Integration &Treatment Bill Brieger | 03 Mar 2014
iCCM – collaboration for commodities
The integrated Community Case Management Symposium (iCCM) in Accra, Ghana this week provides an ideal opportunity to examine the practical issues of getting the commodities to manage cases of malaria, pneumonia and diarrhoea at the community level. http://iccmsymposium.org/
 Ordinarily one would expect the medicines needed for iCCM would be obtained through a country’s normal essential drug management system. ACTs, ORS, amoxicillin, etc., should be available through the regular primary health system of a country to all front line health facilities. It is from this frontline facility that community health workers (CHWs) delivering iCCM would normally receive training and stocks/supplies.
Ordinarily one would expect the medicines needed for iCCM would be obtained through a country’s normal essential drug management system. ACTs, ORS, amoxicillin, etc., should be available through the regular primary health system of a country to all front line health facilities. It is from this frontline facility that community health workers (CHWs) delivering iCCM would normally receive training and stocks/supplies.
The reality is that many front line facilities experience frequent stock-outs. They cannot meet the demands for their own clinic services, let alone provide supplies for community volunteers. Whether it is an issue of financial resources or political will, lack of essential medicines makes it difficult to guarantee child survival more than 25 years after UNICEF, WHO, USAID and other partners launched various initiatives to save children’s lives.
Currently countries are placing hopes in international financial programs such as the Global Fund to solve their commodity needs and scale up to prevent child deaths. http://www.theglobalfund.org/en/ In particular opportunities to develop a basic iCCM infrastructure and obtain appropriate malaria commodities are potentially available through Global Fund malaria grants. Child health program managers must work with national malaria control program staff to access this resource.
The Global Fund’s new funding mechanism is based on the national malaria strategic plan. If that plan does not address iCCM, it is unlikely countries can use their ‘envelop’ of funds for that purpose. Regardless, the Global Fund support will provide only malaria commodities. Where can counties get ORS, zinc and amoxicillin, especially if they do not have well-funded national medical stores/essential drugs program.
The RNMCH* Trust Fund with support from Norwegian and British aid agencies is being established and may help provide these pneumonia and diarrhoea commodities in stocks large enough to scale up iCCM. USAID child health projects also include diarrhoea and zinc. The long term sustainability of iCCM based on donor assistance is questionable. We are far from eliminating malaria, and there is no serious discussion of eradicating diarrhoeal diseases and pneumonia.
A pilot project to improve access to quality child illness case management that is being designed in Bauchi State, Nigeria demonstrates the challenges of coordinating commodities. Some were available through a World Bank Malaria Booster Program under a malaria plus package concept. USAID was providing ORS and zinc to child health projects. The US President’s Malaria Initiative could provide ACTs and RDTs, but the local governments and medicine shops involved in the project would have to buy amoxicillin through their normal wholesale channels. Getting the right mix of medicines at the right time in the right amounts to the right places is not easy.
Collaboration among different disease and health programs is always a challenge, but in the short term, program managers in both malaria control and child health need to work together to tap all available resources for iCCM. In the long run donors need to address health system strengthening so countries can manage their own essential drug programs successfully.
*Reproductive, Neonatal, Maternal and Child Health
Cancer &NCDs &Treatment Bill Brieger | 02 Feb 2014
Malaria and Cancer: World Cancer Day on 4th February
![]() As World Cancer Day approaches it is worth considering the connections between communicable and non-communicable diseases. Below are some brief extracts from recent studies that show relationships between malaria and cancers when it comes to diagnostics, drug research, treatment, prevention and epidemiology.
As World Cancer Day approaches it is worth considering the connections between communicable and non-communicable diseases. Below are some brief extracts from recent studies that show relationships between malaria and cancers when it comes to diagnostics, drug research, treatment, prevention and epidemiology.
PLoS One has a new article entitled: “Sloth Hair as a Novel Source of Fungi with Potent Anti-Parasitic, Anti-Cancer and Anti-Bacterial Bioactivity.” The authors found that, “Seventy-four isolates were cultivated in liquid broth and crude extracts were tested for bioactivity in vitro. We found a broad range of activities against strains of the parasites that cause malaria (Plasmodium falciparum) and Chagas disease (Trypanosoma cruzi), and against the human breast cancer cell line MCF-7.”
The Nature Group’s Scientific Reports sheds some more light on links between malaria and Burkitts lymphoma in the article “Relationship between Plasmodium falciparum malaria prevalence, genetic diversity and endemic Burkitt lymphoma in Malawi”. The researchers report that, “Endemic Burkitt lymphoma (eBL) has been linked to Plasmodium falciparum (Pf) malaria infection, but the contribution of infection with multiple Pf genotypes is uncertain… Further work is needed to evaluate the possible role of Pf genetic diversity in the pathogenesis of endemic BL.”
Recently KH Khan drew our attention to the fact that, “DNA vaccines against cancer, tuberculosis, Edwardsiella tarda, HIV, anthrax, influenza, malaria, dengue, typhoid and other diseases,” have been explored. It was noted that “These vaccines function by generating the desired antigen inside the cells, with the advantage that this may facilitate presentation through the major histocompatibility complex.”
 Hematologists must also deal with a variety of communicable and non-communicable diseases that affect red blood cells. According to Fedovsov and colleagues, “Hematologic disorders arising from infectious diseases, hereditary factors and environmental influences can lead to, and can be influenced by, significant changes in the shape, mechanical and physical properties of red blood cells (RBCs), and the biorheology of blood flow,” as well as broad spectrum of hematologic disorders including certain types of cancer.
Hematologists must also deal with a variety of communicable and non-communicable diseases that affect red blood cells. According to Fedovsov and colleagues, “Hematologic disorders arising from infectious diseases, hereditary factors and environmental influences can lead to, and can be influenced by, significant changes in the shape, mechanical and physical properties of red blood cells (RBCs), and the biorheology of blood flow,” as well as broad spectrum of hematologic disorders including certain types of cancer.
Again in the area of drug research, Hooft van Huijsduijnen and colleagues explore the “Anticancer properties of distinct antimalarial drug classes.” Within these drug classes the researcher observed that “Several of the antimalarials tested in this study have well-established and excellent safety profiles with a plasma exposure, when conservatively used in malaria, that is well above the IC50s that we identified in this study. Given their unique mode of action and potential for unique synergies with established anticancer drugs, our results provide a strong basis to further explore the potential application of these compounds in cancer in pre-clinical or/and clinical settings.”
We need to maintain a broader vision of human health past the 2015 Millennium Development Goals and neglect neither communicable nor non-communicable diseases, but see synergies and complementarities in working on both together.
Morbidity &Treatment Bill Brieger | 29 Jan 2014
Ronald McDonald House Charities Awards Jhpiego Grant to Reach Thousands of Children with Lifesaving Malaria Services
 FOR IMMEDIATE RELEASE
FOR IMMEDIATE RELEASE
Contact: 410.537.1829; www.jhpiego.org
Baltimore, Md. (January 28)—Jhpiego, an affiliate of Johns Hopkins University, received a $150,000 grant from Ronald McDonald House Charities (RMHC) to strengthen and expand malaria prevention and treatment services to vulnerable pregnant women and children in Chad.
 Jhpiego, a global health non-profit working in more than 50 countries, was among nine organizations selected by the global office of RMHC to improve the skills of health care workers through innovative approaches that directly benefit the health and welfare of vulnerable children around the world. The RMHC grant will build on Jhpiego’s current work in Chad to reduce deaths from malaria, the leading cause of death of children under five in the central African country.
Jhpiego, a global health non-profit working in more than 50 countries, was among nine organizations selected by the global office of RMHC to improve the skills of health care workers through innovative approaches that directly benefit the health and welfare of vulnerable children around the world. The RMHC grant will build on Jhpiego’s current work in Chad to reduce deaths from malaria, the leading cause of death of children under five in the central African country.
“Jhpiego is thrilled to begin this new relationship with RMHC to ensure that children receive quality health care services in Chad and survive,’’ said Leslie Mancuso, President and CEO of Jhpiego. “More children under five in Chad die from malaria than from any other cause. In cooperation with the government, we will build the capacity of community health volunteers to educate families on malaria prevention and promote home use of insecticide-treated nets. These volunteers who go door to door are often the first line of care in many countries, providing basic health messages and connecting families to health facilities.”
 The goal of the project funded by RMHC is to allow more children under five and pregnant women to receive much-needed services by training 10 Master Trainers, who will then educate and train 100 community health volunteers in malaria prevention activities. This approach will build a sustainable method for serving pregnant women and children in their communities. Jhpiego will target 109,571 children under five and 25,466 pregnant women who live in malaria-endemic districts in the East Logone region of Chad.
The goal of the project funded by RMHC is to allow more children under five and pregnant women to receive much-needed services by training 10 Master Trainers, who will then educate and train 100 community health volunteers in malaria prevention activities. This approach will build a sustainable method for serving pregnant women and children in their communities. Jhpiego will target 109,571 children under five and 25,466 pregnant women who live in malaria-endemic districts in the East Logone region of Chad.
Through its Global Grants and matching grants program to local U.S. RMHC Chapters, the Charity has awarded nearly $97 million in grants in the last 11 years. “Child mortality rates around the globe continue to be alarming. There is a need to invest in resources and training to create lasting change,” said David C. Herman, MD, MSMM, President and CEO, Vidant Health, and RMHC Board of Trustees member. “For 40 years, RMHC has been part of the solution in helping to eliminate some of the barriers that make it more difficult for families and children to get the health care they need.”
For more information about Jhpiego and its lifesaving mission, contact Melody McCoy, 410-537-1829 or melody.mccoy@jhpigeo.org.
About Jhpiego: Jhpiego (pronounced “ja-pie-go”) is an international, non-profit health organization affiliated with Johns Hopkins University. For 40 years, Jhpiego has empowered front-line health workers by designing and implementing effective, low-cost, hands-on solutions to strengthen the delivery of health care services for women and their families. For more information, go to http://www.jhpiego.org.
About Ronald McDonald House Charities: Ronald McDonald House Charities® (RMHC®), a non-profit, 501 (c) (3) corporation, creates, finds and supports programs that directly improve the health and well-being of children. Through its global network of local Chapters in 58 countries and regions, its three core programs, the Ronald McDonald House®, Ronald McDonald Family Room® and Ronald McDonald Care Mobile®, and millions of dollars in grants to support children’s programs worldwide, RMHC provides stability and resources to families so they can get and keep their children healthy and happy. All RMHC-operated and -supported programs provide access to quality health care and give children and families the time they need together to heal faster and cope better. For more information, visit www.rmhc.org, follow us on Twitter (@RMHC) or like us on Facebook (Facebook.com/RMHC Global).
The following trademarks used herein are owned by McDonald’s Corporation and its affiliates: Ronald McDonald House Charities, Ronald McDonald House Charities Logo, RMHC, Ronald McDonald House, Ronald McDonald Family Room and Ronald McDonald Care Mobile.
Elimination &IPTp &ITNs &Treatment Bill Brieger | 06 Dec 2013
Draft Nigeria 2013 DHS Shows Slow Progress for Malaria
The Nigeria Demographic and Health Survey (DHS) 2013 Draft Preliminary Report from the National Population Commission, Abuja, Nigeria and MEASURE DHS, ICF International, Calverton, Maryland, USA was released in-country in September 2013. These are the same organizations that conducted the 2010 Malaria Information Survey (MIS).
From the malaria perspective this has been a long anticipated event since the country has distributed over 60 million long lasting insecticide-treated nets since 2009. The 2010 MIS showed some progress over the 2008 DHS, but since it took place near the beginning of the massive net distribution effort, there was hope that a subsequent survey would highlight an improvement. If that were the expectation, people will be quite disappointed.
Lets start with nets. Our attached table shows only a slight improvement in the proportion of households owning at least one net. The idea behind the massive net campaigns from 2009-12 were achievement of universal coverage where there would be at least one net for every two people in a household. Where did these nets go? Were they damaged beyond use in the relatively short time that elapsed?
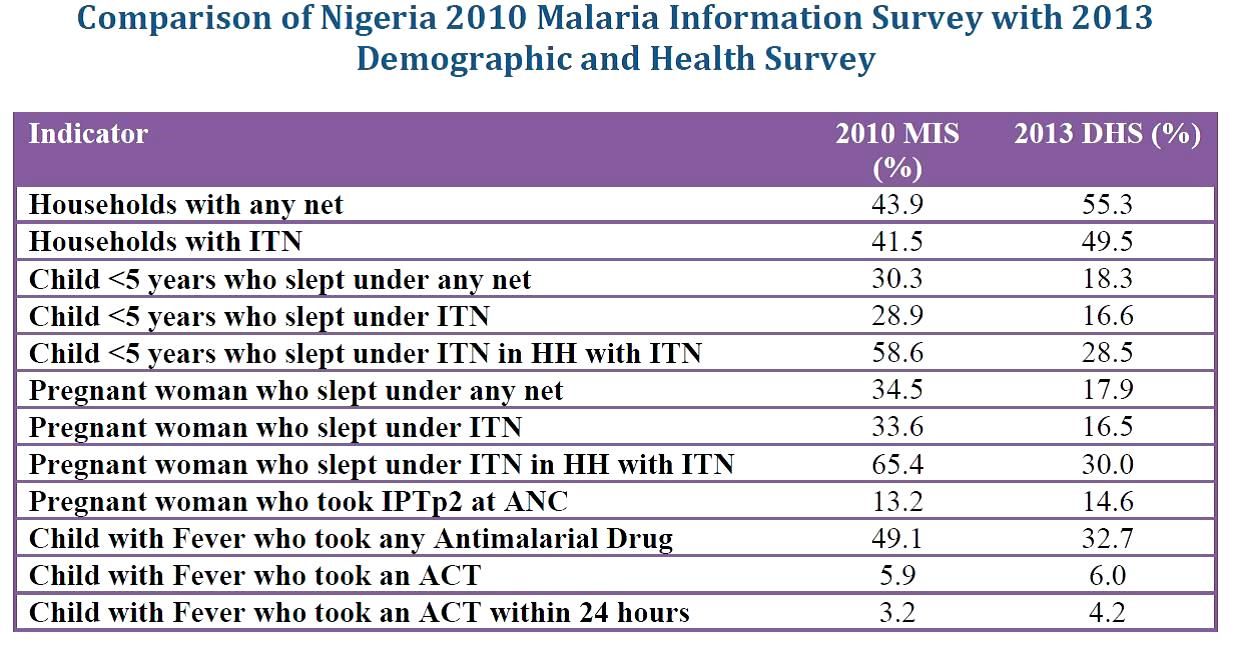 What is more disappointing is that th proportion of young children and pregnant women sleeping under an insecticide treated net (ITN) reduced to just slightly over half of the 2010 figure. This reduction also happened even in households that actually owned ITNs. This is mysterious to say the least.
What is more disappointing is that th proportion of young children and pregnant women sleeping under an insecticide treated net (ITN) reduced to just slightly over half of the 2010 figure. This reduction also happened even in households that actually owned ITNs. This is mysterious to say the least.
Prevention of malaria in pregnancy has been a neglected part of malaria control in many countries, but since the drug used for intermittent preventive treatment (IPT), sulphadoxine-pyrimethamine (SP) is so cheap, it was assumed that most health systems could afford to guarantee every woman attending antenatal care the required dosed. Unfortunately the status of IPT showed almost no improvement between 2010 and 2013 and remained far, far below the 2010 Roll Back Malaria target of 80% coverage. SP is produced in Nigeria; why can it not reach pregnant women?
Finally appropriate malaria treatment of young children is also in the doldrums. The actual number of children who received any anti-malarial drug declined, while those receiving the appropriate artemisinin-based combination therapy (ACT) remained essentially level at around 6%. Where have all the ACTs brought in through Global Fund, the US President’s Malaria Initiative and other donors gone? How can we expect infant and child mortality to decrease in the absence of appropriate treatment for one of the most common child killer diseases?
At the recently concluded 6th Pan African Malaria Conference in Durban, South Africa, participants were told that the only way to truly eliminate malaria is to tackle the high burden countries like Nigeria head on. If these data indicate how we are waging the malaria battle in Nigeria, our hopes for elimination in the near future will be dashed.
Community &Treatment Bill Brieger | 13 Nov 2013
Community directed distributors’ views on their work in community case management of malaria, pneumonia and diarrhoea
Below is the abstract for a another poster being presented by a team from Jhpiego at the upcoming 62nd annual meeting of the American Society for Tropical Medicine and Hygiene November 13-17 2013 at the Marriott Wardman Park in Washington DC. If you are at the conference, stop by poster number LB-2290 on Friday and discuss with Bright Orji.
 Jhpiego adapted the community directed interventions approach pioneered by the African Program for Onchocerciasis Control and the Tropical Disease Research program of WHO and collaborating agencies to deliver a combination of health interventions in 108 kin groups surrounding six primary health care facilities in Akwa Ibom State, Nigeria.
Jhpiego adapted the community directed interventions approach pioneered by the African Program for Onchocerciasis Control and the Tropical Disease Research program of WHO and collaborating agencies to deliver a combination of health interventions in 108 kin groups surrounding six primary health care facilities in Akwa Ibom State, Nigeria.
Volunteer community directed distributors (CDDs) who were selecte dby their co-villagers provided insecticide treated bednets, intermittent preventing treatment of malaria in pregnancy, and integrated community case management (iCCM) of malaria, pneumonia and diarrhoea. Communities selected 1-2 CDDs depending on their size using their own selection criteria.
Experience with volunteer community health workers like CDDs has shown that there are often serious logistical and motivational problems in maintaining a core group of volunteers. The community-selected mainly female CDDs and all had a minimum of secondary school education.
The CDDs were trained by health workers and the nearest primary health care facility. Three nurses who supervised the CDDs asked about their views and experiences as part of the supervisory process. Overall they obtained input from 152 CDDs serving the 108 kin groups. Key reasons why CDDs liked their included rendering service to neighbors (42.6%); reducing malaria (19.5%); reducing death (16.1%); improving Antenatal Care attendance (11.6%) and learning more about malaria (10.2%).
They also voiced discouragements such as working in the heavy rainy season (36.4%); lack of commodities (21.9%); lack of incentives (15.7%); farming season (11.6%); lack of respect from community members (7.2%) and poor road network (0.2%). When the CDDs were asked to identify reasons that they could opt out of the service, lack of commodities topped the list (73.3%). This was followed by lack of incentive (14.4%); and lack of appreciation by the community (9.8%).
The importance of intrinsic perceived benefits as possible motivators augurs well for program continuance. Fortunately few mentioned unsustainable financial incentives. Many of the logistical challenges they face can be tackled by better program management. These views can be incorporated into planning when the CDI approach is expanded into health service areas.
Community &Monitoring &Treatment Bill Brieger | 12 Nov 2013
Community registers in Akwa Ibom State, Nigeria track malaria treatment and integrated services
Below is the abstract for a poster being presented by a team from Jhpiego at the upcoming 62nd annual meeting of the American Society for Tropical Medicine and Hygiene November 13-17 2013 at the Marriott Wardman Park in Washington DC. If you are at the conference, stop by poster number LB-2289 on Friday and discuss with Bright Orji.

Community Directed Distributors bring their registers to the nearby clinic for monthly supervision meetings
Community Directed Treated with Ivermectin (CDTI) for onchocerciasis successfully reached 100,000 African villages with locally selected volunteers known as Community Directed Distributors (CDDs). Recognizing CDTI’s potential other health programs added a variety of interventions to the work of CDDs. Jhpiego (an Affiliate of Johns Hopkins University) successfully engaged communities and their CDDs in Akwa Ibom State, Nigeria to control malaria in pregnancy from 2007-11, and subsequently found the communities willing to expand into integrated community case management (ICCM) of malaria, diarrhoea and pneumonia. This report documents iCCM services given by CDDs.
The project mobilized 108 kin groups (100 +/- people) in 6 clinic catchment areas two Local Government Areas of the State. Each kin group selected 1-2 CDDs. Overall, 152 CDDs were trained by staff of local health centers. CDDs continued to provide intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine and then added malaria rapid diagnostic tests (RDTs); Artemisinin-based Combination Therapy for positive RDT results; oral rehydration solution and zinc tablets for diarrhea, and cotrimoxazole for pneumonia.
Data were extracted one year’s information from a sample of 68 community registers by three health staff using a checklist. During the period 2,202 clients were seen by CDDs with ages ranging from infancy to adulthood. Overall 33.3% were treated for malaria, 20.3% for pneumonia and 7.8% for diarrhoea (a few had multiple problems). Among the client visits, 30.6% were for pregnant women receiving a dose of IPTp.
RDTs were used with 1550 clients (70.4%) who had suspected malaria and 44.1% were positive. The breakdown of the 734 treated for malaria was positive RDT (93.1%), negative RDT (2.2%) and no test (5.2%). Community registers have shown that volunteer CDDs can provide a variety of front line health services, and can fairly correctly follow malaria testing and treatment procedures.
Malaria in Pregnancy &Treatment Bill Brieger | 04 Nov 2013
Improving case management of malaria during pregnancy by antenatal care providers in Akwa Ibom State, Nigeria
Bright Orji, William Brieger, Emmanuel Otolorin and John Orok presented today at the 141st APHA Annual Meeting in Boston of Jhpiego’s  experiences with malaria in pregnancy in Akwa Ibom State Nigeria. A summary appears below.
experiences with malaria in pregnancy in Akwa Ibom State Nigeria. A summary appears below.
In Nigeria malaria causes approximately 11% of maternal deaths. Malaria is responsible for 63% of hospit al admissions and 70% of illness among pregnant women. While intermittent preventive treatment (IPTp) and Long Lasting Insect icide-treated Nets (LUNs) are supposed to be given to pregnant women to prevent the dis·ease, coverage is poor.
Unfortunately since malaria is often being treated presumptively, pregnant women st ill die from other fever-related illnesses. Use of rapid diagnostic test (RDTs) to confirm malaria before treatment provides an opportunity for earlier recognition of febrile illnesses not due to malaria.
This study assessed the pattern of malaria diagnosis and treatment in pregnant women attending Antenatal care (ANC) in Akwa Iborn State, Nigeria. Record cards of pregnant women attending six government owned ANC before and after staff training on malaria diagnosis using RDTs.
The patients’ cards were drawn from ANC clinics with first non- follow-up visit of the year before training (February 20 10) and after (March 20 11) by three nurses/midwives.
Health care providers fever gave 85% of 3 13 women attending ANC antimalarial drugs before the introduction of RDTs training. Afterwards 82% of 179 febrile women were tested with RDTs. All 29 with positive RDT received artemisinin-based combination therapy, 6 RDT-negative women got ACTs, and no women who were not tested were treated for malaria.
Training encouraged health workers to adherence rational prescribing of antimalarials and made it possible t o offer better management of other fever-related illnesses during pregnancy. Support is now needed to scale-up RDTs use in ANC clinics in Nigeria.
Economics &Treatment Bill Brieger | 31 Oct 2013
Household cost of treating fevers in Ghana
Researchers at the Dodowa Health Research Center and the other centers affiliated with Ghana’s Ministry of Health/Ghana Health Service have shared with us their findings and concerns about the costs of treating malaria and febrile illness in Ghana. We can see that despite efforts to reduce costs through such efforts as the Affordable Medicines Facility malaria (AMFm), households are burdened when malaria strikes. Alexander A. A. Nartey, Patricia Akweongo, Elizabeth Awini1, Maxwell Darlaba, Theresa Tawiah, Jonas Akpakli, Doris Sarpong, Christine Clerk, Martin Adjuik, Moses Aikins, Fred Binka and Margaret Gyapong explain in more detail below.

AMFm certified quality drugs available in Chemical Seller Shops in Ghana
The burden of malaria seems to be reducing globally but sub-Saharan African countries continue to bear the greater burden of the disease considering the economic burden on the households. Malaria continues to be the number one cause of morbidity and mortality in Ghana. The household cost burden of malaria is both direct and indirect costs.
The study was a cross sectional cost-of-illness design. The study used self-reported fever as an indicator of malaria. The study household sample was drawn from the entire Health and Demographic Surveillance System (HDSS) databases of the Dangme West, Kintampo (North and South) and Kassena-Nankana (East and West) districts. All patients from such households that have a history of fever in the previous two weeks were interviewed on their care seeking, health providers used, treatment received and the related costs.
The average direct OPD cost of treating fevers was GH¢16.54 (US$11.25) and the average cost of self-treatment was 5 times less than seeking care at health facilities OPDs in Ghana. A household in Ghana was likely to pay GH¢31.43 (US$ 21.38) as direct cost per episode of fever treatment which was equivalent to 32.7% of monthly minimum income in Ghana.
Government of Ghana in its effort to keep the direct cost of treating fever relatively low through the provision of Health Insurance Scheme and the introduction of a subsidized AMFm drugs, the overall lost of productivity to the patient play a significant role especially when there are multiple fever cases within households in a year.
IPTp &ITNs &Treatment Bill Brieger | 24 Oct 2013
Awareness, Accessibility and Use of Malaria Control Interventions Among At-Risk Groups In Lagos State, Nigeria
AK Adeneye, PO Ossai and TS Awolola are sharing with us a pilot study they conducted based from the Nigerian Institute of Medical Research in Yaba, Lagos.
With two years to the MDGs deadline, there is limited evidence of decreases in malaria-related mortality and morbidity in Nigeria. We therefore wanted to evaluate the awareness, accessibility and use of malaria control interventions among at-risk groups in Lagos State, Nigeria.

Lagos State Ministry of Health http://www.lsmoh.com/news/lagos-treats-300-for-malaria#.UmlR9RAQ5aw
In planning for a broader assessment we conducted a descriptive, cross-sectional pilot study of 80 consenting pregnant women and mothers of children below five years of age. It was carried out using a household survey questionnaire and observation in Ikotun and Ketu communities of Lagos State
All respondents identified mosquito as the malaria vector. Respondents’ preferred drugs for malaria treatment were as follows: sulphadoxine-pyrimethamine (31.3%); ACTs (20.2%); artemisinin monotherapies (15.0%); chloroquine (13.8); and analgesics (12.5%). Only (30.0%) had used ACTs, and 55.0% of these had practiced self-medication.
Nearly all knew of and had LLINs. From room observation, only 53.8% (31.5% mothers of under-five vs. 11.3% pregnant women) actually hung the LLINs. Reasons for non-use of LLIN included: “prefer house spraying” (28.8%) and “causes heat” (7.5%).
LLIN use was positively associated with education (p<0.05), ranging from 50.0% (no education) to 77.8% (post-secondary). Only 41.8% got their LLINs through house-to-house mass distribution. Women averaged washing their nets 3 times within an average of 21.7 months of use.
LLIN washing practices showed that 30.5% used toilet soaps compared to detergents and hard soaps (66.7%). Unfortunately, 19.4% sun dried their nets.
While 52.6% of the pregnant women were aware of IPTp, 42.1% actually had received at least one dose.
Results of this pilot showed high awareness but low and poor use of malaria control interventions in populations studied. A wider survey in the near future will inform public health education on the different malaria control interventions that need to be intensified among the women so they can benefit from improved pregnancy and child health outcomes. This is important if the malaria-related MDG targets are to be realized in Lagos and in Nigeria in general.
Diagnosis &Treatment Bill Brieger | 18 Oct 2013
Knowledge of Senior Local Government Level (LGA) Health Workers on Malaria Treatment Guidelines in a South Western Nigerian State
 Esther Ayandipo, Bolatito Aiyenigba, Bukola Omobowale, Adebola Karim?Mohamed, Olusimbo Ige & Abbar Umar from the USAID PMI/MAPS Project (Nigeria) and the Department of Community Medicine University of Ibadan recently presented their findings from interviews with key local government health managers at the Multilateral Initiative for Malaria 6th Pan African Malaria Conference in Durban South Africa. They have shared their presentation below.
Esther Ayandipo, Bolatito Aiyenigba, Bukola Omobowale, Adebola Karim?Mohamed, Olusimbo Ige & Abbar Umar from the USAID PMI/MAPS Project (Nigeria) and the Department of Community Medicine University of Ibadan recently presented their findings from interviews with key local government health managers at the Multilateral Initiative for Malaria 6th Pan African Malaria Conference in Durban South Africa. They have shared their presentation below.
The risk of severe malaria is reduced when the disease is diagnosed accurately and on time [1]. Artemisinin Combination Therapy (ACTs) is the first line of According to the Nigerian national guidelines, parasitological confirmation is recommended in all suspected cases of malaria [2]. Malaria treatment practices have remained suboptimal in many primary health facilities (PHCs) in Oyo State. Routine monitoring visits to public primary health facilities show use of Chloroquine for malaria treatment and indiscriminate use of injection Arthemether for treatment of uncomplicated malaria.
The Medical Officer of Health (MOH) /primary health care coordinator as the apex officers at the Local Government Areas (LGAs) are expected to supervise and ensure compliance to national malaria treatment guidelines at PHCs within their LGAs. This study aims to assess the knowledge of MOHs on malaria treatment guidelines as a measure of their supervisory effectiveness.
Oyo State has 33 LGAs. A cross sectional survey of all 33 MOHs and 17 assistant MOHs was conducted to assess knowledge of current malaria treatment guidelines using a semi structured questionnaire. Knowledge assessed include; current management of fever cases including diagnosis before treatment for malaria; preferred choice of antimalarial drug, symptoms of severe malaria and management of malaria in pregnancy. Descriptive analysis was done using SPSS version 16.
 A total of 50 health workers responded to the questionnaire. Doctors constituted 27%, nurse/midwives 62.5%, and CHOs 10.4% of respondents. Overall, 87.8% had been trained on malaria case management.
A total of 50 health workers responded to the questionnaire. Doctors constituted 27%, nurse/midwives 62.5%, and CHOs 10.4% of respondents. Overall, 87.8% had been trained on malaria case management.
Even though 98% believed that not all fever is malaria, 76% will still treat all fever cases for malaria. Just 62% knew that other causes of fever should be looked for when RDT is negative while 8% will go ahead and treat RDT negatives for malaria.
Many (93.8%) will use ACTs to treat RDT positive cases however 10.6% still felt Chloroquine is the mainstay treatment for malaria. 15.2% will give injection Arthemeter to all malaria cases.
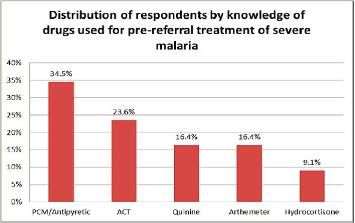
 Symptoms of severe malaria could be recognized by 70% while just 50% knew the correct pre?referral treatment. About two thirds (64.6%) knew quinine was safe for malaria treatment throughout pregnancy while 92% knew the required doses of IPT in pregnancy.
Symptoms of severe malaria could be recognized by 70% while just 50% knew the correct pre?referral treatment. About two thirds (64.6%) knew quinine was safe for malaria treatment throughout pregnancy while 92% knew the required doses of IPT in pregnancy.
This study shows substantial knowledge gap on malaria case management among top LGA health workers. Gaps identified include the use of chloroquine and indiscriminate use of injection Arthemeter. Referral procedures for severe malaria remain fair. Individual capacity building at improving malaria treatment practices need to begin with the supervisors if a significant change in treatment practices is to be expected at PHC level.
References
[1] Daniel J Kyabayinze et al. Use of RDTs to improve malaria diagnosis and fever case management at primary health care facilities in Uganda. Malaria Journal 2010, 9:200.
[2] National Guidelines for diagnosis and treatment of malaria. Federal Ministry of Health. March 2011