Diagnosis &Treatment Bill Brieger | 18 Oct 2013 04:05 am
Knowledge of Senior Local Government Level (LGA) Health Workers on Malaria Treatment Guidelines in a South Western Nigerian State
 Esther Ayandipo, Bolatito Aiyenigba, Bukola Omobowale, Adebola Karim?Mohamed, Olusimbo Ige & Abbar Umar from the USAID PMI/MAPS Project (Nigeria) and the Department of Community Medicine University of Ibadan recently presented their findings from interviews with key local government health managers at the Multilateral Initiative for Malaria 6th Pan African Malaria Conference in Durban South Africa. They have shared their presentation below.
Esther Ayandipo, Bolatito Aiyenigba, Bukola Omobowale, Adebola Karim?Mohamed, Olusimbo Ige & Abbar Umar from the USAID PMI/MAPS Project (Nigeria) and the Department of Community Medicine University of Ibadan recently presented their findings from interviews with key local government health managers at the Multilateral Initiative for Malaria 6th Pan African Malaria Conference in Durban South Africa. They have shared their presentation below.
The risk of severe malaria is reduced when the disease is diagnosed accurately and on time [1]. Artemisinin Combination Therapy (ACTs) is the first line of According to the Nigerian national guidelines, parasitological confirmation is recommended in all suspected cases of malaria [2]. Malaria treatment practices have remained suboptimal in many primary health facilities (PHCs) in Oyo State. Routine monitoring visits to public primary health facilities show use of Chloroquine for malaria treatment and indiscriminate use of injection Arthemether for treatment of uncomplicated malaria.
The Medical Officer of Health (MOH) /primary health care coordinator as the apex officers at the Local Government Areas (LGAs) are expected to supervise and ensure compliance to national malaria treatment guidelines at PHCs within their LGAs. This study aims to assess the knowledge of MOHs on malaria treatment guidelines as a measure of their supervisory effectiveness.
Oyo State has 33 LGAs. A cross sectional survey of all 33 MOHs and 17 assistant MOHs was conducted to assess knowledge of current malaria treatment guidelines using a semi structured questionnaire. Knowledge assessed include; current management of fever cases including diagnosis before treatment for malaria; preferred choice of antimalarial drug, symptoms of severe malaria and management of malaria in pregnancy. Descriptive analysis was done using SPSS version 16.
 A total of 50 health workers responded to the questionnaire. Doctors constituted 27%, nurse/midwives 62.5%, and CHOs 10.4% of respondents. Overall, 87.8% had been trained on malaria case management.
A total of 50 health workers responded to the questionnaire. Doctors constituted 27%, nurse/midwives 62.5%, and CHOs 10.4% of respondents. Overall, 87.8% had been trained on malaria case management.
Even though 98% believed that not all fever is malaria, 76% will still treat all fever cases for malaria. Just 62% knew that other causes of fever should be looked for when RDT is negative while 8% will go ahead and treat RDT negatives for malaria.
Many (93.8%) will use ACTs to treat RDT positive cases however 10.6% still felt Chloroquine is the mainstay treatment for malaria. 15.2% will give injection Arthemeter to all malaria cases.
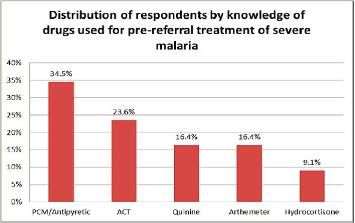
 Symptoms of severe malaria could be recognized by 70% while just 50% knew the correct pre?referral treatment. About two thirds (64.6%) knew quinine was safe for malaria treatment throughout pregnancy while 92% knew the required doses of IPT in pregnancy.
Symptoms of severe malaria could be recognized by 70% while just 50% knew the correct pre?referral treatment. About two thirds (64.6%) knew quinine was safe for malaria treatment throughout pregnancy while 92% knew the required doses of IPT in pregnancy.
This study shows substantial knowledge gap on malaria case management among top LGA health workers. Gaps identified include the use of chloroquine and indiscriminate use of injection Arthemeter. Referral procedures for severe malaria remain fair. Individual capacity building at improving malaria treatment practices need to begin with the supervisors if a significant change in treatment practices is to be expected at PHC level.
References
[1] Daniel J Kyabayinze et al. Use of RDTs to improve malaria diagnosis and fever case management at primary health care facilities in Uganda. Malaria Journal 2010, 9:200.
[2] National Guidelines for diagnosis and treatment of malaria. Federal Ministry of Health. March 2011