Health Systems &IPTp &Malaria in Pregnancy Bill Brieger | 07 Nov 2014
Health Systems Strengthening: Achieving Lasting Results for IPTp
 At the Call to Action for Intermittent Preventive Treatment of Malaria in Pregnancy (IPTp) during the just concluded American Society of Tropical Medicine and Hygiene Annual Meeting, Elaine Roman of Jhpiego/MCSP advocated for strengthened health systems as a basic approach to enhancing IPTp coverage. Below is a summary of her remarks.
At the Call to Action for Intermittent Preventive Treatment of Malaria in Pregnancy (IPTp) during the just concluded American Society of Tropical Medicine and Hygiene Annual Meeting, Elaine Roman of Jhpiego/MCSP advocated for strengthened health systems as a basic approach to enhancing IPTp coverage. Below is a summary of her remarks.
Why should we strengthen the Health System? Addressing the health system at all levels leads to improved outcomes and comprehensive coverage. Increasing IPTp uptake requires strengthening antenatal care (ANC) and other components of the health system.
ANC within a strong health system provides an opportunity to improve the health of pregnant women and their newborns. Malaria in pregnancy (MIP) is a maternal and newborn health issue. When health systems are weak, there is greater likelihood of negative consequences on mother and newborn.
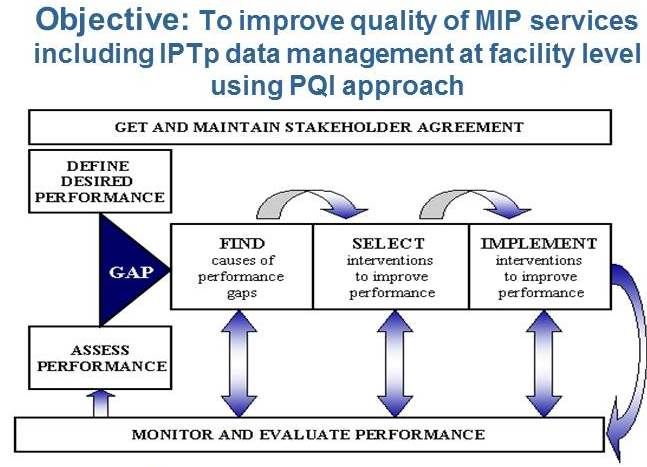
 Improving Health Systems for enhanced IPTp addresses the following health systems components:
Improving Health Systems for enhanced IPTp addresses the following health systems components:
- Integration: Reproductive Health Programs and National Malaria Control Programs
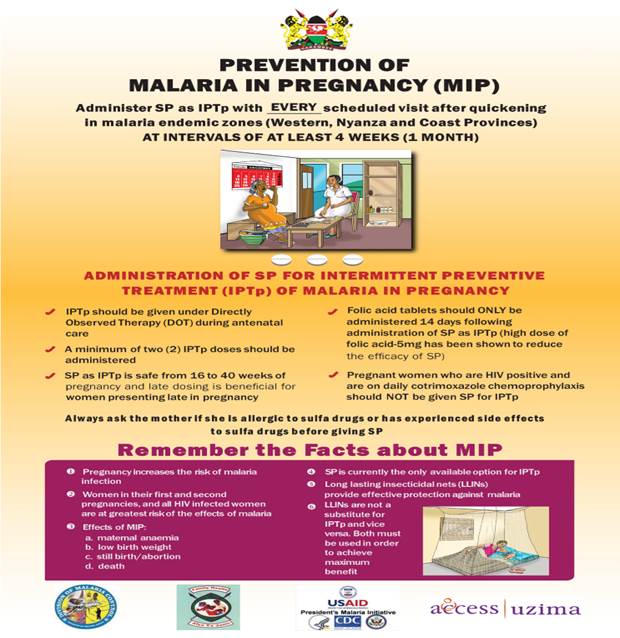
- Policies and Guidelines: Consistency across national documents
- Capacity Development: Bother In-Service Training and Pre-Service Education
- Quality Assurance: Linked directly with support supervision
- Community Engagement: Promotion of early ANC and Promotion of IPTp uptake
- Commodities: Ensuring availability at ANC of sulfadoxine-pyrimethamine (SP) and supplies, as well as long-lasting insecticide-treated bed nets
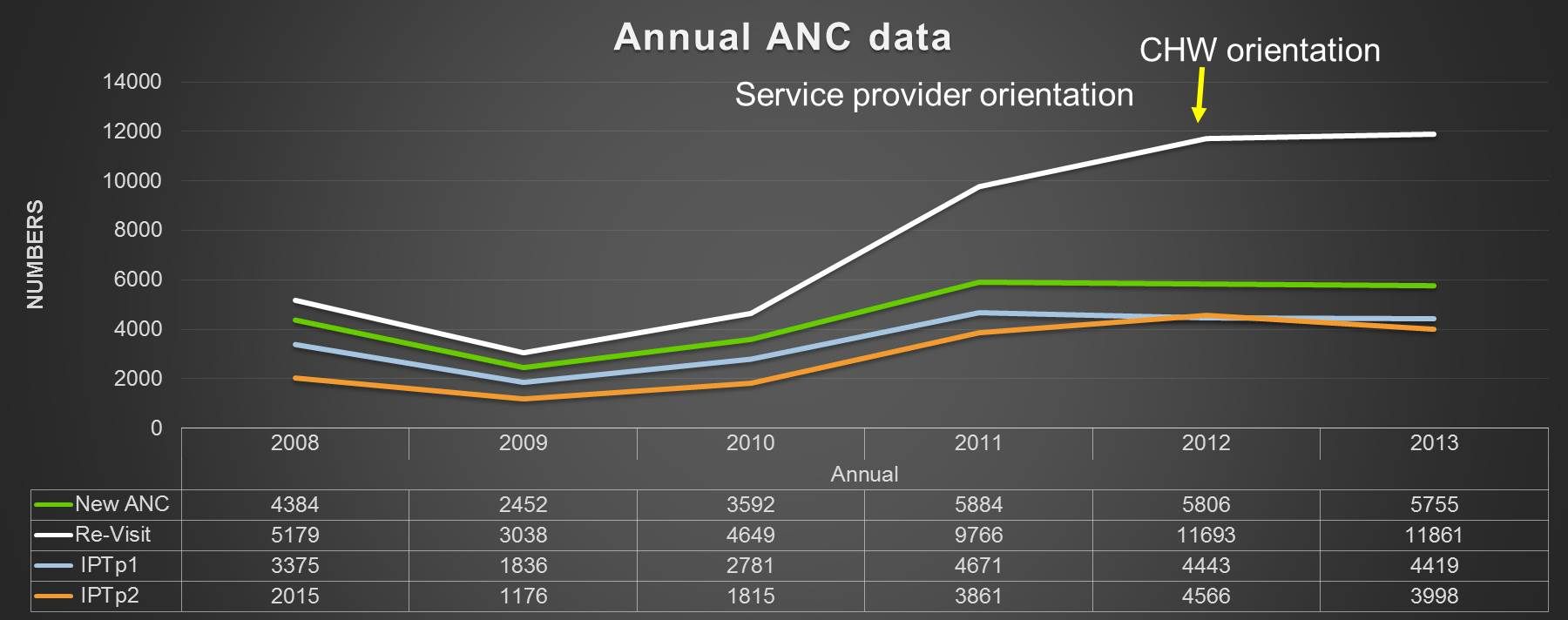
- Monitoring and Evaluation: Facility-level data collection and Data for decision- making
- Finance: Sustained and comprehensive services
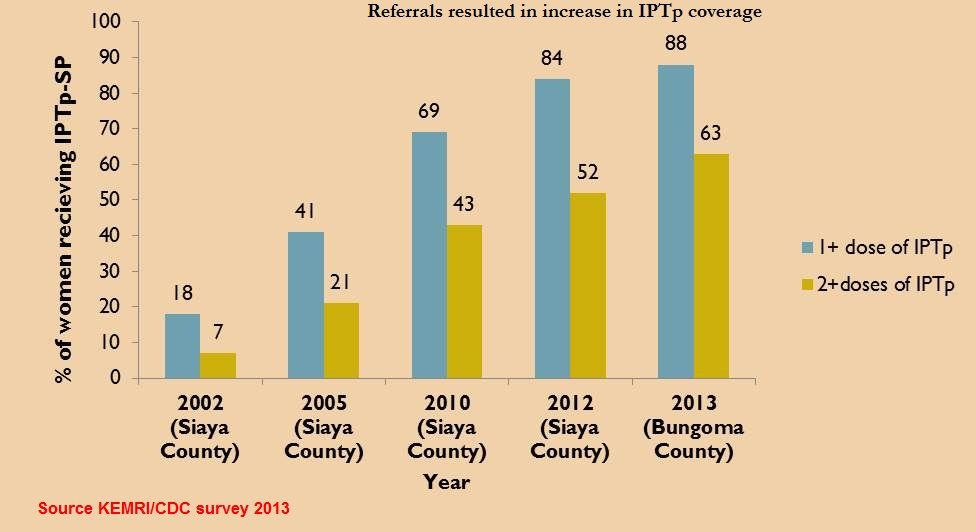
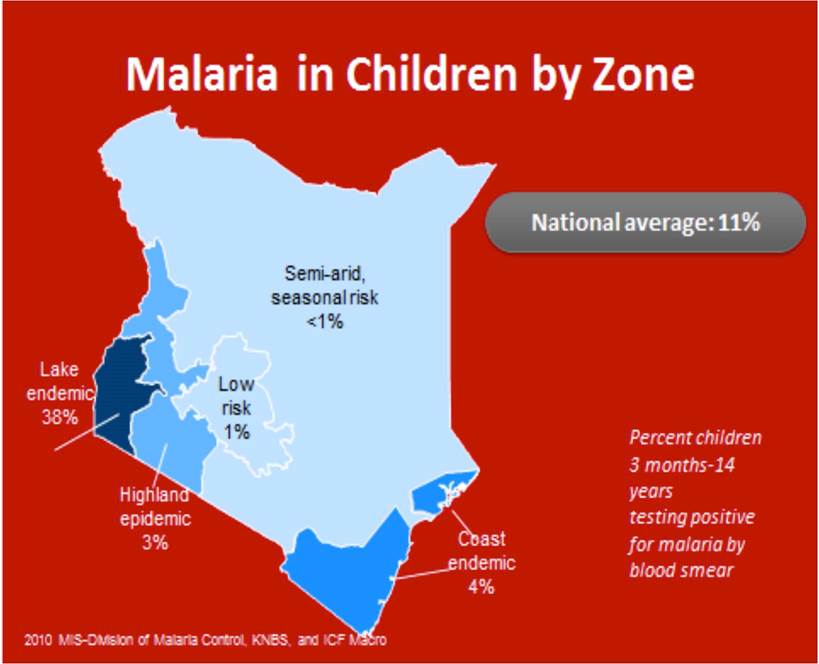
 Systems strengthening works. Strengthened Health Systems for IPTp in Kenya resulted from community engagement, training, supervision: leading to IPTp1 coverage of 91.6% and IPTp2 (or more doses) coverage at 61.1%.
Systems strengthening works. Strengthened Health Systems for IPTp in Kenya resulted from community engagement, training, supervision: leading to IPTp1 coverage of 91.6% and IPTp2 (or more doses) coverage at 61.1%.
In Ghana, Capacity development, commodities, community engagement improvements resulted in IPTp2 (or more doses) coverage of 44% to 65%
In Zambia development of clear policy, integrated training, supervision led to IPTp2 (or more doses) coverage increasing from 63% in 2007 to 72% in 2012.
Moving forward we must advocate for strengthening health systems that will lead to increased IPTp uptake and lasting gains. We must focus on ANC, complemented by efforts at community and policy levels. Finally we must address each health system component, based on country context.