Drug Quality &Private Sector &Treatment Bill Brieger | 23 May 2015
Verifying Malaria Medicines on Your Mobile
On their website Sproxil says that, “Sproxil actively supports Nigeria’s National Agency for Food and Drug Administration and Control (NAFDAC) in the fight against counterfeiting by pioneering Nigeria’s first Mobile Authentication Service.” They note further that …
“On February 2, 2010, NAFDAC launched the NAFDAC MAS, putting the power of product verification right in the hands of the consumer. MAS is powered by Sproxil’s award-winning cloud-based Mobile Product Authentication™ technology, and remains the world’s largest nation-wide implementation of consumer-facing SMS anti-counterfeiting technology in the world.”
Below are two malaria medicine packets recently purchased. After scratching the small label (see it circled, we got the SMS messages as posted. The NAFDAC registration number alone is not enough to ascertain the validity. This is a smart procedure, even without a smart phone. Of course one still needs to read the expiry dates!
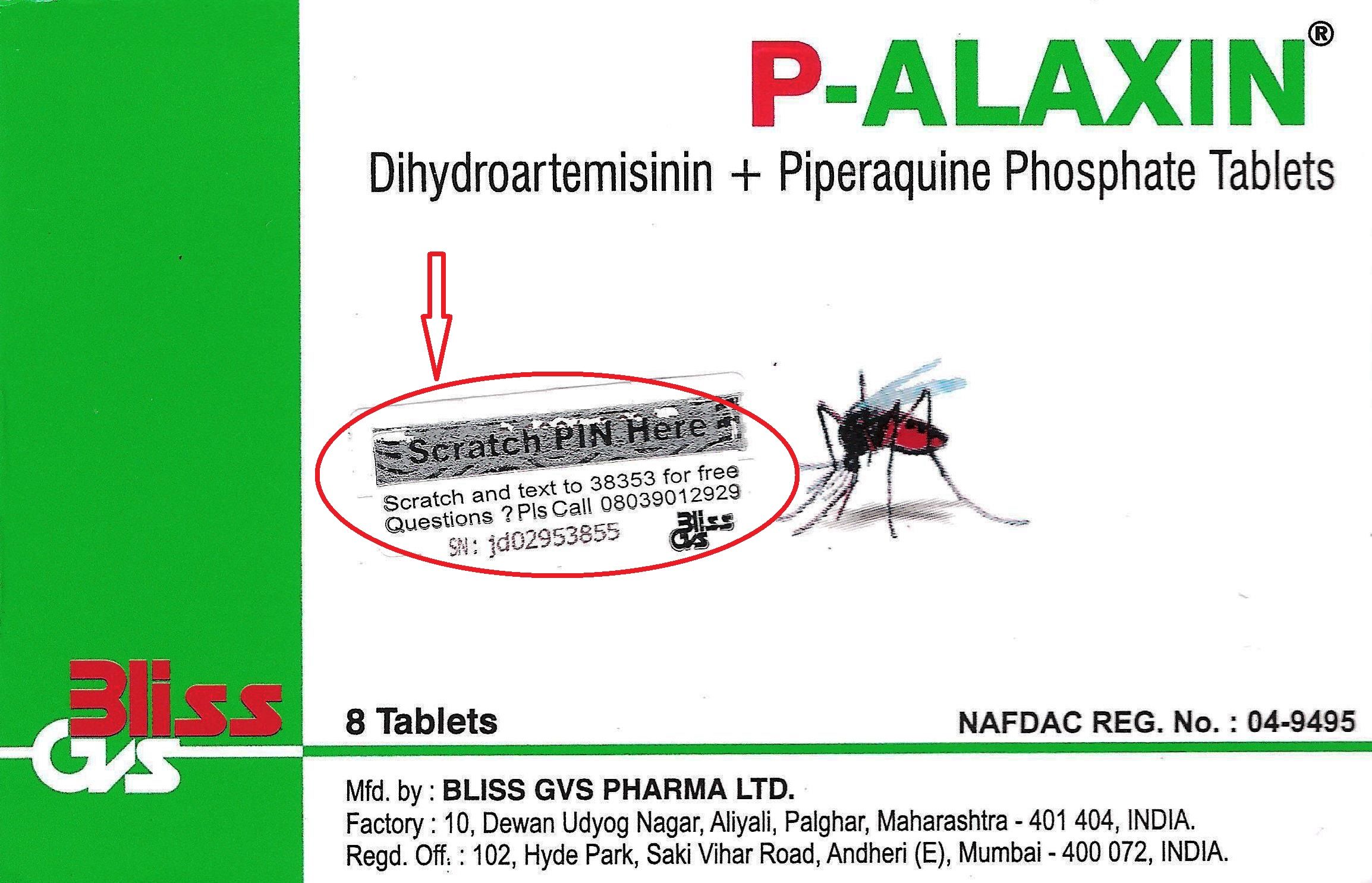 1. OK Genuine P-Alaxin Tablet. Your PIN:949769012921 NRN:04-9495 Problem? Call 08039012929 NAFDAC & Bliss Care Sproxil SMS
1. OK Genuine P-Alaxin Tablet. Your PIN:949769012921 NRN:04-9495 Problem? Call 08039012929 NAFDAC & Bliss Care Sproxil SMS
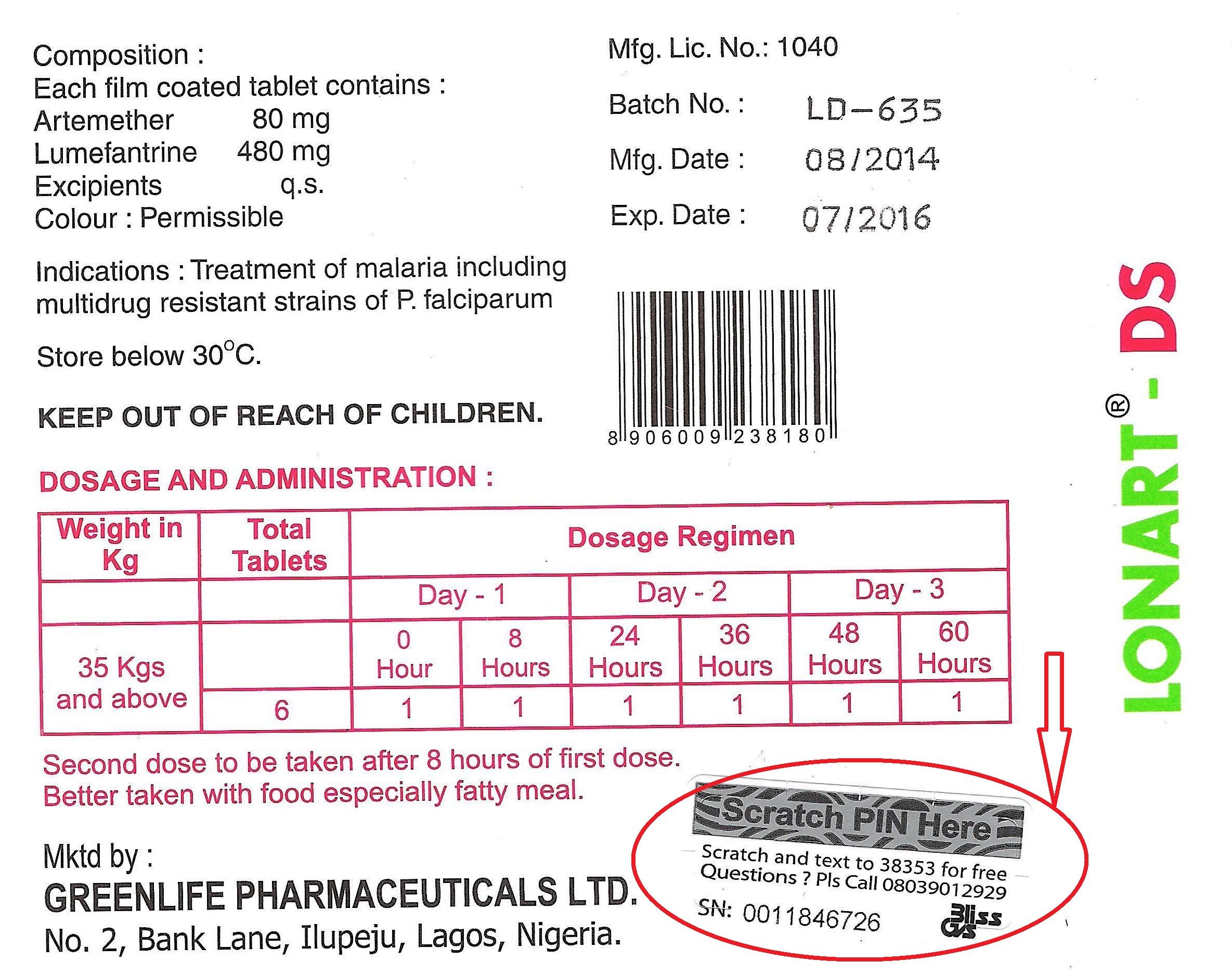 2. OK Original Lonart DS tabs NRN:04-9927 Use mosquito nets to help avoid malaria Problem? Call 08039012929 NAFDAC & GREENLIFE CARE Sproxil Solution
2. OK Original Lonart DS tabs NRN:04-9927 Use mosquito nets to help avoid malaria Problem? Call 08039012929 NAFDAC & GREENLIFE CARE Sproxil Solution
Private Sector &Treatment Bill Brieger | 06 May 2015
Lessons Learned from a Supervisory Visit to a Medicine Shop
 In this posting Hajara Moses John of the Bauchi State Agency for the Control of HIV/AIDS, TBL and Malaria [BACATMA] shares lessons learned in supervising medicine sellers.
In this posting Hajara Moses John of the Bauchi State Agency for the Control of HIV/AIDS, TBL and Malaria [BACATMA] shares lessons learned in supervising medicine sellers.
Our team had planned supervisory visit last week to patent medicine vendors (PMVs) where shop owners have been taught the correct management of childhood illnesses. Our experience one particular shop pulled together so many lessons about training and supervision, and we are sharing this here. In the first shop we visited that day we found a boy aged 12 behind the counter. I took on the role of a mystery client, and mentioned some symptoms to the boy. “My 5-year old son is at home with catarrh. His nose is really running and his breathing is fast. What do you recommend I give him?”
The boy mentioned a local brand of antihistamine. I asked if there was anything else we should do, and the boy said that should work fine.
Next I said my two-year old daughter was also unwell. She was having fever, shivers with aches and pains. Did he have any suggestions for her? His prompt answer was “Ampiclox.”
I then asked him where the owner of the shop was. He said, “Oh my father has traveled.” I asked what class the boy was in school, to which he said the first class of junior secondary school.
Word of our visit must have spread in the area, because then a woman rushed in who it turned out to be the boy’s mother and asked how she could help us.
We explained that we were from the Ministry and were going around to help medicine shop owners improve the quality of their services. The mother happily reported that she had received training “in malaria and those other small small diseases of pickin,” from the Minsirty fo health and again from a NGO.
I went back to case of the child with a respiratory infection and pointed out the breath counting beads on the table. She said it was her husband who had done the training where the beads were explained but never taught her how to use them. We then spent some time explaining to the mother and her son about the beads and demonstrated how to use them, and also explained about management of fever.
Finally I asked the mother why she was not in the shop since her husband had traveled. She said she was in the kitchen preparing lunch for the children, and as the oldest, the 12-year old was assumed capable of running the shop. We encouraged her to discuss as a family how they could share what they have learned about managing child illness and always ensure that a competent person is available in the shop.
Training of PMVs is not a simple matter. The person trained may not always be in the shop nor share what he/she learned with other salespeople. Supervision is necessary in order to reinforce what was learned during training and provides an opportunity to teach others on-the-job. PMVs provide a large portion of the services in many African communities, and we must ensure that they can focus on quality.
Advocacy &Drug Quality &Invest in Malaria Control &IPTp &Malaria in Pregnancy &Treatment Bill Brieger | 22 Apr 2015
World Malaria Day 2015 Blog Postings Help #DefeatMalaria
 A special World Malaria Day 2015 Blog has been established. So far nine postings are available at http://www.worldmalariaday.org/blog. Please read and share with colleagues.
A special World Malaria Day 2015 Blog has been established. So far nine postings are available at http://www.worldmalariaday.org/blog. Please read and share with colleagues.
1. “Investing in integrated health services to defeat malaria”BY ELAINE ROMAN, MCSP Malaria Team Lead.
2. “Fake antimalarials: how big is the problem?”
BY DÉBORA MIRANDA, Technical Communications Officer, ACT Consortium (UK).
3. “Why antimalarial medicines matter”
BY PROFESSOR PAUL NEWTON AND ANDREA STEWART, Worldwide Antimalarial Resistance Network and Laos Oxford University Mahosot Hospital Wellcome Trust Research Unit.
4. “Malaria as an entry point for addressing other conditions”
BY HELEN COUNIHAN, Senior Public Health Specialist, Community Health Systems.
5. “Bridging the Care-Seeking Gap with ProAct”
BY MATT McLAUGHLIN, Program Manager of Peace Corps Stomping Out Malaria in Africa initiative.
 6. “Defeating Malaria in Pregnancy”
6. “Defeating Malaria in Pregnancy”
BY CATHERINE NDUNGU, ELAINE ROMAN AND AUGUSTINE NGINDU, Jhpiego.
7. “Intermittent Preventive Treatment, a Key Tool to Prevent and Control Malaria in Pregnancy”
BY CLARA MENÉNDEZ, Director of ISGlobal’s Maternal Child and Reproductive Health Initiative.
8. “Widespread artemisinin resistance could wipe out a decade of malaria investment”
BY TIM FRANCE, Asia Pacific Leaders Malaria Alliance.
9. “The long walk to a malaria-free world”
BY DAVID REDDY, CEO Medicines for Malaria Venture.
IPTp &ITNs &Monitoring &Treatment Bill Brieger | 07 Apr 2015
Highlights from Malawi’s 2014 Malaria Information Survey
Two major forms of malaria data collection help inform national malaria control programs and their supporters about progress and help focus continued resources and interventions. Routine national health information tells us about program implementation on a regular basis. National surveys give us a point-in-time picture of coverage. For the latter, Malawi has been fortunate in recent times to have conducted Malaria Information Surveys every two years.
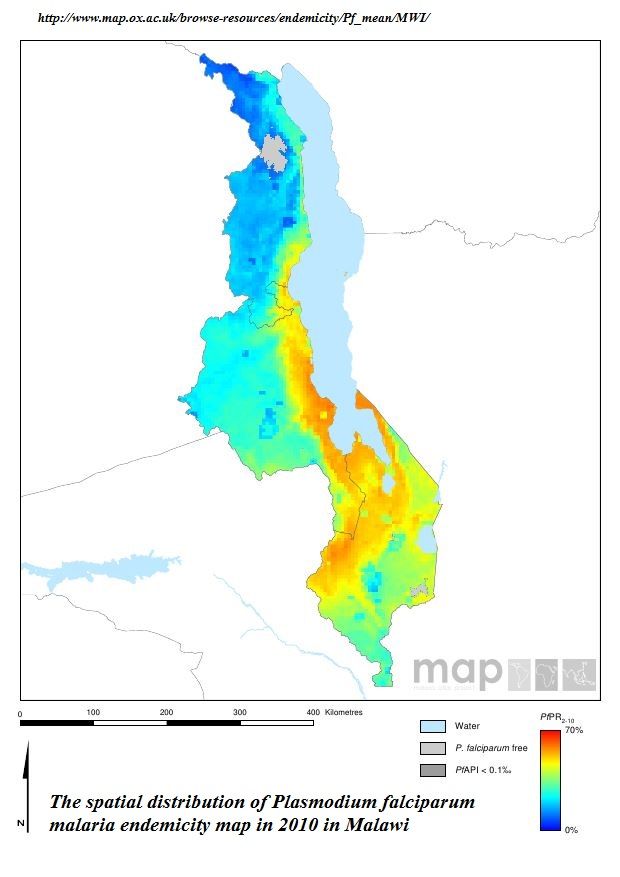 Malawi continues to have endemic malaria as documented by the MAP project in the attached graphic. While some of its neighbors in southern Africa are moving toward elimination, Malawi still experiences prevalence (as measured by rapid diagnostic test) in children below five years of age of 43%, 28% and 33% in 2010, 2012 and 2014 respectively.
Malawi continues to have endemic malaria as documented by the MAP project in the attached graphic. While some of its neighbors in southern Africa are moving toward elimination, Malawi still experiences prevalence (as measured by rapid diagnostic test) in children below five years of age of 43%, 28% and 33% in 2010, 2012 and 2014 respectively.
In the chart below we can see that malaria preventive measures have varied in coverage over the three survey periods and may be said to be on a very slightly upward trend. The Roll Back Malaria target of 80% coverage by 2010 and the US President’s Malaria Initiative target of 85% are still illusive.
In fact, simply having an ITN in the home is no guarantee that people will use it. Overall in 2014 72% of people living in a house with a net slept under one the night before the survey. The rate of use was better for children below five years of age (87%) and pregnant women (85%), but a gap remains.
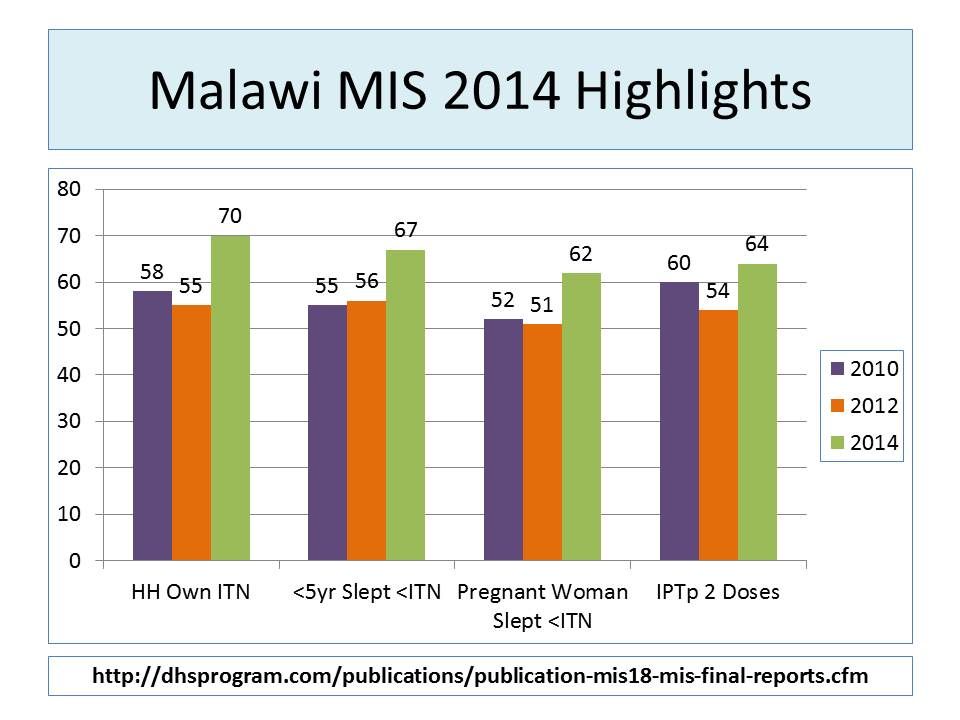 Overall coverage for two doses of sulphadoxine-pyrimethamine (SP) for intermittent preventive treatment in pregnancy (IPTp) remains low. Now that WHO is recommending IPTp with SP during each antenatal care visit after 13 weeks, we are aiming for 3, 4 or more doses. In 2014 89% pregnant women in Malawi received one dose, 63% received two and 12% received three.
Overall coverage for two doses of sulphadoxine-pyrimethamine (SP) for intermittent preventive treatment in pregnancy (IPTp) remains low. Now that WHO is recommending IPTp with SP during each antenatal care visit after 13 weeks, we are aiming for 3, 4 or more doses. In 2014 89% pregnant women in Malawi received one dose, 63% received two and 12% received three.
Malaria treatment for febrile children was the indicator with the best performance (not counting the fact that treatment was not always preceded by a diagnostic test). Most (93%) of children took an artemisinin-based combination therapy (ACT) drug, and 74% took it within a day of fever onset.
The 2014 MIS provides more detailed breakdown by region and socio-economic group, which should be helpful for planning. The major take home message though is that five years after the RBM target dates, many countries, Malawi included, have not been able to scale up and sustain the high intervention coverage needed to bring down mortality and guide us on the pathway to malaria elimination.
As the 2015 Millennium Development Goals are being replaced with a broader development agenda, we hope that malaria will not become a neglected tropical disease again. Actually using data from the MIS to take timely decisions by national programs and donors is essential to keep us on the path.
Advocacy &ITNs &Treatment Bill Brieger | 11 Mar 2015
“Zero Malaria! Count Me In!”: Senegal’s national commitment to the Last Mile to Malaria Elimination
Yacine Djibo, Founder & President of Speak Up Africa is helping focus International Women’s Day (March 8th) on efforts to protect women from malaria in Senegal. She is highlighting the commitments of 8 strong and beautiful women, in Senegal, that are dedicated to eliminating malaria in their country. These commitments are part of an inclusive mass communication campaign that aims to launch a national movement in favor of malaria elimination in Senegal: the “Zero Malaria! Count Me In” campaign
 International Women’s Day, represents an opportunity to celebrate the achievements of women all around the world. This year’s theme is “Empowering Women – Empowering Humanity: Picture it” envisions a world where each woman and girl can exercise her choices, such as participating in politics, getting an education or fighting malaria. Below is the fifth feature on women fighting malaria.
International Women’s Day, represents an opportunity to celebrate the achievements of women all around the world. This year’s theme is “Empowering Women – Empowering Humanity: Picture it” envisions a world where each woman and girl can exercise her choices, such as participating in politics, getting an education or fighting malaria. Below is the fifth feature on women fighting malaria.
Mrs. Oulèye Bèye, Head of the Prevention & Partnership Department at the National Malaria Control Program (NMCP), likes to remind us the national claim stating that “Technicians cure malaria but communities fight it”. It is a simple, yet powerful statement that summarizes the very purpose of all our endeavors. Efforts to reach remote populations and positively change communities’ behaviors are a constant battle for the NMCP.

Mrs. Oulèye Bèye, National Malaria Control Program, Senegal
The scale up of proven interventions recommended by the World Health Organization, have been essential in achieving this drastic decrease in malaria mortality rates over the years. These strategies include ensuring the availability of Artemisinin-based combination therapy (ACT) in health facilities, the mass distribution of free mosquito nets and the introduction of rapid diagnostic tests.
To be effective, all of them require significant and unconditional uptake by beneficiaries. Needless to say that the successes achieved through effective and safe malaria control campaigns, a strong national leadership and a dynamic set of partners are all at risk, if we fail to realize that populations must no longer be considered as plain beneficiaries but as stakeholders of utmost importance.
 By leading the effort around the “Zero Malaria! Count Me In” campaign at the national level, Ouleye strives to create a popular movement and actively engage each and every Senegalese citizen in the fight for a malaria-free Senegal. Sensitization and awareness raising must be the first step of any malaria elimination intervention if we want to achieve positive results in the long run.
By leading the effort around the “Zero Malaria! Count Me In” campaign at the national level, Ouleye strives to create a popular movement and actively engage each and every Senegalese citizen in the fight for a malaria-free Senegal. Sensitization and awareness raising must be the first step of any malaria elimination intervention if we want to achieve positive results in the long run.
*****
Headquartered in Dakar, Senegal, Speak Up Africa is a creative health communications and advocacy organization dedicated to catalyzing African leadership, enabling policy change, securing resources and inspiring individual action for the most pressing issue affecting Africa’s future: child health.
Community &Treatment Bill Brieger | 05 Mar 2015
Fighting Malaria with Community Case Management (CCM) Scale-Up in Kenya

Source: https://www.ifrc.org/Global/Publications/Health/Beyond_Prevention_HMM%20Malaria-EN.pdf
Access to health services is particularly difficult for the poor and those in more inaccessible areas of Kenya. This lack of endemic disease treatment for communities has proven to be quite deadly. With more than 11.3 million cases recorded annually, malaria is the leading killer of children under five years of age in Kenya. CCM, supported by organizations such as WHO and UNICEF, allows Kenya to effectively fight Malaria by using evidence-based life saving treatments that increase the availability and quality of proven interventions.
Using a CCM strategy has shown to decrease under-five malaria mortality by 60% overall under-five mortality by 40%. In Kenya particularly, the CCM pilot program has generated convincing results as seen in the graphic below.

Access to Artemisinin-based Combination Therapy (ACT) has increased and the education of communities provided by health workers has improved treatment seeking behavior. While the pilot CCM program is an important step to combating malaria, we are in the right time to take the success of this program and implement it country-wide.
Most importantly, CCM is part of the National Malaria Strategy, but it requires a more pronounced place in the plan to implement the successes of the pilot program in all 8 districts.
Action Needed: The Kenyan Ministry of Public Health and Sanitation (MoPHS) needs to commit and push ahead their own stated agenda for putting community health first by integrating malaria treatment into the already implemented diarrhea CCM program by the end of 2015.
Graphic: https://www.ifrc.org/Global/Publications/Health/Beyond_Prevention_HMM%20Malaria-EN.pdf
Advocacy &Costs &Equity &Funding &Treatment &Universal Coverage Bill Brieger | 13 Dec 2014
Malaria Care: Can We Achieve Universal Coverage?
![]() In New York on 12 December 2014, a new global coalition of more than 500 leading health and development organizations worldwide was launched to advocate for universal coverage (UC) and urged “governments to accelerate reforms that ensure everyone, everywhere, can access quality health services without being forced into poverty.” This marked Universal Health Coverage Day which fell on the “two-year anniversary of a United Nations resolution … which endorsed universal health coverage as a pillar of sustainable development and global security.”
In New York on 12 December 2014, a new global coalition of more than 500 leading health and development organizations worldwide was launched to advocate for universal coverage (UC) and urged “governments to accelerate reforms that ensure everyone, everywhere, can access quality health services without being forced into poverty.” This marked Universal Health Coverage Day which fell on the “two-year anniversary of a United Nations resolution … which endorsed universal health coverage as a pillar of sustainable development and global security.”
According to WHO delivery of UC involves four components:
- A strong, efficient, well-run health system
- Affordable care
- Accessible care
- A health workforce with sufficient capacity to meet patient needs
To this list we might add a functioning and timely procurement and supply management system, and not trust people to read between the lines on component #1 to consider this need.
 While much attention in malaria control is appropriately on prevention through various vector control measures, we cannot forget the importance of prompt and appropriate case management, especially as cases decline (according to the new 2014 World Malaria Report) and case detection assumes greater importance.
While much attention in malaria control is appropriately on prevention through various vector control measures, we cannot forget the importance of prompt and appropriate case management, especially as cases decline (according to the new 2014 World Malaria Report) and case detection assumes greater importance.
In 2000 Roll Back Malaria sponsored the Abuja Summit where targets were set for malaria intervention coverage. The goals were established at 80% for insecticide-treated nets (ITNs), intermittent preventive treatment and prompt and appropriate malaria treatment. In 2009, the United Nations declared a goal of universal coverage for ITNs. The potential for UC in malaria case management remained vague, but the new international push for US can certainly include malaria. It would not be coming too late because as we can see from the chart, many endemic countries are far from adequate malaria treatment coverage, let alone UC.
 Frequent surveys help us track progress toward RBM goals and UC – Demographic and Health Survey, Malaria Information Survey, Multi Indicator Cluster Survey. Their helpfulness depends on the questions asked. The 2013 MIS from Rwanda gets closest to finding out what is really happening (Chart 2). We might infer a sequence of events that while not everyone seeks care for their febrile child, those who do are screened by the health worker (including volunteer community health workers); those suspected of malaria are tested (microscopy in clinics, RDTs in communities); and only those found positive are given ACTs.
Frequent surveys help us track progress toward RBM goals and UC – Demographic and Health Survey, Malaria Information Survey, Multi Indicator Cluster Survey. Their helpfulness depends on the questions asked. The 2013 MIS from Rwanda gets closest to finding out what is really happening (Chart 2). We might infer a sequence of events that while not everyone seeks care for their febrile child, those who do are screened by the health worker (including volunteer community health workers); those suspected of malaria are tested (microscopy in clinics, RDTs in communities); and only those found positive are given ACTs.
 Equity is a major concern for advocates of UC. Health insurance is one method to address this. In Ghana around 60% of people have taken part in the National Health Insurance Scheme, but only around 5% in Nigeria where 60% of health expenditure comes from out-of-pocket purchases. Rwanda has a system of mutuelles – community insurance schemes. Insurance does not meet the full need for malaria case management, and thus efforts to expand outlets for affordable quality malaria medicines through the Affordable Medicines Facility malaria (AMFm) was piloted in several countries.
Equity is a major concern for advocates of UC. Health insurance is one method to address this. In Ghana around 60% of people have taken part in the National Health Insurance Scheme, but only around 5% in Nigeria where 60% of health expenditure comes from out-of-pocket purchases. Rwanda has a system of mutuelles – community insurance schemes. Insurance does not meet the full need for malaria case management, and thus efforts to expand outlets for affordable quality malaria medicines through the Affordable Medicines Facility malaria (AMFm) was piloted in several countries.
A combination of approaches is needed to achieve UC in malaria case management. Public and private sources are requires. Low cost, subsidized and free care must to be part of the mix. Over half a million people, mostly children, are still dying from malaria annually. Solving the UC challenge for malaria is crucial.
Health Systems &HIV &Malaria in Pregnancy &Treatment Bill Brieger | 02 Dec 2014
Update on Malaria and HIV/AIDS
 World AIDS Day is a time to reflect on the broader impact of HIV and its interactions with other infectious and chronic conditions that must be managed through an integrated health system. The past few months have yielded a variety of published studies on the HIV-Malaria link ranging from pharmacological, and physiological to health systems issues. A brief summary follows.
World AIDS Day is a time to reflect on the broader impact of HIV and its interactions with other infectious and chronic conditions that must be managed through an integrated health system. The past few months have yielded a variety of published studies on the HIV-Malaria link ranging from pharmacological, and physiological to health systems issues. A brief summary follows.
Having HIV does have consequences on malaria infection. Serghides et al. studied malaria-specific immune responses are altered in HIV/malaria co-infected individuals. Fortunately these researchers learned about “the importance of HIV treatment and immune re-constitution in the context of co-infection.”
Malaria, HIV and Pregnancy
Pregnant women are an important group in the population to protect from both HIV and malaria. The link between the diseases may not be one of influencing each other but in the fact that they both appear in the same population with similar negative consequences. Women are at increased risk of anemia in pregnancy due to malaria and/or HIV infection according to Ononge and co-workers. Normally a pregnant woman in a malaria endemic area passes on malaria antibodies to their newborns.
Moro et al. learned that, “Placental transfer of antimalarial antibodies is reduced in pregnant women with malaria and HIV infection.” Chihana and colleagues studied HIV status in Malawian pregnant women and follow-up their children. They reported that, “Maternal HIV status had little effect on neonatal mortality but was associated with much higher mortality in the post-neonatal period and among older children.”
Drug Interactions and Issues
Hoglund and colleagues studied interactions between common antimalarial and HIV medications. They found that, “There are substantial drug interactions between artemether-lumefantrine and efavirenz, nevirapine and ritonavir/lopinavir. Given the readily saturable absorption of lumefantrine, the dose adjustments predicted to be necessary will need to be evaluated prospectively in malaria-HIV coinfected patients.”
 Drugs taken during pregnancy to prevent malaria are influenced by HIV status. It is known that Intermittent Preventive Treatment with sulfadoxine-pyrimethamine should not be administered to HIV-positive pregnant women taking cotrimoxazole prophylaxis. González et al. wanted to learn whether mefloquine (MQ) could be used by HIV+ pregnant women. Unfortunately they learned that, “MQ was not well tolerated, limiting its potential for IPTp … (and) … MQ was associated with an increased risk of mother to child transmission of HIV.”
Drugs taken during pregnancy to prevent malaria are influenced by HIV status. It is known that Intermittent Preventive Treatment with sulfadoxine-pyrimethamine should not be administered to HIV-positive pregnant women taking cotrimoxazole prophylaxis. González et al. wanted to learn whether mefloquine (MQ) could be used by HIV+ pregnant women. Unfortunately they learned that, “MQ was not well tolerated, limiting its potential for IPTp … (and) … MQ was associated with an increased risk of mother to child transmission of HIV.”
Health Systems Issues
Haji and co-investigators reported that malaria care seeking was delayed in Ethiopia because “Children whose guardians believed that covert testing for HIV was routine clinical practice presented later for investigation of suspected malaria.”
The need to adjust clinical guidance and practice as prevalence of malaria changes was addressed by Mahende et al. in Tanzania. They observed that, “Although the burden of malaria in many parts of Tanzania has declined, the proportion of children with fever has not changed.” More accurate diagnosis is needed as demonstrated by the various causes of febrile illness they found including in addition to malaria, respiratory illnesses, blood infections, urine infections, gastrointestinal illness and even HIV.
Finally Mbeye and colleagues report that cotrimoxazole prophylactic treatment reduces incidence of malaria and mortality in children in sub-Saharan Africa and appears to be beneficial for HIV-infected and HIV-exposed as well as HIV-uninfected children. This lesson from HIV programming can have broader implications for malaria control strategies.
Integrated control of infectious diseases is essential for population health, especially at the primary care level. Hopefully research as shown above can assist in planning better services for people living in areas that are endemic to both malaria and HIV.
Treatment Bill Brieger | 19 Nov 2014
Understanding Child Illness and Malaria Care Seeking in Bauchi State Nigeria
Bright Orji, Masduk Abdulkarim, William Sambisa, Amos Paul Bassi, Solomon Thliza, and William Brieger shares a poster at the 2014 American Public Health Association Annual Meeting that focuses on a baseline study for child illness interventions under the USAID Targeted States High Impact Project (TSHIP). The authors work with John Snow International and Jhpiego. The poster abstract follows:
 Seeking of appropriate and quality care for childhood illnesses is a major challenge in much of Africa including Bauchi State, Nigeria. In advance of an intervention to improve available care in the most common points of service (POS), government primary health care centers (PHCs) and patent medicine vendors (PMV), a survey was done of child caregivers in four districts concerning responses to febrile illness, suspected malaria, acute respiratory disease and diarrhea.
Seeking of appropriate and quality care for childhood illnesses is a major challenge in much of Africa including Bauchi State, Nigeria. In advance of an intervention to improve available care in the most common points of service (POS), government primary health care centers (PHCs) and patent medicine vendors (PMV), a survey was done of child caregivers in four districts concerning responses to febrile illness, suspected malaria, acute respiratory disease and diarrhea.
The ethical review committee in the Bauchi State Ministry of Health approved of the study. A total of 3077 children below the age of five were identified in the households sampled.
 Their mothers, fathers or other caregivers consented and were interviewed. Among the children 74% had any Illness, 57% had fever, 26% had cough, and 15% had diarrhoea. Only 8.7% of 1186 febrile children had their blood tested. Care seeking from PMVs varied from 45% with fever, 40% with cough to 36% with diarrhoea.
Their mothers, fathers or other caregivers consented and were interviewed. Among the children 74% had any Illness, 57% had fever, 26% had cough, and 15% had diarrhoea. Only 8.7% of 1186 febrile children had their blood tested. Care seeking from PMVs varied from 45% with fever, 40% with cough to 36% with diarrhoea.
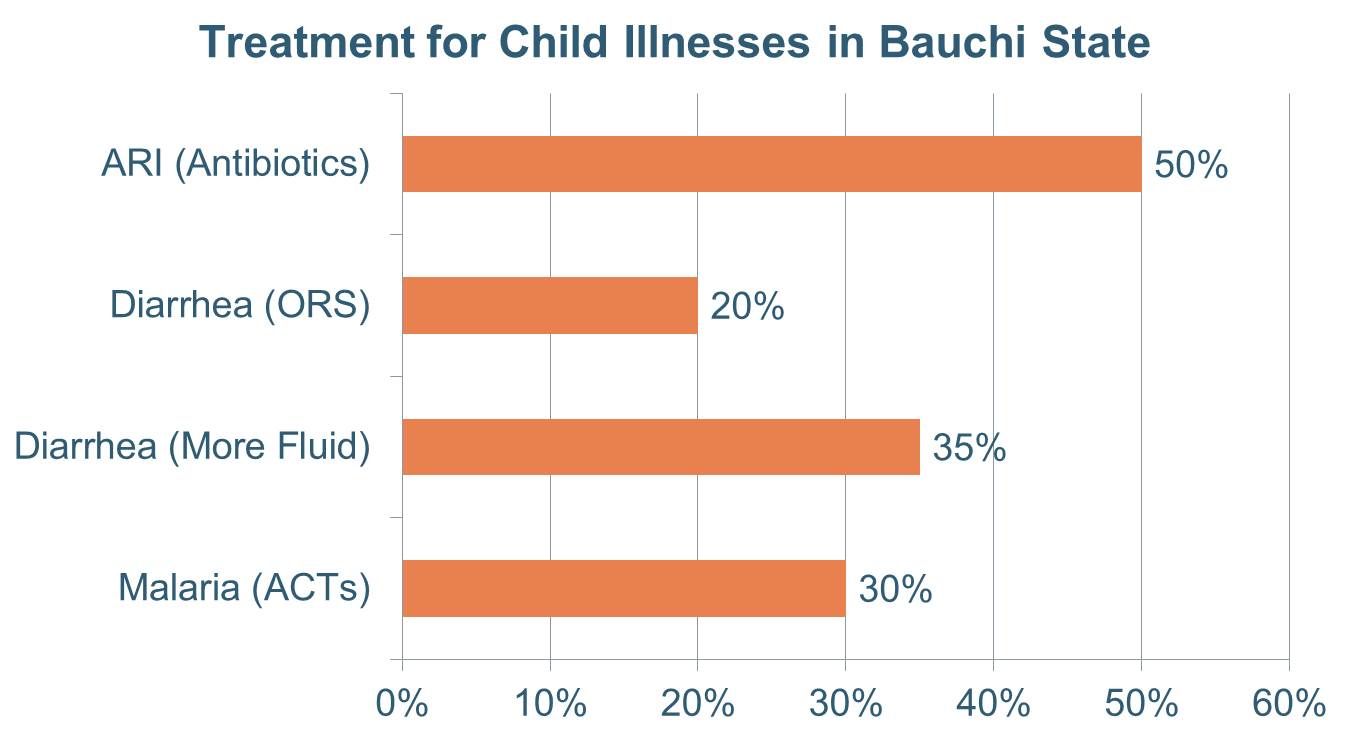
 Care from public sector POS varied from 26-33%. Treatment that might be considered ‘appropriate’ for each also varied with 30% receiving antimalarial drugs for suspected malaria, 20% getting oral rehydration solution for diarrhoea and 50% being given an antibiotic for a suspected acute respiratory illness.
Care from public sector POS varied from 26-33%. Treatment that might be considered ‘appropriate’ for each also varied with 30% receiving antimalarial drugs for suspected malaria, 20% getting oral rehydration solution for diarrhoea and 50% being given an antibiotic for a suspected acute respiratory illness.
The results show that providing quality case management with appropriate commodities through PHCs and PMVs can improve the illness care of a majority of children in Bauchi State, and interventions are currently being planned to do this.
Severe Malaria &Treatment Bill Brieger | 07 Nov 2014
Severe malaria case management practices in selected states in Nigeria: Need for urgent intervention
At the recently concluded American Society of Tropical Medicine and Hygiene 2014 Annual Meeting, USAID’s MAPS Project presented a poster on severe malaria in Nigeria. The authors, Yetunde Oke, Banji Ipadeola, Bolatito Aiyenigba, Grace Nwankwo, Justice Adaji, Olatunde Olotu, Aniefiok Akpasa, and Abba Umar, share their findings below.
![]() Severe malaria is a life threatening medical condition that requires emergency interventions including prompt and effective treatment to prevent death (WHO 2000). The AQUAMAT* study showed a relative reduction in mortality of 22.5% with use of parenteral artesunate compared to quinine in the management of severe P. falciparum malaria and the Nigeria national policy on malaria diagnosis and treatment has been revised based on this evidence.
Severe malaria is a life threatening medical condition that requires emergency interventions including prompt and effective treatment to prevent death (WHO 2000). The AQUAMAT* study showed a relative reduction in mortality of 22.5% with use of parenteral artesunate compared to quinine in the management of severe P. falciparum malaria and the Nigeria national policy on malaria diagnosis and treatment has been revised based on this evidence.
However, implementation of this guideline is still a challenge. The goal of this study was to determine baseline capacity and management practices for severe malaria in selected secondary health facilities in Nigeria with the aim of designing interventions to address specific gaps identified.
A cross?sectional study was conducted to assess twenty?four secondary public health facilities in three states (Benue, Kogi and Oyo States) in Nigeria in August 2013. Data on the capacity of health care providers; malaria services provided at different service delivery points (three months preceding the survey).
Medical supplies were collected using modified WHO severe malaria assessment tools. Data entry was done using the SPSS software programme and analysis done with STATA version 10.0.
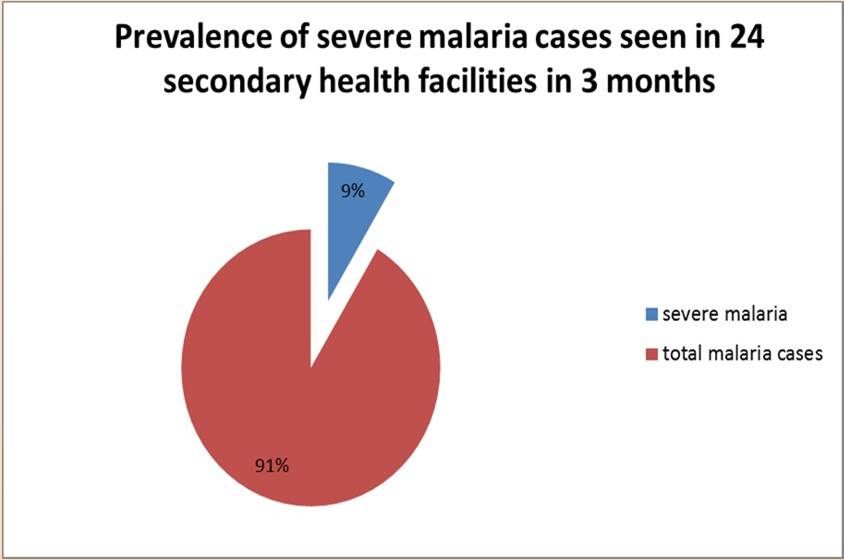 Total number of confirmed malaria cases reported in the three states over the three months preceding the assessment was 18, 695 and diagnosis of severe malaria was made in 8.6% of the total malaria cases. Out of the severe malaria cases, 75.9% were discharged, 3.8% referred and 1.5% died.
Total number of confirmed malaria cases reported in the three states over the three months preceding the assessment was 18, 695 and diagnosis of severe malaria was made in 8.6% of the total malaria cases. Out of the severe malaria cases, 75.9% were discharged, 3.8% referred and 1.5% died.
Fifty per cent of the health care providers had attended training on malaria case management 12 months preceding the survey. The majority of providers managed severe malaria with injectable artemether (45.8%), quinine (37.5%) compared with artesunate (29.2%).
 Most of the health facilities (95.8%) practiced parasite-based diagnosis of malaria but only (29.2%) monitored the parasite clearance of patients with severe malaria. 70% of the facilities did not have basic supplies for ancillary management of severe malaria. 66.7% and 30% of the health facilities experienced stock?out of parenteral artesunate and parenteral quinine respectively in the previous three months.
Most of the health facilities (95.8%) practiced parasite-based diagnosis of malaria but only (29.2%) monitored the parasite clearance of patients with severe malaria. 70% of the facilities did not have basic supplies for ancillary management of severe malaria. 66.7% and 30% of the health facilities experienced stock?out of parenteral artesunate and parenteral quinine respectively in the previous three months.
Health system strengthening with emphasis on capacity building of health care providers, medical commodity security and improvement in supportive/ancillary management of severe malaria is needed to reduce the mortality attributable to severe malaria.