Community &Eradication &Malaria in Pregnancy &Women Bill Brieger | 18 Nov 2016 08:08 pm
Malaria Mass Drug Administration: Ensuring Safe Care of Reproductive Age Women
The potential impact of mass malaria drug administration (MDA) on pregnant women was the focus of Symposium 146 at the recent 65th Annual Meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The symposium was co-chaired by Clara Menéndez and Larry Slutsker who opened the session with an overview.
 As malaria control interventions are scaled up and sustained and malaria transmission levels decline and prevalence falls, an increasing number of countries are starting to see elimination on the horizon. For pregnant women, the antimalarial antibodies that have provided some level of protection in moderate to high malaria transmission settings are reduced as malaria transmission declines.
As malaria control interventions are scaled up and sustained and malaria transmission levels decline and prevalence falls, an increasing number of countries are starting to see elimination on the horizon. For pregnant women, the antimalarial antibodies that have provided some level of protection in moderate to high malaria transmission settings are reduced as malaria transmission declines.
Current evidence shows that as transmission levels decline, the consequences from P. falciparum malaria are even greater for pregnant women. As countries enter pre-elimination stage and move towards eventual elimination, it will be important to address the needs of pregnant women given their increased vulnerability.
To help achieve elimination, countries are exploring strategies involving widespread distribution of anti-malarials, primarily artemisinin-combination therapies (ACTs), to asymptomatic individuals, including both mass drug administration (MDA) and mass screen and treat (MSaT).
Animal studies have suggested potential embryo toxicity and teratogenic effects of artemisinin drugs in the first trimester of pregnancy.
Given the limited human data, ACTs are currently contraindicated in first trimester, except in documented cases of clinical malaria illness where quinine is unavailable. This poses a challenge in mass campaigns, as it requires the identification of women in early pregnancy who are not yet obviously pregnant. Screening including offering pregnancy tests and/or interview to ask a woman her pregnancy status directly may not work as many may not wish to reveal their pregnancy status.
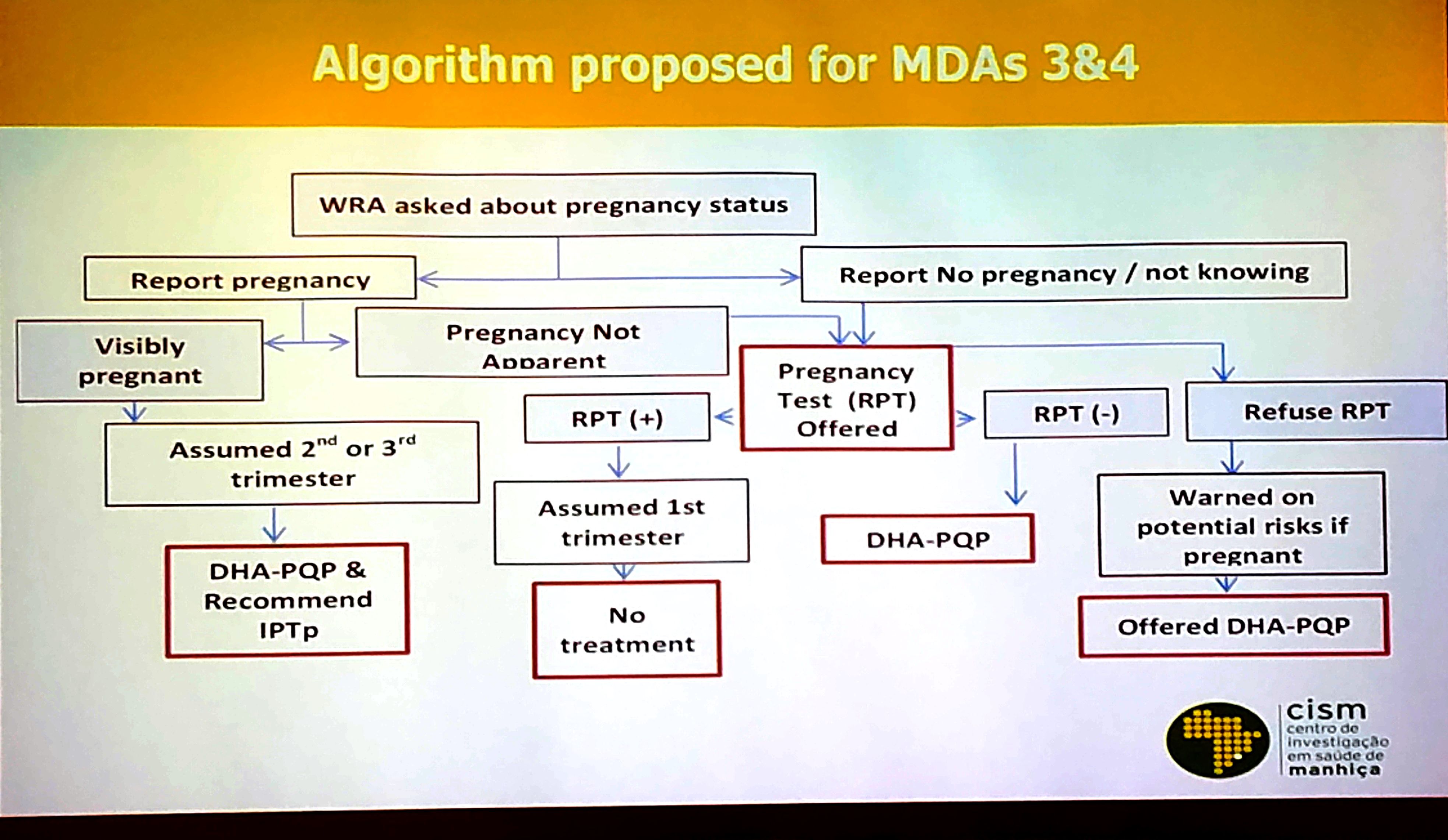
Final Algorithm for Screening Prior to MDA in Mozambique
While only about 5% of the population is pregnant at any given time, and only 1/3 of those are in the first trimester, approximately 20% of the population is comprised of women of reproductive age who may be pregnant. Thus, the number of women who need to be screened for pregnancy is substantial across countries. In addition to privacy issues, costs of screening processes are another barrier.
During the symposium Francisco Saúte from Mozambique and Samuel J. Smith from Sierra Leone shared experiences. Clara Menéndez addressed ethical issues involved in the potential risk of MDA with the ACT Dihydroartemisinin-Piperaquine (DHA-P). These two countries have addressed pregnant women in MDAs in two widely different contexts.
Mozambique is learning whether MDA is a valuable component to malaria elimination in the low transmission areas in the southern part of the country. In Sierra Leone MDA was seen as a lifesaving tool to prevent malaria deaths during the Ebola epidemic when taking blood samples for diagnosis was a major risk.
Over several rounds of MDA, Mozambique refined its pregnancy screening procedures over several rounds of MDA as seen in the attached slide. Costs, confidentiality, convenience and efficiency entered into the equation that saw a greater focus on communicating with women rather that testing. Lessons learned from MDA in Mozambique included –
- Screening for early pregnancy in the context of MDA is challenging, particularly among teenage girls where disclosing pregnancy can be problematic
- Need to train field workers (preferably women) about the need to ensure confidentiality of pregnancy testing/results
- Confidentiality is also crucial to ensure adherence to t

MDA Rationale in Sierra Leone during Ebola Outbreak
he pregnancy testing
- Women not accepting pregnancy test must be warned on risks/ benefits of ACTs in 1st trimester
- Health authorities must understand that IPTp and MDA are not mutually exclusive

The Ebola epidemic in Sierra Leone and its neighbors, Liberia and Guinea, devastated the health workforce, and the availability of any sort of testing supplies was low. The country experienced a major drop in utilization of clinic based MCH services including those for malaria during the period.

MDA Goals in Sierra Leone
Because of initial similarities in presenting symptoms between Ebola and malaria, people were often fearful of going to the health center in case they were detained for Ebola care or were exposed to other patients who had Ebola. Community MDA seemed to be one way to protect the population from malaria in this emergency situation. The attached slide offers a rational for the MDA. A second slide explains Sierra Leone’s goal for MDA with Artesunate-Amodiaquine in the context of Ebola. Though not completely, the Sierra Leone MDAs were able to exclude pregnancy women in their first trimester.

Pregnant women excluded from MDA in Sierra Leone
In conclusion MDA is a tool conceived primarily for countries and areas of countries as part of the pre-elimination strategy. It presents a variety of logistical challenges, but a major concern should also be the ethical issues of giving a potentially toxic drug to women in their first trimester of pregnancy. Alternative strategies to protect these women, including insecticide treated nets, must be explored.