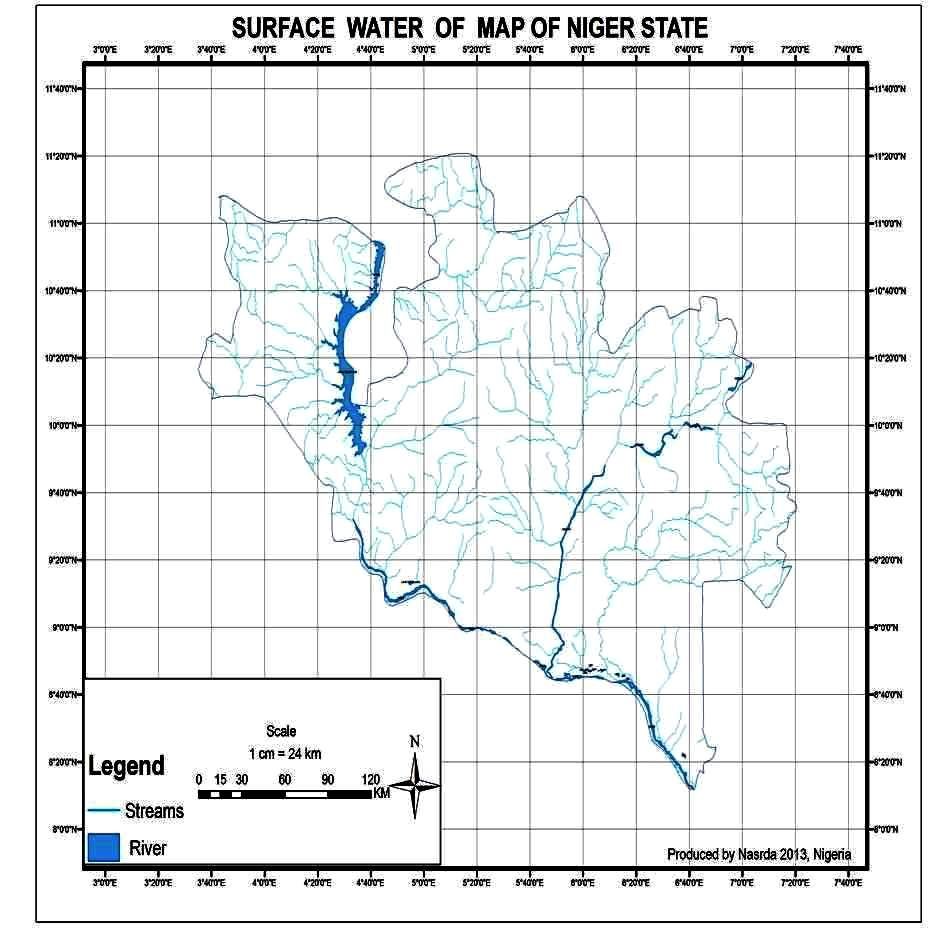
NASRDA explained that the current mapping effort was aimed is to use satellite-based technology to map surface water for Malaria Control in North-central Nigeria with Niger State as a Pilot study. They noted that data in inaccessible locations such as the marshy areas, thick forests, rugged terrain etc. were previously unavailable for relevant environmental policy and decision making in the region and Nigeria.
In addition is will be possible to do infrastructural mapping and inventory of health care facilities, in order to identify and assess the state of health care facilities, how accessible and future areas of need provision of these facilities in the country.
So far NASRDA has identified settlements, and locations of hospitals and health centres throughout Niger State using Global Positioning System (GPS). They have also identified water bodies and wetlands locations throughout the state.
Finally they are developing a map of Surface Water and wetlands in the state showing these in relation to locations of settlements, hospitals and health centres. NMEP is planning to link with colleagues doing similar mapping in Kenya.
NMEP plans to have the final report of the study ready by October for dissemination. Major partners with funding lines in their 2014 work plans for this study are the National Primary Health Care Development Agency (NPHCDA) and NASRDA. Additional funding and support is being sought.
Kenya already is using its mapping to focus appropriate malaria interventions. All countries will benefit in better mapping for targeting their malaria control and elimination efforts.
Epidemiology &Surveillance Bill Brieger | 01 May 2014
The feasibility of achieving and sustaining “malaria-free zones” in southern Zambia
World Malaria Day 2014 was observed at the Johns Hopkins Bloomberg School of Public Health on Friday 25 April. 21 posters were presented. Below is the abstract of a poster presented William Moss and colleagues from the Southern Africa International Centers of Excellence for Malaria Research.
 The Government of Zambia is committed to creating “malaria-free zones” in southern Zambia. Through passive case detection at health care facilities and active case detection through community-based surveys, we have documented a dramatic decline in the burden of malaria in the catchment area of Macha Hospital, Choma District, Southern Province, Zambia from 2008 through 2013.
The Government of Zambia is committed to creating “malaria-free zones” in southern Zambia. Through passive case detection at health care facilities and active case detection through community-based surveys, we have documented a dramatic decline in the burden of malaria in the catchment area of Macha Hospital, Choma District, Southern Province, Zambia from 2008 through 2013.

Macha Hospital: https://www.flickr.com/photos/inmed/sets/72157625850417125/
However, residual foci of transmission exist and the potential for repeated importation remains. We identified individuals with subpatent parasitemia and gametocytemia who may be responsible for sustained, low-level transmission and evaluated reactive case detection strategies to identify and treat these individuals using simulation models.
Factors associated with sustained insecticide-treated bed net use were evaluated in light of the declining burden of malaria. Parasite bar coding of 24 SNPs should permit the identification of imported parasites.
Results of a longitudinal analysis of changes in antibody responses to 500 Plasmodium falciparum antigens using a protein microarray should allow detection of residual transmission and document loss of humoral immunity in the absence of exposure.
Epidemiology &Health Information &Monitoring &Surveillance Bill Brieger | 26 Apr 2014
iPhones for household malaria surveys in Sierra Leone
World Malaria Day 2014 was observed at the Johns Hopkins Bloomberg School of Public Health on Friday 25 April. 21 posters were presented. Below is the abstract of a poster presented by Suzanne Van Hull of Catholic Relief Services.
Catholic Relief Services (CRS) and the Ministry of Health and Sanitation (MoHS) of Sierra Leone (SL) are co-implementing nationwide malaria prevention and treatment activities funded by the Global Fund to fight AIDS, Tuberculosis and Malaria. In order to track progress and impact, CRS and partners led the implementation of a malaria indicator survey (MIS) in early 2013 covering a nationally-representative sample of 6,720 households, inclusive of blood testing to determine prevalence of anemia and malaria. In early 2012, CRS also had the experience of using mobile technology for a Knowledge Attitude and Practices (KAP) study.
Fieldworkers used Apple 3GS iPhones for both surveys to collect data via the iFormBuilder platform, a web-based, software-as-services application with a companion app for the mobile devices allowing for timely data collection, monitoring, and analysis.
This was the first time that iPhones were used for a MIS, and lessons learned include: allowing at least four months to transform paper-based questionnaires into electronic format, giving the program enough time for pre-testing the tool and training data collectors/biomarkers/laboratory technicians, and involving key malaria stakeholders to ensure a nationally-led survey. Global Positioning Systems enabled the MoHS to make in-depth analyses on malaria trends based on geographic locations.
 Overall the benefits of an electronic versus a paper-based MIS questionnaire outweighed the challenges. The iPhone technology eliminated the need for paper transcribing, allowing for quicker data tabulation, real-time identification of mistakes, faster interviewing through skip patterns, and a close-to-clean dataset by the end of data collection saving time and money.
Overall the benefits of an electronic versus a paper-based MIS questionnaire outweighed the challenges. The iPhone technology eliminated the need for paper transcribing, allowing for quicker data tabulation, real-time identification of mistakes, faster interviewing through skip patterns, and a close-to-clean dataset by the end of data collection saving time and money.
Survey results will be used to set evidence-based targets for all partners’ future malaria activities, especially the next 3 years of GF-supported malaria grants
coinfection &Epidemiology &Tuberculosis Bill Brieger | 24 Mar 2014
World TB Day: considering malaria coinfection
Typical of our big disease mindset, most donor agencies think of HIV-Tuberculosis coinfection when addressing a connection among the three Global Fund diseases. Take as an example a recent News Flash from the Global Fund: “In a major step toward addressing the growing number of people affected by co-infection with tuberculosis and HIV, the Global Fund is improving the way it approaches treatment programs in countries with high rates of each disease. Millions of people infected with both TB and HIV could benefit from better services.”
 The possible neglect of TB and malaria interactions might be understood by the fact that HIV and TB have much wider areas of endemicity than malaria. On the other hand both HIV and TB are disproportionately represented in malaria endemic Africa. At present the main connection between malaria and TB is the fact that they must share out of the same ‘envelope’ when new Global Fund support is distributed through the new funding mechanism to countries, a process that some see as moving more toward donor control and AID effectiveness and away from human rights.
The possible neglect of TB and malaria interactions might be understood by the fact that HIV and TB have much wider areas of endemicity than malaria. On the other hand both HIV and TB are disproportionately represented in malaria endemic Africa. At present the main connection between malaria and TB is the fact that they must share out of the same ‘envelope’ when new Global Fund support is distributed through the new funding mechanism to countries, a process that some see as moving more toward donor control and AID effectiveness and away from human rights.
Today the Stop-TB Partnership and related organizations are observing World TB day by noting that at least one-third of newly infected people will not get appropriate treatment. Poor access to or inadequate and inappropriate treatment plagues all three diseases, especially where health systems are weak. We need an integrated approach to strengthen systems and improve care.
In the meantime, researchers have maintained interest in possible interactions between TB and malaria. For example Ann-Kristin Mueller and colleagues have published a study entitled, “An Experimental Model to Study Tuberculosis-Malaria Coinfection upon Natural Transmission of Mycobacterium tuberculosis and Plasmodium berghei,” using a mouse model. A slide presentation on their work is also seen at the website. As Mueller notes, “Concurrent infections most likely modulate the respective immune response to each single pathogen and may thereby affect pathogenesis and disease outcome. Coinfected patients may also respond differentially to anti-infective interventions.”
Mueller puts is mildly when she says that TB-malaria coinfection “has not been studied in detail.” We might need to step back in time over 2900 years where according to Lalremruata and colleagues, “the notion that the agricultural boom and dense crowding occurred in this region (southwest of modern Cairo), especially under the Ptolemies, highly increased the probability for the manifestation and spread of tuberculosis. Here we extend back-wards to ca. 800 BC new evidence for malaria tropica and human tuberculosis co-occurrence in ancient Lower Egypt.”
In a 2013 review on “Co-infection of tuberculosis and parasitic diseases in humans,” Xin-Xu Li and Xiao-Nong Zhou found only two direct reports of malaria and TB co-infection, one a case report from 1945 and the other on host response in malaria and depression of defense against tuberculosis from 1999.
Finally a review of hospital records from 2007 in Luanda, Angola found that Malaria was diagnosed during admission and hospital stay in 37.5% of TB patients. Clearly the time has come to take coinfection seriously as both a research and service delivery topic.