Cholera &Surveillance &water Bill Brieger | 19 Dec 2017 07:51 am
Comprehensive Cholera Prevention and Control: Lessons Learnt from the United Republic of Tanzania
Dafrossa Lyimo of the Ministry of Health, Tanzania presented Tanzania’s experience in preventing and controlling cholera at the 4th African Regional Immunization Technical Advisory Group (RITAG) meeting in Johannesburg, 5-8 December 2017. Those experiences are summarized below.
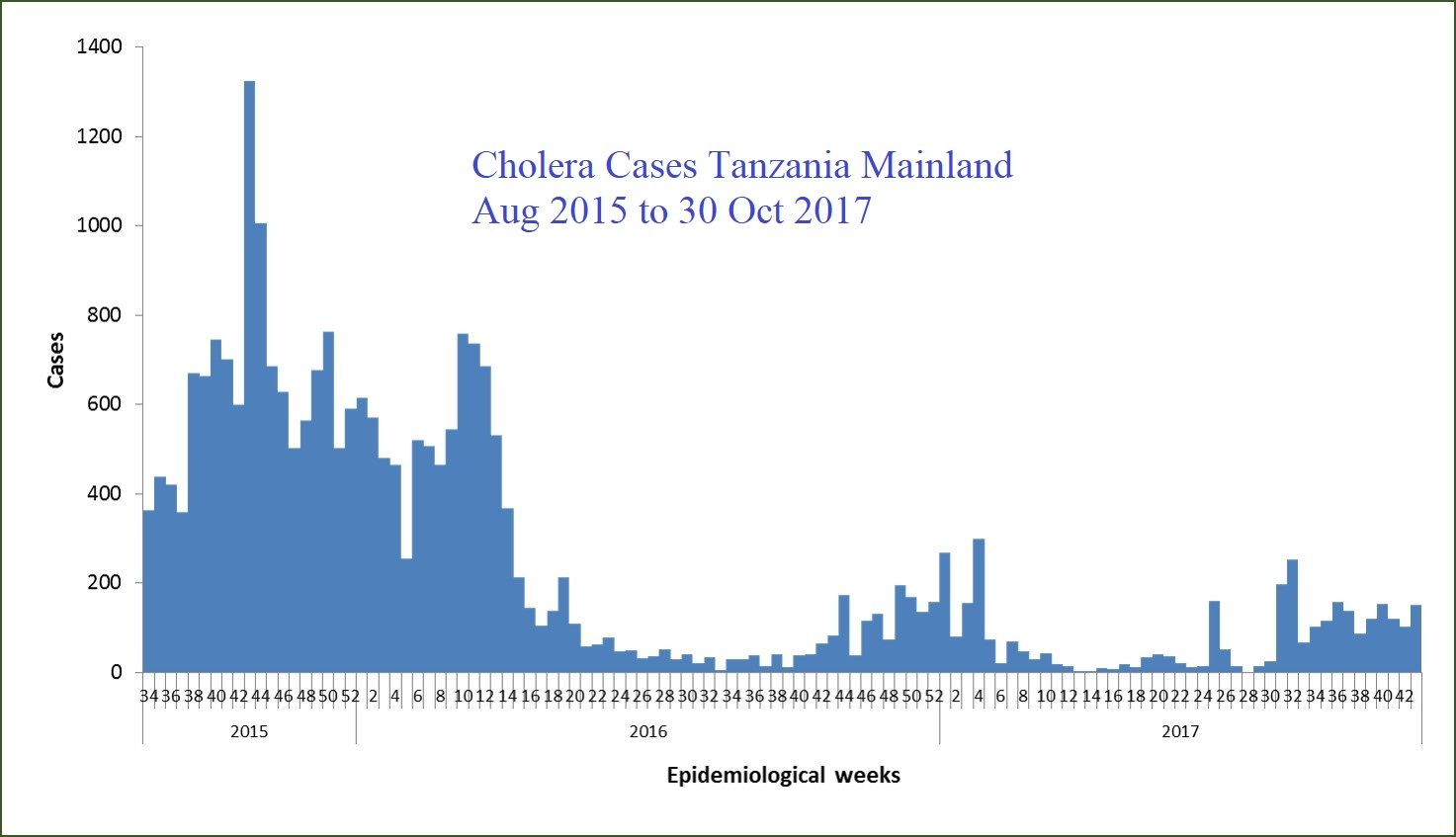
Cholera outbreak in Tanzania started with the index case detected in Dar es Salaam Region on 6 August 2015. The World Health Organization was notified by Ministry of Health on 15 August 2015. By 31 December 2015 the outbreak spread to 22 out of 26 regions in Tanzania Mainland. Zanzibar started reporting cholera cases on 20 September 2015 from Urban West District in Unguja Island. By December 2015, the outbreak spread to all 10 districts of Pemba and Unguja.
 Cumulative cases on the Tanzania Mainland were 12 619 cases with 199 deaths (CFR 1.57%) in 2015, 11 360 cases with 172 deaths (CFR 1.5%) in 2016, and up through Nov 2017, 3 615 cases with 61 deaths (CFR 1.7%). Likewise the Cumulative cases in Zanzibar were 1 143 cases with 15 deaths (1.31%) in 2015, 3 187 cases with 53 deaths (CFR 1.66%) in 2016 and as of Nov 2017, 358 cases with 4 deaths (CFR 1.12%). The last case reported 11 July 2017
Cumulative cases on the Tanzania Mainland were 12 619 cases with 199 deaths (CFR 1.57%) in 2015, 11 360 cases with 172 deaths (CFR 1.5%) in 2016, and up through Nov 2017, 3 615 cases with 61 deaths (CFR 1.7%). Likewise the Cumulative cases in Zanzibar were 1 143 cases with 15 deaths (1.31%) in 2015, 3 187 cases with 53 deaths (CFR 1.66%) in 2016 and as of Nov 2017, 358 cases with 4 deaths (CFR 1.12%). The last case reported 11 July 2017
Best practices for controlling cholera in the country fall in four domains. In the area od Coordination Tanzania established a Public Health Emergency Operations Centre (PHEOC) in the Ministry of Health. To support this the Ministry appointed an Incident Manager, Deputy Incident Manager, and a PHEOC Manager for the cholera outbreak response. The National Task force Team was established with a wider composition which meeting every Friday discussing issues and giving way forward. National Rapid Response Teams were trained. these teams worked based on national response guidelines which were developed and distributed to all districts.
 In the domain of Surveillance, the Ministry initiated a Daily Situation Report (SITREP) for sharing a daily cholera status in the regions and districts , on going interventions and gaps. This group conducted twice a country wide data validation/verification of the reported cases in 17 regions, which also confirmed under-reporting of cases. A Cholera reporting line list register was designed and printed in booklets and distributed to 26 regions in the Tanzania Mainland, to standardize reporting from districts and regions.
In the domain of Surveillance, the Ministry initiated a Daily Situation Report (SITREP) for sharing a daily cholera status in the regions and districts , on going interventions and gaps. This group conducted twice a country wide data validation/verification of the reported cases in 17 regions, which also confirmed under-reporting of cases. A Cholera reporting line list register was designed and printed in booklets and distributed to 26 regions in the Tanzania Mainland, to standardize reporting from districts and regions.
 The third domain consisted of Water Sanitation and Hygiene interventions. The country distributed 21,600,000 aqua tablets of water guards in 514,285 households. Also distributed were 50 drums 45kg each of 70% High Test Hypochlorite to 83 district water authorities for bulk chlorination. Twenty hand pump boreholes were installed in hotspot villages of Mara and Mwanza regions, thereby Improving the access to clean and safe water. One hundred HACH chlorine testers were distributed for monitoring free residue chlorine in cholera reporting districts.
The third domain consisted of Water Sanitation and Hygiene interventions. The country distributed 21,600,000 aqua tablets of water guards in 514,285 households. Also distributed were 50 drums 45kg each of 70% High Test Hypochlorite to 83 district water authorities for bulk chlorination. Twenty hand pump boreholes were installed in hotspot villages of Mara and Mwanza regions, thereby Improving the access to clean and safe water. One hundred HACH chlorine testers were distributed for monitoring free residue chlorine in cholera reporting districts.
Social Mobilization was the fourth domain. Cholera leaflets and fliers were designed and distributed in reporting districts. Cholera messages were developed and aired through community media and mobile phone messaging. Community engagement and owning cholera interventions was undertaken using the community social networks and peer groups who focused on Hand washing, Use of treated water, and Use of toilets behaviors.
 Cholera control and prevention efforts addressed various Challenges
Cholera control and prevention efforts addressed various Challenges
in Tanzania. one concern was a weak surveillance system starting at the district level in several districts. Lack of reporting cholera cases, under-reporting and late reporting occurred. In some districts that had laboratory capacity, only positive cases were reported, but generally there was inadequate laboratory capacity to test and confirm Vibrio. This meant that samples had to be transported to regional laboratories (long turn around time)
A second challenge was Weak coordination at the region and District level. A third was Inadequate and poor access to WASH. this included a Limited supply of clean and safe piped water in most of districts. Thus 52% of rural population get water from unimproved sources. (Shallow wells, river, lakes and few deep wells). In urban settings, water utilities can supply water not more than 50% and still chlorination is not regularly done. there was low latrine coverage especially in rural areas. About 73% of rural population use unimproved latrines and 13% with no latrines. A fourth challenge was the Misconceptions about cholera causation and some of the interventions.
In the process of addressing these challenges several Lesson were learnt. First, a well established surveillance system helped to in the early notification of cases and quick response. Strong coordination at all level of response is important to ensure the control of outbreak is done on time. Effective social mobilization and community engagement helped in the behaviour change towards the control of cholera. Finally Adequate and good access to WASH ensured the control of spread of cholera
Tanzania has put together a comprehensive cholera prevention program based on surveillance, coordination, water & sanitation and social mobilization. While cases have reduced, Tanzania is not relenting in implementing these key interventions.
on 19 Dec 2017 at 3:51 pm 1.Comprehensive Cholera Prevention and Control: Lessons Learnt from the United Republic of… said …
[…] Link: Comprehensive Cholera Prevention and Control: Lessons Learnt from the United Republic of… […]