Community &Health Systems &Treatment Bill Brieger | 05 Nov 2014
Expanding Health Ministry Capacity to Deliver Malaria and Other Health Commodities at the Community Level in Nigerian States
Bright Orji of Jhpiego‘s Nigeria office presents a poster at the American Society of Tropical Medicine and Hygiene 2014 Annual Meeting at noon on 5th November. The poster represents Jhpiego’s technical assistance provided to seven Nigerian States as part the World Bank Malaria Booster Program. The abstract follows:
 The highly participative process of community directed interventions (CDI) was first pioneered in 1996 by the African Program for Onchocerciasis Control for the delivery of ivermectin. CDI was further tested and found effective in delivering other health commodities.
The highly participative process of community directed interventions (CDI) was first pioneered in 1996 by the African Program for Onchocerciasis Control for the delivery of ivermectin. CDI was further tested and found effective in delivering other health commodities.
In 2007 Jhpiego began a proof of concept project in Akwa Ibom State, Nigeria and learned that CDI could be a useful vehicle for increasing access to and coverage of malaria in pregnancy interventions. Building on this success, Jhpiego expanded this work to include integrated community case management of malaria, diarrhoea and pneumonia. through community led efforts.
 The World Bank Malaria Booster Program, observing Jhpiego’s efforts in Akwa Ibom State, asked the Nigeria National Malaria Control Program to enlist Jhpiego’s help in building the capacity of seven State Ministries of Health (MOH) to organize CDI for what was termed the malaria plus package consisting of community case management and health promotion activities. The scale-up process started with workshops for state CDI implementation teams consisting of staff from malaria control and primary health care in the MOHs.
The World Bank Malaria Booster Program, observing Jhpiego’s efforts in Akwa Ibom State, asked the Nigeria National Malaria Control Program to enlist Jhpiego’s help in building the capacity of seven State Ministries of Health (MOH) to organize CDI for what was termed the malaria plus package consisting of community case management and health promotion activities. The scale-up process started with workshops for state CDI implementation teams consisting of staff from malaria control and primary health care in the MOHs.
 Then these state teams developed their own intervention packages and organized workshops for local government teams, who in turn trained staff from their front line health facilities. These facility staff mobilized communities in their facility catchment areas (wards) to select volunteers for training on the CDI process and intervention package.
Then these state teams developed their own intervention packages and organized workshops for local government teams, who in turn trained staff from their front line health facilities. These facility staff mobilized communities in their facility catchment areas (wards) to select volunteers for training on the CDI process and intervention package.
Although technical assistance was provided to each state, challenges arose including commodity supplies and coordination among different program units within the state MOHs. In conclusion, state teams can train local government teams, ultimately cascading CDI to the community in order to scale up maternal and child health interventions.
Human Resources &Training &Treatment Bill Brieger | 03 Nov 2014
Inspiring Quality in Pre-Service Education on Malaria in Tanzania: Jhpiego at ASTMH
Monday at noon (3 October 2014) at the American Society for Tropical Medicine and Hygiene Annual Meeting in New Orleans, Jhpiego will be presenting two posters. Grace Qorro of Jhpiego’s Tanzania office has one entitled: #Quality Inspired Project – A Key to Achieving Results with Malaria Interventions.” Her abstract is shared below.
 With an aim to accelerate malaria case management, Tanzania Ministry of Health and Social Welfare (MoHSW) is strengthening its pre-service education program to ensure graduates have the right knowledge and skills to diagnose and treat malaria. Investment in pre-service education lessens the burden on in-service training since those entering the workforce will have the knowledge and skills they need to provide.
With an aim to accelerate malaria case management, Tanzania Ministry of Health and Social Welfare (MoHSW) is strengthening its pre-service education program to ensure graduates have the right knowledge and skills to diagnose and treat malaria. Investment in pre-service education lessens the burden on in-service training since those entering the workforce will have the knowledge and skills they need to provide.
 Jhpiego, through MAISHA (Mothers And Infants Safe, Healthy and Alive) program, provided technical assistance to the MoHSW to help develop a pre-service malaria case management-updates Learning Resource Package (LRP), which includes: Facilitator’s Manual, Participant’s Manual, Activity Worksheets and Training Modules addenda.
Jhpiego, through MAISHA (Mothers And Infants Safe, Healthy and Alive) program, provided technical assistance to the MoHSW to help develop a pre-service malaria case management-updates Learning Resource Package (LRP), which includes: Facilitator’s Manual, Participant’s Manual, Activity Worksheets and Training Modules addenda.
 The LRP was developed based on national malaria policy, guidelines and in-service training materials; it is taught using job aids, power point presentations, video demonstration and numerous case scenarios which reflect what actually happens in real life situations at service delivery points. The LRP aims at reinforcing appropriate practices for care of malaria patients and management of commodities with emphasis on parasite-based diagnosis and compliance to results, proper recording and reporting; and management of malaria in special situations and groups.
The LRP was developed based on national malaria policy, guidelines and in-service training materials; it is taught using job aids, power point presentations, video demonstration and numerous case scenarios which reflect what actually happens in real life situations at service delivery points. The LRP aims at reinforcing appropriate practices for care of malaria patients and management of commodities with emphasis on parasite-based diagnosis and compliance to results, proper recording and reporting; and management of malaria in special situations and groups.
 The training package is well organized with laboratory and medical supplies which gives each participant an opportunity for hands-on activity to acquire and strengthen their skills. Checklists to guide Quality Assurance/Quality Improvement (QA/QI) processes have been included in these training materials.
The training package is well organized with laboratory and medical supplies which gives each participant an opportunity for hands-on activity to acquire and strengthen their skills. Checklists to guide Quality Assurance/Quality Improvement (QA/QI) processes have been included in these training materials.
The project successfully provided competence-based orientation on malaria case management updates to 210 medical instructors. Annually, it reaches more than 4,000 students from eight Zonal Health Resource Centers and 480 students from Medical Universities.
There is a need to incorporate the addenda developed into these training modules for easy use. In the near future, clinical skills-mentorship will be conducted in selected schools using the nationally approved QA/QI checklists.
Community &Private Sector &Treatment Bill Brieger | 03 Nov 2014
Ghana at ASTMH: Mapping out of antimalarial drugs on stock at the market in a rural districts of Ghana
The first Poster Session of the American Society of Tropical Medicine and Hygiene (Monday noon) will feature a study on availability of malaria medicines in rural Ghana. “Mapping out of antimalarial drugs on stock at the market in a rural districts of Ghana” was developed by Alexander A. Nartey, Evelyn K. Ansah, Patricia Akweongo, Gloria A. Nartey, Mary A. Pomaa, Doris Sarpong, Clement Narh, and Margaret Gyapong of the Dodowa Health Research Centre.
American Society of Tropical Medicine and Hygiene (Monday noon) will feature a study on availability of malaria medicines in rural Ghana. “Mapping out of antimalarial drugs on stock at the market in a rural districts of Ghana” was developed by Alexander A. Nartey, Evelyn K. Ansah, Patricia Akweongo, Gloria A. Nartey, Mary A. Pomaa, Doris Sarpong, Clement Narh, and Margaret Gyapong of the Dodowa Health Research Centre.
 Antimalarial drugs are a very important component of any policy for effective reduction of morbidity and mortality related to the malaria disease. The availability of efficacious and high quality antimalarials and their correct use can mitigate the risk of morbidity and mortality among the people of sub-Saharan Africa who have the highest risk of contracting and dying
Antimalarial drugs are a very important component of any policy for effective reduction of morbidity and mortality related to the malaria disease. The availability of efficacious and high quality antimalarials and their correct use can mitigate the risk of morbidity and mortality among the people of sub-Saharan Africa who have the highest risk of contracting and dying
from malaria.
Chemical (medicine) shops are major source of care for most developing countries where anti-malarial drugs can be purchase at the counter. The paper seeks to identify the different kinds of anti-malarial drugs on the market for malaria treatment in a rural district in Ghana.
 A structured questionnaire was used during two seasons (peak and low malaria transmission seasons) to collect information on anti-malarial drugs from all 58 chemical shops within the Dangme West district now (Shai Osudoku and Ningo Prampram districts). Pictures of the anti-malarial drugs were taken,
A structured questionnaire was used during two seasons (peak and low malaria transmission seasons) to collect information on anti-malarial drugs from all 58 chemical shops within the Dangme West district now (Shai Osudoku and Ningo Prampram districts). Pictures of the anti-malarial drugs were taken,
The active ingredients, and also the source of the drugs documented. GIS locations of the shops were also recorded to ascertain the proximity of the shops to households in the communities. Majority (72.0%) of the chemical and pharmacy shop owners are males. Only 7.0% of the shops are pharmacy while the remainder is licensed chemical shops.
 The total numbers of antimalarial drugs counted were forty nine (49). Among the stock, 4.2% were quinine, 31.9% of them were monotherapies such as artemether, Amodiaquine, Artesunate etc. Altogether, 59.4% of the artemisinin combination therapies (ACTs) were artemether + Lumefantrine, 25.0% were Artesunate + Amodiaquine.
The total numbers of antimalarial drugs counted were forty nine (49). Among the stock, 4.2% were quinine, 31.9% of them were monotherapies such as artemether, Amodiaquine, Artesunate etc. Altogether, 59.4% of the artemisinin combination therapies (ACTs) were artemether + Lumefantrine, 25.0% were Artesunate + Amodiaquine.
Other antimalarials observed were 9.4% Sulfadoxine + Pyrimethamine and 3.1% of of Artesunate + Sulfamethoxypyrazine + Pyrimethamine. About 47% of the anti-malarial drugs were pediatric formulations.
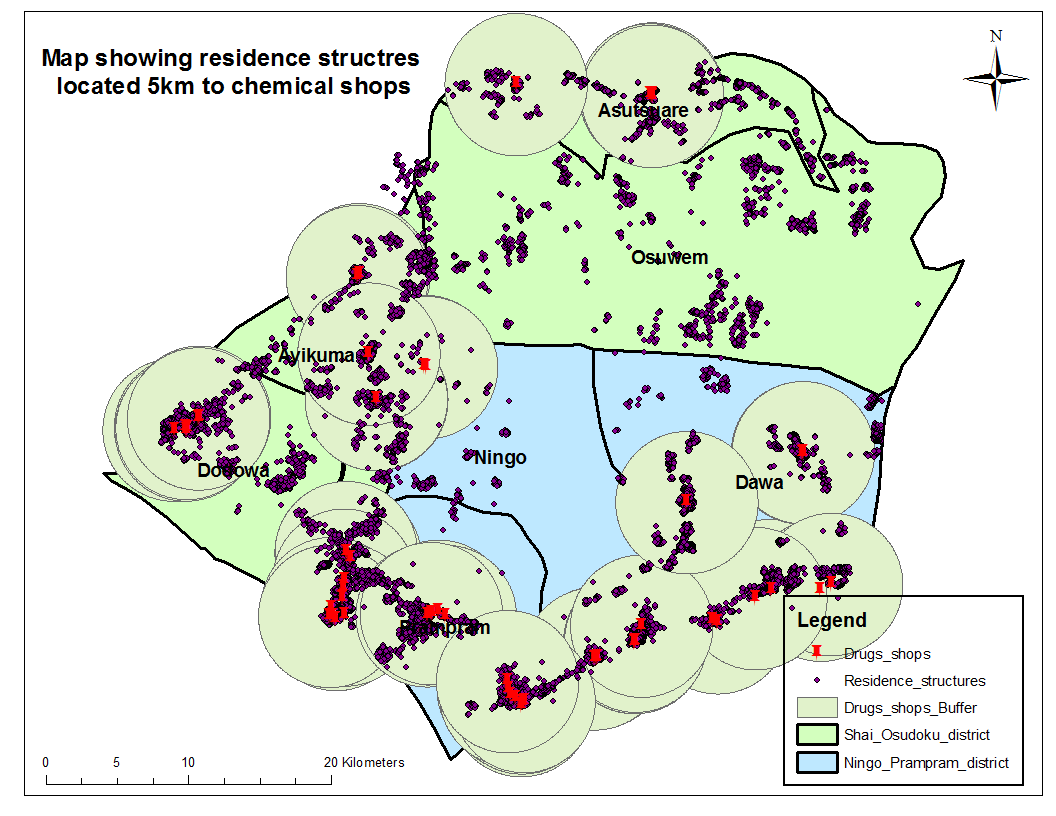 GIS mapping shows that majority of the households are within a periphery of 5km to a chemical shop.
GIS mapping shows that majority of the households are within a periphery of 5km to a chemical shop.
The national antimalarial drug policy recommends the use of ACTs for malaria treatment however; all sorts of anti-malarial drugs which are not ACTs are in stock at the chemical shops in Ghana. Chemical shops are closer to households and play a very important role in the treatment of malaria hence there is the need to train chemical sellers to stock and administer the recommended antimalarials.
Community &Integration &Treatment Bill Brieger | 11 Oct 2014
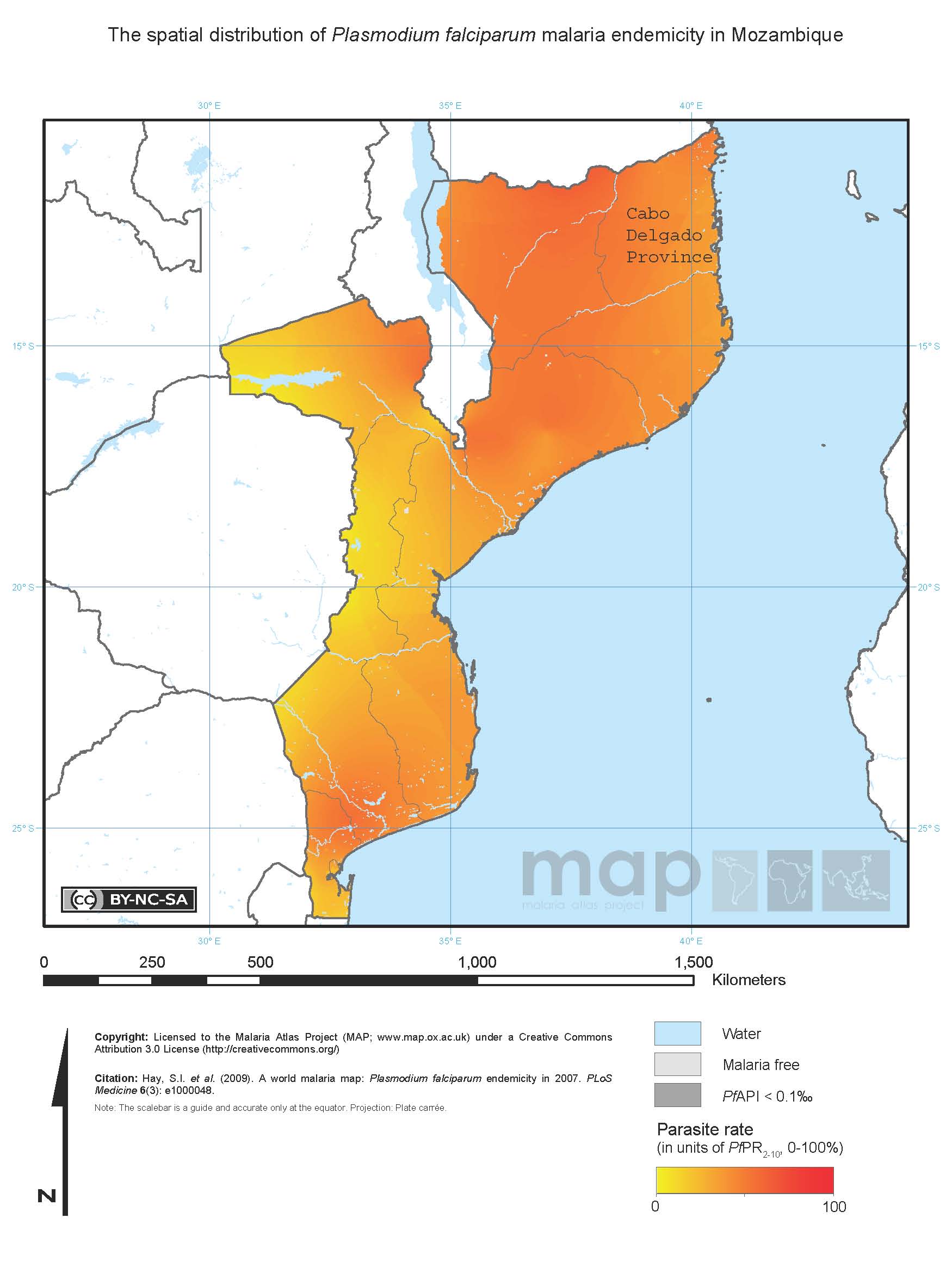
Is community case management sustainable in Mozambique? A qualitative policy analysis
The recently concluded Global Health Systems Research Symposium in Cape Town featured a number of abstracts that touched directly or indirectly on malaria. Malaria services and movement toward malaria elimination cannot be achieved in a country without a strong health system that involves both communities, program staff and policy makers.
 Below is an abstract by Baltazar Chilundo, Julie Cliff, Alda Mariano, Daniela Rodrigues, and Asha George of the University Eduardo Mondlane, Mozambique and the Johns Hopkins School of Public Health on the sustainability of community case management, building on longstanding community health worker programs. They stress the importance of community commitment, an often missing factor when CHW and CCM programs are organized by national agencies.
Below is an abstract by Baltazar Chilundo, Julie Cliff, Alda Mariano, Daniela Rodrigues, and Asha George of the University Eduardo Mondlane, Mozambique and the Johns Hopkins School of Public Health on the sustainability of community case management, building on longstanding community health worker programs. They stress the importance of community commitment, an often missing factor when CHW and CCM programs are organized by national agencies.
“In Mozambique, community case management (CCM) of diarrhoea, malaria and pneumonia is embedded in the national community health worker (CHW) programme. Since 1978 this programme functioned fitfully and was relaunched in 2010, with a target to train and retrain over 6000 CHWs.
 “Considering the checkered history of the CHW program, sustainability lies at the heart of concerns related to the design and implementation of CCM in CHW programs at scale in Mozambique and in people centred health systems more broadly.
“Considering the checkered history of the CHW program, sustainability lies at the heart of concerns related to the design and implementation of CCM in CHW programs at scale in Mozambique and in people centred health systems more broadly.
“Using qualitative retrospective case study methodology, we reviewed 54 national documents and interviewed 21 key national informants for a policy analysis of CCM in Mozambique. The data were analysed thematically according to a sustainability framework and validated though a national debriefing workshop.
“The sustainability of CCM was facilitated by embedding it in the national CHW programme, which was relaunched after wide consultation within government and with supportive donors and non-governmental organizations (NGOs).
“Although communities were not widely consulted, they were eager for CHWs to provide curative services. The new CHW program aimed to improve CHW retention, by paying them a salary and giving priority to females. However, salary costs come from partners and in practice most CHWs are male.
“The poor capacity of the health system to adequately supervise CHWs and guarantee drug supplies for CCM, the dependence on external partners for funding, and on NGOs for implementation and the lack of mobilization of communities and top policy makers remain critical concerns.
“Embedding CCM in the national CHW programme favoured sustainability, however this made CCM susceptible to the same factors that undermine sustainability of the CHW programme. Moving forward, these policy concerns need to be addressed to ensure a national CHW program, responsive to community needs, supportive of CHW themselves and owned by national governments.”
Community &Drug Quality &Private Sector &Treatment Bill Brieger | 08 Oct 2014
Registered drug shops are preferred for treating acute febrile illness in rural Uganda
The recently concluded Global Health Systems Research Symposium in Cape Town featured a number of abstracts that touched directly or indirectly on malaria. Malaria services and movement toward malaria elimination cannot be achieved in a country without a strong health system that involves both communities, program staff and policy makers.
Below is an abstract by Freddy Kitutu, Chrispus Mayora, Phyllis Awor, Forsberg Birger, Stefan Peterson, and Henry Wamani of Makerere University and the Karolinska Institute on use of medicine shops in Uganda.
“Under-five child mortality in Uganda is still high and majority is caused by easily treatable pneumonia, malaria and diarrhoeal diseases among the poorest people. One of the reasons for these deaths is the lack of timely access to proven life saving medicines. This hinders progress towards attainment of MDG 4 target by 2015.
“To increase access to quality medicines and diagnostics for child febrile illnesses, Makerere University School of Public Health (MakSPH) in collaboration with WHO Alliance for Health Policy and Systems Research, is doing a project to assess the potential to deliver quality integrated care for malaria, pneumonia and diarrhoea using integrated community case management (iCCM) strategies and tools. Hence, an assessment was conducted to determine baseline care seeking preferences.
“A baseline household survey interviewed caregivers of children under-five years. The study protocol and data collection tools had been reviewed and approved by Research and Ethics Committees at WHO, MakSPH and Uganda National Council of Science and Technology.
“A total of 2606 households were surveyed. The main childhood diseases reported included fever (70%), cough (77%), and diarrhoea (40%) convulsions (16%) Most households use private drug shops to purchase medicines to manage these illnesses. Use of drug shops was attributed to long distances to public health facilities, availability and reliability of drug stocks at drug shops, perceived high quality of services, and options for credit.
“Interventions that target public health facilities are likely to miss many healthcare seekers especially the poor in rural distant areas. Conclusion: Drug shops are the convenient and preferred outlets for rural poor communities, and therefore need to be included in interventions such as iCCM strategy.
“Significance for the selected field-building dimension: This abstract presents findings from the baseline assessment prior to introducing a health system intervention in drug shops to improve access to and quality of care for under-five children.”
Private Sector &Procurement Supply Management &Treatment Bill Brieger | 05 Oct 2014
Licensed chemical sellers and antimalarial prices in northern Ghana under the affordable medicines facility
The recently concluded Global Health Systems Research Symposium in Cape Town featured a number of abstracts that touched directly or indirectly on malaria. Malaria services and movement toward malaria elimination cannot be achieved in a country without a strong health system that involves both communities, program staff and policy makers.
Below is an abstract by Heather Lanthorn of the Harvard School of Public Health on the AMFm program testing in Ghana. Other abstracts will appear subsequently.
“The Affordable Medicines Facility – malaria (AMFm) represents an important experiment in using private retail chains to improve access to medicines in low- and middle-income countries. AMFm aimed to make quality-assured artemisinin-based combination therapies (QA.ACTs) accessible at the variety of outlets where citizens treat fevers. In Ghana, where ACTs are legally sold over the counter, Licensed Chemical Sellers (LCS) are a key antimalarial provider.
“I use a framework adapted from industrial organization to study a unique, geo-coded data set of 250 LCSs in and around Tamale, Ghana collected explicitly for this study. Through well-integrated quantitative (multiple logistic regression) and qualitative (open thematic analysis) approaches, I analyze: the experiences of LCSs with AMFm; LCS reported compliance with recommended retail prices (RRPs); LCS economic and social explanations for compliance; and associations between LCS objective characteristics – including geo-location – and RRP compliance.
“We find high stocking of subsidized QA.ACTs and high RRP compliance. 18% of LCSs report selling above the RRP. The majority of non-compliers cite rising prices from their supplier as the major determinant of their own pricing. The majority of non-compliers sold at USD 1.5 rather than the RRP, USD 1.0. Indeed, in the quantitative analysis, RRP compliance is most clearly associated with the distributor prices and with LCS reputation (years in business).
 “A driving motivation for experimentally piloting AMFm was to learn whether the QA.ACT subsidy would be passed on to end-line private retailers and, in turn, to consumers. We find that, largely, it is. By considering LCSs both as economic agents and community members, the present analyses accord with, complement and innovate on the large, independent evaluation of AMFm, which focused on prices but neither objective nor perceptual explanations for price-compliance.”
“A driving motivation for experimentally piloting AMFm was to learn whether the QA.ACT subsidy would be passed on to end-line private retailers and, in turn, to consumers. We find that, largely, it is. By considering LCSs both as economic agents and community members, the present analyses accord with, complement and innovate on the large, independent evaluation of AMFm, which focused on prices but neither objective nor perceptual explanations for price-compliance.”
Communication &Treatment Bill Brieger | 27 Aug 2014
Documenting SBCC’s Important Role in Malaria Case Management

Are there examples of effective social and behavior change communication (SBCC) for malaria case management that can be shared with other countries looking to improve their programming?
After examining research, policy documents and program evaluations from Ethiopia, Rwanda, Senegal and Zambia to determine whether effective SBCC activities have been used to improve malaria case management, I haven’t come across many strong examples. Program reports don’t tend to mention SBCC program evaluation. Reports that do mention it are difficult to find credible because the indicators used don’t address the real determinants of behavior.
Behavioral researchers have spent decades trying to illustrate just how insufficient it is to measure only knowledge. Attitudinal factors like perceived risk, self-efficacy and cultural norms are important behavioral determinants conspicuously missing from reports on malaria case management program design and evaluation.
Here’s an example of an attitudinal indicator related to malaria case management: Proportion of health care service providers that believe new diagnosis and treatment guidelines (test before you treat) are effective. I found a carefully designed study (a cluster-randomized controlled trial) assessing community health workers ability to diagnose and treat children. After a brief training, health workers evaluated over a thousand children with fever and accurately treated them based on disease classification 94%-100% of the time. Of note in this study: facility-based health workers (nurses or doctors) in two districts of the Southern Province of Zambia were less likely to follow guidelines or honor the results of rapid diagnostic tests than community health workers.
MalariaCare recently conducted a series of interviews revealing the same pattern. A 2014 systematic review on malaria in pregnancy found health care provider reliance on clinical diagnosis and poor adherence to treatment policy is a consistent problem. Perhaps doctors feel their considerable experience enables them to diagnose patients accurately without policy-mandated tests? Do community health workers adhere to a policy more tightly because they have a limited number of tasks and take pride in fastidiously carrying them out? The point is that the most educated individuals in an entire country – or those most likely to have accurate, timely information – can be outperformed by individuals with little or no formal education when exposed to the exact same set of government guidelines.
The difference is attitude.
Are programs targeting the attitudinal barriers behind adherence to malaria test results? Are evaluators measuring changes in these key attitudes? You can’t measure impact if you didn’t actually change behavior and people don’t change the way they act unless their decision-making process – in all of its beautiful human complexity – is acknowledged and addressed.
The Roll Back Malaria Partnership (RBM) has an SBCC community of practice made up of public health professionals working to promote a more rigorous, evidence-based approach to malaria SBCC program design and evaluation. One of the group’s products, the Malaria Behavior Change Communication Indicator Reference Guide, was developed to help Ministries of Health, donor agencies and implementing partners design and measure levels of behavior change related to malaria prevention and case management. The guide contains a list of indicators that go beyond knowledge and awareness into important behavioral determinants like attitudes. The guide has been available since February 2014 and this month the group is happy to announce its publication in Portuguese (it is also available in French and English).
The answer to the question posed by this desk review is that there is a lot of great work being done in malaria case management but it is being in done in a way that makes it difficult for others to follow. This new tool was developed to ensure SBCC programming is designed in such a way that its impact can be measured and replicated.
Private Sector &Treatment &Universal Coverage Bill Brieger | 25 Apr 2014
Malaria and febrile illness care seeking in Bauchi State, Nigeria
World Malaria Day 2014 was observed at the Johns Hopkins Bloomberg School of Public Health. Admiral Tim Ziemer, the Coordinator of the US President’s Malaria Initiative was keynote speaker. Other speakers from the NGO and faith based organization community also talked about the importance of partnership in fighting a disease that still claims 600,000 lives annually. In addition 21 posters were presented.
Below is the abstract of one poster representing our work with USAID’s Targeted States High Impact Project in Nigeria.
Malaria and febrile illness care seeking in Bauchi State, Nigeria: context for improving case management at the primary level
Seeking of appropriate and q uality care for childhood illnesses is a major challenge in much of Africa including Bauchi State, Nigeria. In advance of an intervention to improve available care in the most common points of service (POS), government primary health care centers (PHCs) and patent medicine vendors (PMV), a survey was done of child caregivers in four districts concerning responses to febrile illness, suspected malaria, acute respiratory disease and diarrhea. The ethical review committee in the Bauchi State Ministry of Health approved of the study.
uality care for childhood illnesses is a major challenge in much of Africa including Bauchi State, Nigeria. In advance of an intervention to improve available care in the most common points of service (POS), government primary health care centers (PHCs) and patent medicine vendors (PMV), a survey was done of child caregivers in four districts concerning responses to febrile illness, suspected malaria, acute respiratory disease and diarrhea. The ethical review committee in the Bauchi State Ministry of Health approved of the study.
A total of 3077 children below the age of five were identified in the households sampled. Their mothers, fathers or other caregivers consented and were interviewed. Among the children 74% had any Illness, 57% had fever, 26% had cough, and 15% had diarrhoea. Only 8.7% of 1186 febrile children had their blood tested.
Care seeking from PMVs varied from 45% with fever, 40% with cough to 36% with diarrhoea. Care from public sector POS varied from 26-33%. Treatment that might be considered ‘appropriate’ for each also varied with 30% receiving antimalarial drugs for suspected malaria, 20% getting oral rehydration solution for diarrhoea and 50% being given an antibiotic for a suspected acute respiratory illness.
The results show that providing quality integrated case management with appropriate commodities through PHCs and PMVs can improve the illness care of a majority of children in Bauchi State, and interventions are currently being planned to do this.
Poster by … William R. Brieger, MPH, CHES, DrPH 1, Bright Orji, MPH 2, Masduk Abdulkarim 3, (1) International Health, Bloomberg School of Public Health, The John Hopkins University, 615 N Wolfe St, Baltimore, MD 21205 (and Jhpiego). (2) Jhpiego, Thames St, Baltimore, MD 21231`. (3) Targeted States High Impact Project USAID Nigeria, Bauchi, Nigeria.
Community &Diagnosis &Treatment Bill Brieger | 20 Mar 2014
iCCM Symposium – Summary from the Accra Meeting
Theresa Diaz, Senior Health Advisor, UNICEF, and colleagues on the integrated Community Case Management (iCCM) Evidence Review Symposium planning committee have made available a summary of the key lessons and experiences from the meeting in Accra as found below, We thank them for their efforts.
 Symposium summary and conclusions
Symposium summary and conclusions
Between 3 and 5 March 2014, over 400 individuals from 35 countries in sub-Saharan Africa and 59 international partner organizations gathered in Accra, Ghana for an Integrated Community Case Management (iCCM)[1] Evidence Review Symposium. The objective of the symposium was twofold: first, to review the current state of the art of iCCM implementation by bringing together researchers, donors, government, implementers and partners to review the map of the current landscape and status of evidence in key iCCM programme areas, in order to draw out priorities, lessons and gaps for improving child and maternal-newborn health. Second, to assist African countries to integrate and take action on key frontline iCCM findings presented during the evidence symposium around eight thematic areas:
- Coordination, Policy Setting and Scale up: The current state of iCCM policies in Africa and challenges in development of policy and scale up
- Human Resources and Deployment: Community health worker (CHW) selection, geographic disbursement, motivation and retention
- Supervision & Performance Quality Assurance: Strategies to ensure high quality care including strategies for effective training, use of alternative models for supervision, and the role of mHealth to support and motivate CHWs to provide quality care
- Supply Chain Management: Which systems ensure continuous supply, how best to forecast needs
- Costs, and cost effectiveness and financing: Identifying cost drivers, improving cost effectiveness and the importance of minimizing patient costs
- Monitoring, Evaluation and Health Information Systems: Innovations in monitoring, integrating with health management information systems, using results to drive programmatic decision-making and improvements, evaluation design and methods
- Demand generation and social mobilisation: The relationship between iCCM and care-seeking, treatment utilisation and treatment adherence, effective strategies to generate demand
- Impact and outcome evaluations: Review of 18 iCCM programme studies with coverage or mortality data.
Conclusions
Several lessons are clear based on the evidence were presented and may serve as recommendations for future iCCM implementation, as relevant:
- National government leadership is essential.
- iCCM must be integrated in national health systems and seen as a priority means of delivering care, and embedded as a costed element of national health sector plans, with a clear budget line.
- Integration is key among all health-related programmes at community level (water and sanitation, nutrition, etc.).
- Coordination mechanisms should extend beyond health to include other sectors (e.g., finance).
- Advocacy on the iCCM model is still paramount to its dissemination.
- There is no single model of human resource management for community based interventions. Countries reported having paid or volunteer CHWs, as well as CHWs with significant skills operating in conjunction with volunteers.
- Charging fees decreases utilisation.
- High supervision rates increase quality, utilisation and motivation.
- Having fewer stock outs increases utilisation.
- Providing treatment for malaria, pneumonia and diarrhoea combined increases utilisation of services for each illness.
- Using rapid diagnostic tests (RDTs) decreases malaria and pneumonia treatments suggesting more appropriate antibiotic/antimalarial usage and improved quality of treatment.
- Private public partnerships should be explored as vehicles for iCCM implementation. In addition, iCCM can be used as vehicle for private sector quality improvement in settings where the private sector is an important source of care for children.
- New technologies such as Rapid SMS, mHealth, and mTRAC can facilitate monitoring and management.
- iCCM programmes must be well documented, periodically reviewed and evaluated in order to guide implementation at scale.
In addition, there were two key messages that emerged from the Symposium:
Increase utilisation of iCCM to be more cost efficient and to ensure maximum impact
- by deploying services to areas of greatest need
- by assessing demand barriers and addressing them through community engagement and mobilisation
- by structuring supervision and management to be affordable and effective
- while maintaining quality of services, continuous supplies and high levels of standardised reporting.
Use routine reporting data to assess progress and only conduct endline evaluations of impact after being at scale (i.e., 80% of providers trained and equipped) with high utilisation for at least 1 year
- Examine routine data to know if you have been providing high rates of appropriate treatments
- Once your routine data show you are providing high rates of treatment, collect data on coverage and quality, and model mortality based on the Lives Saved Tool (LiST)
- Final evaluations should include data from routine sources, as well as contextual, qualitative, coverage, quality of care and costing data
- Given that we know that iCCM treatments are effective in decreasing mortality, and that there are significant methodological challenges attributing outcomes and impact specifically to iCCM, it is perhaps more critical to conduct operational research that supports programmes to increase treatment rates rather than “impact evaluations of iCCM.” It is also important to use routine programme data to track indicators and household surveys (baseline and follow up) to measure care seeking behaviour, source of treatment and timeliness of treatment to assess if these outcomes are moving in the right direction.
The way forward
With 2015 fast approaching, the time for improving iCCM implementation is now. We have effective interventions that respond to the major causes of child mortality and are well packaged for delivery. We have evidence showing that many treatments can be delivered successfully in the community, and now have innovations that facilitate community-based programming, including Rapid Diagnostic Test (RDTs) and mobile technologies. In addition, there are important new opportunities to mobilise resources from domestic as well as external funds (e.g., the Global Fund to Fight AIDS, Tuberculosis and Malaria) and, in many countries, to integrate public private partnerships with government systems.
Following discussions about the opportunities and challenges in their respective countries, participants are poised to work with their colleagues and partners to ensure that iCCM programmes are based on the latest evidence and are most appropriate for, and integrated into, their particular health systems and contexts.
This Symposium was made possible by the generous support of the Government of Canada and the Bill and Melinda Gates Foundation with additional support from USAID. It was coordinated by UNICEF in conjunction with the US Fund for UNICEF, MCHIP, John Snow, Inc., International Rescue Committee, Malaria Consortium, Management Sciences for Health, Population Services International, the MDG Health Alliance, Save the Children, the World Health Organisation, UNICEF Canada, TDR, and the Journal of Global Health. These organizations endorse the findings from this symposium and encourage countries to base their iCCM programs on the evidence presented.
More information regarding the Symposium is available at www.iccmsymposium.org.
[1] iCCM is a strategy to extend case management of childhood illness beyond health facilities so that more children have access to lifesaving treatments. The iCCM package can differ based on particular contexts, but most commonly includes diarrhoea, pneumonia and malaria, and in some cases newborn health and malnutrition as well. In the iCCM model, community health workers (CHWs) are identified and trained in diagnosis and treatment of key childhood illnesses, and also in identifying children in need of immediate referral (Source: CCM Central, http://ccmcentral.com/about/).
Community &Treatment Bill Brieger | 04 Mar 2014
Moving Toward Community Case Management of Malaria in Malawi
Guest posting by Jhpego‘s John Munthali, Malaria Program Officer on the Support for Service Delivery Integration-Services (SSDI-Services) Project, a reproductive, maternal and child health project in Malawi.

Health Surveillance Assistant Treating Child
Case Management with the appropriate antimalarial drug for children below five years of age in Malawi children within 24 hours has not changed much since the Roll Back Malaria Partnership was launched in 2000. RBM set a target of 80% for the year 2010. In 2000 only 10% received the approved drug of that time within 24 hours. Various national surveys including Demographic Health Survey (DHS), and Malaria Indicator Survey MIS) showed an increase to 23% by 2004, but this has not changed perceptibly in the intervening years with only 24% of these children getting the correct medicine on time in 2012.
Integrated community case management (iCCM) was envisioned as an approach to address these coverage/access challenges. The implementation platform is a sector-wide approach focusing on implementation of the national Essential Health Package (EHP) targeting 13 priority health interventions: Approaches emphasized promotion of equity by scaling up access to underserved populations through Community Mobilization (CM), iCCM, Community Based Maternal and Newborn Care (CBMNC) and Scaling Up Nutrition (SUN).
No missed opportunity is aimed for by promotion of integration of EHP services at all levels and by promotion of continuum of care from household to hospital. Jhpiego through USAID’s Support for Service Delivery Integration (SSDI) project supports iCCM. iCCM services delivered by Health Surveillance Assistants (HSAs) at village clinics to treat sick children with pneumonia, diarrhea and malaria including malnutrition screening, use malaria Rapid Diagnostic Tests (mRDTs) and use of rectal artesunate for pre-referral treatment of severe malaria is in the pipeline.
So far 96 trainers refreshed in iCCM. In turn these have trained 722 HSAs on iCCM in all 15 SSDI project districts. The project has also supported ongoing iCCM activities through supervision and mentoring. Equipment for iCCM has been distributed to HSAs. Now there are 1846 HSAs providing iCCM in the 15 districts. They can test and treat for malaria, check for palmar pallor for anemia, and count respirations per minute for acute respiratory infections among other skills.so far HSAs have treated 530 000 cases of malaria in the SSDI supported districts.
Challenges include work overload for HSAs, especially when involved in facility work as well. Transport problems affect some HSAs that reside outside the catchment area. Delays in procurement of the necessary equipment negatively affected the roll out of certain services. Inadequate supervision of services, especially at community level is common. There are weak referral linkages and follow up mechanisms between communities and health facilities. Finally there are drug stock-outs in some village clinics.
Therefore need exists to strengthen integration of service delivery at village clinics and health facilities through better supervision of HSAs. Strengthening of referral linkages and follow-up is also required. Community sensitization will continue to stress the importance of early care seeking and compliance with treatment regimens.