Capacity Building &Costs &Research &Seasonal Malaria Chemoprevention &Surveillance &Treatment Bill Brieger | 04 May 2018
Multilateral Initiative for Malaria: Posters Range from Prevention to Cost to E-Learning and Beyond
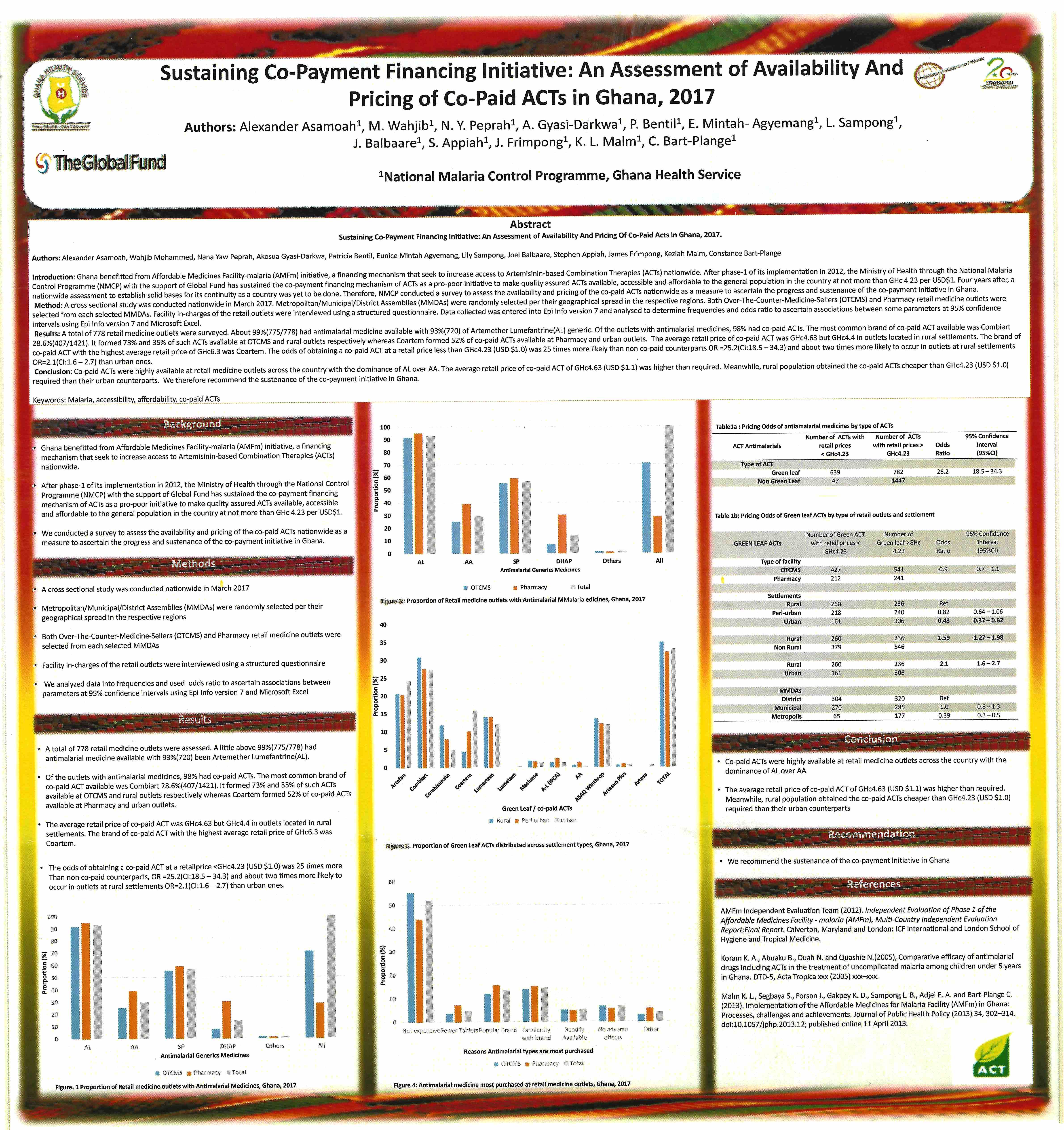
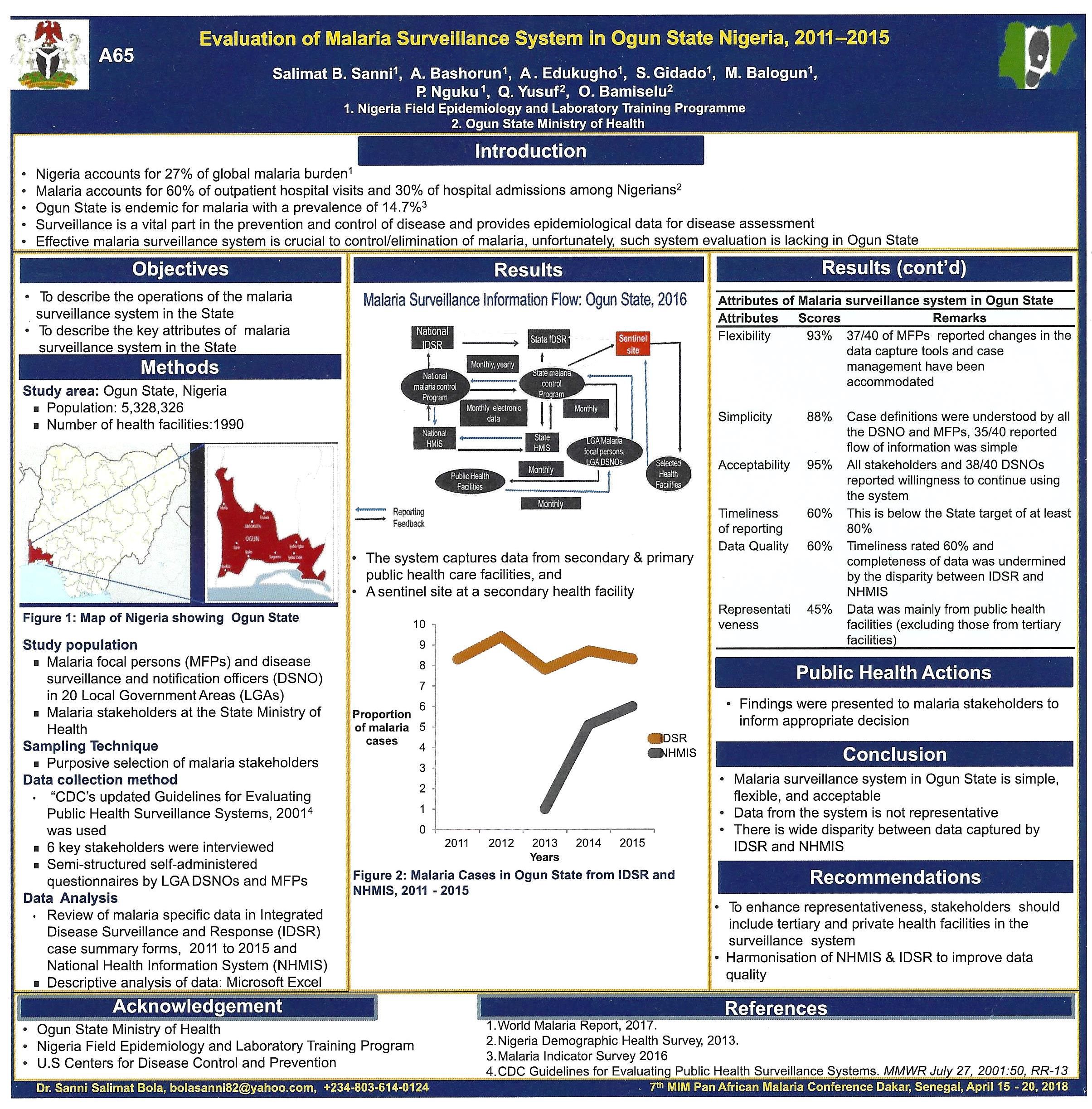
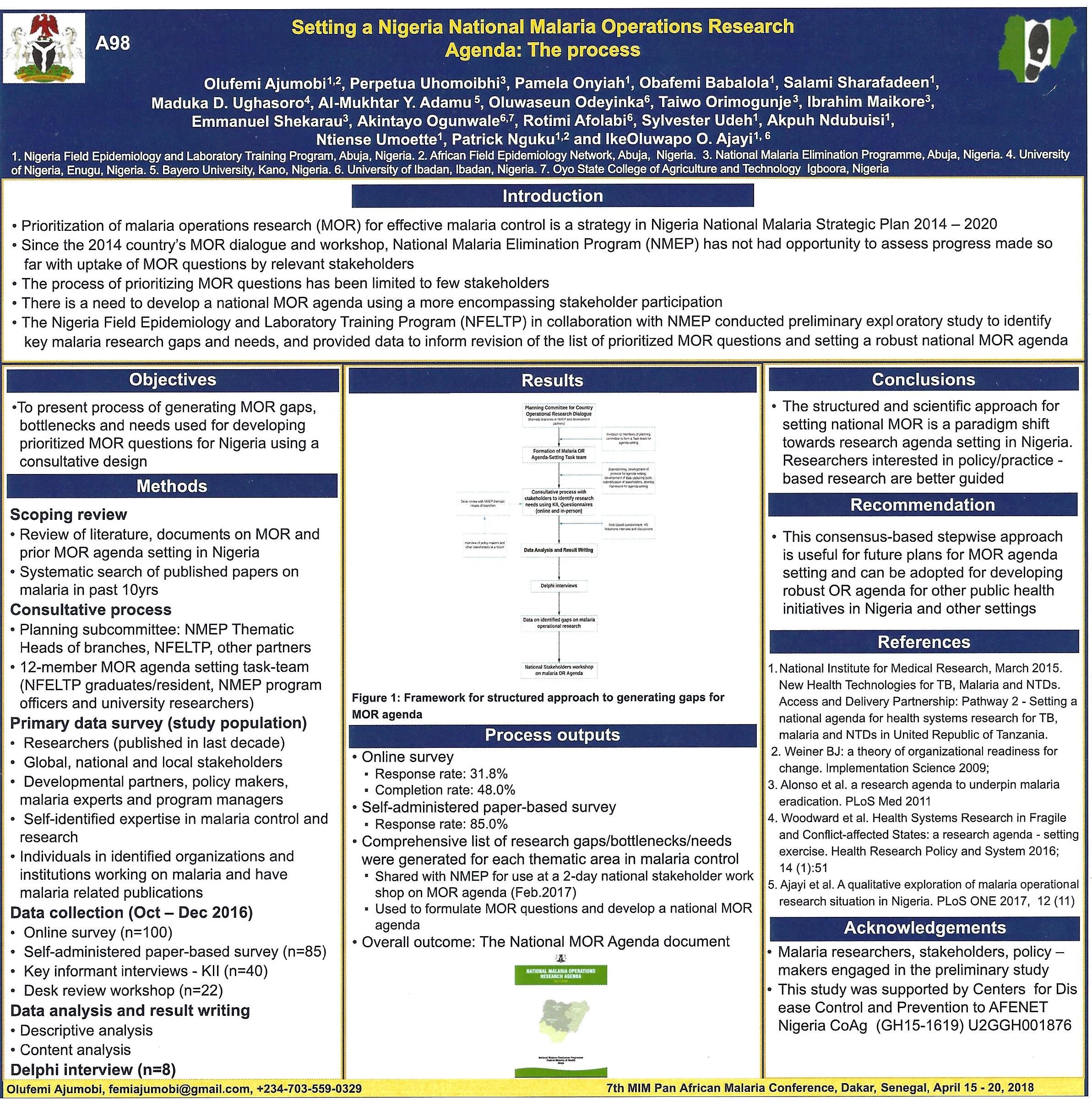
A major feature of all conferences are the poster sessions. These are often overlooked due to timing and placement. Fortunately at the recent 7th Multilateral Initiative for Malaria Conference in Dakar, tea breaks and lunch were made available in the poster tent ensuring more people came to view. Even so some people may have missed the valuable knowledge shared through this medium. We tweeted many of the posters during the event, but below are six posters in more detail.
These range from evaluating a malaria surveillance system to financing systems to sustain malaria drug supplies, including through community pharmacies. The potential of E-Learning for malaria capacity building was explored, and the process pf establishing a national malaria operations research agenda was presented. Several posters examined the seasonal malaria chemoprevention (SMC) program in the Sahel of West Africa including one from Mali as seen below.
Please contact the authors for additional information and updates. Readers who presented a poster at MIM are welcome to share their findings with us.



Eradication &Migration &Surveillance Bill Brieger | 06 Feb 2018
Malaria Should Lead to Compassion, Not Hate
In August 2017 the ‘Almost Impossible’ happened decades after the last of local malaria transmission stopped in Italy. NPR shared news from the Italian newspaper Corriere della Sera that, “A 4-year-old girl has died of malaria in Italy, where the disease is thought to have been wiped out. Troubled health officials are looking for answers.” By coincidence, two children from an African nation were being treated for malaria in the same hospital where the deceased was being treated for diabetes. No epidemiological link could be found.

World Malaria Report: http://www.who.int/malaria/publications/world-malaria-report-2017/en/
Unfortunately that has not stopped anti-immigrant politicians from using the incident to foster hatred. The political party of a “far-right extremist who wounded 6 African immigrants in a racially motivated shooting rampage in central Italy,” blamed the death of the child mentioned above “from malaria on migrants who ‘bring back to Europe’ once, eradicated illnesses.”
A new article in Malaria Journal reports that even though, “Malaria is no longer endemic in Italy since 1970 when the World Health Organization declared Italy malaria-free, … it is now the most commonly imported disease.” The study from Parma, Italy reports that, “Of the 288 patients with suspected malaria, 87 were positive by microscopy: 73 P. falciparum, 2 P. vivax, 8 P. ovale, 1 P. vivax/P. ovale, 1 P. malariae and 2 Plasmodium sp. All samples were positive by ICT except 6. ”
Malaria can travel with anyone who has been in an endemic area, whether migrant, tourist or business person. The likelihood of malaria re-establishing itself in currently non-endemic areas is low, but there is of course value in maintaining epidemiological and entomological surveillance world-wide in the current drive to eradicate the disease.
The identification of malaria anywhere in the world should be cause for concern and compassion, not hate and exclusion.
Advocacy &Borders &Children &Conflict &Costs &Epidemiology &Funding &Human Resources &Leadership &Monitoring &Mortality &NTDs &Partnership &Surveillance Bill Brieger | 03 Feb 2018
African Leaders Malaria Alliance Recognizes Country Achievements, Adds NTDs to its Scorecard
 The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
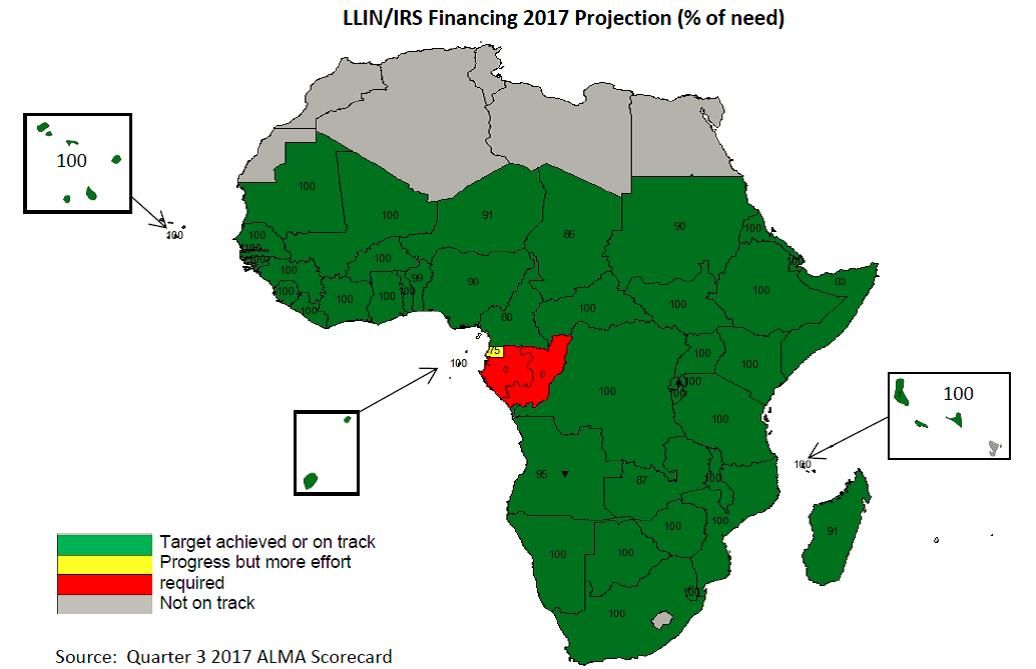
 For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
The scorecard will now “report progress for the 47 NTD-affected countries in sub-Saharan Africa in their strategies to treat and prevent the five most common NTDs: lymphatic filariasis, onchocerciasis, schistosomiasis, soil-transmitted helminths and trachoma. By adding NTDs to the scorecard, African leaders are making a public commitment to hold themselves accountable for progress on these diseases.”
 In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
The combination is based on the logic that NTDs and malaria are both diseases of poverty. Malaria and several NTDs are also vector-borne. Also community platforms are a foundation for delivering needed drugs and supplies to tackle these diseases. Ultimately the decision shows that Heads of State are holding themselves accountable for progress in eliminating these diseases.
 At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
 The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
H.E . Dr. Barnabas Sibusiso Dlamini, the Prime Minister of the Kingdom of Swaziland, whose King and Head of State is the current chair of ALMA, warned all endemic countries that, “When we take our eyes off malaria, the cost for our countries is huge. Yet if we increase our efforts to control and eventually eliminate malaria, the yield we get from it is tremendous. It is time that we dig deep into our pockets and provide malaria programmes with the needed resources.”
 Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
IRIN concludes that, “For now, the biggest challenge for Zambia will be closing the gap in its malaria elimination strategy, which will cost around $160 million a year and is currently only about 50 percent funded – two thirds from international donors and one third from the Zambian government. Privately, international donors say the government must spend more money on its malaria programme if it is to succeed.” Cross-border transmission adds to the problem.
Internal strife is another challenge to malaria success. “The recent nurses’ strike which lasted for five months may have cost Kenya a continental award in reducing the prevalence of malaria during the 30th African Union Summit in Ethiopia on Sunday.” John Muchangi in the Star also noted that, “However, Kenya lost momentum last year and a major malaria outbreak during the prolonged nurses’ strike killed more than 30 people within two weeks in October.”
 Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Fortunately ALMA is equipped with the monitoring and advocacy tools to ensure that its members recognize and respond to such challenges. The Scorecards will keep the fight against the infectious diseases of poverty on track.
Cholera &Surveillance &water Bill Brieger | 19 Dec 2017
Comprehensive Cholera Prevention and Control: Lessons Learnt from the United Republic of Tanzania
Dafrossa Lyimo of the Ministry of Health, Tanzania presented Tanzania’s experience in preventing and controlling cholera at the 4th African Regional Immunization Technical Advisory Group (RITAG) meeting in Johannesburg, 5-8 December 2017. Those experiences are summarized below.
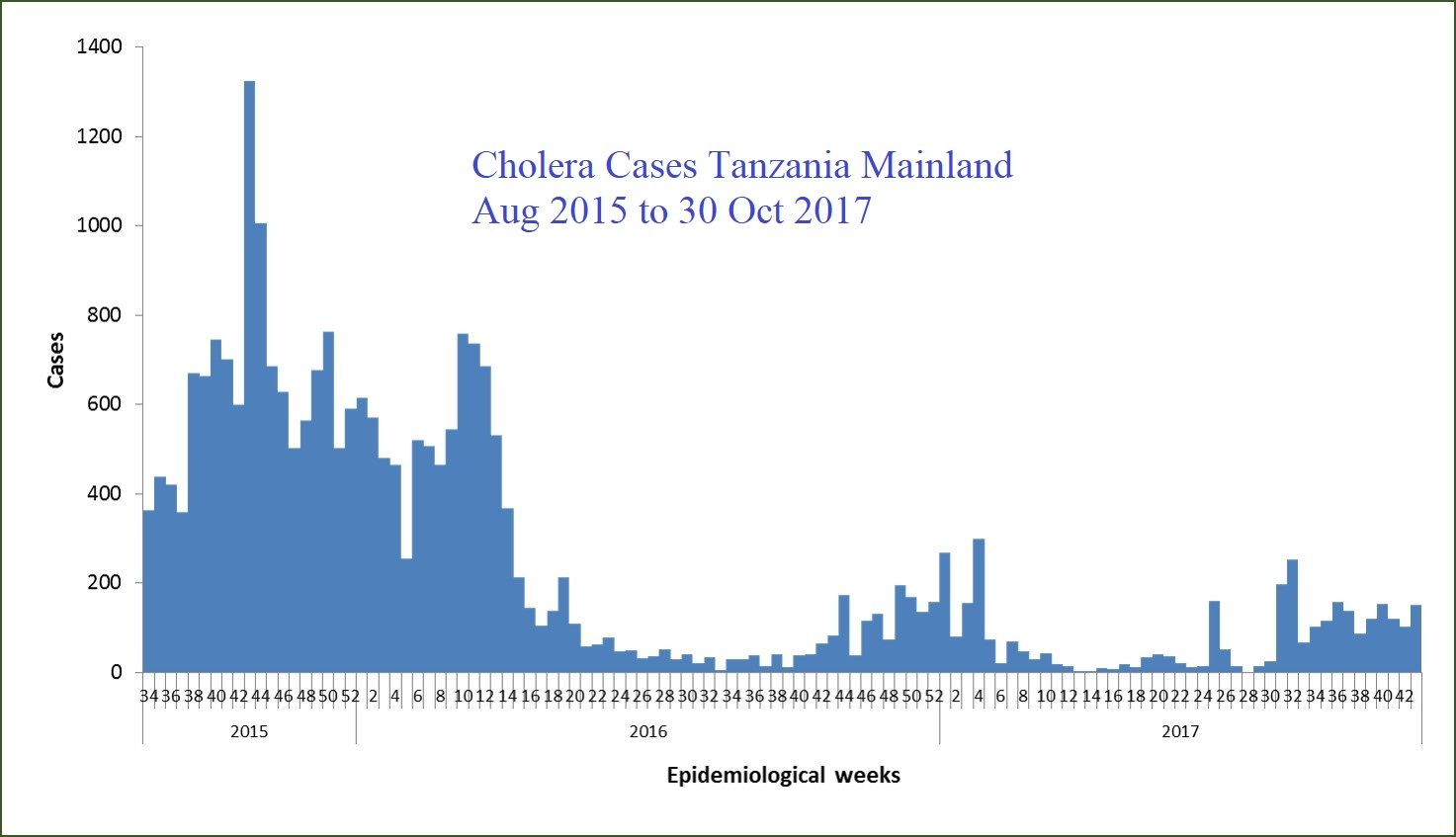
Cholera outbreak in Tanzania started with the index case detected in Dar es Salaam Region on 6 August 2015. The World Health Organization was notified by Ministry of Health on 15 August 2015. By 31 December 2015 the outbreak spread to 22 out of 26 regions in Tanzania Mainland. Zanzibar started reporting cholera cases on 20 September 2015 from Urban West District in Unguja Island. By December 2015, the outbreak spread to all 10 districts of Pemba and Unguja.
 Cumulative cases on the Tanzania Mainland were 12 619 cases with 199 deaths (CFR 1.57%) in 2015, 11 360 cases with 172 deaths (CFR 1.5%) in 2016, and up through Nov 2017, 3 615 cases with 61 deaths (CFR 1.7%). Likewise the Cumulative cases in Zanzibar were 1 143 cases with 15 deaths (1.31%) in 2015, 3 187 cases with 53 deaths (CFR 1.66%) in 2016 and as of Nov 2017, 358 cases with 4 deaths (CFR 1.12%). The last case reported 11 July 2017
Cumulative cases on the Tanzania Mainland were 12 619 cases with 199 deaths (CFR 1.57%) in 2015, 11 360 cases with 172 deaths (CFR 1.5%) in 2016, and up through Nov 2017, 3 615 cases with 61 deaths (CFR 1.7%). Likewise the Cumulative cases in Zanzibar were 1 143 cases with 15 deaths (1.31%) in 2015, 3 187 cases with 53 deaths (CFR 1.66%) in 2016 and as of Nov 2017, 358 cases with 4 deaths (CFR 1.12%). The last case reported 11 July 2017
Best practices for controlling cholera in the country fall in four domains. In the area od Coordination Tanzania established a Public Health Emergency Operations Centre (PHEOC) in the Ministry of Health. To support this the Ministry appointed an Incident Manager, Deputy Incident Manager, and a PHEOC Manager for the cholera outbreak response. The National Task force Team was established with a wider composition which meeting every Friday discussing issues and giving way forward. National Rapid Response Teams were trained. these teams worked based on national response guidelines which were developed and distributed to all districts.
 In the domain of Surveillance, the Ministry initiated a Daily Situation Report (SITREP) for sharing a daily cholera status in the regions and districts , on going interventions and gaps. This group conducted twice a country wide data validation/verification of the reported cases in 17 regions, which also confirmed under-reporting of cases. A Cholera reporting line list register was designed and printed in booklets and distributed to 26 regions in the Tanzania Mainland, to standardize reporting from districts and regions.
In the domain of Surveillance, the Ministry initiated a Daily Situation Report (SITREP) for sharing a daily cholera status in the regions and districts , on going interventions and gaps. This group conducted twice a country wide data validation/verification of the reported cases in 17 regions, which also confirmed under-reporting of cases. A Cholera reporting line list register was designed and printed in booklets and distributed to 26 regions in the Tanzania Mainland, to standardize reporting from districts and regions.
 The third domain consisted of Water Sanitation and Hygiene interventions. The country distributed 21,600,000 aqua tablets of water guards in 514,285 households. Also distributed were 50 drums 45kg each of 70% High Test Hypochlorite to 83 district water authorities for bulk chlorination. Twenty hand pump boreholes were installed in hotspot villages of Mara and Mwanza regions, thereby Improving the access to clean and safe water. One hundred HACH chlorine testers were distributed for monitoring free residue chlorine in cholera reporting districts.
The third domain consisted of Water Sanitation and Hygiene interventions. The country distributed 21,600,000 aqua tablets of water guards in 514,285 households. Also distributed were 50 drums 45kg each of 70% High Test Hypochlorite to 83 district water authorities for bulk chlorination. Twenty hand pump boreholes were installed in hotspot villages of Mara and Mwanza regions, thereby Improving the access to clean and safe water. One hundred HACH chlorine testers were distributed for monitoring free residue chlorine in cholera reporting districts.
Social Mobilization was the fourth domain. Cholera leaflets and fliers were designed and distributed in reporting districts. Cholera messages were developed and aired through community media and mobile phone messaging. Community engagement and owning cholera interventions was undertaken using the community social networks and peer groups who focused on Hand washing, Use of treated water, and Use of toilets behaviors.
 Cholera control and prevention efforts addressed various Challenges
Cholera control and prevention efforts addressed various Challenges
in Tanzania. one concern was a weak surveillance system starting at the district level in several districts. Lack of reporting cholera cases, under-reporting and late reporting occurred. In some districts that had laboratory capacity, only positive cases were reported, but generally there was inadequate laboratory capacity to test and confirm Vibrio. This meant that samples had to be transported to regional laboratories (long turn around time)
A second challenge was Weak coordination at the region and District level. A third was Inadequate and poor access to WASH. this included a Limited supply of clean and safe piped water in most of districts. Thus 52% of rural population get water from unimproved sources. (Shallow wells, river, lakes and few deep wells). In urban settings, water utilities can supply water not more than 50% and still chlorination is not regularly done. there was low latrine coverage especially in rural areas. About 73% of rural population use unimproved latrines and 13% with no latrines. A fourth challenge was the Misconceptions about cholera causation and some of the interventions.
In the process of addressing these challenges several Lesson were learnt. First, a well established surveillance system helped to in the early notification of cases and quick response. Strong coordination at all level of response is important to ensure the control of outbreak is done on time. Effective social mobilization and community engagement helped in the behaviour change towards the control of cholera. Finally Adequate and good access to WASH ensured the control of spread of cholera
Tanzania has put together a comprehensive cholera prevention program based on surveillance, coordination, water & sanitation and social mobilization. While cases have reduced, Tanzania is not relenting in implementing these key interventions.
Emergency &Epidemiology &Social/Cultural &Surveillance Bill Brieger | 17 Aug 2017
The Forest through the Trees: Themes in Social Production of Health
Recently Professor Ayodele S Jegede of the Faculty of Social Sciences, delivered the 419th Inaugural Lecture at the University of Ibadan, Ibadan, Nigeria, during the 2016/2017 academic session. Below Prof. Jegede shares an abstract of his lecture.

Prof Ayodele S Jegede
Knowledge of individual actor’s behaviour is a reflection of the society as tree to the forest. As forest produces large quantities of oxygen and takes in carbon dioxide, society produces the needed resources for human beings to survive through culture. This inter-dependence between man and the environment is summarised by the Yoruba adage which says: “irorun igi ni irorun eye” (meaning: a bird’s peace depends on the peace enjoyed by the tree which harbours it).
Nigeria, a country with a population of about 187 million and a life expectancy of 53 years, 54% of the populace are living below the poverty line with limited access to health care services physically and economically. Although universal health coverage is vital to the achievement of the Sustainable Development Goals (SDGs) cultural perception of disease aside from loss of economic and low purchasing power makes people to attribute their illnesses to spiritual cause and therefore seek alternative health care services. This influences resistance to public health interventions in some African communities resulting in suspicion and distrust between health educators and the public.

Strengthening Health Information Systems
For instance, response to childhood immunizable diseases, mental illness, malaria and HIV/AIDS reported in this lecture was driven by how people define the diseases. Their response did result in delay in seeking modern health care until alternative care sources proved ineffective. This confirms W.I. Thomas (1929: 572) postulation that, “If men define situations as real, they are real in their consequences”.
Our stakeholders’ engagement interventions strategies strengthened by knowledge of how people construct their life, socially and culturally, proved to be a potent vaccine for preventing strain relationship between health workers and clients. Since society consists of individuals who constitute the stakeholders conducting health researches as well as management of epidemics and treatment during epidemics and disease episodes require appropriate ethical behaviours.
This suggests that adequate knowledge of the society is inevitable since a tree does not make a forest which confirms Marx Weber’s Action Theory postulation that an act does not become social unless it involves two or more persons. It is, therefore, that government should establish National Disease Observatory System (NDOS) to document diseases by type, location and related local practices for training health care professionals, clinical practice and emergencies preparedness.
Note also that the lecture was featured in the New Nigerian Newspaper with an emphasis on establishing a national disease observatory. The Nigerian Tribune also featured the lecture stressing the importance of disease emergency preparedness.
Climate &Community &Development &Epidemiology &Malaria in Pregnancy &Mosquitoes &Surveillance &Urban &Zoonoses Bill Brieger | 11 Jul 2017
Population Health: Malaria, Monkeys and Mosquitoes
 On World Population Day (July 11) one often thinks of family planning. A wider view was proposed by resolution 45/216 of December 1990, of the United Nations General Assembly which encouraged observance of “World Population Day to enhance awareness of population issues, including their relations to the environment and development.”
On World Population Day (July 11) one often thinks of family planning. A wider view was proposed by resolution 45/216 of December 1990, of the United Nations General Assembly which encouraged observance of “World Population Day to enhance awareness of population issues, including their relations to the environment and development.”
A relationship still exists between family planning and malaria via preventing pregnancies in malaria endemic areas where the disease leads to anemia, death, low birth weight and stillbirth. Other population issues such as migration/mobility, border movement, and conflict/displacement influence exposure of populations to malaria, NTDs and their risks. Environmental concerns such as land/forest degradation, occupational exposure, population expansion (even into areas where populations of monkeys, bats or other sources of zoonotic disease transmission live), and climate warming in areas without prior malaria transmission expose more populati ons to mosquitoes and malaria.
ons to mosquitoes and malaria.
Ultimately the goal of eliminating malaria needs a population based focus. The recent WHO malaria elimination strategic guidance encourages examination of factors in defined population units that influence transmission or control.
Today public health advocates are using the term population health more. The University of Wisconsin Department of Population Health Sciences in its blog explained that “Population health is defined as the health outcomes of a group of individuals, including the distribution of such outcomes within the group.” World Population Day is a good time to consider how the transmission or prevention of malaria, or even neglected tropical diseases, is distributed in our countries, and which groups and communities within that population are most vulnerable.
World Population Day has room to consider many issues related to the health of populations whether it be reproductive health, communicable diseases or chronic diseases as well as the services to address these concerns.
Elimination &Surveillance &Vector Control Bill Brieger | 11 Apr 2017
A malaria elimination framework that includes high prevalence countries, too
When the Nigeria Malaria Control Program changes its name to Nigeria Malaria Elimination Program (NMEP) a few years ago, people wondered whether this was getting too far ahead of the situation in one of the highest burden malaria countries in the world. The recently released Framework for Malaria Elimination by the Global Malaria Program of WHO shows that all endemic countries can fit into the elimination process.

Recent Webinar by WHO’s Global Malaria Program stressed that all countries have a role in malaria elimination
The Framework stresses that, “Every country can accelerate progress towards elimination through evidence-based strategies, regardless of the current intensity of transmission and the malaria burden they may carry.” The Three pillars of the malaria elimination framework have room for high burden countries. Pillar 1 states that, “Ensure universal access to malaria prevention, diagnosis and treatment.”
First it is important to understand that the Framework defines malaria elimination as the cessation of indigenous mosquito-borne transmission of malaria throughout a country. The Framework also observes that even within countries there are diverse transmission areas. Some are not amenable to malaria transmission, while others may be amenable but do not experience transmission.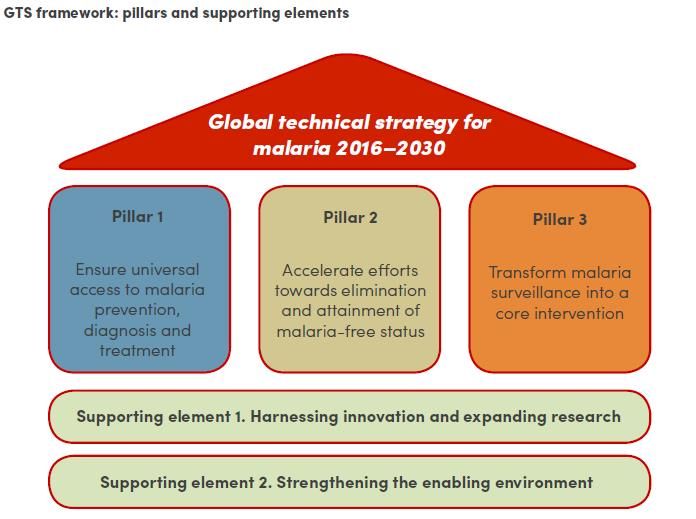
It is important to realize that malaria transmission in most countries is characterized by diversity and complexity. Areas where transmission is occurring range from very low transmission zones where hotspots erupt to high levels of ongoing transmission. Thus even high burden countries may have variation that require development of intervention packages tailored to the specific transmission setting.
This stratifi cation and development of appropriate intervention packages requires, “Excellent surveillance and response are the keys to achieving and maintaining malaria elimination; information systems must become increasingly ‘granular’ to allow identification, tracking, classification and response for all malaria cases (e.g. imported, introduced, indigenous).” This should lead to “subnational elimination targets as internal milestones.”
cation and development of appropriate intervention packages requires, “Excellent surveillance and response are the keys to achieving and maintaining malaria elimination; information systems must become increasingly ‘granular’ to allow identification, tracking, classification and response for all malaria cases (e.g. imported, introduced, indigenous).” This should lead to “subnational elimination targets as internal milestones.”
 For high burden countries key components of Pillar 1 is, “Vector control strategies, such as use of insecticide-treated mosquito nets (ITNs/LLINs) and indoor residual spraying (IRS), together with case management (prompt access to diagnosis and effective treatment) are critical for reducing malaria morbidity and mortality, and reducing malaria transmission.”
For high burden countries key components of Pillar 1 is, “Vector control strategies, such as use of insecticide-treated mosquito nets (ITNs/LLINs) and indoor residual spraying (IRS), together with case management (prompt access to diagnosis and effective treatment) are critical for reducing malaria morbidity and mortality, and reducing malaria transmission.”
Recommendations like ensuring political commitment, private sector involvement and establishment of an independent advisory committee are valuable at all stages of elimination. A challenge for high burden countries will be maintaining political commitment over many years. Early involvement of the private sector will boost coverage of major interventions. An independent advisory/monitoring group will help track data and progress.
It is important to put in place good monitoring systems to ensure that program coverage is well targeted, achieved and maintained. “Systematic tracking of programme actions over time, including budget allocations and adherence to standard operating procedures.” This enables accountability and enhances political commitment.
 Finally the Malaria Atlas Project has mapped most recent data, and as we can see Nigeria does have a variety of transmission settings. We know now that the decision of Nigeria’s malaria program to update its name was appropriate. Hopefully not only the NMEP but also the various state malaria programs will look at their malaria transmission strata and plan according toward elimination.
Finally the Malaria Atlas Project has mapped most recent data, and as we can see Nigeria does have a variety of transmission settings. We know now that the decision of Nigeria’s malaria program to update its name was appropriate. Hopefully not only the NMEP but also the various state malaria programs will look at their malaria transmission strata and plan according toward elimination.
Dengue &Mosquitoes &Surveillance &Urban Bill Brieger | 09 Jan 2017
Malaria, Dengue, Mosquitoes – evolving in the urban environment
As the world increasingly urbanizes, we need to address the role of urban ecosystems and the evolution of disease vectors and organisms. Marina Alberti and colleagues explained that …
“Recent studies show that cities might play a major role in contemporary evolution by accelerating phenotypic changes in wildlife, including animals, plants, fungi, and other organisms. Many studies of ecoevolutionary change have focused on anthropogenic drivers, but none of these studies has specifically examined the role that urbanization plays in ecoevolution or explicitly examined its mechanisms.”
 In their own study they looked at “five types of urban disturbances including habitat modifications, biotic interactions, habitat heterogeneity, novel disturbances, and social interactions.” The researchers learned that, “clear urban signal; rates of phenotypic change are greater in urbanizing systems compared with natural and nonurban anthropogenic systems.” They concluded that there is need to continually “uncover insights for maintaining key ecosystem functions upon which the sustainability of human well-being depends.”
In their own study they looked at “five types of urban disturbances including habitat modifications, biotic interactions, habitat heterogeneity, novel disturbances, and social interactions.” The researchers learned that, “clear urban signal; rates of phenotypic change are greater in urbanizing systems compared with natural and nonurban anthropogenic systems.” They concluded that there is need to continually “uncover insights for maintaining key ecosystem functions upon which the sustainability of human well-being depends.”
Of particular concern in the area of tropical health are the unique urban manifestations of diseases like yellow fever, dengue and malaria. Although Zika virus, for example, was first discovered in forests, it has adapted to an urban cycle involving humans and domestic mosquito vectors in tropical areas where dengue is endemic. Musso and Gubler in their review further explain that although there may be sylvatic cycles of Dengue, “Arboviruses such as DENV have adapted completely to humans and can be maintained in large tropical urban centers in a mosquito-human-mosquito transmission cycle that does not depend on nonhuman reservoirs.”
Weaver et al. note that Zika in spreading to Asia, “emerged on multiple occasions into urban transmission cycles involving Aedes (Stegomyia) spp. Mosquitoes.” In addition it can be hypothesized that phenotypic changes in Asian lineage ZIKV strains made rare disease outcomes such as congenital microcephaly and Guillain-Barré more common and visible.
 According to Estelle Martin and co-researchers, “Puerto Rico, a major metropolitan center in the Caribbean, has experienced increasingly larger and clinically more severe epidemics following the introduction of all four dengue serotypes.” They found that Dengue serotype 4 replaced earlier strains and that “this epidemic strain progressed rapidly, suggesting that the epidemic strain was more fit, and that natural selection may have acted on these mutations to drive them to fixation.”
According to Estelle Martin and co-researchers, “Puerto Rico, a major metropolitan center in the Caribbean, has experienced increasingly larger and clinically more severe epidemics following the introduction of all four dengue serotypes.” They found that Dengue serotype 4 replaced earlier strains and that “this epidemic strain progressed rapidly, suggesting that the epidemic strain was more fit, and that natural selection may have acted on these mutations to drive them to fixation.”
In addition to virus evolution, mosquito changes have been documented by Caroline Louise and colleagues in “One of the world’s largest urban agglomerations infested by Ae. aegypti … the Brazilian megalopolis of Sao Paulo.” They detected microevolution despite a short observational period and stress the implications of the “rapid evolution and high polymorphism of this mosquito vector on the efficacy of control methods.”
“The adaptation of malaria vectors to urban areas is becoming a serious challenge for malaria control,” is a major concern of Antonio-Nkondjio and co-workers. They found, “rapid evolution of pyrethroid resistance in vector populations from the cities of Douala and Yaoundé,” Members of this team also learned that the M form of Anopheles gambiae predominated in the centre of urban agglomerates in Cameroon. Previously it was known that larval habitats polluted with decaying organic matter as found in densely populated urban agglomerates, were unsuitable for Anopheles gambiae. The recent study showed that the “M form showed greater tolerance to ammonia (arising from organic matter) compared to the S form. This trait may be part of the physiological machinery allowing forest populations of the M form to colonize polluted larval habitats.”
The evolutionary response of vectors and disease organisms to urban environments needs continued monitoring. Urban disease control and elimination efforts must adapt to such adaptations in the disease process.
Diagnosis &Surveillance Bill Brieger | 14 Nov 2016
Towards Malaria Pre-Elimination in Rwanda: Active Case Investigation in a Low Endemic District
A poster entitled “Towards Malaria Pre-Elimination in Rwanda: Active Case Investigation in a Low Endemic District” was presented by members of Jhpiego’s Rwanda Team and colleagues:
Noella Umulisa, Angelique Mugirente, Veneranda Umubyeyi, Beata Mukarugwiro, Stephen Mutwiwa, Jean Pierre Habimana, and Corrine Karema, at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
 Rwanda has seen an increase in malaria cases recently with an increase from 514,173 cases in 2012 to 1,957,402 cases in 2015. This change can be attributed to an increase in temperature, rainfall, and resistance to insecticides.
Rwanda has seen an increase in malaria cases recently with an increase from 514,173 cases in 2012 to 1,957,402 cases in 2015. This change can be attributed to an increase in temperature, rainfall, and resistance to insecticides.
Despite this setback, Rwanda is aiming to reach the pre-elimination phase by 2018. In January 2015, 11 health facilities in Rubavu, a low endemic district, started implementing reactive active case detection after training 55 health care providers and 11 lab technicians on the topic. This strategy involves screening and treating individuals living in close proximity to passively detected cases, also known as index cases. Index cases can be used to identify population groups that are sources of infection.
 From January 2015 to December 2015, 16,434 cases of Malaria were detected and treated at 11 health facilities in Rubavu District. Among these cases, 2,917(17.8%) index cases were investigated and 4,943 individuals (between 1 and 2 contacts for each index case) living in proximity of index cases were tested using rapid diagnostic tests by health care providers. Of these, 508 (10.3%) tested positive for malaria and were treated according to national guidelines.
From January 2015 to December 2015, 16,434 cases of Malaria were detected and treated at 11 health facilities in Rubavu District. Among these cases, 2,917(17.8%) index cases were investigated and 4,943 individuals (between 1 and 2 contacts for each index case) living in proximity of index cases were tested using rapid diagnostic tests by health care providers. Of these, 508 (10.3%) tested positive for malaria and were treated according to national guidelines.
These data shows that the number of investigated cases is still lower than the national guidelines of screening 5 individuals residing between 100 to 500 meters of every confirmed case. This low rate could be due to the increase of malaria cases in Rwanda which has placed a burden on health care providers and health facilities in areas like Rubavu which used to be low endemic malaria areas. Additionally, data gathered through supervision activities has indicated a need for additional training on screening investigations in order to adhere to national guidelines and conduct the investigations more efficiently.
Active case investigation could be improved by training and involving more health care providers such as community health workers who could reduce the burden on health center staff. The additional support for case investigation activities and improved training can help to achieve higher coverage of individuals located near index cases.
Borders &Elimination &Resistance &Surveillance Bill Brieger | 29 Sep 2015
Epidemiology of Resurgent Malaria in Eastern Zimbabwe: Risk Factors, Spatio-Temporal Patterns and Prospects for Regaining Malaria Control
Mufaro Kanyangarara and her PhD thesis adviser, Luke Mullany, of the Johns Hopkins Bloomberg School of Public Health Department of International Health, have been looking into the challenges of controlling and eventually eliminating malaria in a multi-country context in southern Africa. We are sharing abstracts from her pioneering work. The first seen below provides an overview of the three components of the study.
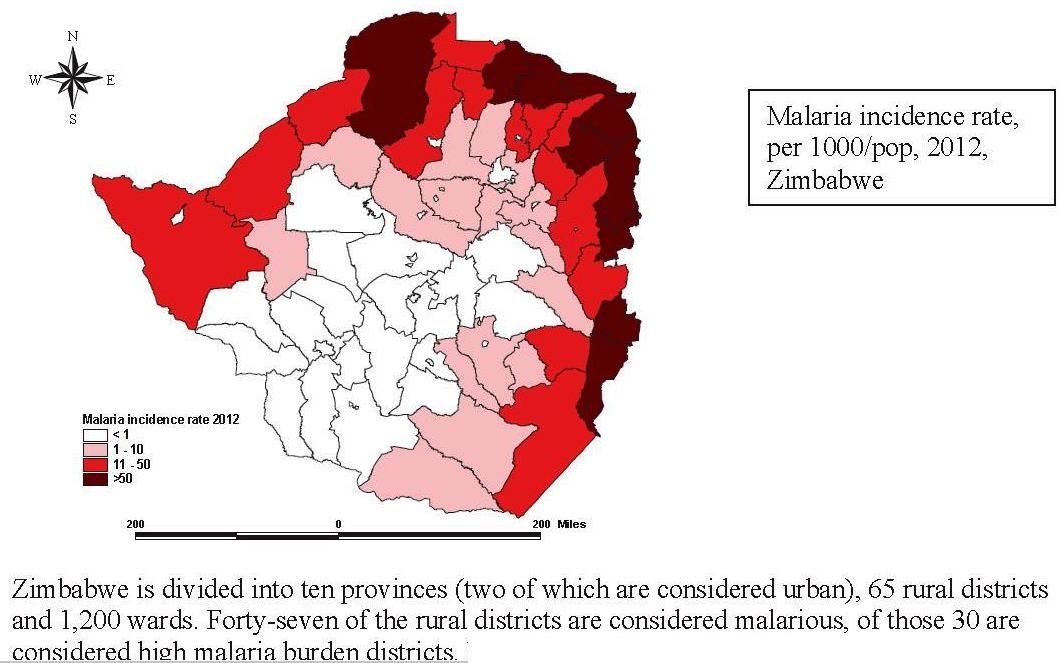 Despite recent reductions in malaria morbidity and mortality due to the scale up of malaria interventions, malaria remains a public health problem in sub-Saharan Africa, especially among children under five years of age, pregnant women and people living with HIV/AIDS. A recent resurgence in malaria, in areas where malaria control was previously successful, has brought to the forefront the importance of research to understand the epidemiology of malaria and the effectiveness of malaria control efforts in resurgent settings. Using cross-sectional surveys, routine data from health-facility based surveillance and freely available remotely sensed environmental data, this research examined the distribution of malaria and the impact of vector control in Mutasa, a rural district in Zimbabwe characterized by resurgent malaria.
Despite recent reductions in malaria morbidity and mortality due to the scale up of malaria interventions, malaria remains a public health problem in sub-Saharan Africa, especially among children under five years of age, pregnant women and people living with HIV/AIDS. A recent resurgence in malaria, in areas where malaria control was previously successful, has brought to the forefront the importance of research to understand the epidemiology of malaria and the effectiveness of malaria control efforts in resurgent settings. Using cross-sectional surveys, routine data from health-facility based surveillance and freely available remotely sensed environmental data, this research examined the distribution of malaria and the impact of vector control in Mutasa, a rural district in Zimbabwe characterized by resurgent malaria.
Firstly, individual- and household level factors independently associated with individual malaria risk were identified using multilevel logistic regression models based on data from cross-sectional surveys conducted between October 2012 and September 2014. Secondly, geostatistical methods and remotely sensed environmental data were used to model the spatial and seasonal distribution of household malaria risk; then develop seasonal malaria risk maps with corresponding maps of the prediction uncertainty. Lastly, an evaluation of the effect of introducing an organophosphate for indoor residual spraying was conducted using routine health facility data covering 24 months before and 6 months after the campaign.
The results of multilevel model suggested that malaria risk was significantly higher among individuals who were younger than 25 years, did not sleep under a bed net, and lived close to the Zimbabwe-Mozambique border. The spatial risk maps depicted relatively increased risk of finding a positive household in low-lying areas along the Mozambique border during the rainy season. Lastly, the introduction of organophosphates to this pyretheroid resistant area resulted in a significant reduction in malaria incidence following spraying. These findings elucidate the heterogeneous distribution of malaria, identify risk factors driving malaria transmission and assess the quantitative impact of switching insecticide classes on health outcomes. Collectively, the findings provide evidence to guide country-specific decision making for regaining malaria control and underscore the need for strong between-country initiatives to curb malaria in Mutasa District and elsewhere.