CHW &Diagnosis &Elimination &Epidemiology Bill Brieger | 01 Apr 2018 07:02 am
Improving the efficacy of reactive screen-and-treat for malaria elimination in southern Zambia
Global Health Day 2018 sponsored by the Johns Hopkins University Center for Global Health featured a poster presentation by several colleagues on Improving the efficacy of reactive screen-and-treat for malaria elimination in southern Zambia. Fiona Bhondoekhan, William Moss, Timothy Shields, Douglas Norris, Kelly Searle, Jennifer Stevenson, Harry Hamapumba, Mukuma Lubinda and Japhet Matoba (Southern Africa International Centers of Excellence in Malaria Research, the JHU Bloomberg School of Public Health, and the Macha Research Trust, Zambia) share their findings below.
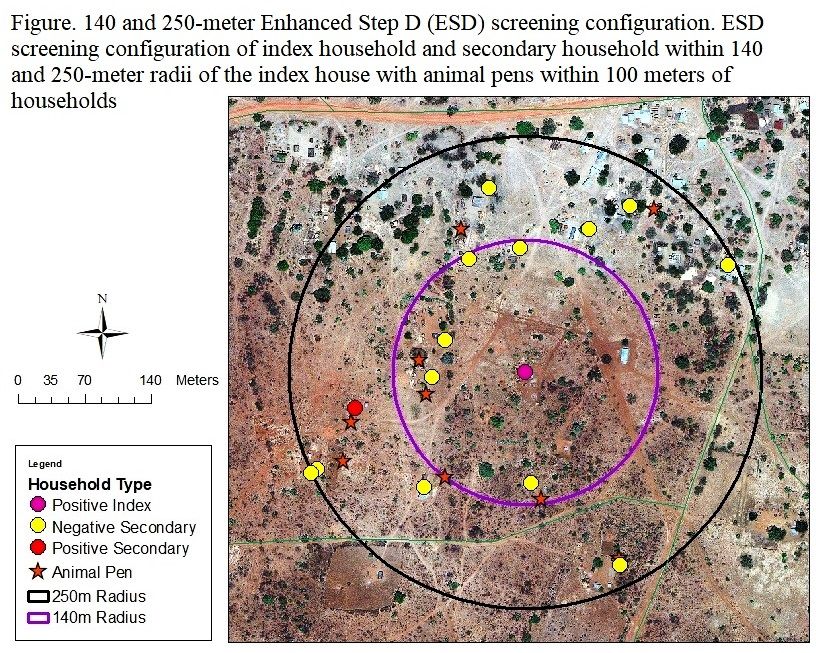 Background: Malaria screen-and-treat (called Step D in Zambia) is a reactive case detection strategy in which cases detected at a health center trigger community health workers (CHWs) to screen for secondary malaria cases within a 140-meter radius of the index case household using PfHRP2 rapid diagnostic tests (RDTs). Few studies evaluated whether an evidence-based strategy using environmental features that characterize the immediate surroundings of a household, can improve the efficiency of secondary case identification.
Background: Malaria screen-and-treat (called Step D in Zambia) is a reactive case detection strategy in which cases detected at a health center trigger community health workers (CHWs) to screen for secondary malaria cases within a 140-meter radius of the index case household using PfHRP2 rapid diagnostic tests (RDTs). Few studies evaluated whether an evidence-based strategy using environmental features that characterize the immediate surroundings of a household, can improve the efficiency of secondary case identification.
Objective: This study utilized the Step D and extended the screening radius to 250-meters (termed Enhanced Step D or ESD) to assess which local environmental variables can guide CHWs to identify secondary cases more efficiently. As Zambia works toward eliminating malaria, more refined and targeted case detection strategies are required to find the untreated malaria cases that could serve as potentially asymptomatic sources of infection. This study can help guide and plan reactive case detection strategies in Zambia that allow community health workers/field teams to employ an evidence-based strategy to find malaria-positive secondary households situated near index case houses more efficiently.
 Methods: Demographic information, malaria diagnosis, bed-net use and ownership, cooking energy source, and household floor material were obtained from surveys. Households were stratified into malaria positive and negative secondary households using RDT and qPCR results. ArcGIS was used to generate the following local environmental variables: screening radius (140 vs. 250-meters), number of animal pens within 100-meters, distance to nearest animal pen, distance and elevation difference between index and secondary houses, as well as the following large scale environmental variables: distance to main road and nearest stream category. Generalized estimating equations (GEE) estimated the cross-sectional effect for the difference in odds of a positive vs. negative secondary household for each predictor. For the secondary analysis GEE with the same model specifications was used to estimate the cross-sectional difference in odds of a positive vs. negative household for each environmental predictor. Model fit was evaluated with the Hosmer-Lemeshow goodness of fit test and significance was evaluated as a p-value of 0.05. Statistical analyses were carried out using STATA 14.2.
Methods: Demographic information, malaria diagnosis, bed-net use and ownership, cooking energy source, and household floor material were obtained from surveys. Households were stratified into malaria positive and negative secondary households using RDT and qPCR results. ArcGIS was used to generate the following local environmental variables: screening radius (140 vs. 250-meters), number of animal pens within 100-meters, distance to nearest animal pen, distance and elevation difference between index and secondary houses, as well as the following large scale environmental variables: distance to main road and nearest stream category. Generalized estimating equations (GEE) estimated the cross-sectional effect for the difference in odds of a positive vs. negative secondary household for each predictor. For the secondary analysis GEE with the same model specifications was used to estimate the cross-sectional difference in odds of a positive vs. negative household for each environmental predictor. Model fit was evaluated with the Hosmer-Lemeshow goodness of fit test and significance was evaluated as a p-value of 0.05. Statistical analyses were carried out using STATA 14.2.
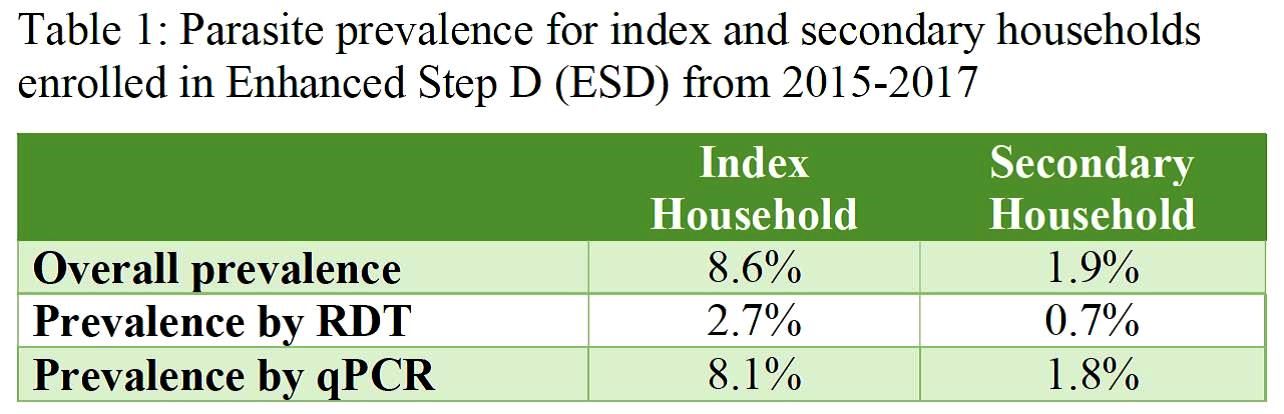
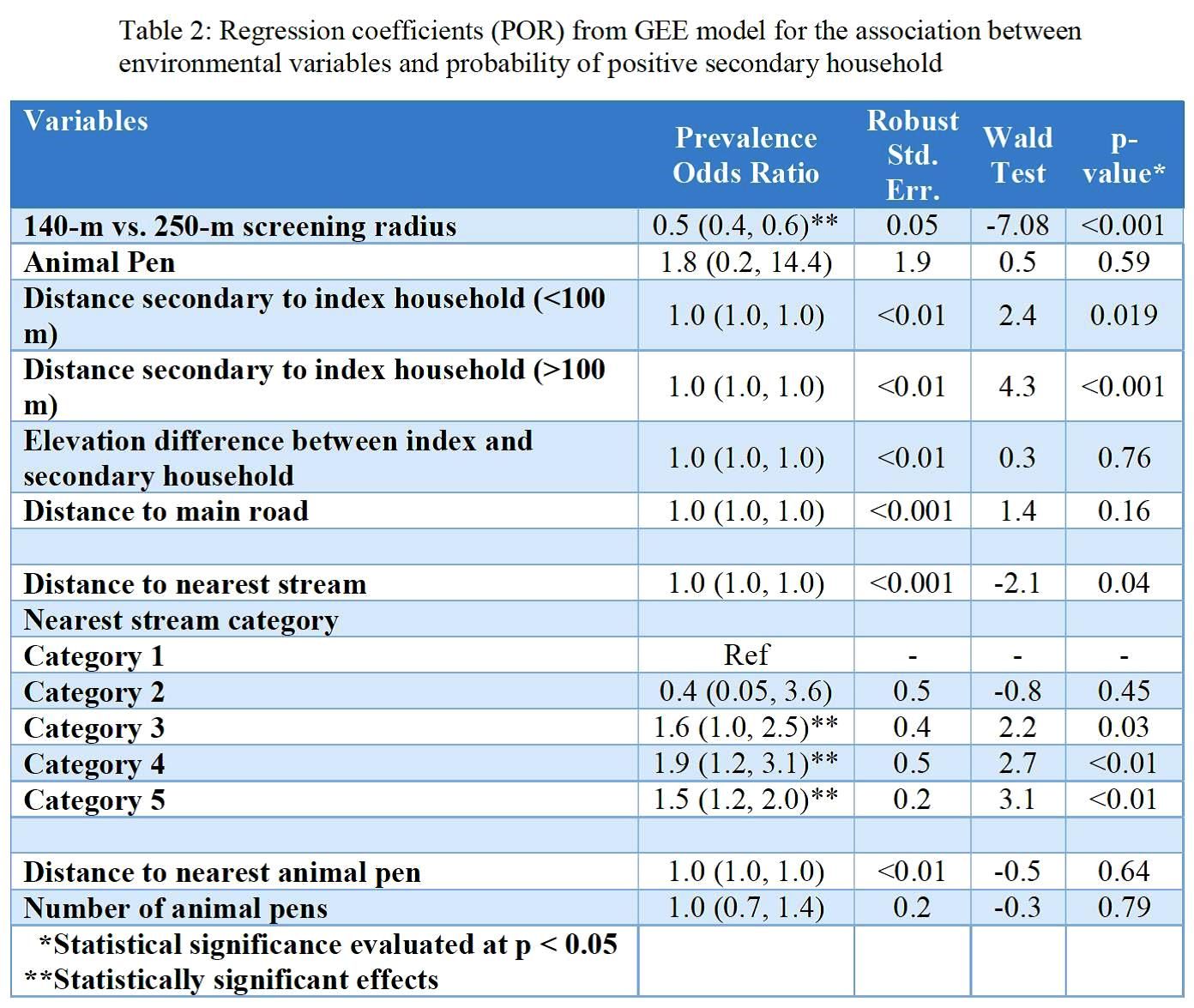 Results: Screening within the index households yielded an overall parasite prevalence of 8.6%, which was higher by qPCR (8.1%) than RDT (2.7%) as seen in Table 1. Secondary households had an overall parasite prevalence of 1.9% with similar differences by test used. Key results from regression analysis seen in Table 2 include a difference in prevalence according to screening radius as well as by proximity to the nearest stream. Secondary analysis produced similar results but showed statistically significant higher odds for households where animal pens were present.
Results: Screening within the index households yielded an overall parasite prevalence of 8.6%, which was higher by qPCR (8.1%) than RDT (2.7%) as seen in Table 1. Secondary households had an overall parasite prevalence of 1.9% with similar differences by test used. Key results from regression analysis seen in Table 2 include a difference in prevalence according to screening radius as well as by proximity to the nearest stream. Secondary analysis produced similar results but showed statistically significant higher odds for households where animal pens were present.
Conclusion: Screening for secondary households within low-transmission setting in Zambia could be optimized by using both local-scale indicators such as the presence of animal pens and large-scale indicators such as streams as environmental guiding tools.
Acknowledgements: This research was supported in part the Bloomberg Philanthropies and the Johns Hopkins Malaria Research Institute, and the NIH-sponsored Southern and Central Africa ICEMR 2U19AI089680.

on 01 Apr 2018 at 8:18 pm 1.Improving the efficacy of reactive screen-and-treat for malaria elimination in southern Zambia said …
[…] Read the original post: Improving the efficacy of reactive screen-and-treat for malaria elimination in southern Zambia […]
on 16 Apr 2018 at 12:28 pm 2.Your MACEPA Malaria Minute: Let the surveys begin! | Making Malaria History said …
[…] in Malaria Research, the JHU Bloomberg School of Public Health, and the Macha Research Trust on Improving the efficacy of reactive screen-and-treat for malaria elimination in southern Zambia. The study concluded that screening for secondary households could be optimized by using indicators […]