Case Management &Epidemiology &Malaria in Pregnancy Bill Brieger | 09 Dec 2017
Prof Lateef A Salako, 1935-2017, Malaria Champion
 Professor Lateef Akinola Salako was an accomplished leader in malaria and health research in Nigeria whose contributions to the University of Ibadan and the Nigeria Institute for Medical Research (among others) advanced the health of the nation, the region and the world. His scientific research and his over 140 scientific publications spanned five decades.
Professor Lateef Akinola Salako was an accomplished leader in malaria and health research in Nigeria whose contributions to the University of Ibadan and the Nigeria Institute for Medical Research (among others) advanced the health of the nation, the region and the world. His scientific research and his over 140 scientific publications spanned five decades.
His research not only added to knowledge but also served as a mentoring tool to junior colleagues. Some of his vast areas of interest in malaria ranged from malaria epidemiology, to testing the efficacy of malaria drugs to tackling the problem of malaria in pregnancy. He led a team from three research sites in Nigeria that documented care seeking for children with malaria the acceptability of pre-packaged malaria and pneumonia drugs for children that could be used for community case management. Prof Salako was also involved in malaria vaccine trials and urban malaria studies.
As recent as 2013 Prof Lateef Salako, formerly of NIMR said: “It is true there is a reduction in the rate of malaria cases in the country, but to stamp out this epidemic there is the urgent need for a synergy between researchers, the government, ministries, departments and agencies and involved in malaria control. That will enable coordinated activities that will produce quicker results than what obtains at the moment.”
At least one website has been set up where people can express their condolences. As one person wrote, “Professor Lateef Salako was an exceptional student, graduating with distinction from medical school; an unforgettable teacher, speaking as a beneficiary of his tutelage; an exemplary scholar, mentoring many others; an accomplished scientist, making indelible contributions to knowledge. May his legacy endure.”
Readers are also welcome to add their own comments here about Prof Salako’s contribution to malaria and tropical health.
Health Workers &IPTp &Malaria in Pregnancy Bill Brieger | 09 Nov 2017
Improving intermittent preventive treatment for pregnant women (IPTp) coverage in 5 districts in Chad and Cameroon
 Kodjo Morgah and Naibei Mbaïbardoum of Jhpiego with support from the ExxonMobil Foundation ave been working to increase interventions that protect pregnant women from malaria. The results below were shared at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Kodjo Morgah and Naibei Mbaïbardoum of Jhpiego with support from the ExxonMobil Foundation ave been working to increase interventions that protect pregnant women from malaria. The results below were shared at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Malaria is the leading cause of morbidity and mortality in Cameroon and Chad, where an estimated 500,000 and 1.5 million cases occur every year, respectively. In Cameroon, 55% of hospitalizations and 241 deaths among pregnant women reported in 2010 were due to malaria. In Chad, malaria accounted for 30% of hospital admissions and 41% of deaths among pregnant women in 2013.
 To improve uptake of intermittent preventive treatment for pregnant women (IPTp) for malaria in 5 districts in Chad and the Kribi district of Cameroon, Jhpiego adopted strategies targeting the 4 levels of the health system in each country: updating national policies and guidelines, building capacity of providers, building community health workers’ (CHWs) capacity, and engaging in behavior change communication.
To improve uptake of intermittent preventive treatment for pregnant women (IPTp) for malaria in 5 districts in Chad and the Kribi district of Cameroon, Jhpiego adopted strategies targeting the 4 levels of the health system in each country: updating national policies and guidelines, building capacity of providers, building community health workers’ (CHWs) capacity, and engaging in behavior change communication.
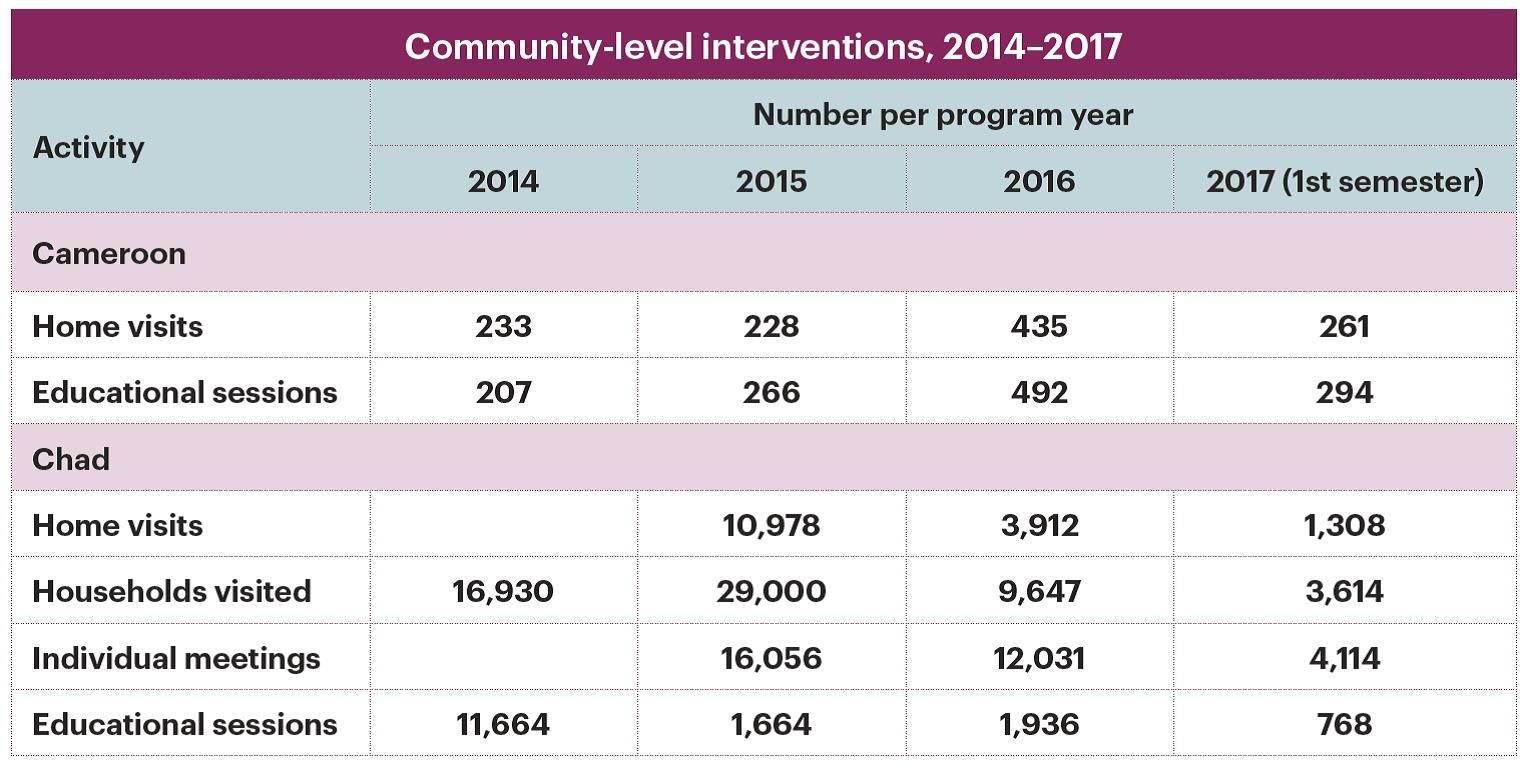 Nationally, Jhpiego provided technical guidance to the Ministries of Health to develop tools including: training and malaria in pregnancy (MIP) reference manuals for providers and CHWs, guidelines on IPTp, and key supervision and data collection tools. At the regional/district levels, 38 supervisors were trained, and they conducted 248 supervisory visits in both countries, reaching 137 health facilities.
Nationally, Jhpiego provided technical guidance to the Ministries of Health to develop tools including: training and malaria in pregnancy (MIP) reference manuals for providers and CHWs, guidelines on IPTp, and key supervision and data collection tools. At the regional/district levels, 38 supervisors were trained, and they conducted 248 supervisory visits in both countries, reaching 137 health facilities.
 At the facility level, 234 providers were trained in malaria prevention and management, MIP, data collection and commodity management. At the community level, 146 CHWs in both countries were trained to raise awareness on malaria prevention and control.
At the facility level, 234 providers were trained in malaria prevention and management, MIP, data collection and commodity management. At the community level, 146 CHWs in both countries were trained to raise awareness on malaria prevention and control.
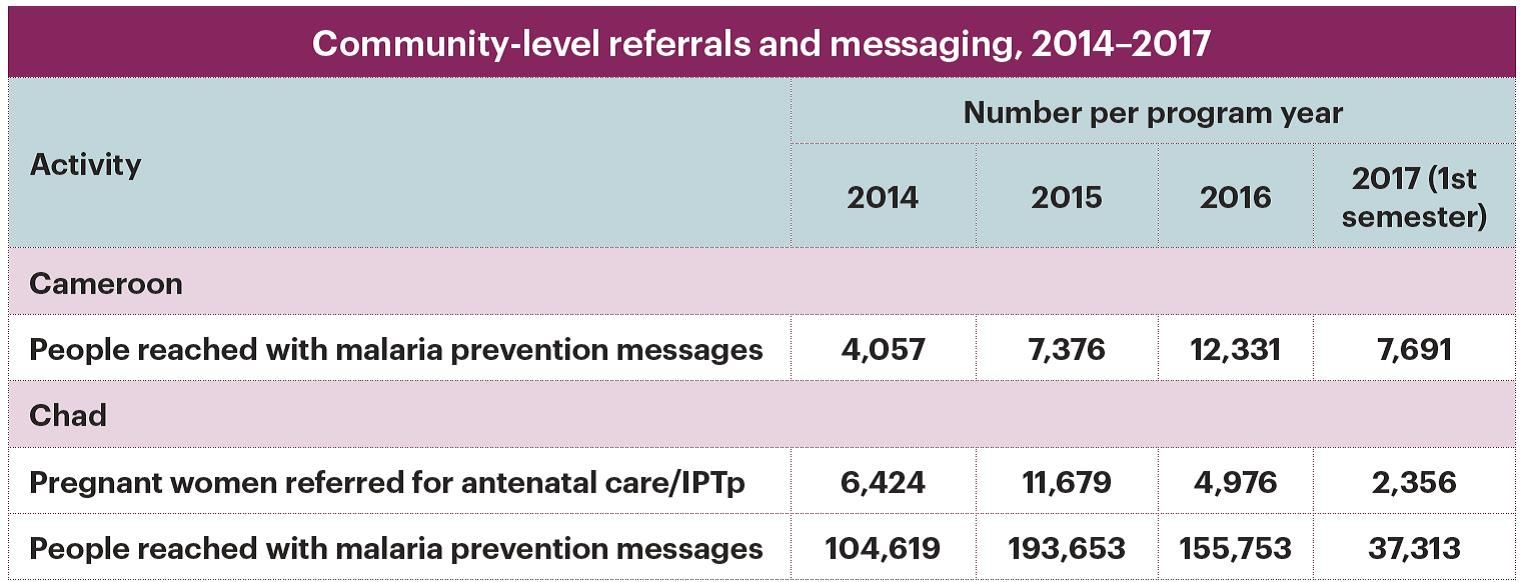
 In Chad, CHWs referred 6424 pregnant women for antenatal care/IPTp and 11679 pregnant women for malaria treatment in 2014 and 2015. Health facility and CHW data collection tools were revised and monthly validation of district data was implemented to improve data reliability, completeness, and readiness.
In Chad, CHWs referred 6424 pregnant women for antenatal care/IPTp and 11679 pregnant women for malaria treatment in 2014 and 2015. Health facility and CHW data collection tools were revised and monthly validation of district data was implemented to improve data reliability, completeness, and readiness.
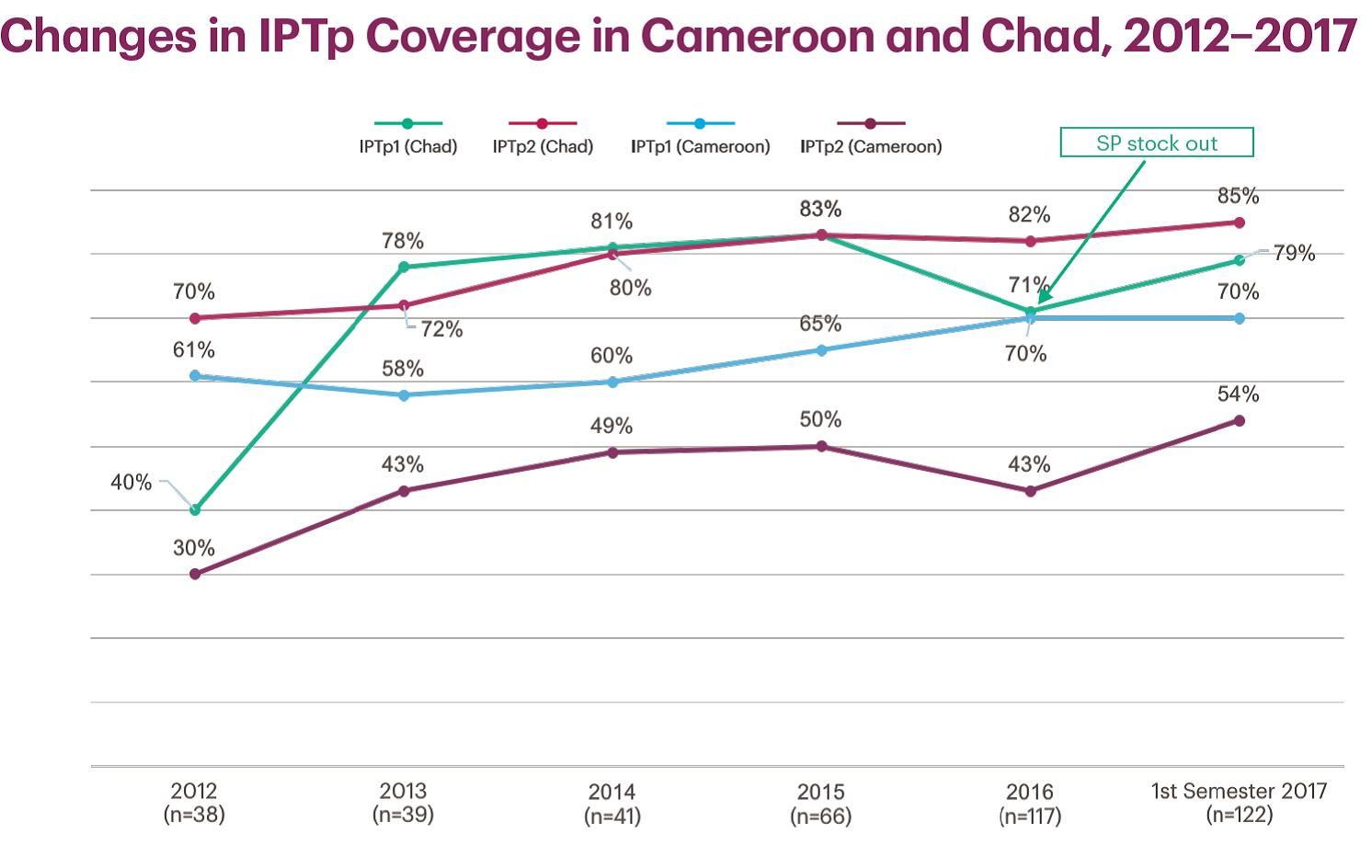
As a result of Jhpiego’s activities in Kribi, IPTp rates increased from the start of the project in 2012 to 2015: from 70% to 83% (IPTp1), 61% to 80% (IPTp2), and 12.7% to 28.1% (IPTp3). Similarly, from 2012 to 2015 in Chad, IPTp1 rates increased from 40% to 83% and from 30% to 50% for IPTp2. These gains are a result of training paired with coaching and supervision activities of trained providers and targeted facilities.
Health Workers &IPTp &Malaria in Pregnancy &Performance &Quality of Services Bill Brieger | 09 Nov 2017
Results of an evaluation of the Toolkit to Improve Early and Sustained Intermittent Preventive Treatment in Pregnancy (IPTp) Uptake in Mozambique and Madagascar
 Lalanirina Ravony, Elana Fiekowsky, Lisa Noguchi, Patricia P. Gomez, Jean Pierre Rakotovao, Eliane Razafimandimby, Armindo Tiago, Kathryn Smock, Arsene Ratsimbarisoa, Kristen Vibbert, and Robert Sellke shared their efforts to apply a toolkit to enable health providers to ensure better uptake of intermittent preventive treatment for malaria during antenatal clinics. As seen below, they presented their findings at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Lalanirina Ravony, Elana Fiekowsky, Lisa Noguchi, Patricia P. Gomez, Jean Pierre Rakotovao, Eliane Razafimandimby, Armindo Tiago, Kathryn Smock, Arsene Ratsimbarisoa, Kristen Vibbert, and Robert Sellke shared their efforts to apply a toolkit to enable health providers to ensure better uptake of intermittent preventive treatment for malaria during antenatal clinics. As seen below, they presented their findings at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
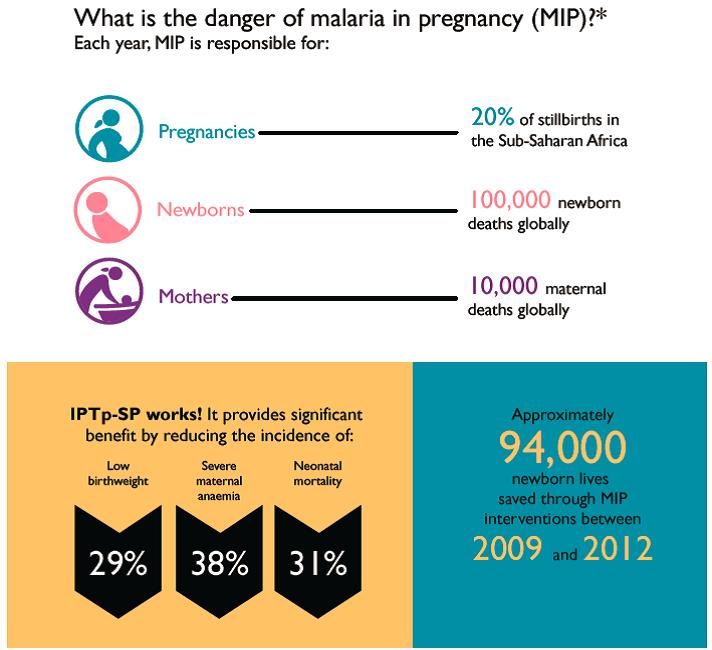
Malaria in pregnancy (MIP) is a leading cause of maternal and newborn morbidity and mortality; however uptake of intermittent preventive treatment in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP), an effective prevention tool, remains alarmingly low across sub-Saharan Africa, including Mozambique and Madagascar.
 The WHO 2012 policy recommendations to prevent MIP include early enrollment into antenatal care (ANC), accurate estimation of gestational age (GA) and administration of IPTp-SP during ANC visits beginning early in the second trimester, spaced at least one month apart. Preventing MIP remains a challenge in settings with inconsistent application of these recommendations and inadequate provider training in estimating GA.
The WHO 2012 policy recommendations to prevent MIP include early enrollment into antenatal care (ANC), accurate estimation of gestational age (GA) and administration of IPTp-SP during ANC visits beginning early in the second trimester, spaced at least one month apart. Preventing MIP remains a challenge in settings with inconsistent application of these recommendations and inadequate provider training in estimating GA.
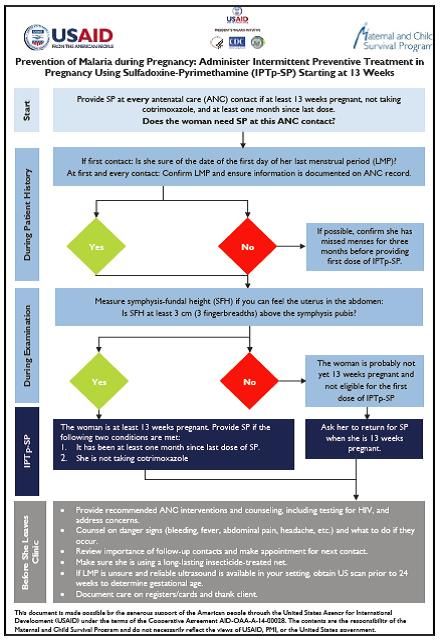 To improve adherence to these recommendations, a toolkit was designed which includes a job aid with an algorithm to guide providers during ANC visits to determine IPTp-SP eligibility. Twenty-four providers from 24 facilities in Madagascar and 29 providers from seven facilities in Mozambique were trained on use of the job aid and interviewed three months later about their experience.
To improve adherence to these recommendations, a toolkit was designed which includes a job aid with an algorithm to guide providers during ANC visits to determine IPTp-SP eligibility. Twenty-four providers from 24 facilities in Madagascar and 29 providers from seven facilities in Mozambique were trained on use of the job aid and interviewed three months later about their experience.
Individual providers were interviewed using a questionnaire to assess the clarity and utility to the job aid, and their opinions of the practicality of the orientation. Interviewers also gathered information on years of experience and clinical certification. All providers reported that the job aid reminded them to estimate GA and measure fundal height, which is particularly helpful since few women remember the date of their last menstrual period (LMP).
 Health workers also reported that the job helped them encourage the use of long-lasted insecticide treated nets, and reminded them of the proper timing to start IPTp-SP. We conclude that the toolkit is useful to prompt providers to calculate GA and offer IPTp as early as possible in the second trimester.
Health workers also reported that the job helped them encourage the use of long-lasted insecticide treated nets, and reminded them of the proper timing to start IPTp-SP. We conclude that the toolkit is useful to prompt providers to calculate GA and offer IPTp as early as possible in the second trimester.
Future potential directions include revision of all Toolkit components to reflect input from this evaluation, including development of a wall poster version to enhance readability, and inclusion of a pregnancy wheel to facilitate calculation of GA and estimated date of delivery.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Communication &Health Workers &IPTp &Malaria in Pregnancy Bill Brieger | 09 Nov 2017
Results from a Formative Evaluation of the Malaria in Pregnancy Case Management Job Aid in Nigeria
Job Aids can provide valuable assistance to health workers, but it is important to evaluate if they serve the intended purpose. With support from USAID’s Maternal and Child Survival Program, Bright Orji, Enobong Ndekhedehe, Elana Fiekowsky, Patricia Gomez, Aimee Dickerson, Reena Sethi, Bibian Udeh, Kristin Vibbert, and Robert Sellke reported at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene on their evaluation of a Job Aid for Nigeria on the prevention of malaria in pregnancy as seen below.
 Annually, nearly 7 million pregnant women in Nigeria are at risk of malaria in pregnancy (MIP). Although antenatal care is the platform for the prevention and treatment of MIP, malaria is also treated at outpatient departments.
Annually, nearly 7 million pregnant women in Nigeria are at risk of malaria in pregnancy (MIP). Although antenatal care is the platform for the prevention and treatment of MIP, malaria is also treated at outpatient departments.
It is known that women of reproductive age (WRA) are often treated for malaria without assessing pregnancy status, although artemisinin combination therapies are contraindicated in the first trimester of pregnancy, and many pregnant women do not receive the recommended low cost interventions.
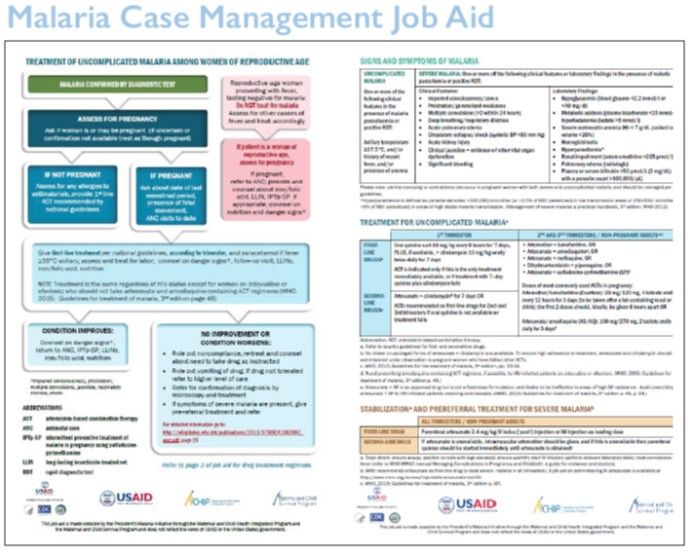
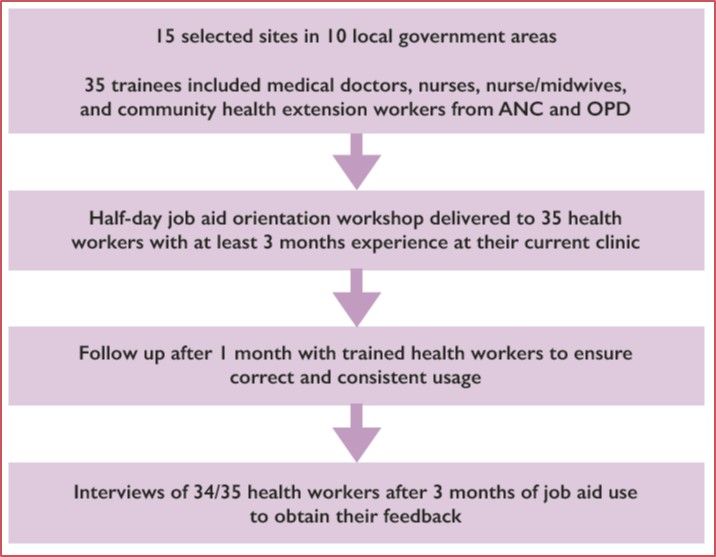 In order to increase access to these MIP interventions, the President’s Malaria Initiative supported the Maternal and Child Survival Program and partners to develop a two-page job aid for case management of uncomplicated malaria among WRA. In collaboration with the Nigeria Malaria Elimination Program, the job aid was evaluated in Ebonyi State, a high malaria burden area, to determine providers’ perceptions of its clarity, acceptability, and utility.
In order to increase access to these MIP interventions, the President’s Malaria Initiative supported the Maternal and Child Survival Program and partners to develop a two-page job aid for case management of uncomplicated malaria among WRA. In collaboration with the Nigeria Malaria Elimination Program, the job aid was evaluated in Ebonyi State, a high malaria burden area, to determine providers’ perceptions of its clarity, acceptability, and utility.
 A half-day workshop on use of the job aid was provided to 35 health workers (nurses – 20%; nurse-midwives – 20%; community health extension workers – 48%; and medical doctors – 12%) already trained on MIP case management, selected from 15 facilities where WRA seek care. After 3 months of use, a one-page questionnaire was administered to 34 health workers.
A half-day workshop on use of the job aid was provided to 35 health workers (nurses – 20%; nurse-midwives – 20%; community health extension workers – 48%; and medical doctors – 12%) already trained on MIP case management, selected from 15 facilities where WRA seek care. After 3 months of use, a one-page questionnaire was administered to 34 health workers.
One-hundred percent stated that the job aid helped them to do the following: identify pregnant women among the WCBA presenting with fever; use rapid diagnostic tests to diagnose malaria; and treat uncomplicated MIP. Sixty-eight percent used the job aid to provide correct treatment for severe malaria and 88% used it while providing services all or most of the time.
The results indicated that after a half-day orientation on use of the job aid, health workers were able to use it to help them identify women who may be pregnant and provide appropriate treatment for uncomplicated MIP. They are also able to explain its use to colleagues.
It is suggested that a poster-size version could be printed and disseminated to appropriate cadres of health workers in clinics where WRA seek care for fever, as it is anticipated that providers could benefit from its use.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Malaria in Pregnancy &Quality of Services Bill Brieger | 09 Nov 2017
Using the Antenatal Care Quality Improvement Tool and targeted training to strengthen ANC Services including MiP in Tanzania
 Malaria prevention in pregnancy (MIP) is a major component of antenatal services in endemic countries. Jasmine Chadewa, Dunstan Bishanga, Elaine Roman, Godlisten Martin, Kristen Vibbert, Lauren Borsa, Agrey Mbilinyi, Jeremie Zoungrana, and Hussein Kidanto describe how they applied a quality improvement tool to strengthen ANC and MIP services at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings follow:
Malaria prevention in pregnancy (MIP) is a major component of antenatal services in endemic countries. Jasmine Chadewa, Dunstan Bishanga, Elaine Roman, Godlisten Martin, Kristen Vibbert, Lauren Borsa, Agrey Mbilinyi, Jeremie Zoungrana, and Hussein Kidanto describe how they applied a quality improvement tool to strengthen ANC and MIP services at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings follow:
Malaria in Pregnancy (MiP) is a major, preventable cause of maternal morbidity and poor birth outcomes. In collaborations with partners, Tanzania’s National Malaria Control Program (NMCP) and the Reproductive and Child Health Unit has been working to promote the World Health Organization’s three-pronged approach to address the burden of MiP.
 A malaria training for 180 supervisors and 360 ANC providers from 221 health facilities was conducted in the Kagera and Mara regions. Updates included an orientation on MiP as well as malaria case management, screening, data management and ITN promotion.
A malaria training for 180 supervisors and 360 ANC providers from 221 health facilities was conducted in the Kagera and Mara regions. Updates included an orientation on MiP as well as malaria case management, screening, data management and ITN promotion.
Prior to the training, facility baseline assessments were conducted using the Ministry of Health, Community Development, Gender, Elderly and Children (MOHCDGEC) antenatal care quality improvement (ANC QI) tool to identify gaps in knowledge and skills of health providers to better target trainings to improving the quality of ANC services.
A second assessment took place six months post training. Both assessments included hospital, health facility and dispensary levels and included observation, interviews, record reviews and skills assessments.
 Results demonstrated that over 90% of the facilities scored below 30% across all categories in the overall baseline assessment with a high score of 35 %, while the 2nd assessment showed a large improvement with 40% of the facilities scoring below 30% and a high score of 70%.
Results demonstrated that over 90% of the facilities scored below 30% across all categories in the overall baseline assessment with a high score of 35 %, while the 2nd assessment showed a large improvement with 40% of the facilities scoring below 30% and a high score of 70%.
The ANC QI tool is effective in determining the impact of ANC health provider’s knowledge and skills to target training to improve ANC service quality.
The presentation was made possible through support provided to the USAID Boresha Afya Project, under the terms of the Cooperative Agreement AID-621-A-16-00003 by the President’s Malaria Initiative via the United States Agency for International Development (USAID), an inter-agency agreement with Centers for Disease Control and Prevention (CDC). The opinions expressed herein are those of the author(s) and do not necessarily reflect the views of the President’s Malaria Initiative via the US Agency for International Development.
IPTp &Malaria in Pregnancy Bill Brieger | 08 Nov 2017
Missed Opportunities for Uptake of Intermittent Preventative Treatment for Malaria in Pregnancy in Tanzania
 A major reason that coverage targets for intermittent treatment of malaria in pregnancy fall short are missed opportunities at health service sites. Jasmine Chadewa, Yusuph Kulindwa, Dunstan Bishanga, Mary Drake, Jeremie Zoungrana, Elaine Roman, Hussein Kidanto, Naomi Kaspar, Kristen Vibbert, and Lauren Borsa share what they have learned about this issue at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
A major reason that coverage targets for intermittent treatment of malaria in pregnancy fall short are missed opportunities at health service sites. Jasmine Chadewa, Yusuph Kulindwa, Dunstan Bishanga, Mary Drake, Jeremie Zoungrana, Elaine Roman, Hussein Kidanto, Naomi Kaspar, Kristen Vibbert, and Lauren Borsa share what they have learned about this issue at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
 About 35 million people in Tanzania are at risk of malaria, with pregnant women and under five children being the most vulnerable. The Tanzania National Malaria Control Program’s (NMCP) Strategic Plan for 2007–2012 reports that malaria accounts for 30% of the national disease burden, with about 1.7 million cases per year among pregnant women.
About 35 million people in Tanzania are at risk of malaria, with pregnant women and under five children being the most vulnerable. The Tanzania National Malaria Control Program’s (NMCP) Strategic Plan for 2007–2012 reports that malaria accounts for 30% of the national disease burden, with about 1.7 million cases per year among pregnant women.
 To prevent the effect of malaria in pregnancy, the Tanzania Government adopted IPTp3+ therapy for pregnant women per the WHO recommendations for IPTp-SP. This study explores missed opportunities to deliver IPT by looking at predictors causing the drop between coverage of IPTp2 (34%) and IPTp3+ (7%).
To prevent the effect of malaria in pregnancy, the Tanzania Government adopted IPTp3+ therapy for pregnant women per the WHO recommendations for IPTp-SP. This study explores missed opportunities to deliver IPT by looking at predictors causing the drop between coverage of IPTp2 (34%) and IPTp3+ (7%).
The study examined Tanzania Demographic and Health Survey (TDHS) 2015/2016 data on women aged 15-49 with a live birth in the two years preceding the survey and at least 2 doses or more of IPTp during ANC (n=4219) to identify factors associated with differences in IPTp uptake. Variables of interest were identified, recoded and generated as required. Data was analyzed using STATA v14, whereby frequency distributions were calculated and cross-tabs and logistic regressions were done comparing dependent and independent variables.
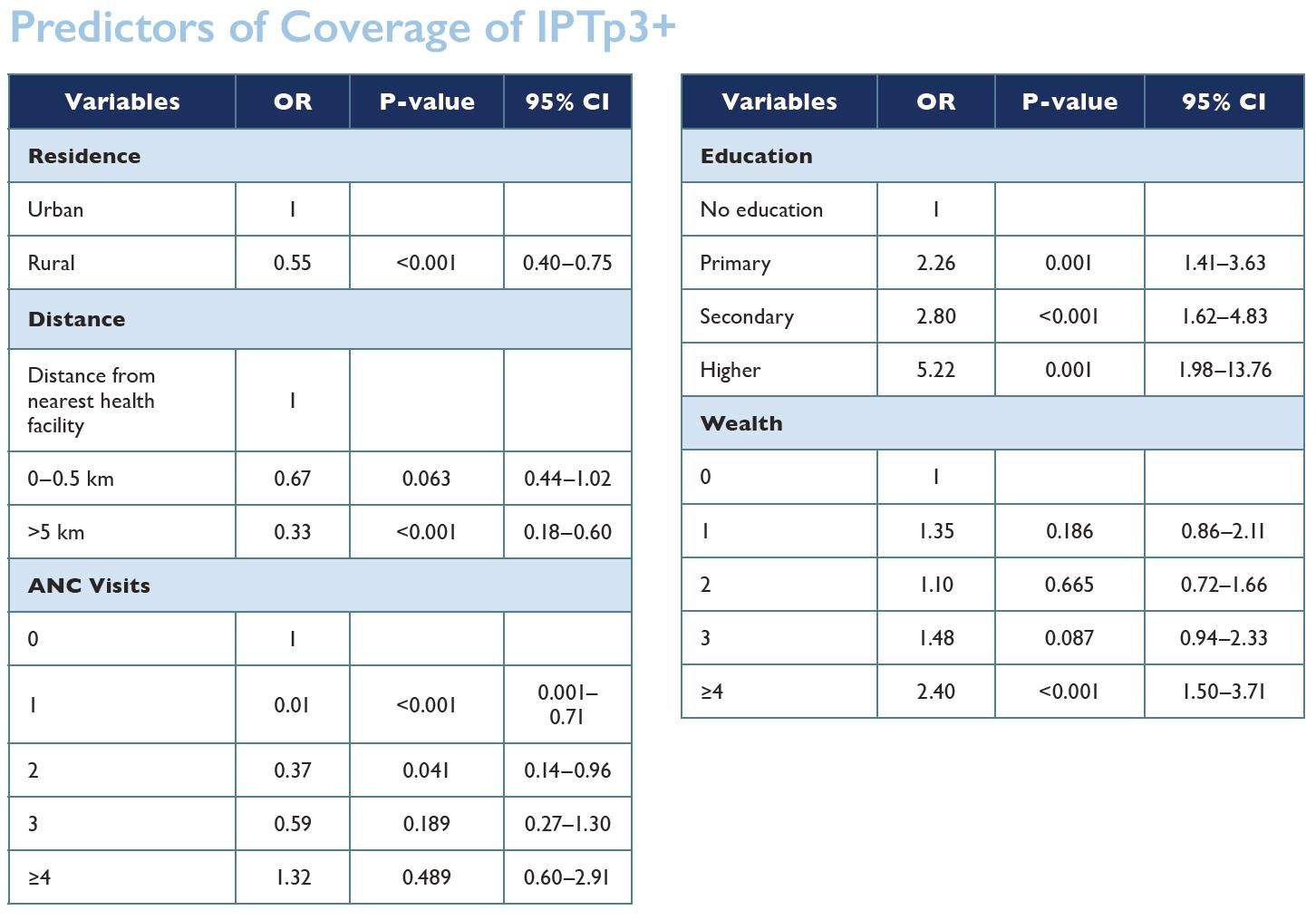 The analysis shows the factors contributing to the drop of IPTp uptake include wealth (the richest people are 2.5 times more likely to take at least three doses of IPTp) and education (those with no education are less likely to take more doses of IPTp compared to those who are educated). Residency is the largest contributing factor: 50% of pregnant mothers in rural areas are less likely to take three or more doses of SP.
The analysis shows the factors contributing to the drop of IPTp uptake include wealth (the richest people are 2.5 times more likely to take at least three doses of IPTp) and education (those with no education are less likely to take more doses of IPTp compared to those who are educated). Residency is the largest contributing factor: 50% of pregnant mothers in rural areas are less likely to take three or more doses of SP.
Clients living within 5 km of health facilities have higher uptake of IPTp3+ compared to their counterparts who live further from the health facilities (33% less likely). However, our analysis shows that there is no correlation between IPTp3+ uptake and number of ANC visits, health insurance or number of children.
Based on these results, it is important to strategize to make health services and education more accessible to the population in order to increase IPTp uptake among pregnant women.
Community &IPTp &Malaria in Pregnancy Bill Brieger | 08 Nov 2017
Baseline for Coverage of Intermittent Preventive Treatment of Malaria in Pregnancy for Planning Community Interventions in Burkina Faso

Under supervision from health center Community Health Worker provides SP for IPTp to Pregnant Woman
Now that the World Health Organization recommends that pregnant women in high and stable malaria transmission areas receive three or more doses of Intermittent Preventive Treatment (IPTp) with Sulfadoxine-pyrimethamine, it is necessary to learn ways to reach more women with this intervention. William R. Brieger, Mathurin Dodo, Danielle Burke, Ousmane Badolo, Justin Tiendrebeogo, Kristen Vibbert, Susan J Youll, and Julie R Gutman conducted a baseline household survey of recently pregnant women in Burkina Faso to learn about the extent of current IPTp coverage and where improvements are needed. With support from the US President’s Malaria Initiative and the USAID Maternal and Child Survival Program Their findings were made available at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
The World Health Organization recommends intermittent preventive treatment (IPTp) to prevent the adverse effects of malaria in pregnancy in high burden settings; IPTp coverage has lagged behind international targets. In Burkina Faso, the 2014 Malaria Indicator Survey found that 22% of women received 3 or more doses of IPTp (IPTp3). In 2014, Burkina Faso’s IPTp policy was updated from recommending 2 doses to providing at least 3 doses of IPTp. Prior studies have suggested that use of community health workers to deliver IPTp can increase coverage.
 To improve IPTp coverage, we will pilot community delivery of IPTp within 3 southern districts: Po, Ouargaye, and Batie. Here we report results from a baseline assessment in the selected districts. Health Management Information System (HMIS) data for 2015 were collected in each district, and IPTp3 coverage was 37%. Four health facilities per district were randomly selected to participate in the pilot. In 2017, a baseline household survey was conducted among recently pregnant women in the catchment areas of these health facilities.
To improve IPTp coverage, we will pilot community delivery of IPTp within 3 southern districts: Po, Ouargaye, and Batie. Here we report results from a baseline assessment in the selected districts. Health Management Information System (HMIS) data for 2015 were collected in each district, and IPTp3 coverage was 37%. Four health facilities per district were randomly selected to participate in the pilot. In 2017, a baseline household survey was conducted among recently pregnant women in the catchment areas of these health facilities.
 Women were asked to recall the number of antenatal care (ANC) visits and IPTp doses they had received during their most recent pregnancy. The same information was extracted from their ANC cards. A total of 374 women were interviewed during the baseline survey.
Women were asked to recall the number of antenatal care (ANC) visits and IPTp doses they had received during their most recent pregnancy. The same information was extracted from their ANC cards. A total of 374 women were interviewed during the baseline survey.
ANC attendance was reported to be 98% for any visit, and 84% for four visits; these rates were 90% and 62% as documented on the ANC cards. Over 95% of women recalled receiving the first dose of IPTp, while over 80% of cards verified that the first dose was given.
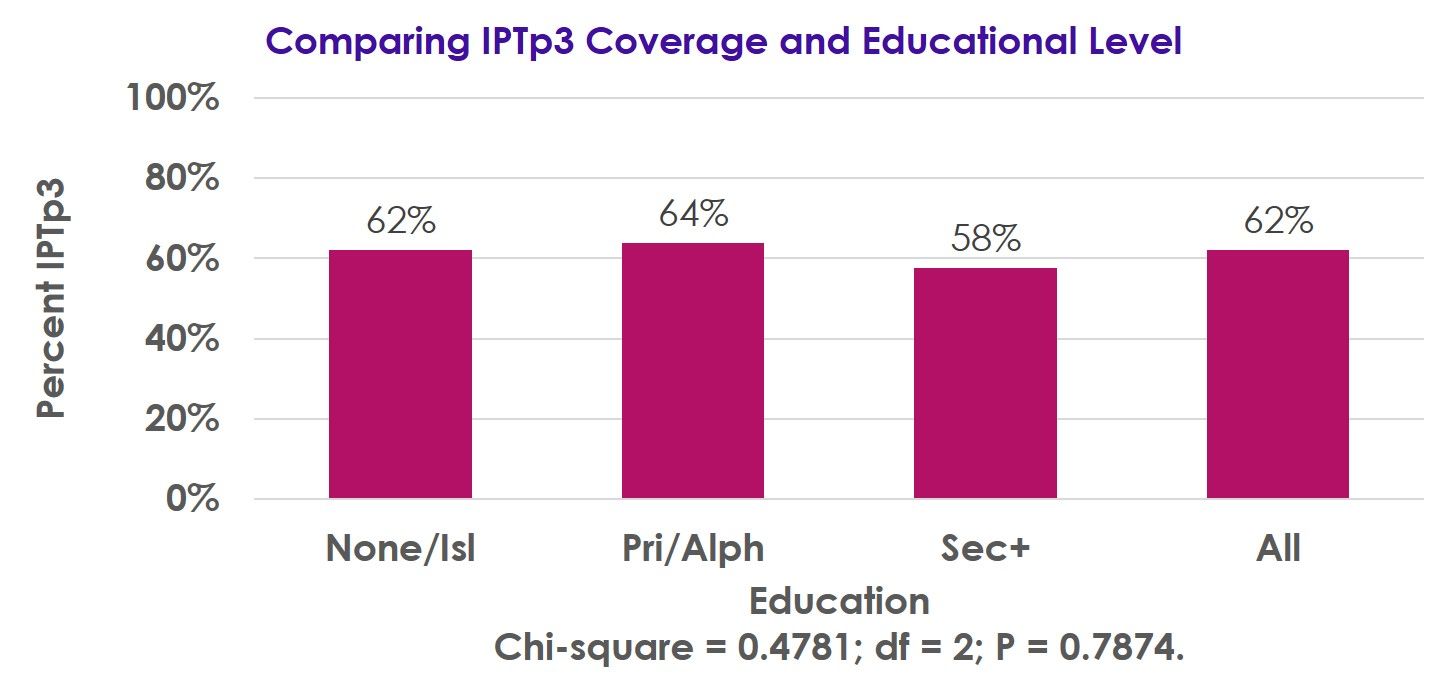 Receipt of the third IPTp dose was 62% by recall and 52% as recorded on the ANC cards, while receipt of 4 doses was 32% by recall and 19% per the ANC cards. IPTp3 coverage was not associated with parity or educational level.
Receipt of the third IPTp dose was 62% by recall and 52% as recorded on the ANC cards, while receipt of 4 doses was 32% by recall and 19% per the ANC cards. IPTp3 coverage was not associated with parity or educational level.
Following implementation of the revised IPTp policy, there has been a substantial improvement in IPTp coverage, though more work is needed to achieve the national 85% coverage target.
Our pilot will examine the impact that delivery of IPTp by community workers has on IPTp coverage, with endline surveys planned for 2018.
Health Information &Malaria in Pregnancy Bill Brieger | 07 Nov 2017
Improving Quality of Data to Advance Malaria in Pregnancy Indicator Coverage in Ebonyi State, Nigeria
Progress in preventing malaria in pregnancy depends on good data. Bright Orji, Gladys Olisaekee, Onyinye Udenze, Enobong Umoekeyo, Chika Nwankwo, Boniface Onwe, Chibugo Okoli, and Emmanuel Otolorin of Jhpiego discussed ways to improve data quality in Nigeria at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene with support from the USAID Maternal and Child Health Program. A summary of their points follows:

Reviewing Health Facility Data
Quality data are crucial for informed decision-making to address health challenges and improve malaria service delivery among countries on the pathway to malaria elimination. This emphasis on better data quality was reflected in the World Malaria Day theme of “Counting Malaria Out” in 2009 and 2010.
In Nigeria, improving malaria data quality has been difficult due to critical health system challenges including poor coordination across different departments, institutional complexities, and a shortage of medical record officers and service providers sufficiently trained in data visualization and use of data for decision-making. In response, the Maternal and Child Health Survival Program (MCSP) in Nigeria embarked on the implementation of key activities to improve quality of malaria data in Ebonyi State.
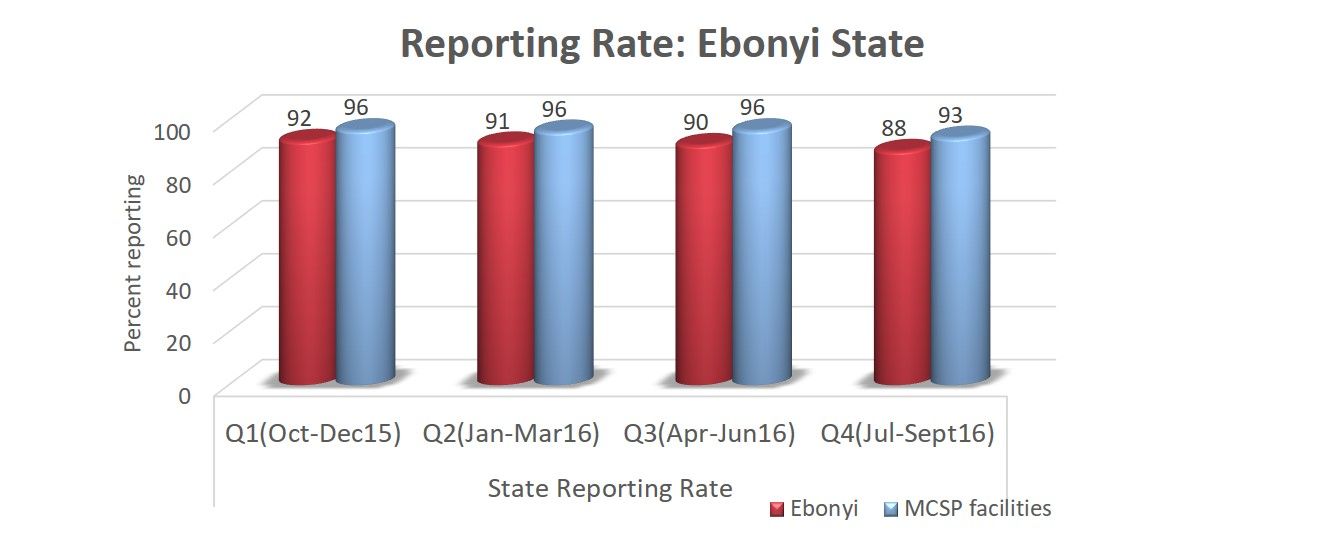 These activities included training on record keeping and use of data for decision-making; post training follow-up; dash boards at the frontline for better data visualization; monthly data collation meetings; improved synergy among service departments; and quarterly data quality assurance visits. As a result, more than 75% of facilities graphed malaria indicators thereby increasing data visualization and use of data for decision-making.
These activities included training on record keeping and use of data for decision-making; post training follow-up; dash boards at the frontline for better data visualization; monthly data collation meetings; improved synergy among service departments; and quarterly data quality assurance visits. As a result, more than 75% of facilities graphed malaria indicators thereby increasing data visualization and use of data for decision-making.
An example of data improvements leading to service increases was Intermittent Preventive Treatment for malaria in pregnancy (IPTp). IPTp1 service statistics in MCSP-supported facilities improved from 54.1% in Oct-Dec 2015 to 81.3% by Jul-Sept 2016 compared to 54.7% to 67.8% in the same periods for non-MCSP facilities.
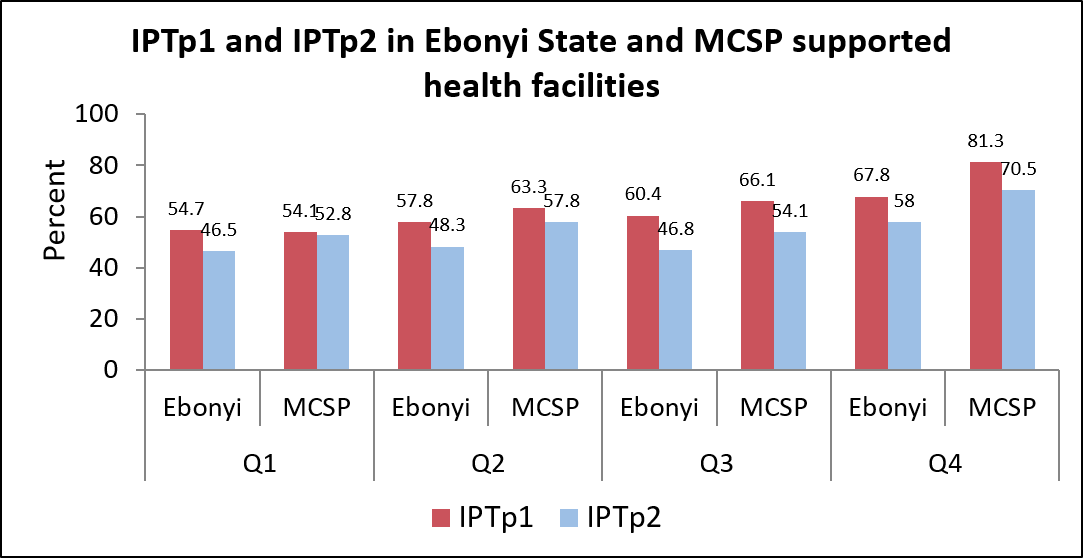 Similarly, IPTp2 service statistics in MCSP-supported facilities improved from 52.8% to 70.5%compared to 46.5% to 58.0% in the same period for non-MCSP facilities.
Similarly, IPTp2 service statistics in MCSP-supported facilities improved from 52.8% to 70.5%compared to 46.5% to 58.0% in the same period for non-MCSP facilities.
Data quality improvement interventions such as monthly data collation and validation meetings prior uploading data to DHIS can contribute to improved quality of malaria performance indicators, better coordination between antenatal care, outpatient and pharmacy departments and increased IPTp coverage.
CHW &Community &IPTp &Malaria in Pregnancy Bill Brieger | 07 Nov 2017
Potential Contribution of Community-Based Health Workers to Improving Prevention of Malaria in Pregnancy
 Justin Tiendrebeogo, Ousmane Badolo, Mathurin Dodo, Danielle Burke, and Bill Brieger of Jhpiego have designed and are implementing a study to determine the effect of delivering Intermittent Preventive Treatment for Malaria in Pregnancy through community health workers in Burkina Faso with the support of the US President’s Malaria Initiative and the USAID Maternal and Child Survival Project. They have shared the design and start-up activities for the study at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. A summary follows:
Justin Tiendrebeogo, Ousmane Badolo, Mathurin Dodo, Danielle Burke, and Bill Brieger of Jhpiego have designed and are implementing a study to determine the effect of delivering Intermittent Preventive Treatment for Malaria in Pregnancy through community health workers in Burkina Faso with the support of the US President’s Malaria Initiative and the USAID Maternal and Child Survival Project. They have shared the design and start-up activities for the study at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. A summary follows:
CHW Flipchart Page
The Ministry of Health of Burkina Faso with the support of its partners initiated a study on the feasibility of increasing provision of Intermittent Preventive Malaria Treatment in pregnant women (IPTp) with sulfadoxine-pyrimethamine (SP) by involving existing community-based health workers (CBHWs). As Burkina Faso adopted the WHO recommendations for more doses of IPTp during pregnancy, it was proposed that the challenge of achieving coverage of third, fourth and additional doses could be met using CBHWs.
The approved protocol calls for CBHWs to refer pregnant women to antenatal care (ANC) to receive their first IPTp dose. Subsequent doses at one-month intervals would be provided by trained CBHWs, who would report back to supervising midwives at the ANC clinics. Several steps were taken to gain approval and set up the intervention.
CHW Using Flipchart
First, IPTp data from the health information system was gathered. IPTp coverage based on ANC registration in the 6 intervention clinics was 69% IPTp1, 68% IPTp2, 56% IPTP3, and 1% IPTp4. Similar information was obtained from the 6 control clinic catchment areas. Situation analysis found that while CBHW curriculum stresses the importance of ANC, it does not address IPTp at community level.
In response updated training materials have been developed. The study team also collected information on village size and availability of CBHWs, especially females. Among the villages in the catchment of the 6 intervention ANC clinics, 33 were found to lack female CBHWs.

Supervisory Meeting
As a result, the team needed to recruit additional female CBHWs, as revised national recruitment guidance stressed attainment of primary school certificate over gender, meaning mainly men had been hired previously. Two institutional review boards were involved and suggested the need to address the potential rare side effects of SP and concerns that community IPTp would not detract from ANC clinic attendance.
Since district and clinic level health staff will be involved in implementing the program using the national CBHW program, lessons learned from this effort to expand the work of CBHWs in preventing malaria in pregnancy should be applicable and adaptable to the whole country.
CHW &IPTp &Malaria in Pregnancy Bill Brieger | 05 Nov 2017
Improving Early ANC Attendance and IPT Uptake through Community Health Volunteers
 Community health workers are playing an increasing role in maternal health programming. Augustine Ngindu, Susan Ontiri, Gathari Ndirangu, Beth Barasa, Evans Nyapada, David Omoit, Johnstone Akatu, and Mildred Mudany of The Matewrnal and Child Survival Program, The Kenya Ministry of Health and Jhpiego share their experiences in Kenya at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene in Baltimore on 2017-11-06. If you are in Baltimore, hear more at Scientific Session 13. Below is an abstract of their presentation
Community health workers are playing an increasing role in maternal health programming. Augustine Ngindu, Susan Ontiri, Gathari Ndirangu, Beth Barasa, Evans Nyapada, David Omoit, Johnstone Akatu, and Mildred Mudany of The Matewrnal and Child Survival Program, The Kenya Ministry of Health and Jhpiego share their experiences in Kenya at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene in Baltimore on 2017-11-06. If you are in Baltimore, hear more at Scientific Session 13. Below is an abstract of their presentation
 Kenya adopted the use of intermittent preventive treatment with sulfadoxine pyrimethamine in 1998 but the proportion of pregnant women receiving at least two doses (22% (2010) and 56% (2015) has remained below the national target of 80%. In 2015, the country adopted an IPTp3 indicator for monitoring IPTp uptake; that year, the proportion of women taking at least 3 doses was 38% (2015).
Kenya adopted the use of intermittent preventive treatment with sulfadoxine pyrimethamine in 1998 but the proportion of pregnant women receiving at least two doses (22% (2010) and 56% (2015) has remained below the national target of 80%. In 2015, the country adopted an IPTp3 indicator for monitoring IPTp uptake; that year, the proportion of women taking at least 3 doses was 38% (2015).
Some of the factors leading to low IPTp coverage include poor knowledge on the need for early antenatal care (ANC), distances to health facilities, sociocultural practices and a lack of financial resources. In 2012, community health volunteers (CHVs) were enlisted through a pilot program in one county to deliver messages aimed at increasing the proportion of women starting ANC ? 20 weeks of gestation and thus expand the proportion of women receiving IPTp early in the second trimester.
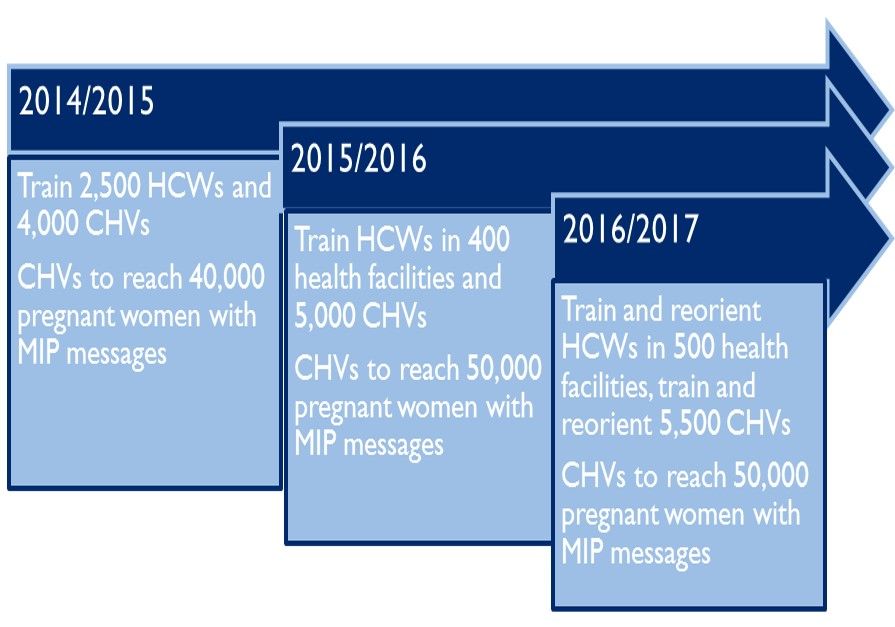
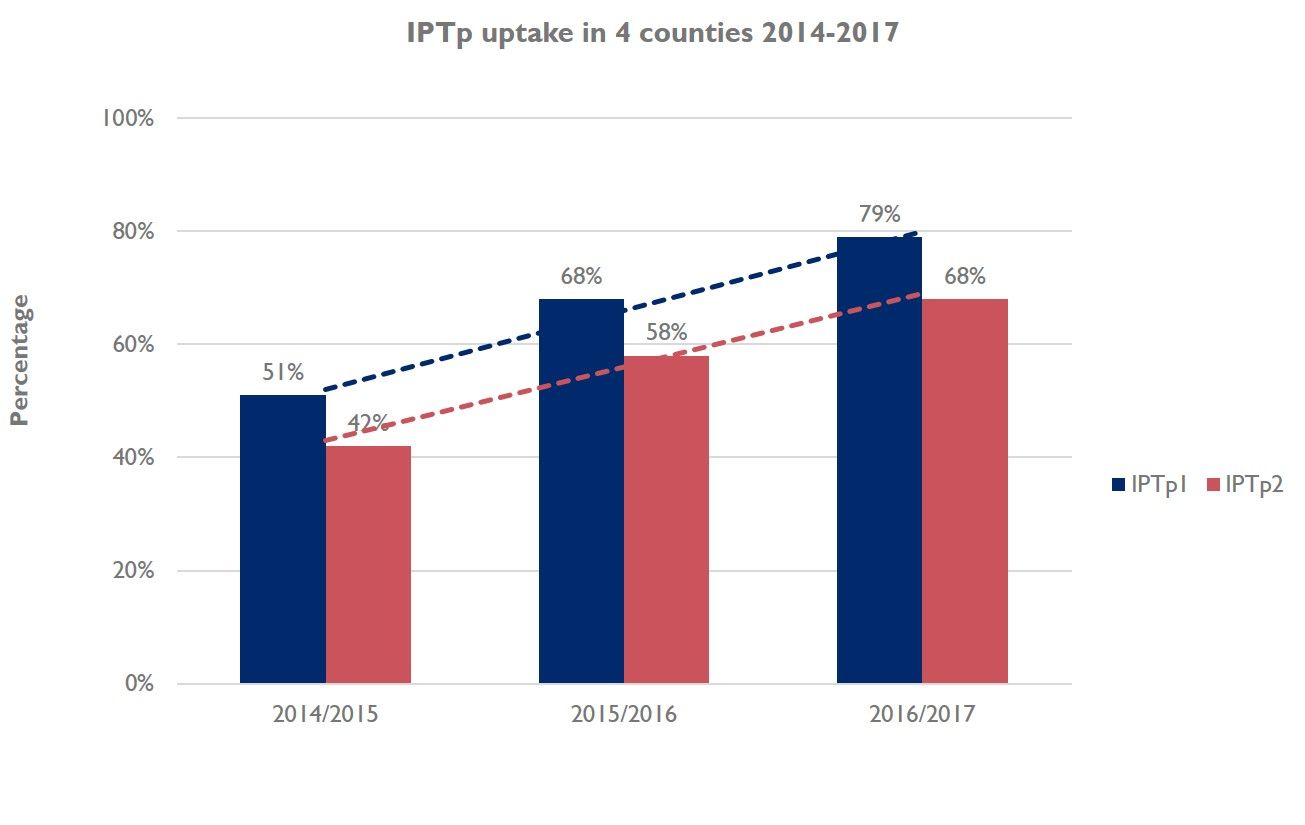 A community survey in 2013 showed an increase in IPTp2 from 22% in 2010 to 63%. The practice was considered a success story, and was subsequently replicated in 30 sub-counties, in 4 out of 14 malaria endemic counties. The rollout involved training of 9,042 CHVs, in 761 community units. Between 2015 and 2016, the CHVs reached 86,433 women with MiP messages. During this time, there was an average increase in IPTp1 from 51% to 68%, and IPTp2 increased from 42% to 55% (p? 0.001). This could be attributed to early ANC attendance, which increased from 32% to 48% in the same period.
A community survey in 2013 showed an increase in IPTp2 from 22% in 2010 to 63%. The practice was considered a success story, and was subsequently replicated in 30 sub-counties, in 4 out of 14 malaria endemic counties. The rollout involved training of 9,042 CHVs, in 761 community units. Between 2015 and 2016, the CHVs reached 86,433 women with MiP messages. During this time, there was an average increase in IPTp1 from 51% to 68%, and IPTp2 increased from 42% to 55% (p? 0.001). This could be attributed to early ANC attendance, which increased from 32% to 48% in the same period.
The use of CHVs to sensitize pregnant women to start IPTp early in the second trimester and continue with scheduled ANC visits increases the probability that women will receive the recommended IPTp-SP doses. The rollout of the practice to other malaria endemic counties is likely to have contributed to increase in IPTp uptake in the four target counties.
.![]()