Diagnosis &Essential Medicines &IPTi &Malaria in Pregnancy &Seasonal Malaria Chemoprevention &Treatment &Zero Malaria Bill Brieger | 25 Apr 2019 09:00 am
Zero Malaria Starts with Universal Coverage: Part 2 Preventive and Curative Treatments
April hosts several important global health days or observances. On World Health Day 2019 WHO stressed that, “Universal health coverage (UHC) is WHO’s number one goal. Key to achieving it is ensuring that everyone can obtain the care they need, when they need it, right in the heart of the community.” Nationwide monitoring through the Demographic and Health Surveys (DHS), the Malaria Indicator Surveys (MIS) and the Multi-Indicator Cluster Surveys (MICS) can document the status of appropriate malaria treatment and intermittent preventive treatment in pregnant women (IPTp).
 Definitions of indicators have evolved for treatment-related malaria interventions. When Intermittent Preventive Treatment for pregnant women (IPTp) began in the early 2000s, the recommended dosing was twice during pregnancy after the first trimester one month apart in high and/or stable transmission areas. Due to lessening efficacy of sulfadoxine-pyrimethamine (SP), the dosage recommendation has changed to at least three times, still a month apart from the beginning of the second trimester.
Definitions of indicators have evolved for treatment-related malaria interventions. When Intermittent Preventive Treatment for pregnant women (IPTp) began in the early 2000s, the recommended dosing was twice during pregnancy after the first trimester one month apart in high and/or stable transmission areas. Due to lessening efficacy of sulfadoxine-pyrimethamine (SP), the dosage recommendation has changed to at least three times, still a month apart from the beginning of the second trimester.
This updated policy was broadcast widely between 2012 and 2013, but it took countries some time to build capacity and scale up for the expanded coverage goals. UNICEF Data5 again show that between 2014 and 2017 coverage was far below either 80% of pregnant women, let alone reaching them universally (Figure 2). Most countries achieved 30% or less coverage. Zambia at 50% was the highest. Low coverage leaves both pregnant women and the unborn child at risk for anemia and death in the former and low birth weight, still birth or miscarriage for the latter. The World Malaria Report of 2018 estimates that three doses of IPTp were received by only 22% of pregnant women in the target countries in 2017.
The concept of IPT was investigated for infants and children during by a consortium of researchers in several African Countries. It was found that IPTi with SP could have a positive effect on preventing malaria. To operationalize this concept, the World Health Organization developed what is known as Seasonal Malaria Chemoprevention (SMC) that would be delivered in the Sahel region of West Africa where malaria transmission itself is seasonal and where there are some countries with very low transmission with implications for malaria elimination.
 The SMC delivery process was not linked to immunization but provided by community health workers and volunteers. SP and Amodiaquine (SP-AQ) were used in combination and provided monthly, three or four times during the rainy/high transmission season. Coverage was targeted at children below school age. It is only recently that SMC has been scaled up to reach all eligible countries or states and regions within designated countries.
The SMC delivery process was not linked to immunization but provided by community health workers and volunteers. SP and Amodiaquine (SP-AQ) were used in combination and provided monthly, three or four times during the rainy/high transmission season. Coverage was targeted at children below school age. It is only recently that SMC has been scaled up to reach all eligible countries or states and regions within designated countries.
WHO states that SMC focuses on, “children aged 3–59 months (and) reduces the incidence of clinical attacks and severe malaria by about 75%.” In some countries the coverage is extended to primary school aged children, making comparisons and calculations of coverage (universal por otherwise) challenging.
 The World Malaria Report of 2018 notes that, “In 2017, 15.7 million children in 12 countries in Africa’s Sahel subregion were protected through seasonal malaria chemoprevention (SMC) programs. However, about 13.6 million children who could have benefited from this intervention were not covered, mainly due to a lack of funding.” This implies that 54% of eligible children were reached. Coverage of SMC can refer to receiving any of the doses or as having received all the monthly doses offered by a nation’s malaria control program. Specifically, the World Malaria Report 2018 drew on surveys in 7 countries that provided 4 monthly doses to determine that 53% of children received all doses.
The World Malaria Report of 2018 notes that, “In 2017, 15.7 million children in 12 countries in Africa’s Sahel subregion were protected through seasonal malaria chemoprevention (SMC) programs. However, about 13.6 million children who could have benefited from this intervention were not covered, mainly due to a lack of funding.” This implies that 54% of eligible children were reached. Coverage of SMC can refer to receiving any of the doses or as having received all the monthly doses offered by a nation’s malaria control program. Specifically, the World Malaria Report 2018 drew on surveys in 7 countries that provided 4 monthly doses to determine that 53% of children received all doses.
 Determining coverage for malaria treatment for sick people is not as straightforward as finding out the numbers who slept under an ITN or swallowed IPTp doses, and even those are not simple. As defined, correct treatment first consists of parasitological diagnosis, which at the primary care level could be by microscopy or rapid diagnostic test (RDT). The next issue is treating only those with positive tests. Finally, the treatment must consist of age- or weight-specific doses of an approved artemisinin-based combination therapy (ACT) drug. Very few clinic records or surveys document whether the treatment given is ‘correct’ by these standards.
Determining coverage for malaria treatment for sick people is not as straightforward as finding out the numbers who slept under an ITN or swallowed IPTp doses, and even those are not simple. As defined, correct treatment first consists of parasitological diagnosis, which at the primary care level could be by microscopy or rapid diagnostic test (RDT). The next issue is treating only those with positive tests. Finally, the treatment must consist of age- or weight-specific doses of an approved artemisinin-based combination therapy (ACT) drug. Very few clinic records or surveys document whether the treatment given is ‘correct’ by these standards.
WHO addresses the need for achieving universal access to malaria diagnostic testing and notes this will not be easy. They provide a successful example of Senegal, where following the introduction of malaria RDTs in 2007, malaria diagnostic testing rates rose rapidly from 4% to 86% (by 2009). Logistics, funding, training and supportive supervision complicate implementation.
UNICEF Data report that performance of malaria diagnostics in febrile children in surveys 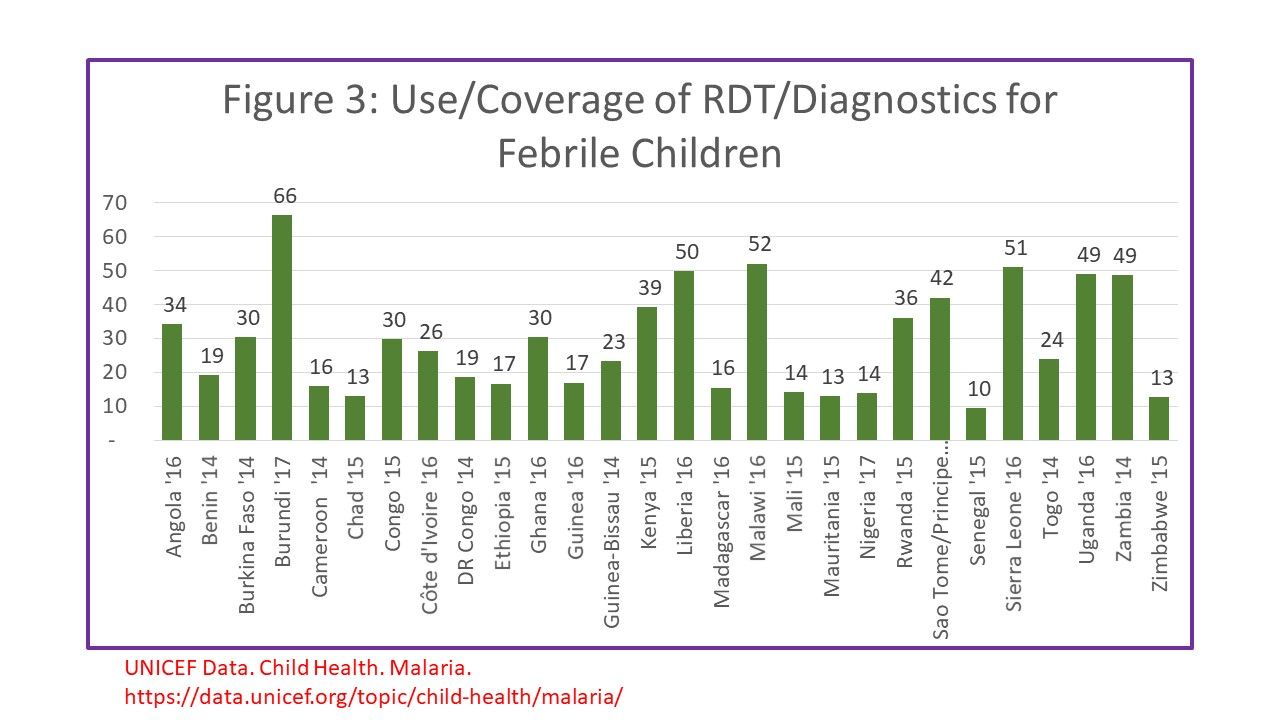 between 2014-17 was approximately 30% on average for countries with national surveys within that time frame (Figure 3). Only 4 countries achieved 50% or better. Most surveys then go on to report the number of febrile children who received ACTs, but do not necessary indicate how many who were correctly diagnoses were given ACTs vs those who received ACT but did not receive a test or tested negative.
between 2014-17 was approximately 30% on average for countries with national surveys within that time frame (Figure 3). Only 4 countries achieved 50% or better. Most surveys then go on to report the number of febrile children who received ACTs, but do not necessary indicate how many who were correctly diagnoses were given ACTs vs those who received ACT but did not receive a test or tested negative.
The Nigeria 2015 Malaria Indicator Survey Illustrates this dilemma. Among 2600 children who reported having a fever in the two weeks preceding the survey, 66.1% sought advice (or care). Overall, 12.6% of febrile children received a diagnostic test as defined in the question as to whether the child was stuck on the finger or heel to obtain blood. Among the febrile children 37.6% reportedly were given some type of antimalarial drug. Overall 15.5% of febrile children were given an ACT. Even if ACTs were given only to tested children, not all tests would have been positive.
The overall implication of measuring treatment without a link to testing is that if more children receive any, let alone the correct drugs, is that evidence for actual presence of disease. We have a long way to go to measure malaria treatment coverage correctly, not to mention achieving universal coverage with appropriate treatment. Different malaria treatment-related interventions with different steps and different target groups in different regions of Africa and the World make defining, no less achieving UHC, a huge challenge.
on 26 Apr 2019 at 12:55 pm 1.Zero Malaria Starts with Universal Coverage: Part 2 Preventive and Curative Treatments said …
[…] Go here to see the original: Zero Malaria Starts with Universal Coverage: Part 2 Preventive and Curative Treatments […]