Health Workers &Human Resources &IPTp &Training &Treatment Bill Brieger | 07 Nov 2017
Using rapid task analysis to strengthen Pre-Service Education (PSE) learning and performance of critical malaria interventions in Liberia
 Understanding the tasks that health workers perform in real life can improve their basic Training. Marion Subah of MCSP and Jhpiego shares experiences in using Task Analysis to improve pre-service training of midwives and lab technicians in Liberia. Her findings summarized below, are presented at the American Society of Tropical Medicine’s 66th Annual Meeting.
Understanding the tasks that health workers perform in real life can improve their basic Training. Marion Subah of MCSP and Jhpiego shares experiences in using Task Analysis to improve pre-service training of midwives and lab technicians in Liberia. Her findings summarized below, are presented at the American Society of Tropical Medicine’s 66th Annual Meeting.
Health worker task analysis helps human resource planners and managers update pre-service education (PSE) curricula and plan needed in- service training. In Liberia, a task analysis was conducted focusing on Liberia’s midwives’ and Medical Laboratory Technicians’ (MLT) work practices.
service training. In Liberia, a task analysis was conducted focusing on Liberia’s midwives’ and Medical Laboratory Technicians’ (MLT) work practices.
Task lists were developed using curricula, job descriptions and professional scope of practice, and validated by key stakeholders for each cadre. Responses from 25 MLTs and 26 midwives were examined that addressed the following questions:
- How often do you do the task (frequency)?
- Where did you learn to do the task (location)?
- How well do you think you are able to perform the task (performance)?
- How critical is the task in terms of patient and/or public health outcomes (criticality).
 Eligibility criteria included those currently practicing between 6 months and 5.5 years following graduation. Midwives were assessed for five tasks relating to malaria service provision, including provision of preventive treatment for malaria in pregnancy, management of vector borne diseases, diagnosis and management uncomplicated malaria in adults and children (respectively), and provision of malaria preventive services.
Eligibility criteria included those currently practicing between 6 months and 5.5 years following graduation. Midwives were assessed for five tasks relating to malaria service provision, including provision of preventive treatment for malaria in pregnancy, management of vector borne diseases, diagnosis and management uncomplicated malaria in adults and children (respectively), and provision of malaria preventive services.
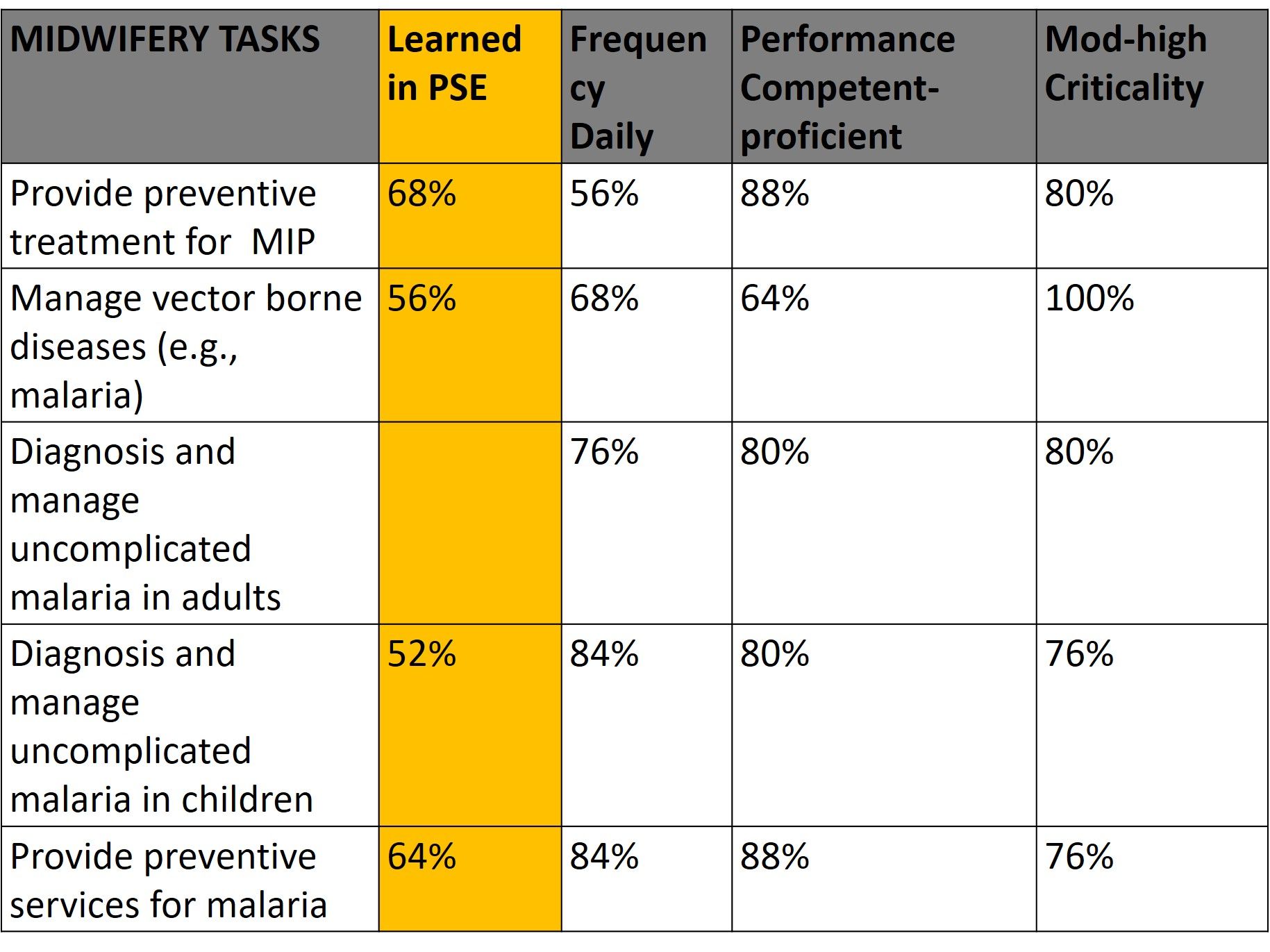 Lab technicians were assessed for one malaria task, performance of parasitological tests. On average 61% of midwives learned these malaria tasks in PSE, 74% said they performed these tasks daily, 80% felt proficient in performing the tasks, and 82% rated the tasks moderate to high in criticality. For MLTs, 88% learned malaria testing in pre-service education, 100 % performed this task daily, 77% felt they were proficient and 93% said the task was of moderate to high criticality.
Lab technicians were assessed for one malaria task, performance of parasitological tests. On average 61% of midwives learned these malaria tasks in PSE, 74% said they performed these tasks daily, 80% felt proficient in performing the tasks, and 82% rated the tasks moderate to high in criticality. For MLTs, 88% learned malaria testing in pre-service education, 100 % performed this task daily, 77% felt they were proficient and 93% said the task was of moderate to high criticality.
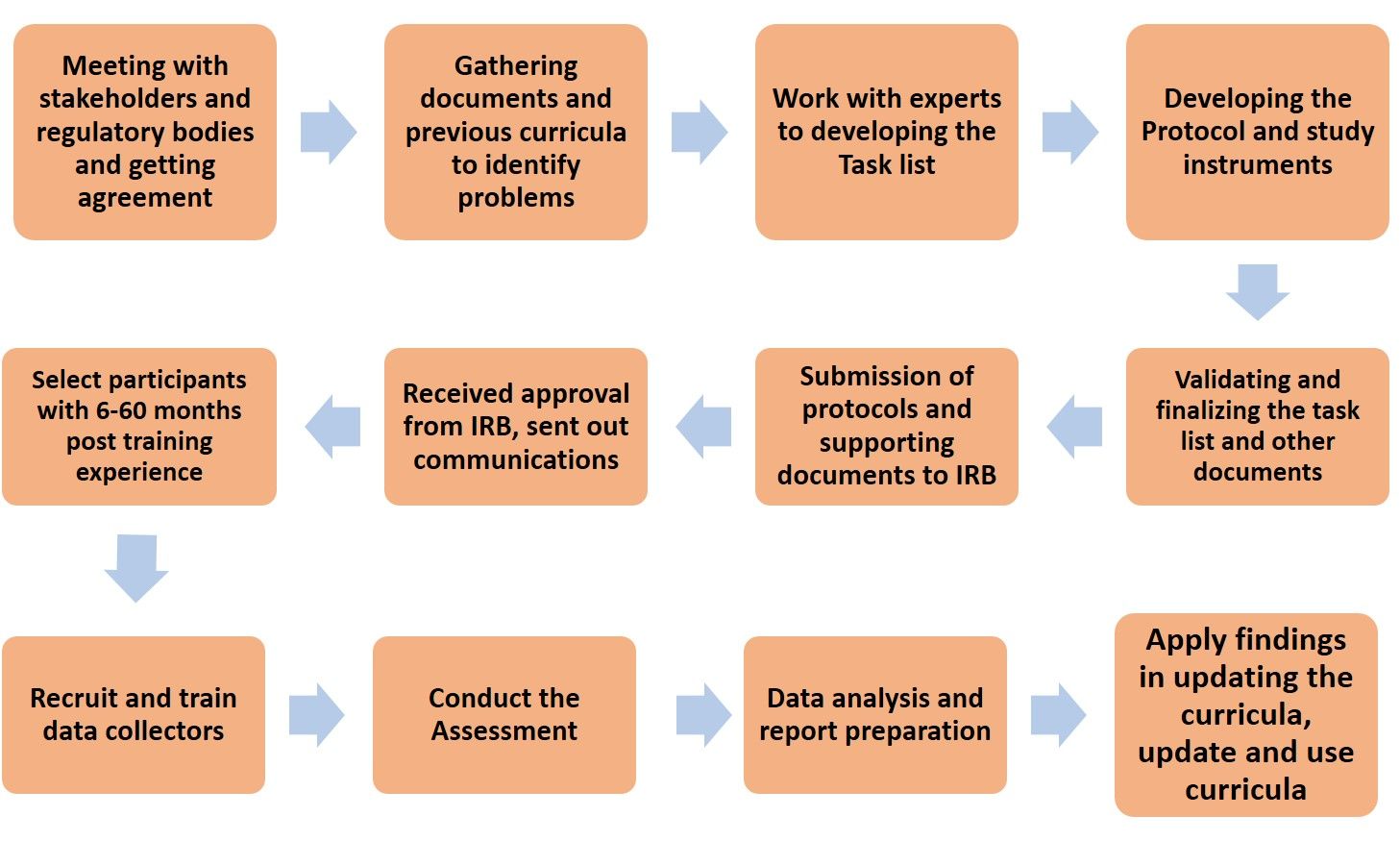
Task Analysis Flow Chart
The results from this rapid task analysis are being applied to the current curricula review. Courses that could be updated or strengthened have been identified. Malaria Case Management Technical Update and Effective Teaching Skills Training are being organized for tutors at the training schools. Finally, integrated supportive supervision tools are being strengthened to improve performance of these malaria tasks by midwives and lab technicians.
IPTp &ITNs &Malaria in Pregnancy &Treatment Bill Brieger | 10 Jul 2017
Liberia’s Fight against Malaria Continues
Liberia was making steady progress against malaria in the years after the civil war. Despite the devastation of Ebola, the health authorities have continued to push against malaria. The DHS Program has released key findings from the 2016 Malaria Information Survey. We have compared those against the 2011 MIS, and while there is progress, much work needs to be done in this highly endemic area – not just in fighting malaria, but in rebuilding health systems damaged by war and Ebola.
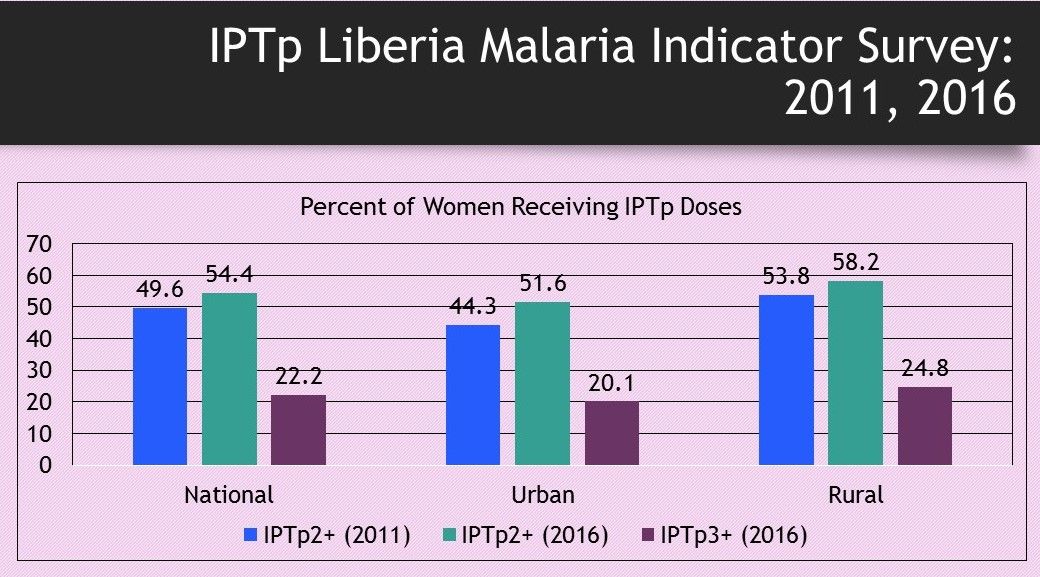 Targets for Intermittent Preventive Treatment in pregnancy of malaria have risen from at least 2 doses in 2011 to three or more when the 2016 data were collected. While the IPTp2+ doses have increased by a little less than 5%, the challenge of IPTp3 and greater has become quite evident. It is interesting that coverage of IPTp is slightly better in rural areas, but there is still a long way to go to protect pregnant Liberian women.
Targets for Intermittent Preventive Treatment in pregnancy of malaria have risen from at least 2 doses in 2011 to three or more when the 2016 data were collected. While the IPTp2+ doses have increased by a little less than 5%, the challenge of IPTp3 and greater has become quite evident. It is interesting that coverage of IPTp is slightly better in rural areas, but there is still a long way to go to protect pregnant Liberian women.
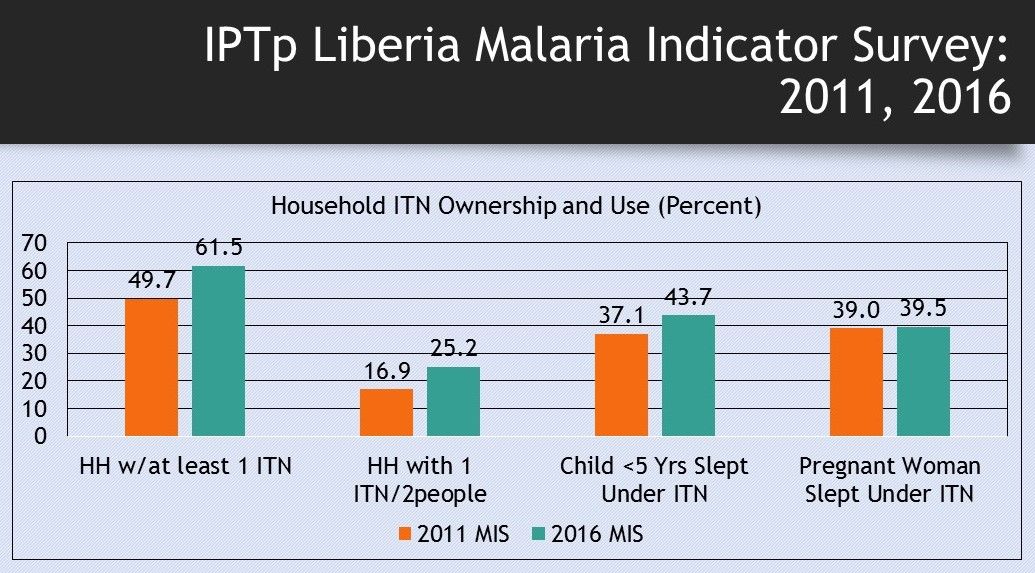 The situation with access to and use of insecticide treated nets has also improved over the 5-year period, but still remains well below the targets of universal coverage. Even though nearly two-thirds of households have at least one ITN, only a quarter have enough nets to reach the goal of one net for every two people. Net use by children below the age of 5 years is better than that of pregnant women, though in both cases less that half of these vulnerable populations are covered. Nets are particularly important for pregnant women who cannot take IPTp in the first trimester.
The situation with access to and use of insecticide treated nets has also improved over the 5-year period, but still remains well below the targets of universal coverage. Even though nearly two-thirds of households have at least one ITN, only a quarter have enough nets to reach the goal of one net for every two people. Net use by children below the age of 5 years is better than that of pregnant women, though in both cases less that half of these vulnerable populations are covered. Nets are particularly important for pregnant women who cannot take IPTp in the first trimester.
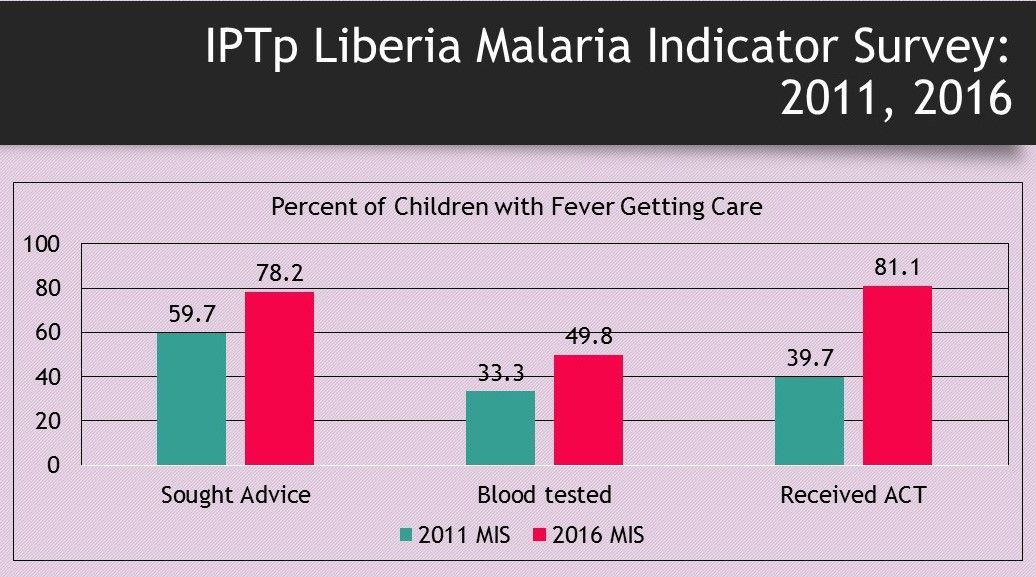 Care for febrile children also has improved, but questions remain about appropriate care due to the nature of the questioning processes in the MIS. Seeking advice increased by 20% as did getting blood tests (RDT or microscopy) once care is sought. Double the number of febrile children received artemisinin-based combination therapy in 2016 compared to 2011, but since the rate of testing is low, we do not know if they were being appropriately treated – given ACT only is tests were positive.
Care for febrile children also has improved, but questions remain about appropriate care due to the nature of the questioning processes in the MIS. Seeking advice increased by 20% as did getting blood tests (RDT or microscopy) once care is sought. Double the number of febrile children received artemisinin-based combination therapy in 2016 compared to 2011, but since the rate of testing is low, we do not know if they were being appropriately treated – given ACT only is tests were positive.
Liberia does receive support from donors such as the Global Fund and the US President’s Malaria Initiative. These and other partners need to strategize with the Liberian Ministry of Health and other local partners (NGOs, Businesses, etc.) in order to mobilize the support to put Liberia more squarely on the road to malaria elimination.
Epidemiology &IPTp &ITNs &Malaria in Pregnancy &Morbidity &Treatment Bill Brieger | 26 Jun 2017
Burundi: when will citizens see real protection from malaria?
Preliminary findings from Burundi’s 2015-16 DHS have been made available. The country has a long way to go to meet targets for basic control of malaria.
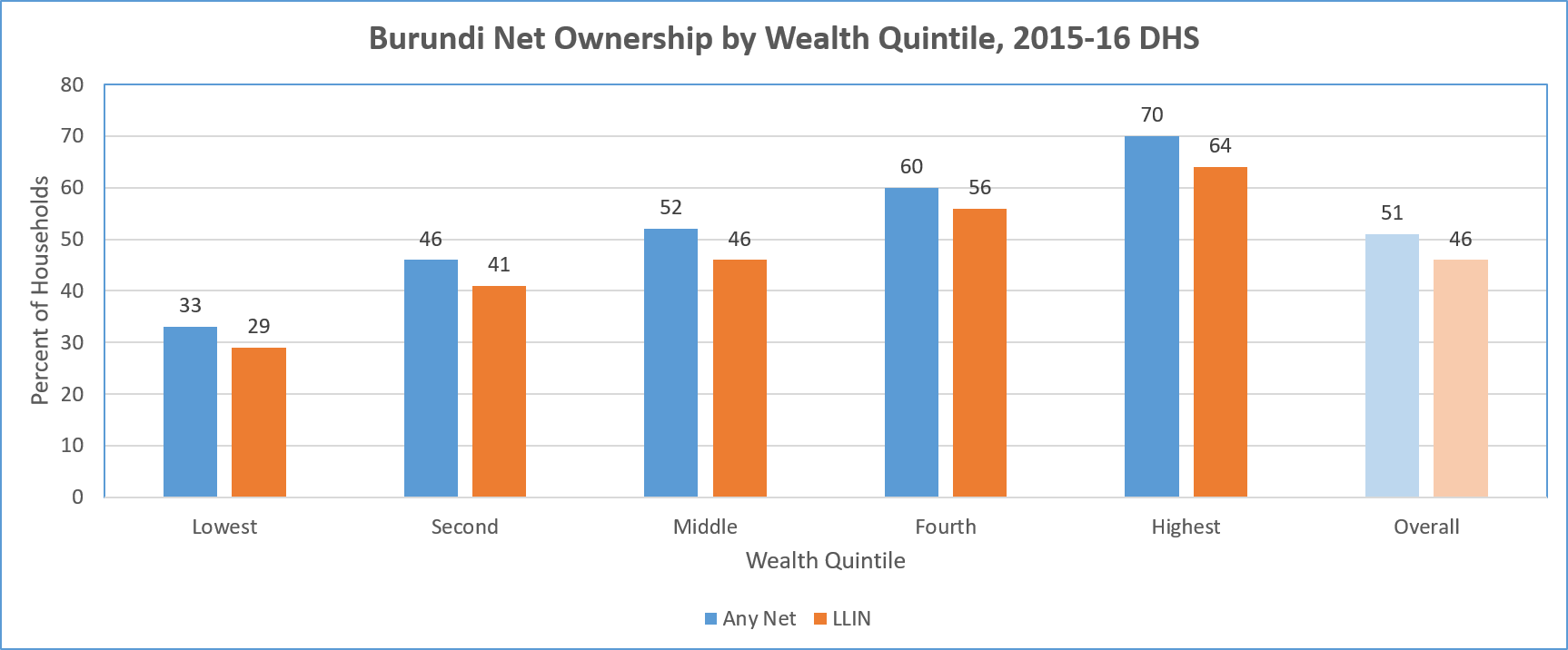 LLIN availability by household is an overall disappointing 32%. Ironically there is greater coverage of households in in urban areas (50%) than rural (30%). There is also great variation among the provinces with 52% coverage in Bujumbura metropolitan but only 19% in Canzuko. The overall average is less than one treated net per household.
LLIN availability by household is an overall disappointing 32%. Ironically there is greater coverage of households in in urban areas (50%) than rural (30%). There is also great variation among the provinces with 52% coverage in Bujumbura metropolitan but only 19% in Canzuko. The overall average is less than one treated net per household.
A major concern is equity. The chart above shows a steep gradation from 19% coverage among the lowest fifth of the wealth quintile, up to 48% in the highest. Even in households that have at least one net, only 17% of of people slept under a net the night before the survey.
In terms of use by those traditionally defined as vulnerable, the DHS shows only 40% of children below 5 years of age overall slept under a treated net the night prior to the survey. Even in households that own at least one net, 78% of these children slept under one.
A similar pattern is seen for treated net use by pregnant women. Overall 44% slept under a treated net, and 84% did so in households that owned at least one treated net. The internal household dynamics of net use where one is available does appear to favor these two groups.
Overall coverage of Intermittent Preventive Treatment for pregnant women is very low. Less than 30% of pregnant women received even the first dose of SP. This decreased to 21% for two doses and 13% for three. In contrast to net coverage, more rural women (31%) received the first dose of IPTp than urban ones (19%).
 Nearly 40% of children below five years of age were found to have had a fever in the two weeks preceding the survey. Among those care was sought for only two-thirds. Eleven percent of those with fever received an artemisinin-based combination therapy drug. The report did not mention whether these children had received any testing prior to treatment, so appropriateness of treatment cannot be judged. Prevalence testing of the children in the sample found 38% with parasitemia. Therefore one might assume that more children should have received ACTs.
Nearly 40% of children below five years of age were found to have had a fever in the two weeks preceding the survey. Among those care was sought for only two-thirds. Eleven percent of those with fever received an artemisinin-based combination therapy drug. The report did not mention whether these children had received any testing prior to treatment, so appropriateness of treatment cannot be judged. Prevalence testing of the children in the sample found 38% with parasitemia. Therefore one might assume that more children should have received ACTs.
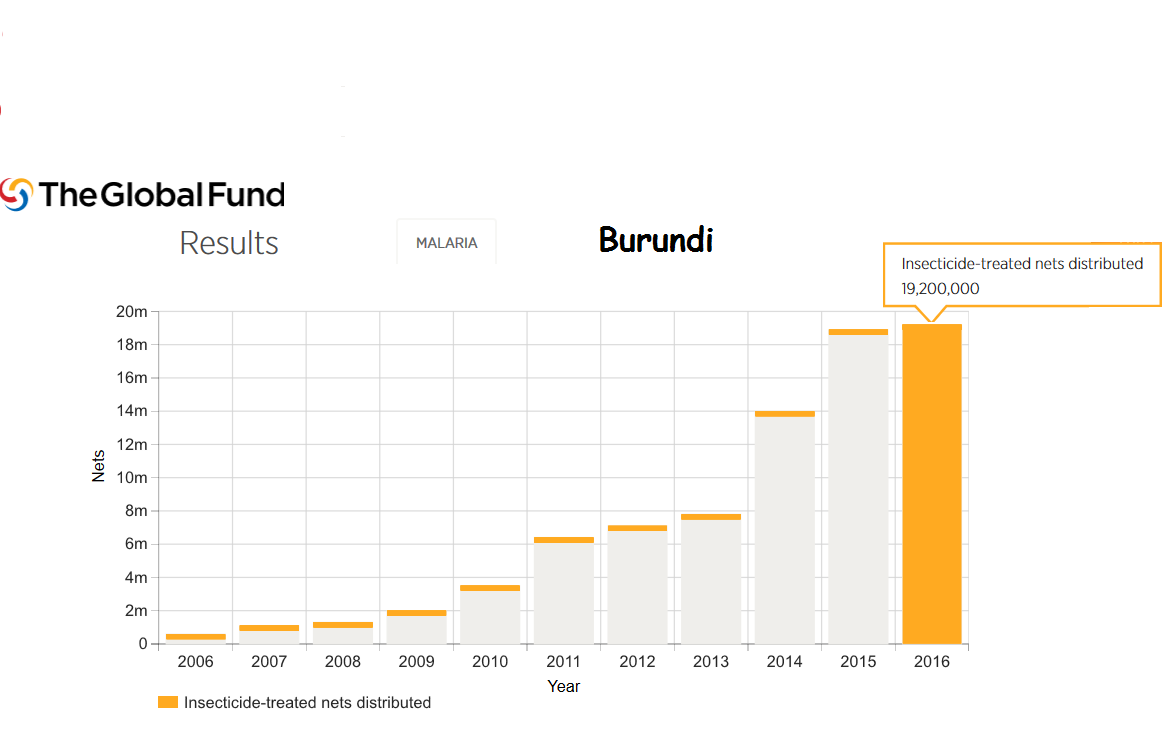
Burundi still faces major political and social challenges. Even so Burundi is the recipient of malaria support from the Global Fund. For example 18 million LLINs were distributed in 2015 and 19 million in 2016.
Much work is needed to bring Burundi even close to universal coverage of malaria interventions. In today’s climate of questionable donor commitment, it is hoped that regional partners may play a role since malaria knows no boundaries.
Drug Development &Treatment Bill Brieger | 29 May 2017
World No Tobacco Day – except to make malaria drugs
 May 31st marks World No Tobacco Day. The Theme for 2017 is “Tobacco – a threat to development.” According to WHO, “Tobacco control has been enshrined in the Sustainable Development Agenda. It is seen as one of the most effective means to help achieve SDG target 3.4 of a one-third reduction globally, by 2030, of premature deaths from noncommunicable diseases (NCDs).” Control is also associated with positive environmental and anti-poverty outcomes.
May 31st marks World No Tobacco Day. The Theme for 2017 is “Tobacco – a threat to development.” According to WHO, “Tobacco control has been enshrined in the Sustainable Development Agenda. It is seen as one of the most effective means to help achieve SDG target 3.4 of a one-third reduction globally, by 2030, of premature deaths from noncommunicable diseases (NCDs).” Control is also associated with positive environmental and anti-poverty outcomes.
It is ironic then that the tobacco plant itself may be modified to produce life saving anti-malarial medicines. Nature reported that because Artemisia annua produces a precursor of the compound, artemisinic acid, only in low quantities, it is expensive to grow. Consequently, “a team led by Ralph Bock at the Max Planck Institute of Molecular Plant Physiology in Potsdam-Golm, Germany, inserted genes for artemisinic acid synthesis into tobacco plants’ chloroplasts — abundant organelles that have their own DNA. By adding ‘accessory genes’ that make artemisinic acid production more efficient, they created a line that pumps out 120 milligrams of artemisinic acid per kilogram of biomass.”
Science magazine followed up to report that although “several years ago researchers transplanted the drugmaking genes into yeast, allowing them to collect the compound from a microbial brew, the fermentation process is still relatively expensive.” Tobacco, on the other hand, is an “inexpensive, high-volume crop.” Inserting the right genes into tobacco, they noted, would enable “harvesting artemisinic acid from a plot of land 200 square kilometers—less area than a city the size of Boston—would provide enough artemisinin to meet the entire worldwide demand.”
Malhotra et al. discovered another novel approach that found that, “Partially purified extracts from the leaves of transgenic tobacco plants inhibited in vitro growth progression of Plasmodium falciparum-infected red blood cells. Oral feeding of whole intact plant cells bioencapsulating the artemisinin reduced the parasitemia levels in challenged mice in comparison with commercial drug. Such novel synergistic approaches should facilitate low-cost production and delivery of artemisinin and other drugs through metabolic engineering of edible plants.”
Another approach looks at malaria vaccines. Beiss et al. note that malaria “transmission blocking vaccine (TBVs) need to be produced in large quantities at low cost.” They found a high level transient expression in fresh leaves of Nicotiana benthamiana of an effective TBV candidate. Likewise Jones et al. demonstrated the potential of the new malaria vaccine candidate and also support feasibility of expressing Plasmodium antigens in Nicotiana benthamiana.
The American Cancer Society observed that most African Countries are in the early stages of the tobacco epidemic. This may be a good time to switch the production of tobacco on the continent from purveyor of cancer and NCDs to a ‘factory’ for producing malaria medicines. The sooner this can be done, the better since artemisinin resistance is a growing threat.
Elimination &Epidemiology &Funding &IPTp &ITNs &Procurement Supply Management &Treatment Bill Brieger | 20 May 2017
Ghana – spotlight on malaria indicators
 The Demographic and Health Surveys has released a brief on key indicators from the Ghana Malaria Indicator Survey of 2016. While much of the malaria community is discussing the elimination framework and processes, the reality is that many high burden countries are still trying to scale up basic interventions to achieve universal coverage.
The Demographic and Health Surveys has released a brief on key indicators from the Ghana Malaria Indicator Survey of 2016. While much of the malaria community is discussing the elimination framework and processes, the reality is that many high burden countries are still trying to scale up basic interventions to achieve universal coverage.
The overall prevalence across the country in children aged 6-59 months at the time of the survey was 27% using Rapid Diagnostic test and 20% using microscopy. Among children reporting fever in the previous two weeks care/advice was sought for only 72%. Although only only 30% received some sort of blood based diagnostic test, 61% of the febrile children were given the antimalarial artemisinin-based combination therapy drugs.
 Children are still being treated without the benefit of parasitological testing, a key procedure highlighted in WHO case management guidelines. Presumptive treatment for malaria without testing means that a child could inappropriately receive antimalarial drugs and die of another underlying febrile illness. Appropriate testing and adherence to test results is one of the main areas of focus of Ghana’s grants from the US President’s Malaria Initiative. Improved testing is also an important element in Ghana’s current Global Fund support. Clearly more value for money is needed from these inputs.
Children are still being treated without the benefit of parasitological testing, a key procedure highlighted in WHO case management guidelines. Presumptive treatment for malaria without testing means that a child could inappropriately receive antimalarial drugs and die of another underlying febrile illness. Appropriate testing and adherence to test results is one of the main areas of focus of Ghana’s grants from the US President’s Malaria Initiative. Improved testing is also an important element in Ghana’s current Global Fund support. Clearly more value for money is needed from these inputs.
Preventive measures as documented in the MIS fare somewhat better., but at present only 73% of households own an insecticide treated bednet. When considering the recommended 1 net for every 2 household members, the indicator drops to 50%. Concerning the typical ‘vulnerable’ populations, we see that only 52% of children below the age of 5 years slept under an ITN the night before the survey; only 50% of pregnant women did likewise.
 Malaria prevention in pregnancy results reflect the fact that Ghana has promoted at least three IPTp doses for around ten years. Most pregnant women (78% ) had received the previously recommended minimum of two doses, and now 60% have received at least three doses.
Malaria prevention in pregnancy results reflect the fact that Ghana has promoted at least three IPTp doses for around ten years. Most pregnant women (78% ) had received the previously recommended minimum of two doses, and now 60% have received at least three doses.
One of the important issues stressed in WHO’s new malaria elimination framework is stratifying the country by prevalence to the lowest level possible in order to plan appropriate interventions. Fortunately the Ghana 217 MIS key indicator brief does stratify prevalence and intervention coverage by region. Prevalence through RDT testing ranges from nearly 5% in the urbanized greater Accra area to 44% in the Central Region. Interestingly ITN use is nearly 20% higher in Central than greater Accra.
Hopefully future planning in Ghana will build on this stratification. Better mobilization of donor, national and private sector resources will address likely issues of stock-outs and increase the likelihood of universal coverage of basic interventions that is needed to move the country along the road to malaria elimination.
CHW &Community &IRS &Treatment Bill Brieger | 27 Apr 2017
Rwanda Celebrates World Malaria Day 2017 – community is a major focus
Dr. Noella Umulisa, the Malaria Team Lead or the USAID Maternal and Child Survival Program in Kigali Rwanda shares with us experiences from Rwanda’s recent observance of World Malaria Day 2017.
The Malaria Day celebration took place in Huye districts in the southern Province. Why the southern province? – because among the 10 high endemic districts, 6 are the southern province. Why Huye district? – because IRS has been launched in Huye district yesterday and in another district Nyanza in Southern province.
 The ceremony was attended by USAID and WHO representative, local leaders, MOH staff, partners, population of Simbi sector and the guest of honour was Dr Jeannine Condo the Director General of Rwanda Biomedical Center (which houses malaria activities).
The ceremony was attended by USAID and WHO representative, local leaders, MOH staff, partners, population of Simbi sector and the guest of honour was Dr Jeannine Condo the Director General of Rwanda Biomedical Center (which houses malaria activities).
A special recognition was given to community health workers (CHWs) who are playing a key role and are on the front line of fighting Malaria through sensitization of the population, testing and treating the population through community case management (iCMM and HBM) of Malaria, and now when a big number of CHWs will be involved in spraying households in their community.
 The World Malaria Day celebration in Rwanda is marked by different activities for Malaria prevention conducted at community level from 24th to 29th April 2017. Also, Malaria prevention and control messages are being disseminated using different communication tools and approaches such as radio and TV programs, community outreach activities, educating communities on proper use of bed nets.
The World Malaria Day celebration in Rwanda is marked by different activities for Malaria prevention conducted at community level from 24th to 29th April 2017. Also, Malaria prevention and control messages are being disseminated using different communication tools and approaches such as radio and TV programs, community outreach activities, educating communities on proper use of bed nets.
Door to door mobilization is being conducted about the Indoor Residual Spraying (IRS) in high malaria burden districts of Huye and Nyanza. MCSP, with support from the US President’s Malaria Initiative, has participated actively in this event by supporting Community outreaches though theatre skits in the first 10 high endemic district.
 The Director General made the following statement:
The Director General made the following statement:
In January 2016, the Government of Rwanda and partners developed a Malaria Contingency Plan in response to the increase in malaria cases. The following interventions were implemented to address malaria rise in Rwanda: A Home Based Management of fever for adults at community level was set up countywide to reduce the malaria burden and prevent severe malaria and death. From Nov 2016 up to March 2017, the country distributed more than 6 million nets in 30 districts ensuring universal coverage of the entire population.
The country has increased access to health services for all through Community Based Health Insurance (CBHI). The Government of Rwanda provides free treatment of malaria to the most vulnerable population (Ubudehe 1&2 categories) to ensure that all financial barriers are no more to hinder the health service delivery for the community. Extension of Indoor residual spraying (IRS) in districts with high malaria burden where 5 out of 8 were sprayed (Nyagatare, Kirehe, Bugesera, Gisagara and Gatsibo).
We hope that this commitment will keep Rwanda on track to control and eventually eliminate malaria.
CHW &Diagnosis &Health Workers &Performance &Training &Treatment Bill Brieger | 06 Apr 2017
World Health Workers Week, a Time to Recognize Health Worker Contributions to Malaria Care
 Since the beginning of the Roll Back malaria Partnership in 1998 there has been strong awareness that malaria control success is inextricably tied to the quality of health systems. Achieving coverage of malaria interventions involves all aspects of the health system but most particularly the human resources who plan, deliver and assess these services. World Health Worker Week is a good opportunity to recognize health worker contributions to ridding the world of malaria.
Since the beginning of the Roll Back malaria Partnership in 1998 there has been strong awareness that malaria control success is inextricably tied to the quality of health systems. Achieving coverage of malaria interventions involves all aspects of the health system but most particularly the human resources who plan, deliver and assess these services. World Health Worker Week is a good opportunity to recognize health worker contributions to ridding the world of malaria.
We can start with community health workers who may be informal but trained volunteers or front line formal health staff. According to the Frontline Health Workers Coalition, “Frontline health workers provide immunizations and treat common infections. They are on the frontlines of battling deadly diseases like Ebola and HIV/AIDS, and many families rely on them as trusted sources of information for preventing, treating and managing a variety of leading killers including diarrhea, pneumonia, malaria and tuberculosis.”
 The presence of CHWs exemplifies the ideal of a partnership between communities and the health system. With appropriate training and supervision CHWs ensure that malaria cases are diagnosed and treated promptly and appropriately, malaria prevention activities like long lasting insecticide-treated nets are implemented and pregnant women are protected from the dangers of the disease. CHWs save lives according to Nkonki and colleagues who “found evidence of cost-effectiveness of community health worker (CHW) interventions in reducing malaria and asthma, decreasing mortality of neonates and children, improving maternal health, increasing exclusive breastfeeding and improving malnutrition, and positively impacting physical health and psychomotor development amongst children.”
The presence of CHWs exemplifies the ideal of a partnership between communities and the health system. With appropriate training and supervision CHWs ensure that malaria cases are diagnosed and treated promptly and appropriately, malaria prevention activities like long lasting insecticide-treated nets are implemented and pregnant women are protected from the dangers of the disease. CHWs save lives according to Nkonki and colleagues who “found evidence of cost-effectiveness of community health worker (CHW) interventions in reducing malaria and asthma, decreasing mortality of neonates and children, improving maternal health, increasing exclusive breastfeeding and improving malnutrition, and positively impacting physical health and psychomotor development amongst children.”
 CHWs do not act in isolation but depend on health workers at the facility and district levels for training, supervision and maintenance of supplies and inventories. These health staff benefit from capacity building – when they are capable of performing malaria tasks, they can better help others learn and practice.
CHWs do not act in isolation but depend on health workers at the facility and district levels for training, supervision and maintenance of supplies and inventories. These health staff benefit from capacity building – when they are capable of performing malaria tasks, they can better help others learn and practice.
A good example of this capacity building is the Improving Malaria Care (IMC) project in Burkina Faso, implemented by Jhpiego and supported by USAID and the US President’s malaria Initiative. IMC builds capacity of health workers at facility and district level to improve malaria prevention service delivery and enhance accuracy in malaria diagnosis and treatment. Additionally capacity building is provided to health staff in the National Malaria Control Program to plan, design, manage and coordinate a comprehensive malaria control program. As a result of capacity building there has been a large increase in malaria cases diagnosed using parasitological techniques and in the number of women getting more doses of intermittent preventive treatment to prevent malaria during pregnancy.
Malaria care is much more than drugs, tests and nets. Health worker capacity is required to get the job done and move us forward on the pathway to eliminate malaria.
Asia &ITNs &Treatment Bill Brieger | 29 Mar 2017
Myanmar – update on malaria indicators
 Myanmar is one of the countries at the epicenter of the developing resistance of malaria parasites to artemisinin based drugs. This means there is a strong need for prompt, appropriate and thorough diagnosis and treatment of febrile illnesses and malaria as well as the regular use of effective malaria preventive technologies. The 2015-16 Demographic and Health Survey for the country is thus a timely source of information to improve malaria interventions. Highlights from the DHS follow.
Myanmar is one of the countries at the epicenter of the developing resistance of malaria parasites to artemisinin based drugs. This means there is a strong need for prompt, appropriate and thorough diagnosis and treatment of febrile illnesses and malaria as well as the regular use of effective malaria preventive technologies. The 2015-16 Demographic and Health Survey for the country is thus a timely source of information to improve malaria interventions. Highlights from the DHS follow.
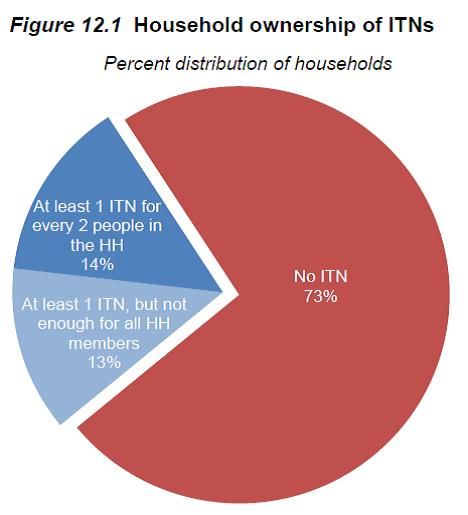
The first major concern is both lack of insecticide treated nets as well as low use of those available as the pie chart from the DHS makes clear. Ironically 97% of households have some kind of net, but 73% do not have an insecticide treated one. Although the Global Fund has supported distribution of 4.3 million ITNs in the country, there are over 56 million people living there. The US President’s Malaria Initiative has procured nearly 900,000 ITNs for the country. 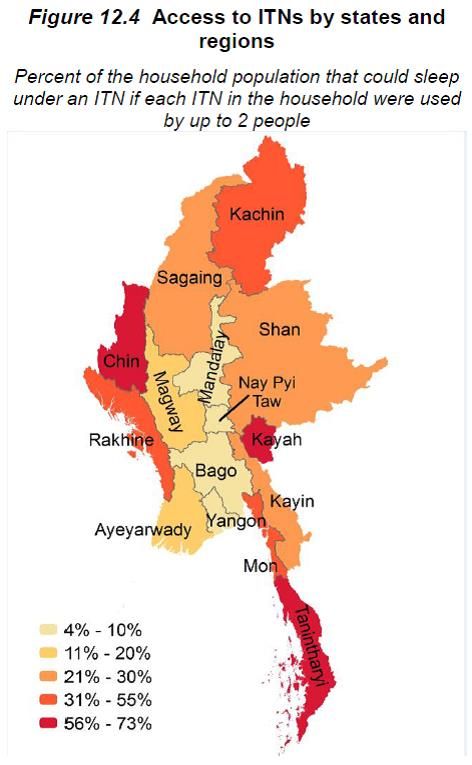 Although low across all economic strata, the lowest wealth quintile have the highest ITN possession (35%).
Although low across all economic strata, the lowest wealth quintile have the highest ITN possession (35%).
The 2013 concept note submitted by Myanmar to Global Fund under the new funding mechanism identifies many of the challenges: “Factors that may cause inequity to services for treatment and prevention: There are several population groups, which are poorly served by the health system and malaria services such as those living in remote border areas, migrant populations, forest workers and miners where malaria transmission is intense. Many of them are internal and external migrants who usually have limited access to malaria prevention and control. Major factors include distance from health facilities and poor awareness of malaria and its prevention.”
 Key strategies in the Global Fund Concept Note do address quality malaria diagnostics and appropriate treatment. Unfortunately DHS results do not yet show the impact of improved diagnosis and treatment. “Overall, 16% of children under age 5 had a fever in the 2 weeks before the survey. Advice or treatment was sought for 65% of these children with recent fever, and 3% had blood taken from a finger or heel, presumably for diagnostic testing.” A variety of public and private sources were used to seek fever treatment, but “Only
Key strategies in the Global Fund Concept Note do address quality malaria diagnostics and appropriate treatment. Unfortunately DHS results do not yet show the impact of improved diagnosis and treatment. “Overall, 16% of children under age 5 had a fever in the 2 weeks before the survey. Advice or treatment was sought for 65% of these children with recent fever, and 3% had blood taken from a finger or heel, presumably for diagnostic testing.” A variety of public and private sources were used to seek fever treatment, but “Only  1% of children received antimalarial drugs for treatment of fever in the 2 weeks preceding the survey.”
1% of children received antimalarial drugs for treatment of fever in the 2 weeks preceding the survey.”
In addition to formal donors, there are coalitions and consortia who provide encouragement, technical assistance, advocacy and capacity building for eliminating malaria in the Asia-Pacific region. While the country needs to take stronger leadership in malaria elimination, all groups need to come together and strengthen the malaria interventions in Myanmar as these have implications for eliminating the disease in the region as a whole.
Diagnosis &Elimination &Ivermectin &MDA &Treatment Bill Brieger | 20 Nov 2016
Leadership and Support for Malaria Pre-Elimination in Nepal
Emmanuel Le Perru, Jhpiego field staff in Nepal, shared his experiences in aiding the malaria pre-elimination efforts in the country during a retreat that preceded the 65th Annual Meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. Here are some highlights of his talk.
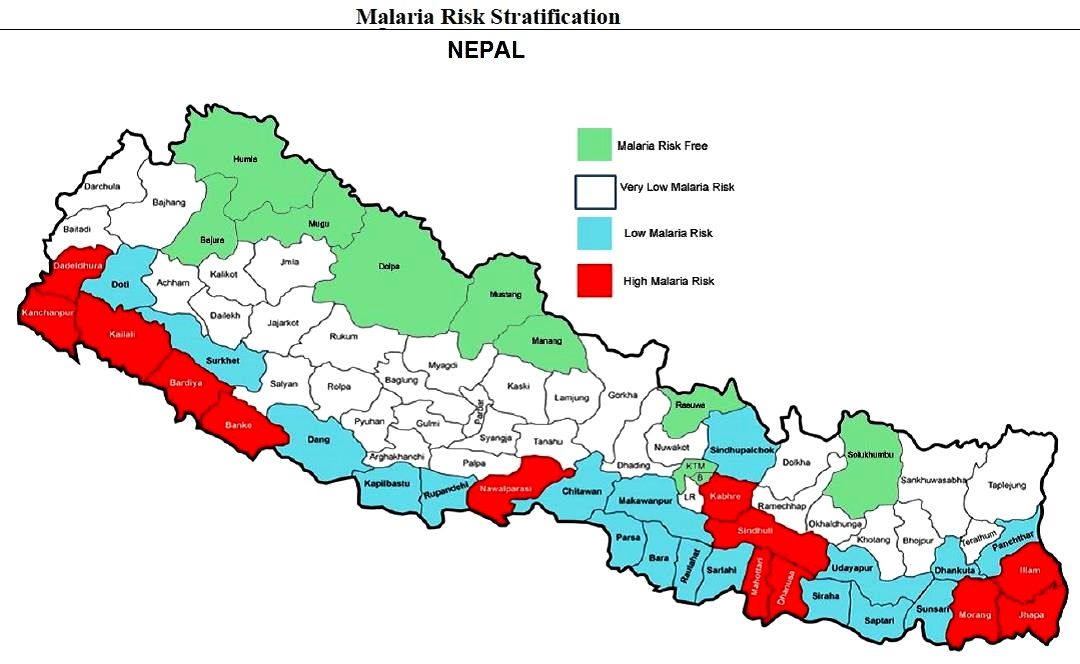 Malaria Pre-Elimination efforts are targeting 0 deaths as well as investigation of 100% of confirmed cases in Nepal. Systematic entomology investigation/interventions are required. Glucose-6-Phosphate Dehydrogenase deficiency (enzyme genetic defect causing hemolysis with primaquine) testing for Plasmodium vivax in high G6PDd prevalence communities is required. Cases should receive treatment within 72 hours of symptoms for Pf (to quickly prevent transmission and gametocyte reservoir). There is also a need to distinguish between indigenous and imported cases.
Malaria Pre-Elimination efforts are targeting 0 deaths as well as investigation of 100% of confirmed cases in Nepal. Systematic entomology investigation/interventions are required. Glucose-6-Phosphate Dehydrogenase deficiency (enzyme genetic defect causing hemolysis with primaquine) testing for Plasmodium vivax in high G6PDd prevalence communities is required. Cases should receive treatment within 72 hours of symptoms for Pf (to quickly prevent transmission and gametocyte reservoir). There is also a need to distinguish between indigenous and imported cases.
Jhpiego is providing technical assistance and capacity building for Nepal’s Ministry of Health pre-elimination efforts as follows:
- Integrated Vector Management
- Micro-stratification
- Entomology curriculum to be conducted in medical college (need new positions)
- Case-based Surveillance guidelines
- Private-sector engagement (for increased reporting and product quality control/procurement such as Antigen RDTs)
- Capacity Assessments in 9 health systems strengthening components at central and district levels (Jhpiego Malaria Implementation Guide)
- Human resources: clear job descriptions and performance goals
- Leadership & Management development program
 Program highlights include the fact that the Global Fund malaria grant rating improved from B2 (inadequate but demonstrating potential) in January 2016, but now A2 (meeting expectations) in November 2016. Concept note for operational research at 2 or 3 border check points has been developed in order to determine whether such intervention (communication & voluntary screening) is cost-effective and relevant to catch/target imported cases, raise awareness on malaria available services, detect/prevent sources of potential outbreaks. This will inform GFATM on the relevance to fund such intervention. A similar approach was done at the China-Myanmar border but was not recognized by not WHO.
Program highlights include the fact that the Global Fund malaria grant rating improved from B2 (inadequate but demonstrating potential) in January 2016, but now A2 (meeting expectations) in November 2016. Concept note for operational research at 2 or 3 border check points has been developed in order to determine whether such intervention (communication & voluntary screening) is cost-effective and relevant to catch/target imported cases, raise awareness on malaria available services, detect/prevent sources of potential outbreaks. This will inform GFATM on the relevance to fund such intervention. A similar approach was done at the China-Myanmar border but was not recognized by not WHO.
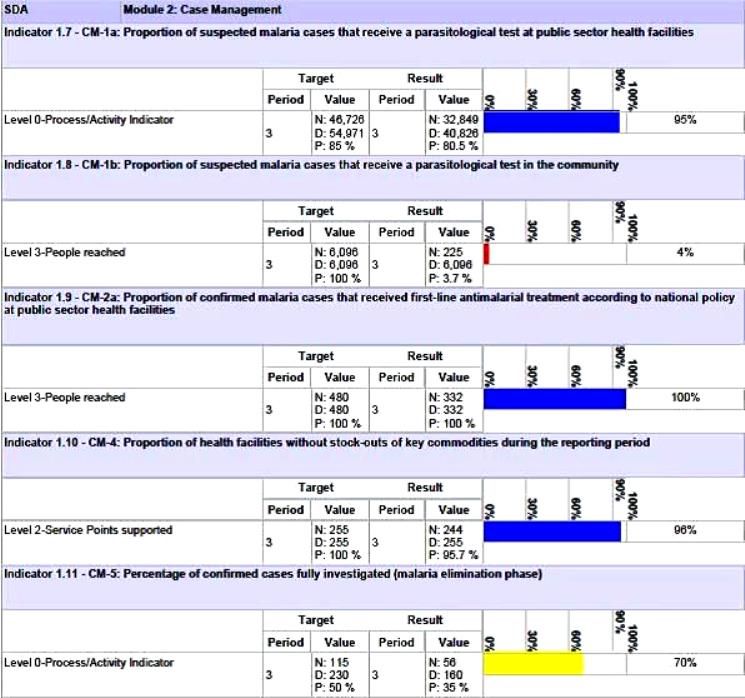
Nepal’s Global Fund Grant Indicators for Malaria Case Management
Although the National Malaria Strategic Plan refers to high risk groups (forest workers, national parks security personnel, refugees, prisoners, etc.) evidence is needed to back this up. A study or improved investigation forms are needed to identify such groups and use this information to design appropriate behavior change communications and other interventions.
Special Programming Highlights include proposing a focus on Closed/Isolated Settings/Foci (limited migration, duration and population) to WHO and GFATM. Considering a targeted mass drug administration (MDA) Plasmodium vivax (not yes recommended by WHO) with Primaquine/G6PD testing. Consideration is being given to new drugs in the pipeline such as Ivermectin. Molecular Testing using Polymerase Chain Reaction (PCR) to detect low parasitemia, asymptomatic or re-infection cases (Pv includes inactive/dormant sporozoites known as hypnozoites) is being proposed.
Community based testing as proposed in the Global Fund grant needs strengthening. Therefore RDT use by Female Community Health Volunteer is being considered. Active case detection is another possibility for those areas moving toward pre-elimination. As mentioned, there is also need for studies of asymptomatic infection.
Lessons learned so far for best practices for efforts in identifying specific pre-elimination interventions include the value of getting consensus at national level through the Malaria Technical Working Group. There is also need to challenge WHO recommendations and engage dialogue to get creative. At present there is a risk of a Catch 22 situation wherein the GFATM asks for innovative interventions but at the same time tries to adhere strictly WHO to existing guidance.
The Nepalese malaria program is in constant dialogue with the GFATM Fund Portfolio Manager and team on the local context and technical challenges in order to get them involved in looking for innovative solutions.
Challenges arise in malaria diagnostics. While systematic microscopy is the gold standard, quality can be poor because of low stain/re-agent quality, constant staff turnover and donor reluctance to fund additional training. Also microscopy confirmation and slide quality control are time consuming, and often this process is not clear or well followed. PCR require specific equipment, training and qualifications. Takes time to be operational.
There are opportunities moving forward. Progress could be made if there were more “elimination experts” to position to influencer to WHO to seek and propose new interventions for the pre-elimination stage. Nepal provides an ideal opportunity to test new ideas. It will also be necessary for the national malaria program staff to receive regular technical updates on program issues such as new drugs (Ivermectin?) and on-going pilots of MDA.
CHW &Diagnosis &iCCM &Treatment Bill Brieger | 14 Nov 2016
A Pilot to Use Malaria RDTs at the Community Level in Burkina Faso
A poster entitled “The Improving Malaria Care (IMC) Project’s Contribution to follow up a Pilot to Use Rapid Diagnostic Tests (RDTs) at the Community Level in Burkina Faso” was presented by members of Jhpiego’s Burkina Faso Team: Ousmane Badolo, Stanislas P. Nebie, Moumouni Bonkoungou, Mathurin Dodo, Rachel Waxman, Danielle Burke, William Brieger at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
CHWs provide malaria testing, treatment and health education
Early and correct case management of malaria in health facilities and at the community level is among the priorities of Burkina Faso’s National Malaria Control Program (NMCP). In line with this initiative, the NMCP piloted use of Rapid Diagnostic Tests (RDTs) by Community Health Workers (CHWs) to confirm malaria cases in the three health districts of Kaya, Saponé and Nouna between 2013 and 2015. With PMI support, follow-up visits were organized to document best practices, as well as challenges, on RDT use by CHWs that could serve as lessons learned for scale-up.
During follow-up visits, malaria commodities management (supply, storage and use) at the community level was examined, use of RDTs was assessed, and implementation at the community 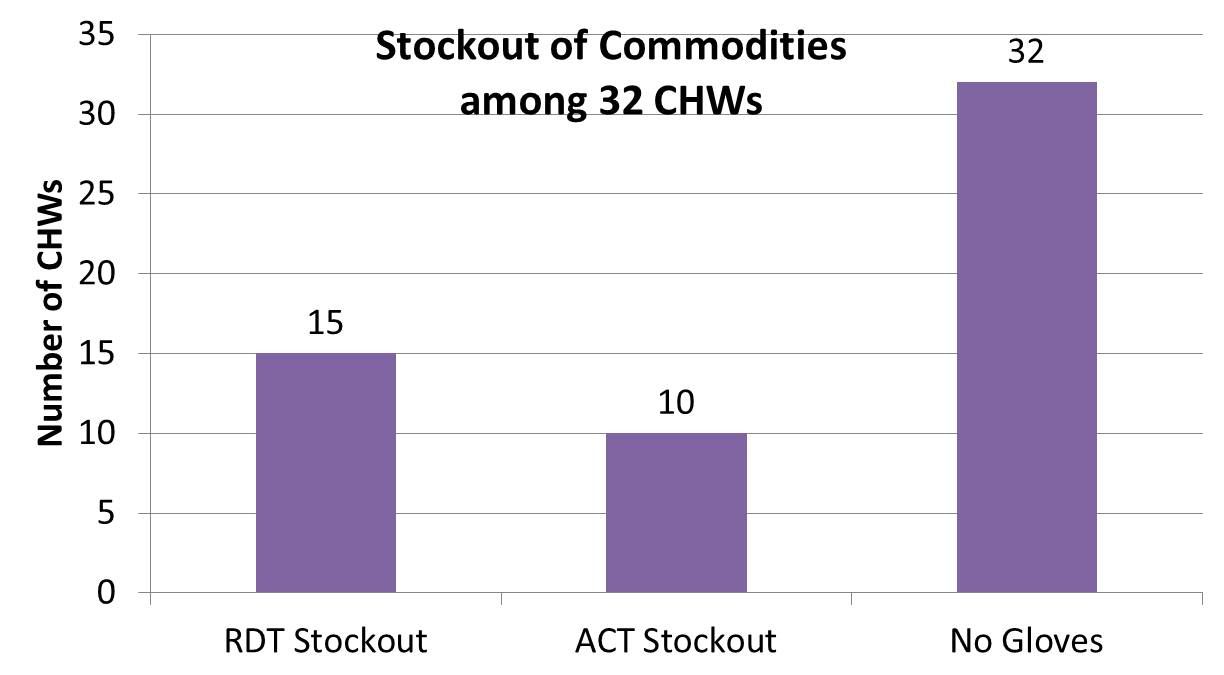 level was discussed with all actors at regional, district, health facilities, and community levels. The team examined the monitoring/supervision processes at all levels, used a check list on malaria commodities management, and employed a questionnaire for each type of actor. Both qualitative and quantitative data have been collected. A total of 108 persons were contacted including 32 CHWs, 42 community leaders and 34 health care providers and managers.
level was discussed with all actors at regional, district, health facilities, and community levels. The team examined the monitoring/supervision processes at all levels, used a check list on malaria commodities management, and employed a questionnaire for each type of actor. Both qualitative and quantitative data have been collected. A total of 108 persons were contacted including 32 CHWs, 42 community leaders and 34 health care providers and managers.
 Findings revealed frequent stock-outs of RDTs and artemisinin-based combination therapies, non-payment of stipends to CHWs (a demotivator) and insufficient supervision of CHW by health teams. From the community perspective, 66% of community leaders were satisfied with their CHW’s work (diagnosis and treatment of uncomplicated malaria
Findings revealed frequent stock-outs of RDTs and artemisinin-based combination therapies, non-payment of stipends to CHWs (a demotivator) and insufficient supervision of CHW by health teams. From the community perspective, 66% of community leaders were satisfied with their CHW’s work (diagnosis and treatment of uncomplicated malaria  and referral of severe cases to health facilities). However, 46% of community leaders complained of frequent stock-outs and unanimously agreed on the importance of regular payment of premiums to CHW.
and referral of severe cases to health facilities). However, 46% of community leaders complained of frequent stock-outs and unanimously agreed on the importance of regular payment of premiums to CHW.
Follow up of the pilot was valuable in obtaining community, CHW and health worker perspectives for improving the program. While the community finds the program acceptable, its sustainability will require that solutions be found for stock-outs, non-payment, and insufficient supervision before scale up takes place.