Borders &Elimination &Indoor Residual Spraying &Monitoring &Surveillance &Vector Control Bill Brieger | 13 Jun 2015
Moving toward Malaria Elimination in Botswana
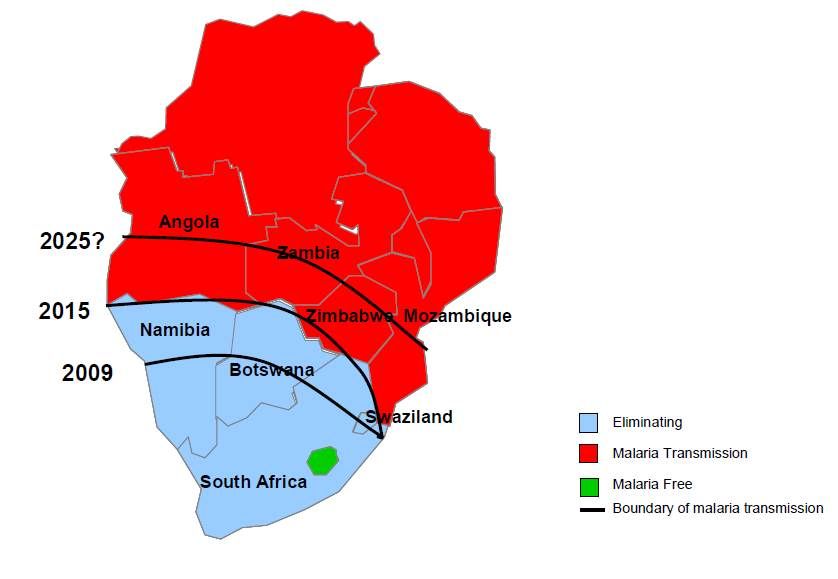 The just concluded 2015 Global Health Conference in Botswana, hosted by Boitekanelo College at Gaborone International Convention Centre on 11-12 June provided us a good opportunity to examine how Botswana is moving toward malaria elimination. Botswana is one of the four front line malaria elimination countries in the Southern African Development Community and offers lessons for other countries in the region. Combined with the 4 neighboring countries to the north, they are known collectively as the “Elimination Eight”.
The just concluded 2015 Global Health Conference in Botswana, hosted by Boitekanelo College at Gaborone International Convention Centre on 11-12 June provided us a good opportunity to examine how Botswana is moving toward malaria elimination. Botswana is one of the four front line malaria elimination countries in the Southern African Development Community and offers lessons for other countries in the region. Combined with the 4 neighboring countries to the north, they are known collectively as the “Elimination Eight”.
The malaria elimination countries are characterised by low leves of transmission in focal areas of the country, often in seasonal or epidemic form. The pathway to malaria elimination requires that a country or defined areas in a country reach a slide positivity rates during peak malaria season of < 5%.
 Chihanga Simon et al. provide us a good outline of 60+ years of Botswana’s movements along the pathway beginning with indoor residual spraying (IRS) in the 1950s. Since then the country has expanded vector control to strengthened case management and surveillance. Particular recent milestones include –
Chihanga Simon et al. provide us a good outline of 60+ years of Botswana’s movements along the pathway beginning with indoor residual spraying (IRS) in the 1950s. Since then the country has expanded vector control to strengthened case management and surveillance. Particular recent milestones include –
- 2009: Malaria elimination policy required all cases to be tested before treatment malaria elimination target set for 2015
- 2010: Malaria Strategic Plan 2010–15 using recommendations from programme review of 2009; free LLINs
- 2012: Case-based surveillance introduced
The national malaria elimination strategy includes the following: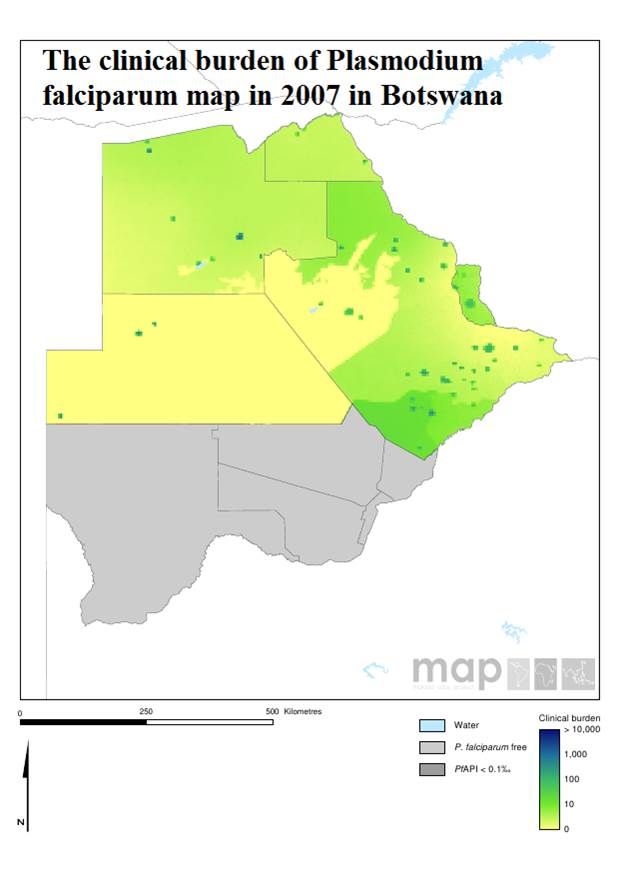
- Focus distribution LLIN & IRS in all transmission foci/high risk districts
- Detect all malaria infections through appropriate diagnostic methods and provide effective treatment
- Develop a robust information system for tracking of progress and decision making
- Build capacity at all levels for malaria elimination
Botswana like other malaria endemic countries works with the Roll Back Malaria Partnership to compile an annual road map that identifies progress made and areas for improvement. The 2015 Road Map shows that –
- 116,229 LLINs distributed during campaigns in order to maintain universal coverage in the 6 high risk districts
- 200,721 IRS Operational Target structures sprayed
- 2,183,238 RDTs distributed and 9,876 microscopes distributed
- While M&E, Behavior Change, and Program Management Capacity activities are underway
 Finally the African Leaders Malaria Alliance (ALMA) provides quarterly scorecards on each member. Botswana is making a major financial commitment to its malaria elimination commodity and policy needs. There is still need to sustain high levels of IRS coverage in designated areas.
Finally the African Leaders Malaria Alliance (ALMA) provides quarterly scorecards on each member. Botswana is making a major financial commitment to its malaria elimination commodity and policy needs. There is still need to sustain high levels of IRS coverage in designated areas.
Monitoring and evaluation is crucial to malaria elimination. Botswana has a detailed M&E plan that includes a geo-referenced surveillance system, GIS and malaria database training for 60 health care workers, traininf for at least 80% of health workers on Case Based Surveillance in 29 districts, and regular data analysis and feedback.
M&E activities also involve supervision visits for mapping of cases, foci and interventions, bi-annual malaria case management audits, enhanced diagnostics through PCR and LAMP as well as Knowledge, Attitudes, Behaviour, and Practice surveys.
Malaria elimination activities are not simple. Just because cases drop, our job is easier. Botswana, like its neighbors in the ‘Elimination Eight’ is putting in place the interventions and resources needed to see malaria really come to an end in the country. Keep up the good work!
IPTp &ITNs &Monitoring Bill Brieger | 27 Apr 2015
Invest in Using Preventive Services: an Update from the 2014-15 Uganda Malaria Information Survey
 The Demographic and Health Survey people have just released the preliminary MIS results for Uganda. From the viewpoint to the Millennium Development Goals (MDGs), there are cautiously positive signs.
The Demographic and Health Survey people have just released the preliminary MIS results for Uganda. From the viewpoint to the Millennium Development Goals (MDGs), there are cautiously positive signs.
Insecticide treated bednet ownership by households has reached 90%. Equity appears to have been achieved with the households in the lowest, second and third wealth quintiles registering 92%, 94% and 93% ownership. The highest and next highest quintiles had 85% and 88% ownership respectively. Those in the higher wealth quintiles often have better quality housing that of itself offers preventive benefits.
An interesting number is that over 86% of households obtained their nets through campaigns. It appears that the catch up phase of net distribution is repeating itself and the more sustainable keep up phase where nets are provided through routine services has not taken effect.
Household ownership of at least one net translates into use by only 69% of residents generally, and still only 74% in homes that actually own a net. Net use by ‘vulnerable groups’ was a bit better: 74% for children below five years of age and 75& for pregnant women. Thus we can see that household ownership does not guarantee that we meet the 2010 target of 80% coverage/use.
We have moved from recommending two doses of sulfadoxine-pyrimethamine as intermittent preventive treatment for malaria in pregnancy to three or more. The MIS does not report on increased doses but even for two contacts, only 25% of recently pregnant women in Uganda were covered.
The results show that malaria prevention is still an elusive goal. Thirty per cent of children given malaria rapid diagnostic tests during the survey had malaria parasite antigens. We must invest more in ensuring that preventive interventions are routinely available and are actually used before our attention is diverted from the MDGs to the SDGs.
IPTp &ITNs &Monitoring &Treatment Bill Brieger | 07 Apr 2015
Highlights from Malawi’s 2014 Malaria Information Survey
Two major forms of malaria data collection help inform national malaria control programs and their supporters about progress and help focus continued resources and interventions. Routine national health information tells us about program implementation on a regular basis. National surveys give us a point-in-time picture of coverage. For the latter, Malawi has been fortunate in recent times to have conducted Malaria Information Surveys every two years.
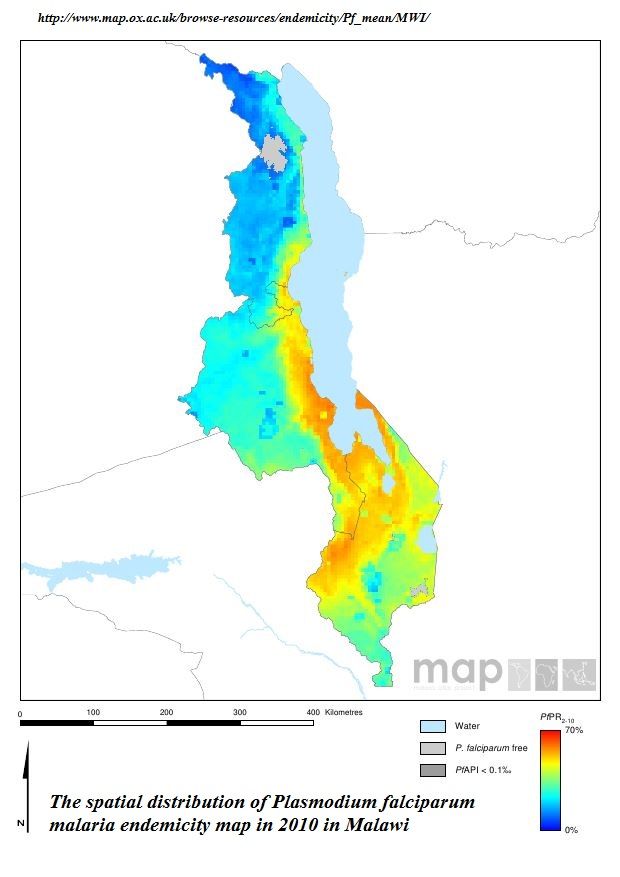 Malawi continues to have endemic malaria as documented by the MAP project in the attached graphic. While some of its neighbors in southern Africa are moving toward elimination, Malawi still experiences prevalence (as measured by rapid diagnostic test) in children below five years of age of 43%, 28% and 33% in 2010, 2012 and 2014 respectively.
Malawi continues to have endemic malaria as documented by the MAP project in the attached graphic. While some of its neighbors in southern Africa are moving toward elimination, Malawi still experiences prevalence (as measured by rapid diagnostic test) in children below five years of age of 43%, 28% and 33% in 2010, 2012 and 2014 respectively.
In the chart below we can see that malaria preventive measures have varied in coverage over the three survey periods and may be said to be on a very slightly upward trend. The Roll Back Malaria target of 80% coverage by 2010 and the US President’s Malaria Initiative target of 85% are still illusive.
In fact, simply having an ITN in the home is no guarantee that people will use it. Overall in 2014 72% of people living in a house with a net slept under one the night before the survey. The rate of use was better for children below five years of age (87%) and pregnant women (85%), but a gap remains.
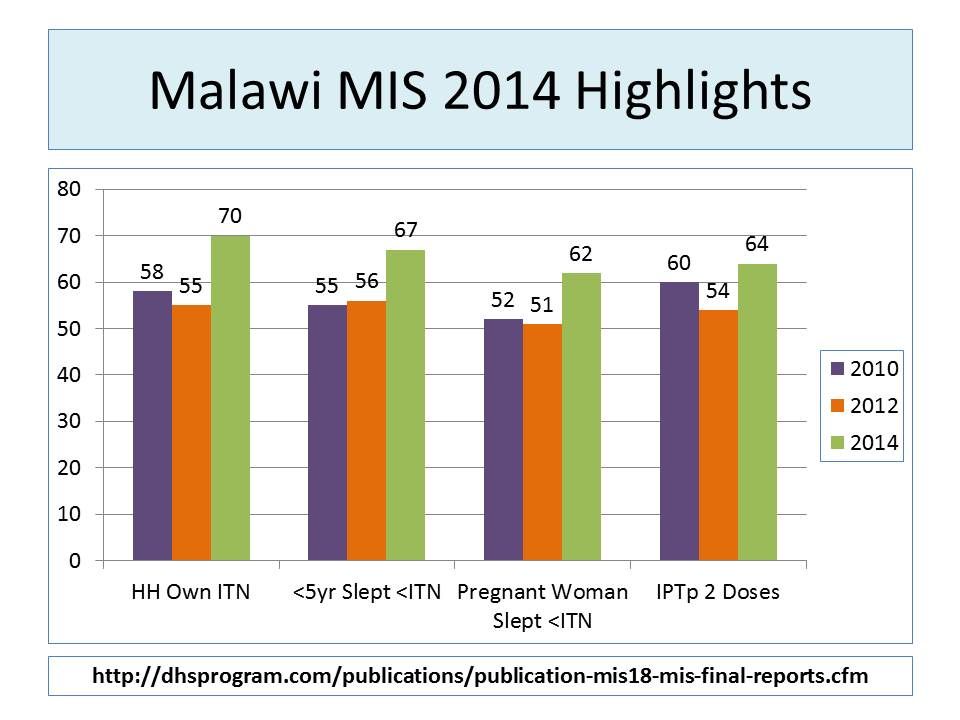 Overall coverage for two doses of sulphadoxine-pyrimethamine (SP) for intermittent preventive treatment in pregnancy (IPTp) remains low. Now that WHO is recommending IPTp with SP during each antenatal care visit after 13 weeks, we are aiming for 3, 4 or more doses. In 2014 89% pregnant women in Malawi received one dose, 63% received two and 12% received three.
Overall coverage for two doses of sulphadoxine-pyrimethamine (SP) for intermittent preventive treatment in pregnancy (IPTp) remains low. Now that WHO is recommending IPTp with SP during each antenatal care visit after 13 weeks, we are aiming for 3, 4 or more doses. In 2014 89% pregnant women in Malawi received one dose, 63% received two and 12% received three.
Malaria treatment for febrile children was the indicator with the best performance (not counting the fact that treatment was not always preceded by a diagnostic test). Most (93%) of children took an artemisinin-based combination therapy (ACT) drug, and 74% took it within a day of fever onset.
The 2014 MIS provides more detailed breakdown by region and socio-economic group, which should be helpful for planning. The major take home message though is that five years after the RBM target dates, many countries, Malawi included, have not been able to scale up and sustain the high intervention coverage needed to bring down mortality and guide us on the pathway to malaria elimination.
As the 2015 Millennium Development Goals are being replaced with a broader development agenda, we hope that malaria will not become a neglected tropical disease again. Actually using data from the MIS to take timely decisions by national programs and donors is essential to keep us on the path.
Health Systems &Human Resources &IPTp &Malaria in Pregnancy &Monitoring Bill Brieger | 03 Nov 2014
Jhpiego at ASTMH: Performance Quality Improvement for IPTp in Kenya
Monday afternoon (3 October 2014) at the American Society for Tropical Medicine and Hygiene Annual Meeting in New Orleans, Jhpiego and USAID/PMI are sponsoring a panel on “Integrating and Innovating: Strengthening Care for Mothers and Children with Infectious Diseases.” If you are at the meeting please attend to learn more about our Malaria activities in Kenya.
 One of the panel presentations is “Performance Quality Improvement Lending to Corrected Documented Outcomes for Intermittent Preventive Treatment in Kenya,” by Jhpiego staff Muthoni Kariuki, Augustine Ngindu Isaac Malonza, and Sanyu Kigondu, who are working with USAID’s Maternal & Child Health Integrated Project (MCHIP).
One of the panel presentations is “Performance Quality Improvement Lending to Corrected Documented Outcomes for Intermittent Preventive Treatment in Kenya,” by Jhpiego staff Muthoni Kariuki, Augustine Ngindu Isaac Malonza, and Sanyu Kigondu, who are working with USAID’s Maternal & Child Health Integrated Project (MCHIP).
According to Malaria policy in Kenya all pregnant women in malaria endemic areas receive free intermittent preventive treatment with SP have access to free malaria diagnosis and treatment when presenting with fever have access to LLINs (National Malaria Strategy (NMS) 2009–2017).
By 2013 80% of people living in malaria risk areas should be using appropriate malaria preventive interventions. Intermittent Preventive Treatment of malaria in pregnancy using Sulfadoxine Pyrimethamine (IPTp-SP) intervention is recommended for use in malaria endemic region.
 MCHIP broadly implemented Capacity Development and service delivery and improvement interventions that also had impact on the delivery of malaria in pregnancy services through collaboration with the Ministry of Health divisions/units at national level: (malaria, reproductive health, community health).
MCHIP broadly implemented Capacity Development and service delivery and improvement interventions that also had impact on the delivery of malaria in pregnancy services through collaboration with the Ministry of Health divisions/units at national level: (malaria, reproductive health, community health).
At county level scale up provision of IPTp at facility level took place in 14 malaria endemic counties. This included 8 counties in the lake endemic region including Bondo sub-county (the MCHIP model sub-county) and 6 in the coastal endemic region.
Quality Improvement through Performance Quality Improvement (PQI) process was instituted to enhance service delivery. The MCHIP era in Bondo Strengthened ANC Services using the following:
- Development of MIP Standards-Based Management and Recognition (SBM-R) standards
- Orientation of facility in-charges, supervisors and service providers on the standards
- Monitoring of IPTp uptake using DHIS2 data
- Feedback to facility in-charges and supervisors on DHIS2 findings
- Collection of ANC data from ANC registers (2011-2013)
- Feedback to facility in-charges and supervisors on ANC data
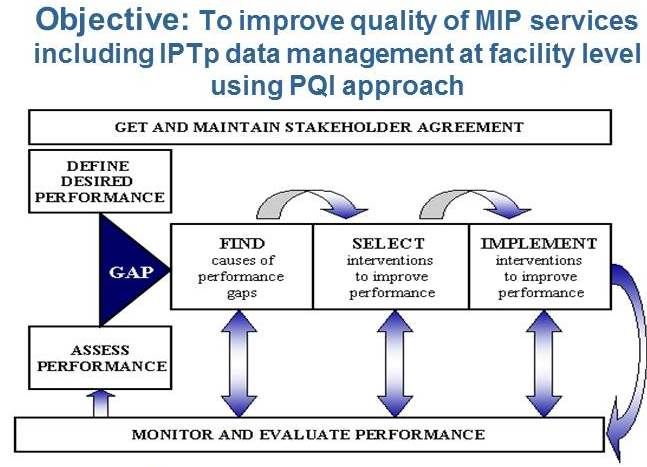
Quality improvement in the malaria in pregnancy component was undertaken with the objective to improve quality of MIP services including IPTp data management at facility level using PQI approach. An Example of a MIP SBM-R standard is seen below.
 In-service training focused on orientation of facility in-charges on PQI who then continued orientation at Facility Level. Overall we oriented 1200 facility in-charges and 100 supervisors on the standards. Facility in-charges cascaded orientation to 2,441 service providers.
In-service training focused on orientation of facility in-charges on PQI who then continued orientation at Facility Level. Overall we oriented 1200 facility in-charges and 100 supervisors on the standards. Facility in-charges cascaded orientation to 2,441 service providers.
 We then analysed ANC data from DHIS (2011-2013) indicated proportion of pregnant women receiving IPTp2 was higher than IPTp1 (IPTp2+ doses reported as IPTp2 dose). We helped improve reporting by service providers not oriented on use of the ANC register in order to reduce data errors.
We then analysed ANC data from DHIS (2011-2013) indicated proportion of pregnant women receiving IPTp2 was higher than IPTp1 (IPTp2+ doses reported as IPTp2 dose). We helped improve reporting by service providers not oriented on use of the ANC register in order to reduce data errors.
In conclusion, PQI is a best practice in provision of MIP services. Standardization of knowledge among service providers is essential in provision of quality MIP services. Development of facility in-charges as mentors in the facility to ensure continued orientation of new service providers.
Use of appropriate monitoring tools is necessary to assist in assessment of quality of services provided including data management. Feedback to service providers is one of the performance rewards and encourages participation in knowledge acquisition
Monitoring Bill Brieger | 17 Jul 2014
Improving the Quality of Malaria Data in Burkina Faso
Jhpiego and partners have been implementing USAID’s Improving Malaria Care (IMC) project in Burkina Faso for the past 9 months. In the paragraphs below, the team in Ouagadougou has reported their experiences in improving the quality of malaria data reported from the district level. Good quality data are needed to identify challenges and successes and make decisions for future malaria programming
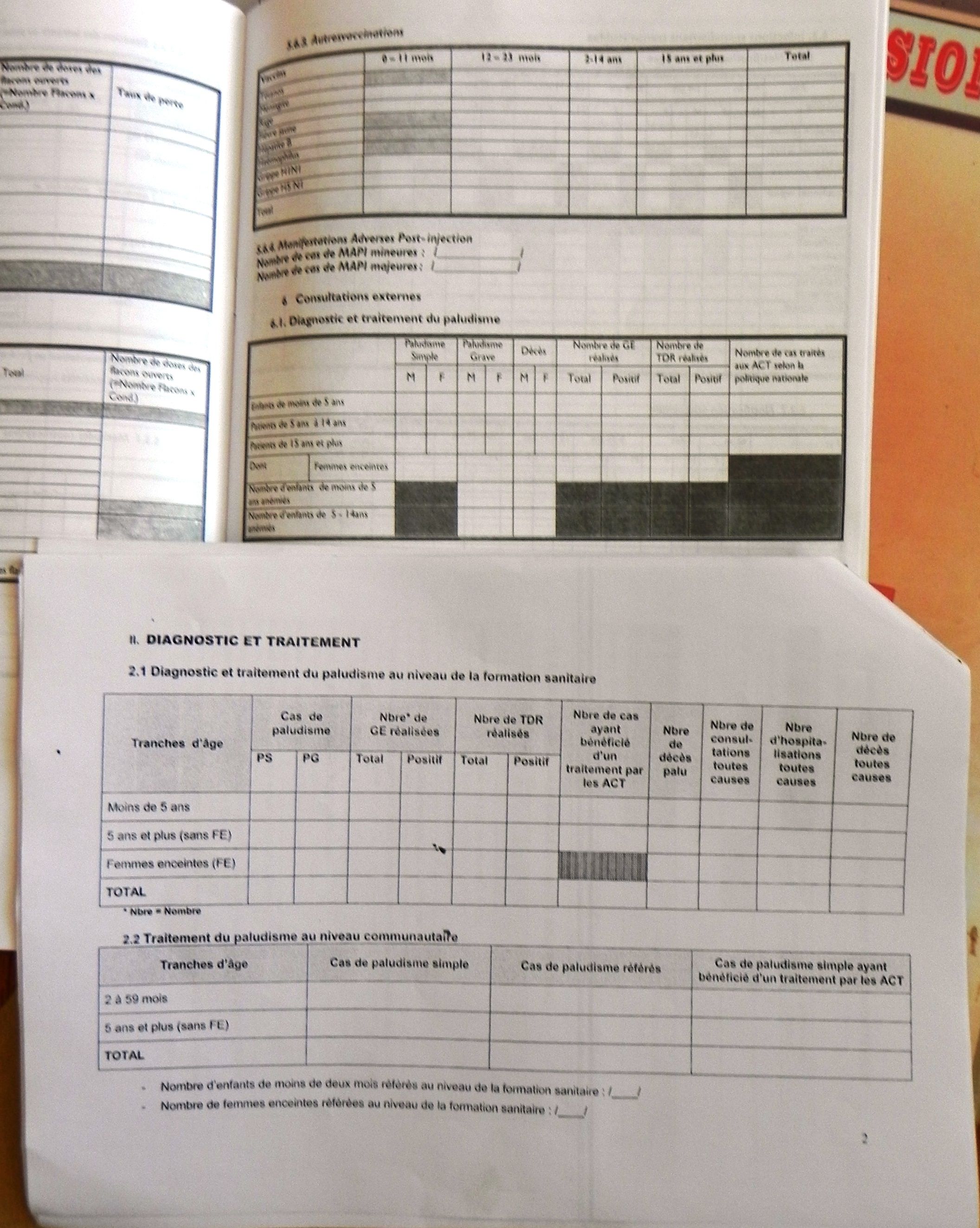 IMC involves data collectors (Healthcare providers) directly in the data validation process. Previously, the malaria data validation was supported by the Global Funds and was done at the Regional level. The new approach proposed by IMC is to organize malaria data validation at district level where the healthcare providers who continuously collect data, can participate in the data validation meetings.
IMC involves data collectors (Healthcare providers) directly in the data validation process. Previously, the malaria data validation was supported by the Global Funds and was done at the Regional level. The new approach proposed by IMC is to organize malaria data validation at district level where the healthcare providers who continuously collect data, can participate in the data validation meetings.
The pilot phase was conducted in the first 20 supported Health Districts in April (14th – 18th). In total, 520 healthcare providers attended the data validation meetings across 20 Health Districts. The most important lessons learnt are following:
- The involvement of the primary data collectors (Healthcare providers) in this activity reinforced their capacity to improve data quality;
- The correction of the mistakes made during these meeting have been integrated in the national database (BD_Malaria);
- This was another opportunity to explain the key indicators of malaria and how to control the data quality inside of the Health Facility;
- Based on the quantity of the mistakes noted during these data validation meetings in only 20 Health Districts (20 of 63 HD), we can affirm that these are some important data quality issues.
 Dr Kam Semon, District Medical Officer of Banfora Health District, after the Data validation workshop shared his views of the experience.
Dr Kam Semon, District Medical Officer of Banfora Health District, after the Data validation workshop shared his views of the experience.
“Firstly, allow me to thank Jhpiego for his permanent assistance and innovation regarding healthcare management. I have appreciated the new approach developed by Jhpiego to ensure data quality. During this meeting I have noted that they are lot of mistakes in the data we used to plan and to make decision.
“I have noted that the Data manager at District level and healthcare providers (who collect routine data) have to work very closely to improve and ensure data quality. That means we have to more involve the Data Manager of District in the regular supervision visits. […] I promised you to use the new approach for all health data validation.
“I will discuss with my team, to include the data validation using that new approach in our quarterly health management meeting. I would like to thank Jhpiego once again. I also thank USAID for his financial support to the IMC project. “
Health Information &Monitoring Bill Brieger | 22 Jun 2014
Regular data Review Meetings in Mozambique, a Path to Improving Malaria Service Delivery
Health Alliance International (HAI) of the University of Washington, is collaborating with Centro de Investigação Operacional da Beira (CIOB) is based in Beira, Mozambique to improve the quality and use of routine monitoring and evaluation data from the health facility through to the district in Sofala Province. The aim is to strengthen the health system through data for decision making and improve quality and uptake of services. This effort is sponsored by a grant from the Doris Duke Charitable Foundation.
 A key feature of the program is a regular data review meeting where representatives from health facilities in a district come together and each presents his/her standard Ministry of Health service indicators in a simple slide format. After each presentation the speaker received feedback from the group, including members of the district health management team, on successes and challenges and is encouraged to make plans to improve both data quality and service uptake.
A key feature of the program is a regular data review meeting where representatives from health facilities in a district come together and each presents his/her standard Ministry of Health service indicators in a simple slide format. After each presentation the speaker received feedback from the group, including members of the district health management team, on successes and challenges and is encouraged to make plans to improve both data quality and service uptake.
The data review meetings started with an overview of all HIV, reproductive, maternal and child health indicators. Separate review meetings for malaria service indicators have been recently introduced.
According to members of the district teams, the individual facility staff presenters have grown more skilled in formatting their data and presenting to an audience. Overall, participants in these meetings appear enthusiastic and interested in the results of their peers. Constructive critiques are the norm, and speakers express appreciation for suggestions on how they can improve their services and the resulting data.
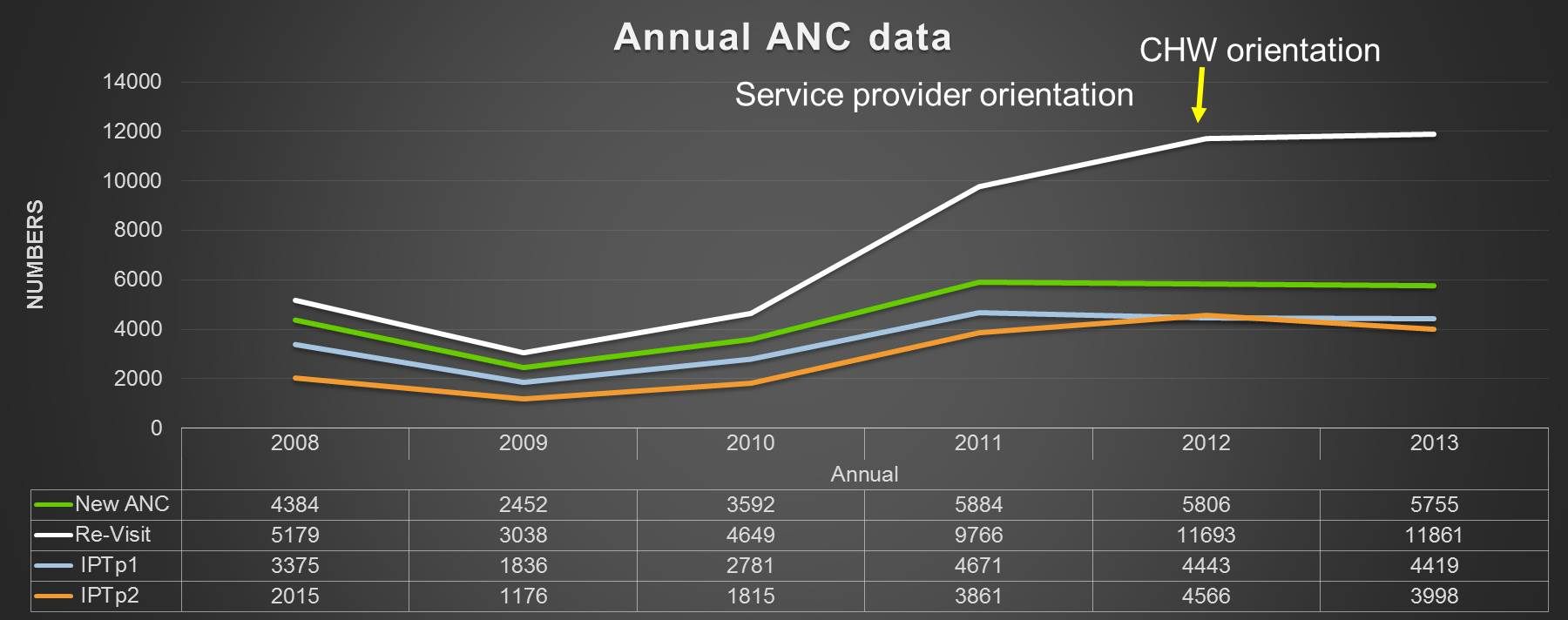
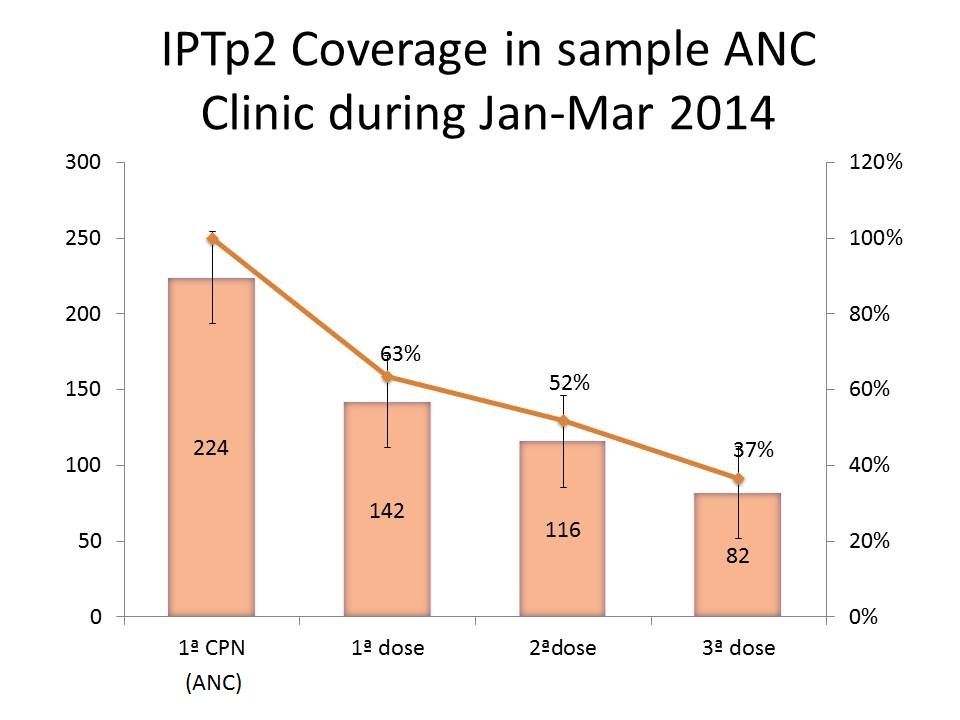 A sample chart from a health facility showing a quarterly review of intermittent preventive treatment for malaria in pregnancy (IPTp) is seen to the right. After viewing this, meeting participants might ask the presenter what are the reasons for the drop-off in coverage. If for example, the problem of late antenatal care (ANC) attendance is mentioned, the group can ask the presenter to consider how to encourage women to attend earlier.
A sample chart from a health facility showing a quarterly review of intermittent preventive treatment for malaria in pregnancy (IPTp) is seen to the right. After viewing this, meeting participants might ask the presenter what are the reasons for the drop-off in coverage. If for example, the problem of late antenatal care (ANC) attendance is mentioned, the group can ask the presenter to consider how to encourage women to attend earlier.
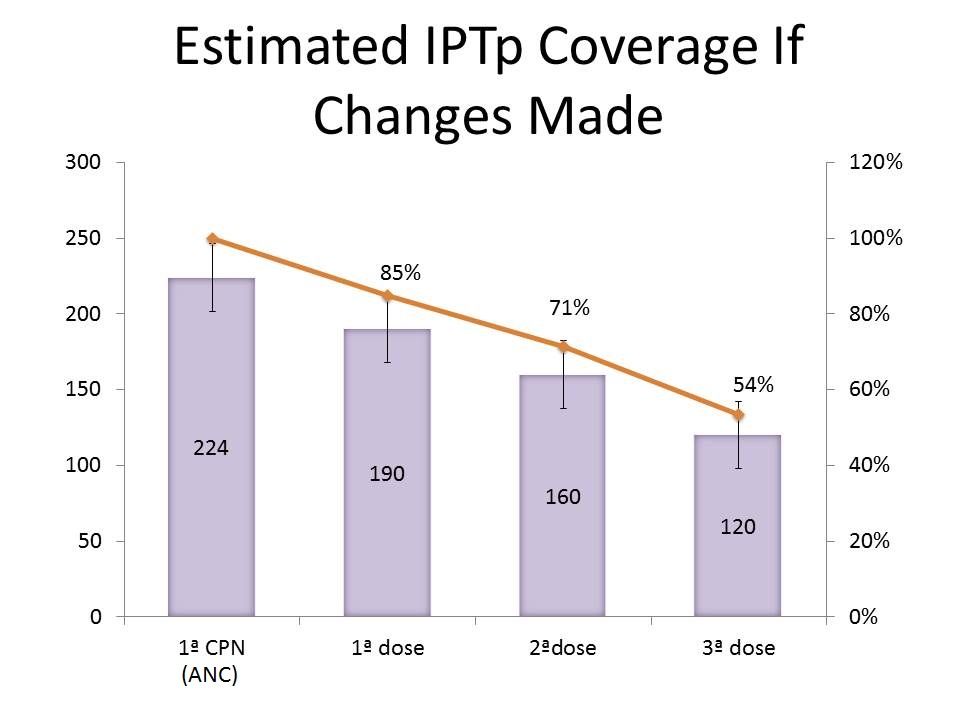 If the presenter then goes back and implements the suggestions, the second chart might reflect the results of improved service uptake. In this way the overall project hopes that close examination of their own data by service providers can strengthen service delivery and the health system.
If the presenter then goes back and implements the suggestions, the second chart might reflect the results of improved service uptake. In this way the overall project hopes that close examination of their own data by service providers can strengthen service delivery and the health system.
We look forward to hearing more about this unique process so that it can be disseminated in other malaria endemic countries.
Epidemiology &Health Information &Monitoring &Surveillance Bill Brieger | 26 Apr 2014
iPhones for household malaria surveys in Sierra Leone
World Malaria Day 2014 was observed at the Johns Hopkins Bloomberg School of Public Health on Friday 25 April. 21 posters were presented. Below is the abstract of a poster presented by Suzanne Van Hull of Catholic Relief Services.
Catholic Relief Services (CRS) and the Ministry of Health and Sanitation (MoHS) of Sierra Leone (SL) are co-implementing nationwide malaria prevention and treatment activities funded by the Global Fund to fight AIDS, Tuberculosis and Malaria. In order to track progress and impact, CRS and partners led the implementation of a malaria indicator survey (MIS) in early 2013 covering a nationally-representative sample of 6,720 households, inclusive of blood testing to determine prevalence of anemia and malaria. In early 2012, CRS also had the experience of using mobile technology for a Knowledge Attitude and Practices (KAP) study.
Fieldworkers used Apple 3GS iPhones for both surveys to collect data via the iFormBuilder platform, a web-based, software-as-services application with a companion app for the mobile devices allowing for timely data collection, monitoring, and analysis.
This was the first time that iPhones were used for a MIS, and lessons learned include: allowing at least four months to transform paper-based questionnaires into electronic format, giving the program enough time for pre-testing the tool and training data collectors/biomarkers/laboratory technicians, and involving key malaria stakeholders to ensure a nationally-led survey. Global Positioning Systems enabled the MoHS to make in-depth analyses on malaria trends based on geographic locations.
 Overall the benefits of an electronic versus a paper-based MIS questionnaire outweighed the challenges. The iPhone technology eliminated the need for paper transcribing, allowing for quicker data tabulation, real-time identification of mistakes, faster interviewing through skip patterns, and a close-to-clean dataset by the end of data collection saving time and money.
Overall the benefits of an electronic versus a paper-based MIS questionnaire outweighed the challenges. The iPhone technology eliminated the need for paper transcribing, allowing for quicker data tabulation, real-time identification of mistakes, faster interviewing through skip patterns, and a close-to-clean dataset by the end of data collection saving time and money.
Survey results will be used to set evidence-based targets for all partners’ future malaria activities, especially the next 3 years of GF-supported malaria grants
Diagnosis &Monitoring &Surveillance Bill Brieger | 21 Jan 2014
World Malaria Report 2013: Surveillance and Monitoring, Getting to the Heart of the Matter
Although “Malaria surveillance, monitoring and evaluation” is the seventh of eight chapters in the 2013 World Malaria Report (WMR), it is in fact the heart of the matter. Progress on goals, finance, vector control, preventive therapies, diagnosis and treatment and of course impact (chapters 2-6 and 8) could not be produced without the documentation processes discussed in Chapter Seven. So what does WMR 2013 tell us about the status of malaria surveillance?
 The global press has been taken by World Health Organization estimates that deaths from malaria world-wide have reduced by fifty percent since 2000.[i] These claims have been made despite the note in WMR 2013 that, “In 2012, in 62 countries of 103 that had ongoing malaria transmission in 2000, reporting was considered to be sufficiently consistent to make a reliable judgment about malaria trends for 2000–2012. In the 41 remaining countries, which account for 80% of estimated cases, it is not possible to reliably assess malaria trends using the data submitted to WHO. Information systems are weakest, and the challenges for strengthening systems are greatest, where the malaria burden is greatest.”[ii]
The global press has been taken by World Health Organization estimates that deaths from malaria world-wide have reduced by fifty percent since 2000.[i] These claims have been made despite the note in WMR 2013 that, “In 2012, in 62 countries of 103 that had ongoing malaria transmission in 2000, reporting was considered to be sufficiently consistent to make a reliable judgment about malaria trends for 2000–2012. In the 41 remaining countries, which account for 80% of estimated cases, it is not possible to reliably assess malaria trends using the data submitted to WHO. Information systems are weakest, and the challenges for strengthening systems are greatest, where the malaria burden is greatest.”[ii]
WHO explains that, “Improved surveillance for malaria cases and deaths will help ministries to determine which areas or population groups are most affected and help to target resources to communities most in need.” WHO suggests that the design of malaria surveillance systems focuses on two fundamental factors. First, the level of malaria transmission should be ascertained, and the resources available to conduct surveillance must be made available. WHO has released two manuals to strengthen malaria surveillance depending on whether the country is high burden and still at the level of “Malaria Control,”[iii] or the country is approaching “Malaria Elimination.”[iv]
 The World Health Organization has issued a series of documents focusing on “Test. Treat. Track.” or ‘3T’. In short these documents support malaria-endemic countries in their efforts to achieve universal coverage with 1) diagnostic testing, 2) antimalarial treatment, and 3) strengthening their malaria surveillance systems to track the disease.[v]
The World Health Organization has issued a series of documents focusing on “Test. Treat. Track.” or ‘3T’. In short these documents support malaria-endemic countries in their efforts to achieve universal coverage with 1) diagnostic testing, 2) antimalarial treatment, and 3) strengthening their malaria surveillance systems to track the disease.[v]
WHO notes that in elimination settings, surveillance systems should seek to identify and immediately provide notification of all malaria infections, whether they are symptomatic or not. A summary of WHO’s recommendations for the “Track” or surveillance aspect of 3T follow:
- Individual cases should be registered at health facility level. This allows for the recording of suspected cases, diagnostic test results, and treatments administered
- In the malaria control phase, countries should report suspected, presumed and confirmed cases separately, and summarize aggregate data on cases and deaths on a monthly basis
- Countries in elimination phase should undertake a full investigation of each malaria case.
Some country examples of surveillance efforts in the move toward malaria elimination will be featured in the upcoming January 2014 issue of Africa Health. Watch for it at: http://www.africa-health.com/
[i] Pizzi M. WHO: Malaria deaths of young children cut by half, but gains ‘fragile’. Aljazeera America. December 11, 2013. http://america.aljazeera.com/articles/2013/12/11/who-malaria-battlehalfwaywon.html
[ii] WHO GLOBAL MALARIA PROGRAMME. World Malaria Report: 2013. World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland, 2013. http://www.who.int/malaria/publications/world_malaria_report_2013/en/index.html
[iii] World Health Organization. Disease surveillance for malaria control. World Health Organization, Geneva, 2012.
[iv] World Health Organization. Disease surveillance for malaria elimination: an operational manual. World Health Organization, Geneva, 2012.
[v] World Health Organization. Test. Treat. Track. Scaling up diagnostic testing, treatment and surveillance for malaria. World Health Organization, Geneva, 2012.
Monitoring &Surveillance Bill Brieger | 16 Nov 2013
Malaria Highlights at TropMed2013 Saturday 16th November
Below please find a brief list of some of the presentations coming up today at the American Society of Tropical Medicine 62nd Annual Conference in Washington DC. Click links to view abstracts.

Rapid clearance of parasitemia by the novel spiroindolone KAE609 in a phase 2 open-label study of adults with acute, uncomplicated Plasmodium falciparum or vivax malaria mono-infection by Nicholas White et al.
In summary, when administered 30 mg daily for 3 days, KAE609 was well tolerated and achieved rapid parasite clearance in adult patients with uncomplicated P. vivax or P. falciparum malaria infection.
Symposium on Implementation of Mass Drug Administration for Malaria Control and Elimination. Symposium Organizer: Roly Gosling, Global Health Group, University of California, San Francisco, San Francisco
With the recognition that a large proportion of malaria infections are low density, below the level of detection by microscopy or Rapid Diagnostic Test, MDA is coming back into favor. The speakers will explore the drug choices available for MDA in different settings; for example, for P. falciparum settings in Haiti, The Gambia and the Artemsisinin Resistance Containment zone, and for P. vivax in Asia and the Pacific.
Innovative Field Tools for Detecting Counterfeit Medicines – The Case Study of Anti-Malarials. Symposium Organizer: JOEL BREMAN, FOGARTY INTERNATIONAL CENTER, NATIONAL INSTITUTES OF HEALTH
The need for innovative field tools for the detection of spurious/falsely-labelled/falsified/counterfeit medicines is becoming increasingly important, particularly in low-resource settings. A global public health crisis is looming, especially in malaria treatment and prevention, where up to 90 percent of antimalarials in surveys done in Asia and Africa are reported to be falsified or substandard.
Session: Malaria Epidemiology – Tracking Trends and Finding Foci, Village-level characteristics associated with spatial distributions of malaria-infected individuals in an area of Southern Zambia receiving mass screening and treatment by David A Larson et al.
Varying spatial distributions of malaria-infected individuals appear to be driven by vector abundance and gametocyte prevalence in the population. The ability to clearly delineate village malaria prevalence may assist in developing mechanisms for focused interventions to optimize their effectiveness.
Session: Malaria Epidemiology – Tracking Trends and Finding Foci. Reservoirs of asymptomatic malaria in Malawi: results of two cross-sectional studies by Jenny A. Walldorf et al.
In Malawi and potentially in other endemic settings, school age children represent important reservoirs of asymptomatic infection and should be targeted for interventions to interrupt transmission.
Session: Malaria Epidemiology – Tracking Trends and Finding Foci. Sustained Declining Burden of Malaria at Community level in Northeastern Tanzania. by Acleus S. Rutta et al.
The reported decline of malaria in most parts of Tanzania has some implication on accuracy of malaria diagnosis and management. The current remarkable and sustained decline in malaria suggests that these areas might be moving from control to pre-elimination levels.
Community &Monitoring &Treatment Bill Brieger | 12 Nov 2013
Community registers in Akwa Ibom State, Nigeria track malaria treatment and integrated services
Below is the abstract for a poster being presented by a team from Jhpiego at the upcoming 62nd annual meeting of the American Society for Tropical Medicine and Hygiene November 13-17 2013 at the Marriott Wardman Park in Washington DC. If you are at the conference, stop by poster number LB-2289 on Friday and discuss with Bright Orji.

Community Directed Distributors bring their registers to the nearby clinic for monthly supervision meetings
Community Directed Treated with Ivermectin (CDTI) for onchocerciasis successfully reached 100,000 African villages with locally selected volunteers known as Community Directed Distributors (CDDs). Recognizing CDTI’s potential other health programs added a variety of interventions to the work of CDDs. Jhpiego (an Affiliate of Johns Hopkins University) successfully engaged communities and their CDDs in Akwa Ibom State, Nigeria to control malaria in pregnancy from 2007-11, and subsequently found the communities willing to expand into integrated community case management (ICCM) of malaria, diarrhoea and pneumonia. This report documents iCCM services given by CDDs.
The project mobilized 108 kin groups (100 +/- people) in 6 clinic catchment areas two Local Government Areas of the State. Each kin group selected 1-2 CDDs. Overall, 152 CDDs were trained by staff of local health centers. CDDs continued to provide intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine and then added malaria rapid diagnostic tests (RDTs); Artemisinin-based Combination Therapy for positive RDT results; oral rehydration solution and zinc tablets for diarrhea, and cotrimoxazole for pneumonia.
Data were extracted one year’s information from a sample of 68 community registers by three health staff using a checklist. During the period 2,202 clients were seen by CDDs with ages ranging from infancy to adulthood. Overall 33.3% were treated for malaria, 20.3% for pneumonia and 7.8% for diarrhoea (a few had multiple problems). Among the client visits, 30.6% were for pregnant women receiving a dose of IPTp.
RDTs were used with 1550 clients (70.4%) who had suspected malaria and 44.1% were positive. The breakdown of the 734 treated for malaria was positive RDT (93.1%), negative RDT (2.2%) and no test (5.2%). Community registers have shown that volunteer CDDs can provide a variety of front line health services, and can fairly correctly follow malaria testing and treatment procedures.