Community &Health Information &IPTp &Malaria in Pregnancy &Monitoring &Procurement Supply Management Bill Brieger | 01 Nov 2018
Setting the Stage to Introduce a Groundbreaking Community Approach to Prevent Malaria in Pregnancy in Sub-Saharan Africa
 Maya Tholandi, Lolade Oseni, Anne McKenna, Herbert Onuoha, Solofo Razakamiadana, Elsa Nhantumbo, Alain Mikato, Elaine Roman of Jhpiego and the Johns Hopkins Bloomberg School of Public Health shared important Baseline Readiness Assessment Findings from Democratic Republic of the Congo, Mozambique, Madagascar, and Nigeria from the UNITAID-supported TIPTOP on Intermittent Preventive Treatment of malaria in pregnancy at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene as seen below.
Maya Tholandi, Lolade Oseni, Anne McKenna, Herbert Onuoha, Solofo Razakamiadana, Elsa Nhantumbo, Alain Mikato, Elaine Roman of Jhpiego and the Johns Hopkins Bloomberg School of Public Health shared important Baseline Readiness Assessment Findings from Democratic Republic of the Congo, Mozambique, Madagascar, and Nigeria from the UNITAID-supported TIPTOP on Intermittent Preventive Treatment of malaria in pregnancy at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene as seen below.
Intermittent preventive treatment of malaria in pregnancy (IPTp) is unacceptably low in most of sub-Saharan Africa. A Jhpiego-led consortium is implementing the Transforming Intermittent Preventive Treatment for Optimal Pregnancy (TIPTOP) project, which supports community distribution of quality-assured sulfadoxine-pyrimethamine (SP).
 TIPTOP aims to increase IPTp3 coverage from 19% to 50% of eligible pregnant women in project areas in Democratic Republic of the Congo (DRC), Madagascar, Mozambique, and Nigeria. The project, operating from 2017 to 2022, provides quality-assured SP, promotes community awareness, and supports supervision and coordination efforts between health facilities and community health workers (CHWs).
TIPTOP aims to increase IPTp3 coverage from 19% to 50% of eligible pregnant women in project areas in Democratic Republic of the Congo (DRC), Madagascar, Mozambique, and Nigeria. The project, operating from 2017 to 2022, provides quality-assured SP, promotes community awareness, and supports supervision and coordination efforts between health facilities and community health workers (CHWs).
In 2017, a baseline assessment examined facility readiness for malaria in pregnancy management, antenatal care (ANC) provider knowledge, CHW characteristics and health facility linkages, and health management information system (HMIS) quality. TIPTOP assessed 140 facilities and interviewed 175 ANC providers and 67 CHW supervisors.
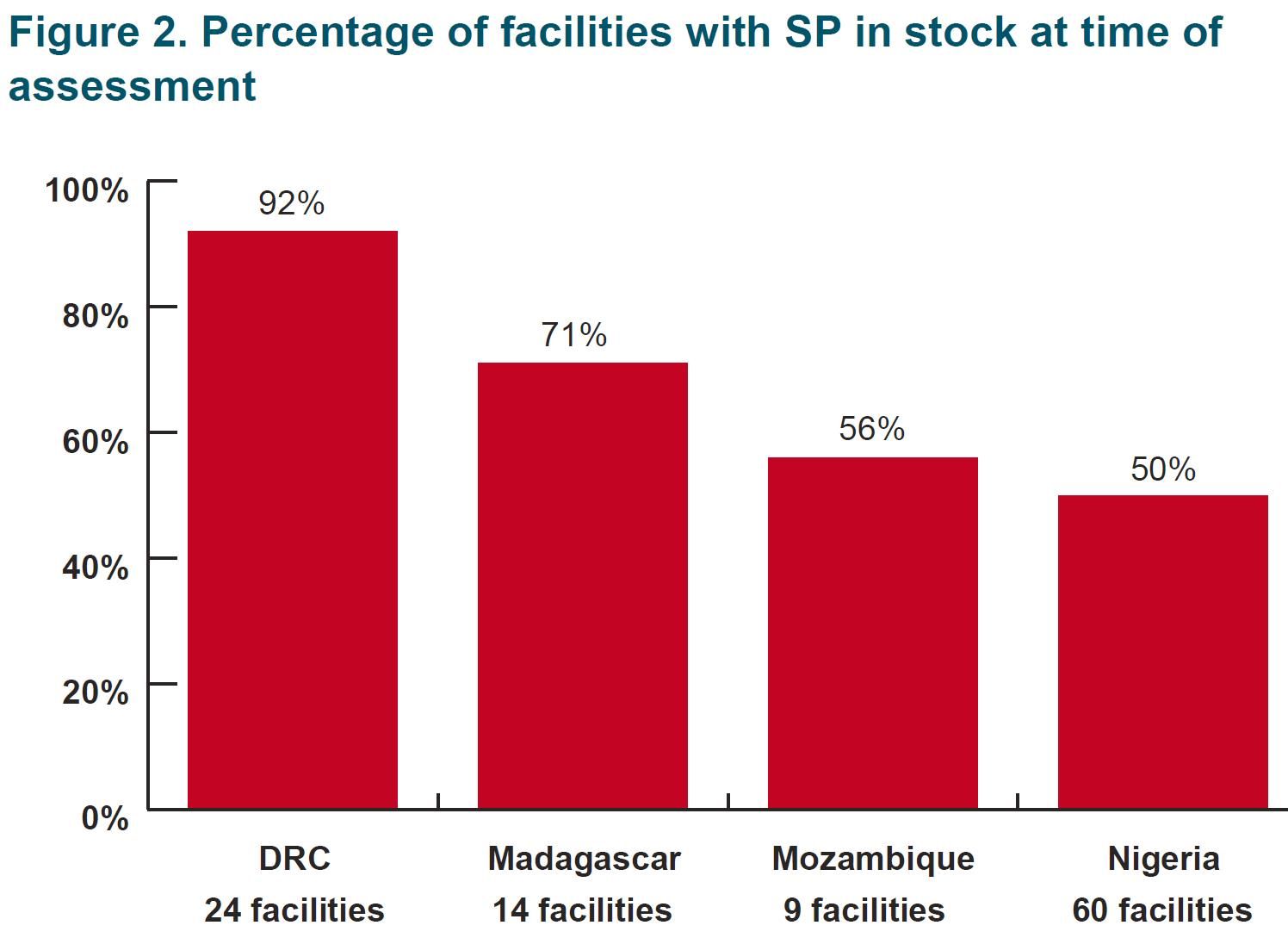
 At project startup, the teams examined SP stock, ANC providers and CHW availability. SP Stock assessment showed a disparate stock maintenance processes and stock-out next steps indicate lack of a coherent and consistent approach to stock monitoring. In half of all cases, caregivers offer a prescription when stock is not available in the facility, with smaller numbers requesting.
At project startup, the teams examined SP stock, ANC providers and CHW availability. SP Stock assessment showed a disparate stock maintenance processes and stock-out next steps indicate lack of a coherent and consistent approach to stock monitoring. In half of all cases, caregivers offer a prescription when stock is not available in the facility, with smaller numbers requesting.
Among ANC providers, 80% on average correctly reported that at least three doses of IPTp are recommended. On average, 64% correctly responded that SP should be initiated in the second trimester. Out of the 170 providers interviewed across countries, only five knew all the key signs of suspected malaria.
 A low numbers of CHWs in some districts may limit their reach and capacity. Inadequate CHW education and ANC familiarity may diminish training effectiveness. In particular, low numbers of female CHWs may decrease community acceptance and pregnant women’s acceptability of receiving IPTp from CHWs.
A low numbers of CHWs in some districts may limit their reach and capacity. Inadequate CHW education and ANC familiarity may diminish training effectiveness. In particular, low numbers of female CHWs may decrease community acceptance and pregnant women’s acceptability of receiving IPTp from CHWs.
Data Quality and Availability from the routine services would affect monitoring of interventions. Over-reporting of ANC contacts and IPTp service provision is a data quality challenge. The HMISs in Nigeria and Mozambique record IPTp3 provision, but only at the local level. Supervising facilities do not always review data before HMIS entry for accuracy.
Concerning Monitoring and Evaluation System Components, Mozambique’s HMIS is the strongest of the four countries in terms of linking to the national system, current tools and reporting forms available in the facilities, and providers reporting an understanding of indicators and data reporting processes. Nigerian facilities had limited knowledge of indicators and their definitions, despite this information being available in Federal Ministry of Health-provided registers. Madagascar struggled with indicator definitions and data management processes. DRC faced the most challenges: Tools and reporting forms were not available in health facilities, and there were limited monitoring and evaluation structures and processes.
 In Conclusion, Results from the baseline assessment are Informing efforts to improve data quality and CHW facility data flow in TIPTOP implementation areas.
In Conclusion, Results from the baseline assessment are Informing efforts to improve data quality and CHW facility data flow in TIPTOP implementation areas.  There is need to strengthen ANC provider knowledge through TIPTOP-supported trainings. One also needs to address CHW variation by country and support health facilities to monitor their SP stock. These findings are being shared with ministries of health and key stakeholders to inform malaria implementation and data quality efforts.
There is need to strengthen ANC provider knowledge through TIPTOP-supported trainings. One also needs to address CHW variation by country and support health facilities to monitor their SP stock. These findings are being shared with ministries of health and key stakeholders to inform malaria implementation and data quality efforts.
CHW &Community &IPTp &Malaria in Pregnancy Bill Brieger | 29 Oct 2018
Community Health Workers Can Enhance Coverage of Intermittent Preventive Treatment of Malaria in Pregnancy and Promote Antenatal Attendance
Among the poster presentations on malaria from Jhpiego, the President’s Malaria Initiative and partners at the 2018 ASTMH Annual Meeting, WR Brieger, J Tiendrebeogo, O Badolo, M Dodo, D Burke, K Vibbert, SJ Youll, and JR Gutman shared the findings from a 15-month intervention that tested the ability of community health workers to deliver intermittent preventive treatment of malaria in pregnancy in 3 districts in Burkina Faso. Please check out the poster and talk to one of the co-investigators at Poster Session A on Monday 29 October. Their results are found below.
Malaria in pregnancy is responsible for a substantial proportion of low-birthweight and stillborn infants in sub-Saharan Africa. To prevent this, the World Health Organizatio n (WHO) recommends that pregnant women receive intermittent preventive treatment of malaria in pregnancy (IPTp) using sulfadoxine-pyrimethamine. Specifically, WHO recommends an optimal three or more doses (e.g., IPTp3, IPTp4).
n (WHO) recommends that pregnant women receive intermittent preventive treatment of malaria in pregnancy (IPTp) using sulfadoxine-pyrimethamine. Specifically, WHO recommends an optimal three or more doses (e.g., IPTp3, IPTp4).
In stable malaria endemic countries, IPTp coverage remains unacceptably low, at around 19% for IPTp3. Community IPTp might provide an answer. Community delivery can improve coverage as seen in previous study in Nigeria and Malawi, but its effects on antenatal care (ANC) attendance have been mixed. Additional data are needed to determine whether delivery of IPTp-SP by community health workers (CHWs) is effective and does not detract from ANC attendance. Hence the Burkina Faso intervention was designed and implemented
The study piloted community delivery of IPTp (c-IPTp) in three districts of Burkina Faso  with high malaria transmission: Po, Ouargaye, and Batie. Four health facilities per district were randomly selected to participate (two intervention and two control).
with high malaria transmission: Po, Ouargaye, and Batie. Four health facilities per district were randomly selected to participate (two intervention and two control).
In 2017, following a baseline household survey of women who recently became pregnant, implementation of c-IPTp began in intervention areas by existing CHWs trained and supervised by health staff. At Baseline in each of the three study districts, four health centers (CSPSs) and the villages in their catchment areas were selected—two as intervention and two as control. A random sample of 374 women who had been pregnant within the last 9 months were interviewed in CSPS catchment villages. There were no significant differences in ANC attendance (ANC1=90%, ANC4=62%) or IPTp coverage between intervention and control areas:
- IPTp3 was 81% (intervention) and 86% (control).
- IPTp4 was 22% (intervention) and 16% (control).
 The Intervention consisted of building on Burkina Faso’s existing CHWs. They were trained and monitored by clinic staff. The CHWs encouraged women to attend the first ANC visit to obtain IPTp1. Then the CHWs provided monthly doses of IPTp, submitted monthly reports, and continued to promote ANC. ANC attendance and IPTp uptake were monitored through monthly clinic and CHW reports. The catchment area populations were roughly the same, and monitoring showed that the additional provision of IPTp by CHWs resulted in more women being reached while at the same time ANC attendance remained high.
The Intervention consisted of building on Burkina Faso’s existing CHWs. They were trained and monitored by clinic staff. The CHWs encouraged women to attend the first ANC visit to obtain IPTp1. Then the CHWs provided monthly doses of IPTp, submitted monthly reports, and continued to promote ANC. ANC attendance and IPTp uptake were monitored through monthly clinic and CHW reports. The catchment area populations were roughly the same, and monitoring showed that the additional provision of IPTp by CHWs resulted in more women being reached while at the same time ANC attendance remained high.
An endline su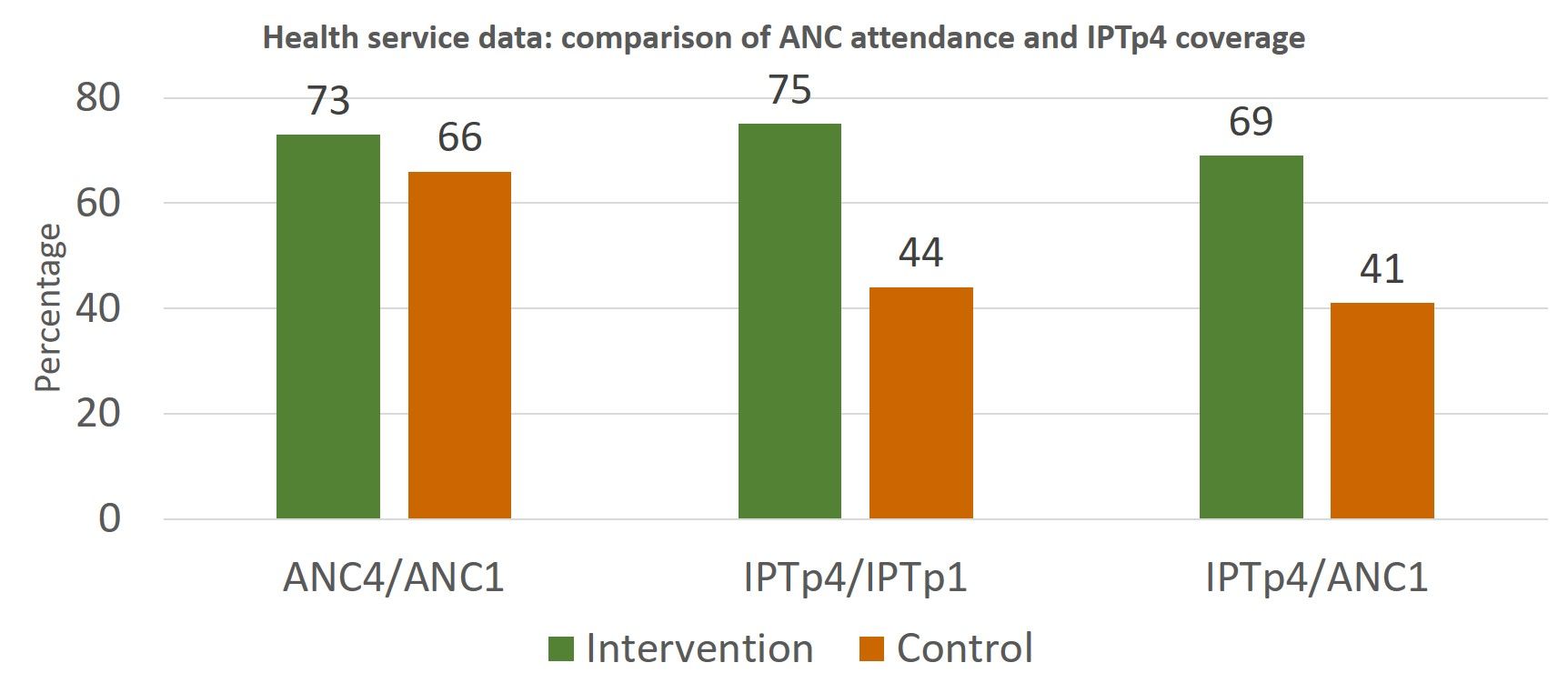 rvey was conducted after 18 months of implementation. Changes over time were compared between baseline and endline in intervention versus control villages. Attendance at ANC1 and ANC4 increased in both groups between baseline and endline but was significantly better for the intervention group. Likewise, coverage of IPTp3 and IPTp4 increased between baseline and endline for intervention and control women, but the difference was significant only in the intervention areas.
rvey was conducted after 18 months of implementation. Changes over time were compared between baseline and endline in intervention versus control villages. Attendance at ANC1 and ANC4 increased in both groups between baseline and endline but was significantly better for the intervention group. Likewise, coverage of IPTp3 and IPTp4 increased between baseline and endline for intervention and control women, but the difference was significant only in the intervention areas.
 Monthly monitoring of CHW and ANC registers and the household surveys both documented that community delivery of IPTp resulted in the desired increased uptake of services without detracting from ANC attendance. Community IPTp may be a promising strategy to improve coverage of IPTp.
Monthly monitoring of CHW and ANC registers and the household surveys both documented that community delivery of IPTp resulted in the desired increased uptake of services without detracting from ANC attendance. Community IPTp may be a promising strategy to improve coverage of IPTp.
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Announcement &Case Management &CHW &Community &Ebola &Infection Prevention &IPTp &Malaria in Pregnancy &Quality of Services Bill Brieger | 29 Oct 2018
Malaria Featured in Jhpiego Sessions at ASTMH 2018

Below is a list of Jhpiego Sessions at this week’s American Society of Tropical Medicine Annual Meeting in New Orleans (28 October-1 November). Please attend if you are at the conference:
![]() Poster Session A, Monday, October 29 (Posters in Marriott Grand Ballroom – 3rd Floor )
Poster Session A, Monday, October 29 (Posters in Marriott Grand Ballroom – 3rd Floor )
- Poster Number 098: Performance of community health workers in providing integrated community case management services (iCCM) in 8 districts of Rwanda
- Poster 380: Contribution of quarterly malaria data review and validation to data quality and malaria services Improvement
- Poster LB-5117: Community based health workers can enhance coverage of intermittent preventive treatment of malaria in pregnancy and promote antenatal attendance
Poster Session B, Tuesday 30 October
- Poster 1088: Assessing organizational capacity to deliver quality malaria services in rural Liberia
- Poster 1092: Contribution of IMC project in transforming the face of malaria control for vulnerable populations in Burkina Faso
- Poster 1093: Malaria response plan in times of high transmission: An approach to improving the quality of hospital malaria management
- Poster 1111: Setting the stage to introduce a ground breaking approach to prevent malaria in pregnancy in Sub-Saharan Africa: baseline-readiness assessment findings from Democratic Republic of Congo, Mozambique, Madagascar, and Nigeria
- Poster 1337: Institutionalizing infection prevention and control practices in health facilities in Liberia following the Ebola epidemic
 Scientific Session 87, Tuesday, 1:45 – 3:30 p.m. Marriott – La Galerie 1 & 2 – 2nd Floor: Improving procurement and redeployment of district level malaria commodities using SMS and web mapping in Madagascar
Scientific Session 87, Tuesday, 1:45 – 3:30 p.m. Marriott – La Galerie 1 & 2 – 2nd Floor: Improving procurement and redeployment of district level malaria commodities using SMS and web mapping in Madagascar
Poster Session C, Wednesday 31 October
- Poster 1816: Experiences and perceptions of care seeking for febrile illness among caregivers and providers in 8 districts of Madagascar
- Poster 1818: Improving adherence to national malaria treatment guidelines by village health workers in selected townships through a low-dose, high-frequency training approach
- Poster 1819: Improving malaria case management through national roll-out of Malaria Service and Data Quality Improvement (MSDQI): A Case study from Tanzania
- Poster 1820: Collaborative quality improvement framework to support data quality improvement, experience from 10 collaborative facilities in Uganda
- Poster 1821: Using malaria death audits to improve malaria case management and prevent future malaria related preventable deaths
- Poster 1833: Multiple approaches for malaria case management in the struggle to reach pre-elimination of malaria.
Scientific Session 182, Thursday, November 1, 10:15 am – 12:00 p.m. Marriott – Balcony I,J,K – 3rd Floor: Seasonal malaria chemoprevention, an effective intervention for reducing malaria morbidity and mortality
Malaria in Pregnancy &Neonatal Bill Brieger | 03 Jul 2018
Could a Triple-Hit Hypothesis Explain the Pathway from Malaria in Pregnancy to Adverse Infant Neurodevelopmental Outcomes?
Harriet L. S. Lawford 1 , Mary C. Ghazawy 1 , Tessa R. Donaldson 2 , Jack Donaldson 3 , and Samudragupta Bora 1 shared their researct at the Malaria World Congress in Melbourne this week and present their findings below.
- Mothers, Babies and Women’s Health Program, Mater Research Institute, Faculty of Medicine, The University of Queensland, Australia
- Department of Psychology, University of Canterbury, Christchurch, New Zealand
- Dunedin School of Medicine, University of Otago, Dunedin, New Zealand
![]() Each year, millions of pregnant women in malaria-endemic areas are at risk of Plasmodium falciparum infection and the development of placental malaria. Given that malaria in pregnancy is known to contribute to a number of perinatal and infant deaths, this suggests that a significant proportion of live-births may have been exposed to placental malaria in utero. Whilst the neurodevelopmental consequences of cerebral malaria in children have been widely documented, there has been little focus on the impact of placental malaria on infant neurodevelopment.
Each year, millions of pregnant women in malaria-endemic areas are at risk of Plasmodium falciparum infection and the development of placental malaria. Given that malaria in pregnancy is known to contribute to a number of perinatal and infant deaths, this suggests that a significant proportion of live-births may have been exposed to placental malaria in utero. Whilst the neurodevelopmental consequences of cerebral malaria in children have been widely documented, there has been little focus on the impact of placental malaria on infant neurodevelopment.
 This research gap is critical to address. Placental malaria is associated with adverse birth outcomes including preterm birth, low birthweight and intrauterine growth restriction, which themselves are well recognized independent risk factors for adverse short-term and long-term neurodevelopment. Furthermore, the additive effects of prenatal environmental and social factors on infant neurodevelopment remain poorly understood. Hence, we propose a Triple-Hit Hypothesis to explain the potential pathway from placental malaria to poor infant neurodevelopmental outcomes.
This research gap is critical to address. Placental malaria is associated with adverse birth outcomes including preterm birth, low birthweight and intrauterine growth restriction, which themselves are well recognized independent risk factors for adverse short-term and long-term neurodevelopment. Furthermore, the additive effects of prenatal environmental and social factors on infant neurodevelopment remain poorly understood. Hence, we propose a Triple-Hit Hypothesis to explain the potential pathway from placental malaria to poor infant neurodevelopmental outcomes.

As per our hypothesis, prenatal socioeconomic, environmental and maternal factors represent the first-hit that influences the risk of developing placental malaria. Poverty and low socioeconomic status are known to increase the likelihood of malaria infection, as well as negatively influence access to and uptake of malaria treatment and prevention tools. The use of sulfadoxine-pyrimethamine in resistant areas has been seen to increase placental inflammation and parasitisation, as well as the proportion of resistant parasites, which can lead to more severe placental infection. Lastly, maternal factors, including parity and age, are known to influence the likelihood of placental malaria; the risk of placental malaria among primigravidae is 2-4 times higher than multigravidae, and is seen to increase with decreasing age
The second-hit is represented by the direct activation of maternal immuno-inflammatory factors in response to placental malaria and resultant placental dysfunction. The infiltration of maternal immune and inflammatory factors and placental histopathological changes, such as thickening of the trophoblastic basement membrane, can cause mechanical blockage of materno-foetal oxygen and nutrient exchange, leading to hypoxic conditions and oxidative stress as well as impaired placental vascularisation. Evidence from the literature also suggests activation of complement and a TH1/TH2 imbalance, further contributing to the maternal immunological response.
The severity of placental infection represents the third-hit, wherein the risk of poor neurodevelopment is indirectly impacted by the increased likelihood of adverse birth outcomes associated with infection. Low birthweight, preterm birth and intrauterine growth restriction are themselves risk factors for adverse foetal brain development, and adversities include long-term volumetric brain reductions and cognitive, motor and behavioural deficits. Furthermore, research has shown a direct link between maternal inflammation, placental pathology and poor neurological and neurodevelopmental outcomes.
Taken together, this involvement of both direct and indirect pathways culminate in a unique foetal phenotype, where not only do we expect to see the adverse birth outcomes commonly associated with placental malaria, but also adversities including increased risks of neurological, cognitive and behavioural deficits that may impact the quality of life in this high-risk population. Validation of the link between placental malaria and adverse neurodevelopment is needed.
For feedback and any further information, please contact: harriet.lawford@mater.uq.edu.au.
Health Systems &IPTp &Malaria in Pregnancy &Neonatal &Procurement Supply Management Bill Brieger | 03 Jul 2018
Progress on Malaria in Pregnancy in 12 PMI Focus Countries
The challenges of implementing programs to control malaria in pregnancy based on experiences with US President’s Malaria Initiative Countries was presented at the Malaria World Congress in Melbourne this week. The team included Katherine Wolf, MCSP/Jhpiego, Marianne Henry, PMI/USAID, Lia Florey, PMI/USAID, Gabrielle Conecker, MCSP/Jhpiego, Betsy Hendrickson, MCSP/Jhpiego, Katherine Lilly, MCSP/Jhpiego, Nicholas
Furtado, GFATM, Maria Petro, GFATM, Susan Youll, PMI/USAID, and Julie Gutman, PMI/CDC, and their findings are shared below.
 What is the danger of malaria in pregnancy (MiP)? Each year MIP is responsible for 20% of stillbirths in Sub-Saharan Africa, 100,000 Newborn deaths globally, 11% of newborn deaths in Africa and 10,000 maternal deaths globally. Four interventions are aimed at MIP, Intermittent Preventive Treatment in Pregnancy (IPTp), consistent use of insecticide treated nets, effective diagnosis and treatment and low-dose folic acid during antenatal care. IPTp with sulfadoxine-pyrimethamine reduces low birth weight by 29%, severe maternal anemia by 38% and neonatal mortality by 31%. What can be done?
What is the danger of malaria in pregnancy (MiP)? Each year MIP is responsible for 20% of stillbirths in Sub-Saharan Africa, 100,000 Newborn deaths globally, 11% of newborn deaths in Africa and 10,000 maternal deaths globally. Four interventions are aimed at MIP, Intermittent Preventive Treatment in Pregnancy (IPTp), consistent use of insecticide treated nets, effective diagnosis and treatment and low-dose folic acid during antenatal care. IPTp with sulfadoxine-pyrimethamine reduces low birth weight by 29%, severe maternal anemia by 38% and neonatal mortality by 31%. What can be done?
- Scale-up and full coverage of the WHO lifesaving interventions
- Promote early and regular ANC
- Preserve SP efficacy by avoiding its use for treating clinical cases of malaria
- Reserve SP stocks for IPTp at ANC clinics
 Methodology for MiP country review: Initial survey took place in 23 PMI countries. PMI resident advisors were surveyed, Qualitative and quantitative responses were collected and Input from NMCP/partners was obtained. Country selection resulted in 12 that were Tiptop-implementing countries, represented Geographic diversity, had varied IPTp coverage, and made clear progress or best practices to share.
Methodology for MiP country review: Initial survey took place in 23 PMI countries. PMI resident advisors were surveyed, Qualitative and quantitative responses were collected and Input from NMCP/partners was obtained. Country selection resulted in 12 that were Tiptop-implementing countries, represented Geographic diversity, had varied IPTp coverage, and made clear progress or best practices to share.
Desk review including HMIS and house hold survey data, current studies and recent assessments, Selected interviews with PMI resident advisors, Jhpiego field staff and current/former NMCP staff. Analysis was a Review and clarification of qualitative and qualitative data.
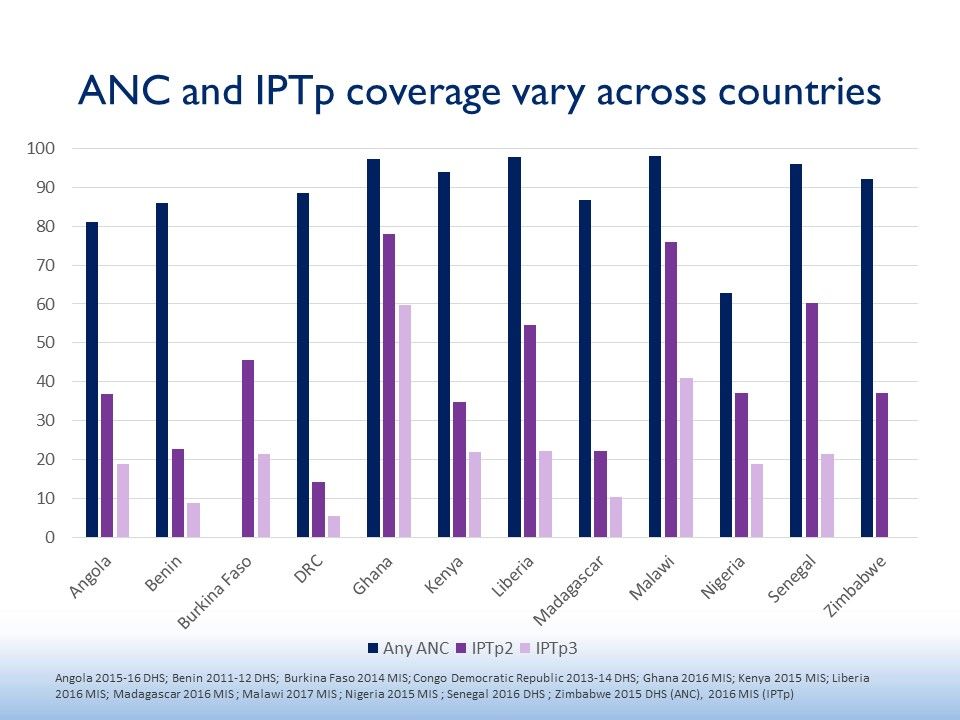
 The 12 countries included Angola, Benin, Burkina Faso, DRC, Ghana, Kenya, Liberia, Madagascar, Malawi, Nigeria, Senegal, and Zimbabwe (see map). The figure shows that none of these attained 80% of 2 doses of IPTp. The current recommendations are for monthly dosages from the 13th week of pregnancy. Often less that half of those receiving IPTp2 also got IPTp3.
The 12 countries included Angola, Benin, Burkina Faso, DRC, Ghana, Kenya, Liberia, Madagascar, Malawi, Nigeria, Senegal, and Zimbabwe (see map). The figure shows that none of these attained 80% of 2 doses of IPTp. The current recommendations are for monthly dosages from the 13th week of pregnancy. Often less that half of those receiving IPTp2 also got IPTp3.
Several health systems findings helped explain the IPT results. For Policy & Implementation, Countries reporting strong, coordinated leadership delivered
high IPTp coverage. With Community Engagement, countries reported a diversity of approaches to community health promotion and service delivery.
Concerning Service Delivery, Many countries struggle to implement MiP policies consistently and with quality in the private sector. Commodities were a challenge. Some countries continue to struggle with SP stockouts at facility level, whether ongoing or episodic. Monitoring and Evaluation processes need to catch up. Countries’ routine information systems are transitioning from tracking IPTp2 to IPTp3.
The team offered several Recommendations.
- Strengthen consistency of IPTp policies across malaria and reproductive health programs
- Scale up of evidence-based country appropriate
community engagement strategies - Alleviation of supply chain bottlenecks at peripheral level
- Inclusion and harmonization of key MIP indicators in routine information systems
For more information please visit www.mcsprogram.org, facebook.com/MCSPglobal and twitter.com/MCSPglobal
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative AgreementAID-OAA-A-14-00028. The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government.
IPTp &Malaria in Pregnancy &Maternal Health &Reproductive Health Bill Brieger | 28 Jun 2018
Intermittent Preventive Treatment of Malaria In Pregnancy in Tanzania
Intermittent Preventive Treatment of malaria in pregnancy (IPTp) using sulfadoxin e-pyrimethamine (SP) has been a long standing intervention to protect pregnant women and their unborn children from the dangerous effects of malaria in stable transmission settings. Placental malaria deprives the fetus of nutrients leading to low birth weight, still birth and miscarriages. The mother herself suffers anemia and potentially, death.
e-pyrimethamine (SP) has been a long standing intervention to protect pregnant women and their unborn children from the dangerous effects of malaria in stable transmission settings. Placental malaria deprives the fetus of nutrients leading to low birth weight, still birth and miscarriages. The mother herself suffers anemia and potentially, death.
There had always been a challenge to getting pregnant women to obtain at least two doses of IPTp-SP due to a variety of factors ranging from health system lapses to late antenatal care attendance by mothers. This phenomenon of dropping out of multi-contact interventions is not uncommon and seen equally in programs such as childhood immunization. Therefore when the World Health Organization raised the bar and recommended IPTp starting in the 13th week of pregnancy and monthly thereafter, the challenge of providing three or more doses arose.
 The Malaria Indicator Surveys (MIS) and the Demographic and Health Surveys (DHS) are an ideal was to trace the progress of malaria intervention over multiple years. With the release of the preliminary results of 2017 Tanzania MIS it is now possible to track this service from over a decade. The Attached chart, using MIS/DHS reports shows that so far Tanzania has not come near achieving 80% coverage of this indicator. While there had been major increases over recent years, reports of IPTp coverage in 2017 show only 56% of recently pregnant women received at least two doses, and only 26% received three or more.
The Malaria Indicator Surveys (MIS) and the Demographic and Health Surveys (DHS) are an ideal was to trace the progress of malaria intervention over multiple years. With the release of the preliminary results of 2017 Tanzania MIS it is now possible to track this service from over a decade. The Attached chart, using MIS/DHS reports shows that so far Tanzania has not come near achieving 80% coverage of this indicator. While there had been major increases over recent years, reports of IPTp coverage in 2017 show only 56% of recently pregnant women received at least two doses, and only 26% received three or more.
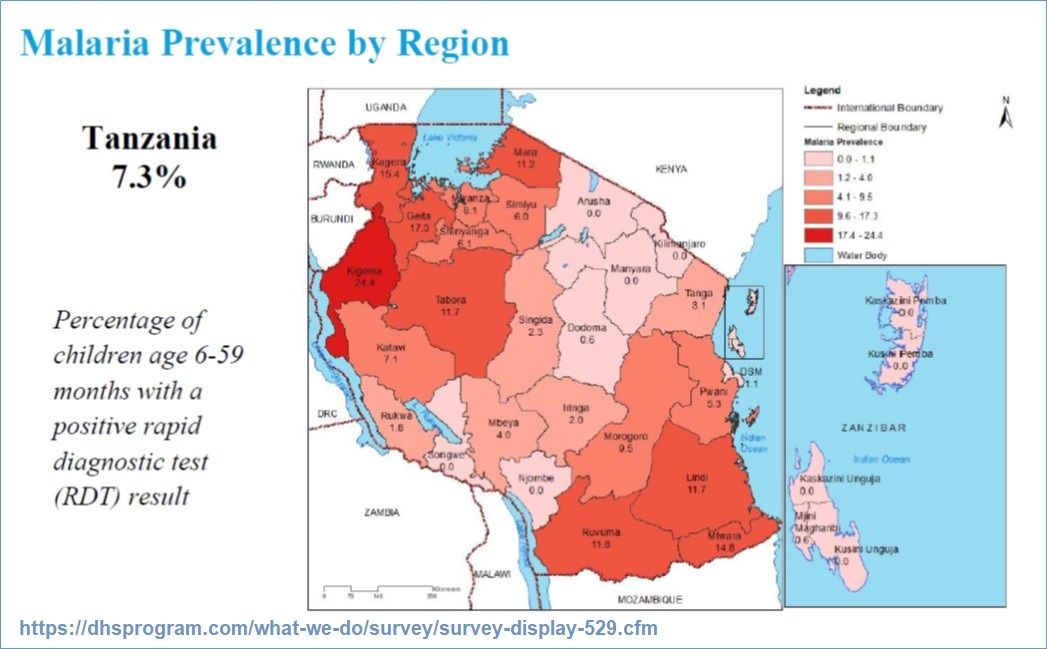 It should be noted that countries are beginning to stratify their interventions according to available transmission data. Therefore as noted in the US President’s Malaria Initiative Malaria Operations Plan for 2018, Zanzibar where transmission is low, has stopped IPTp and focuses on prompt and appropriate case management, while the mainland of Tanzania continues with all MIP interventions. Of interest is the most recent child prevalence map found in the 2017 MIS results that shows other parts of the mainland may also be approaching very low transmission.
It should be noted that countries are beginning to stratify their interventions according to available transmission data. Therefore as noted in the US President’s Malaria Initiative Malaria Operations Plan for 2018, Zanzibar where transmission is low, has stopped IPTp and focuses on prompt and appropriate case management, while the mainland of Tanzania continues with all MIP interventions. Of interest is the most recent child prevalence map found in the 2017 MIS results that shows other parts of the mainland may also be approaching very low transmission.
Moving forward it will be useful if Tanzania and other endemic countries not only gather epidemiological data to help stratify appropriate interventions (as suggested in the WHO malaria elimination framework), but go further to focus reporting by strata. That said, the health system and community difficulties in achieving high IPTp coverage wherever it is appropriate will remain a challenge if services remain based in static health facilities. Community roles must be explored.
CHW &Health Workers &IPTp &Malaria in Pregnancy Bill Brieger | 19 Apr 2018
Acceptance of the Contribution of Community-Based Health Workers (CBHWs) to Improving Prevention of Malaria in Pregnancy in Burkina Faso by Health Center Staff
 Efforts are underway to test the a community-based system for providing IPTp to pregnant women in Burkina Faso as a means of increasing coverage. Justin Tiendrebeogo, Ousmane Badolo, Mathurin Dodo, Yacouba Savadogo, Danielle Burke, Susan Youll, and William Brieger share a formative study among health staff concerning their perceptions of the ability of Community Based Health Workers to provide increased doses. This was presented at the 7th Multilateral Initiative for Malaria Conference in Dakar. Below are the findings.
Efforts are underway to test the a community-based system for providing IPTp to pregnant women in Burkina Faso as a means of increasing coverage. Justin Tiendrebeogo, Ousmane Badolo, Mathurin Dodo, Yacouba Savadogo, Danielle Burke, Susan Youll, and William Brieger share a formative study among health staff concerning their perceptions of the ability of Community Based Health Workers to provide increased doses. This was presented at the 7th Multilateral Initiative for Malaria Conference in Dakar. Below are the findings.
The Burkina Faso Ministry of Health, with support from its partners, initiated a study on the feasibility of increasing provision of intermittent preventive malaria treatment in pregnant women (IPTp) with sulfadoxine-pyrimethamine (SP). Existing community-based health workers (CBHWs) were enlisted to deliver the third and fourth doses recommended by the World Health Organization. Currently, only facility-based health care providers give SP, and women in rural areas have trouble accessing health facilities for the medicine.
Using CBHWs has the potential to reach more women with a greater number of doses of IPTp-SP. Direct training and supervision of CBHWs is the responsibility of frontline health care staff, including antenatal care (ANC) providers. Therefore, to ensure a successful rollout of community delivery of IPTp, it is crucial that these staff accept the new roles of CBHWs. This baseline study was conducted to learn the frontline staff’s views about existing and proposed CBHW activities.
 Study’s Geographic Areas. Three districts (Batié, Pô, and Ouargaye) in the southern part of Burkina Faso. Twelve centre de santé et de promotion sociale (health and social promotion centers [CSPS]) were selected in Ouargaye, Pô, and Batié Health Districts. In each district, two CSPS were randomly assigned as intervention catchment areas, for a total of six centers. Then using matching criteria, the remaining six CSPS were designated as control sites.
Study’s Geographic Areas. Three districts (Batié, Pô, and Ouargaye) in the southern part of Burkina Faso. Twelve centre de santé et de promotion sociale (health and social promotion centers [CSPS]) were selected in Ouargaye, Pô, and Batié Health Districts. In each district, two CSPS were randomly assigned as intervention catchment areas, for a total of six centers. Then using matching criteria, the remaining six CSPS were designated as control sites.
 Health Worker Interviews were conducted among a total of 35 CSPS staff: 23 were men, and 12 were women. Semi-structured interview guides were used in this formative study. Open-ended questions sought the views of ANC providers and CBHW supervisors about the current work of CBHWs and the feasibility of using this health cadre to administer IPTp to pregnant women. The Study sought to understand provider opinions to design an IPTp-SP intervention involving CBHWs.
Health Worker Interviews were conducted among a total of 35 CSPS staff: 23 were men, and 12 were women. Semi-structured interview guides were used in this formative study. Open-ended questions sought the views of ANC providers and CBHW supervisors about the current work of CBHWs and the feasibility of using this health cadre to administer IPTp to pregnant women. The Study sought to understand provider opinions to design an IPTp-SP intervention involving CBHWs.
Qualitative analysis identified common themes in the open-ended responses. Providers like the CBHW program, noting that “CBHWs come from the community” and help with language barriers. However, CBHWs are not always available or move frequently from one community to another. A few male providers noted issues with timely payment of stipends to CBHWs.
 Most providers were open to CBHWs providing IPTp-SP to pregnant women: “It will reduce [our] workload.” Unlike female providers, some male providers stressed the need for CBHWs to be “well trained.”
Most providers were open to CBHWs providing IPTp-SP to pregnant women: “It will reduce [our] workload.” Unlike female providers, some male providers stressed the need for CBHWs to be “well trained.”
Providers commented that CBHWs were needed and could contribute. For example CBHWs could increase the uptake of IPTp-SP, prevent deaths and malaria, educate women and the community, and prevent stock-outs of SP. While CBHWs do not currently provide IPTp-SP, several providers noted that CBHWs already conduct community education sessions with pregnant women on taking IPTp-SP.
A few noted that CBHWs already monitor adherence to IPTp-SP doses and send women to the health facility when doses are needed. Providers expressed the importance of including information on malaria prevention and treatment, IPTp-SP administration, stock management, and data collection in the CBHW training.
 The findings guided discussions and planning with both district and CSPS staff in the design of the CBHW training and IPTp-SP intervention. The results led to development of the training-of-trainers process that started with the district health team, who then trained CSPS staff—the CSPS staff then trained CBHWs.
The findings guided discussions and planning with both district and CSPS staff in the design of the CBHW training and IPTp-SP intervention. The results led to development of the training-of-trainers process that started with the district health team, who then trained CSPS staff—the CSPS staff then trained CBHWs.
Gaining the frontline staff’s acceptance of and perceptions about CBHWs—and building on them—will hopefully lead to greater ownership and better management of project implementation at the community level.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID, PMI, or the United States Government.
CHW &IPTp &Malaria in Pregnancy Bill Brieger | 18 Apr 2018
Community-Based Health Workers in Burkina Faso: Are they ready to take on a larger role to prevent malaria in pregnancy?
Community Based Health Worker (CBHW) opinions were sought prior to establishing community delivery of intermittent preventive treatment of malaria in pr4egnancy in Burkina Faso. Bill Brieger, Danielle Burke, Justin Tiendrebeogo, Ousmane Badolo, Mathurin Dodo, Yacouba Savadogo, and Susan Youll report on the findings from the CBHWs at the 7th Multilateral Initiative for Malaria Meeting in Dakar.
 In 2012 and 2013, World Health Organization recommended that a minimum of three doses—rather than two doses—of intermittent preventive treatment of malaria in pregnancy (IPTp). This three-dose recommendation has made it more challenging to achieve the 85% national coverage target in Burkina Faso. Existing health services in other endemic countries have also had difficulty achieving the two-dose target. Using a formative approach, this study tested if the 85% target could be achieved by having IPTp delivered to the community through trained community-based health workers (CBHWs) who are supervised by the health system.
In 2012 and 2013, World Health Organization recommended that a minimum of three doses—rather than two doses—of intermittent preventive treatment of malaria in pregnancy (IPTp). This three-dose recommendation has made it more challenging to achieve the 85% national coverage target in Burkina Faso. Existing health services in other endemic countries have also had difficulty achieving the two-dose target. Using a formative approach, this study tested if the 85% target could be achieved by having IPTp delivered to the community through trained community-based health workers (CBHWs) who are supervised by the health system.
Existing training materials for these CBHWs outline a basic role in promoting antenatal care (ANC) and guiding communities to use curative and preventive malaria services. The question was to what extent are the CBHWs practicing what they were taught, and could training in community delivery of IPTp build on their existing roles.
Because of continuous malaria transmission, these three districts in the southern part of Burkina Faso were chosen for the intervention study: Batie, Po, and Ouargaye. Also in these three districts, community health workers have been involved in the implementation of other programs, such as immunization, malaria, nutrition, and family planning.
As part of this formative study to design the community-based IPTp intervention, semi-structured interviews were conducted with CBHWs in three health districts (Batie, Po, and Ouargaye) with a high malaria burden. In general, the Directorate of Health Promotion in the Ministry of Health encourages communities to select one male and one female CBHW, although the actual CBHWs chosen would depend on availability and literacy of the CBHW.
In each district, four centre de santé et de promotion sociale (health and social promotion centers [CSPS] were selected, and their catchment areas were divided among intervention and control groups. Effort was made to reach all CBHWs currently practicing in these 12 catchment areas. Numerical and narrative data were entered in a database and analyzed by gender based on major themes relating to ANC, pregnancy, and malaria services. Interview transcripts were manually reviewed for themes.
 Of the CBHWs interviewed, a total of 62 were male and 42 were female. Both female and male CBHWs provide advice and education to women in their villages, which may include advising women to go to the CSPS for pregnancy or ANC, family planning, immunization, or illness. Some CBHWs stated that they remind women about follow-up ANC appointments. As one female CBHW explained, “on their return [from CSPS for care], I ask [the pregnant woman] what has been said and I shall ensure they practice this.”
Of the CBHWs interviewed, a total of 62 were male and 42 were female. Both female and male CBHWs provide advice and education to women in their villages, which may include advising women to go to the CSPS for pregnancy or ANC, family planning, immunization, or illness. Some CBHWs stated that they remind women about follow-up ANC appointments. As one female CBHW explained, “on their return [from CSPS for care], I ask [the pregnant woman] what has been said and I shall ensure they practice this.”
A male CBHW noted that he “direct[s] women, in case of amenorrhea, [to] go to CSPS to check for pregnancy, to [receive] follow[-up] care, and be in good health.” Many male CBHWs were likely to mention malaria-related activities, including education about causes and prevention of malaria. A few male CBHWs talked about helping people recognize malaria, seek treatment, and comply with recommended medicine regimens.
A few male and female CBHWs specifically mentioned encouraging women to take sulfadoxine-pyrimethamine for IPTp. Some reported involvement in distributing bed nets. In contrast to the male CBHWs, some female CBHWs may even accompany women to ANC to ensure that the women receive services.
 Some challenges were faced by CBHWs. At least a third of the CBHWs noted difficulties in carrying out their work, but they also had encouragements: “Acceptance by the community of my activities facilitates the task.” “Nothing is easy, but with the understanding of people, there are no problems.” While officially, CBHWs were to receive a stipend, one CBHW explained that “nothing is easy, especially that I am not paid for all these activities.” Others also noted that “for the moment, there is nothing that is easy as we lack the tools [for the job].”
Some challenges were faced by CBHWs. At least a third of the CBHWs noted difficulties in carrying out their work, but they also had encouragements: “Acceptance by the community of my activities facilitates the task.” “Nothing is easy, but with the understanding of people, there are no problems.” While officially, CBHWs were to receive a stipend, one CBHW explained that “nothing is easy, especially that I am not paid for all these activities.” Others also noted that “for the moment, there is nothing that is easy as we lack the tools [for the job].”
CBHWs report being active in promoting the health of pregnant women and encouraging women and the community to prevent and treat malaria. Although their training stresses postnatal care, this area was not mentioned during interviews. Likewise, CBHWs did not address the danger signs of malaria in pregnancy during the interviews, which is in their training. Female CBHWs were more likely to encourage pregnant women to attend ANC at CSPS and follow up with them after the visit, while the male CBHWs were more focused on providing health information. Logistical challenges and payment of stipends need to be addressed before adding more duties for the CBHW to complete. Overall, CBHWs are positioned to deliver IPTp under the supervision of CSPS staff.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID, PMI, or the United States Government.
IPTp &Malaria in Pregnancy &Quality of Services Bill Brieger | 15 Apr 2018
Improved IPTp Uptake: MCSP Restoration of Health Services Experience in Liberia
Nyapu D.Taylor, Birhanu Getahun,Topian Zikeh, Anne Fiedler, and Allyson Nelson of the USAID supported Maternal and Child Survival Program/Jhpiego in Liberia are presenting their project aimed at strengthening health services in Liberia to improve uptake of Intermittent preventive treatment of malaria in pregnancy at the 7th Multilateral Initiative for Malaria in Dakar this week. Below are a description of their work and their main findings.

Mother and baby in Liberian Government Hospital, Grand Bassa County, Liberia. Photo by Kate Holt, Jhpiego.
In Liberia more than 170,000 pregnancies occur each year. Provision of two or more doses of SP for IPTp (IPTp2+) merely increased from 50% 2016. Provision of the three or more doses of
IPTp (IPTp3+) remains at 22%.Liberia adopted WHO’s IPTp3+ guideline but it is not practiced all over the country. There is a gap in the competency of the health care workforce. There are recurring stock-outs of SP.The Maternal and Child Survival Program (MCSP) Restoration of Health Services (RHS) intended to address these challenges. Project
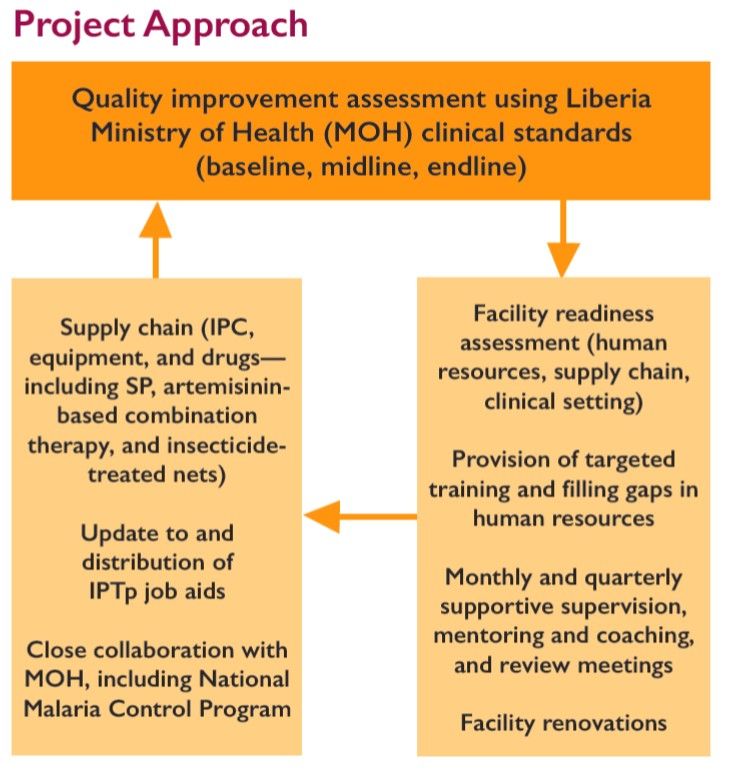
Objectives included Prevention at facilities by strengthening infection prevention and control (IPC) practices at 77 health facilities through training, intensive supportive supervision, triage, improvement of waste management, and provision of essential IPC commodities and supplies. Also the project aimed to Increase utilization of and demand for maternal and child health services bu restoring delivery of quality primary health care services through implementation of integrated reproductive, maternal, newborn, child, and adolescent health as part of the Essential Package of Health Services in 77 facilities.
 MCSP RHS supported health facilities in three counties:
MCSP RHS supported health facilities in three counties:
- Grand Bassa: 30 (91% of health facilities in county)
- Lofa: 17 (27% of health facilities in county)
- Nimba: 30 (46% of health facilities in county)
Population coverage was 900,000 or 20% of population. This included 45,000 pregnancies per year. The Project timeline is September 2015–June 2018. The quality improvement process used in the project is seen in the attached diagram.
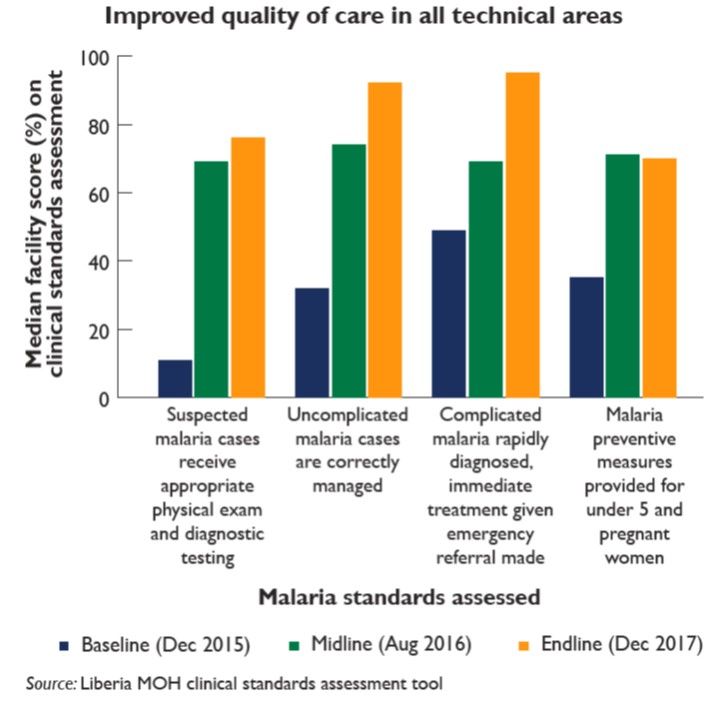
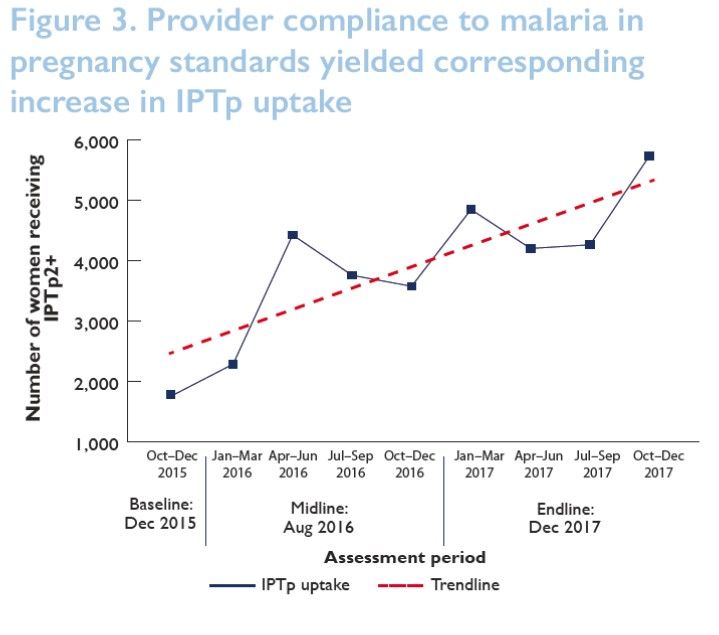
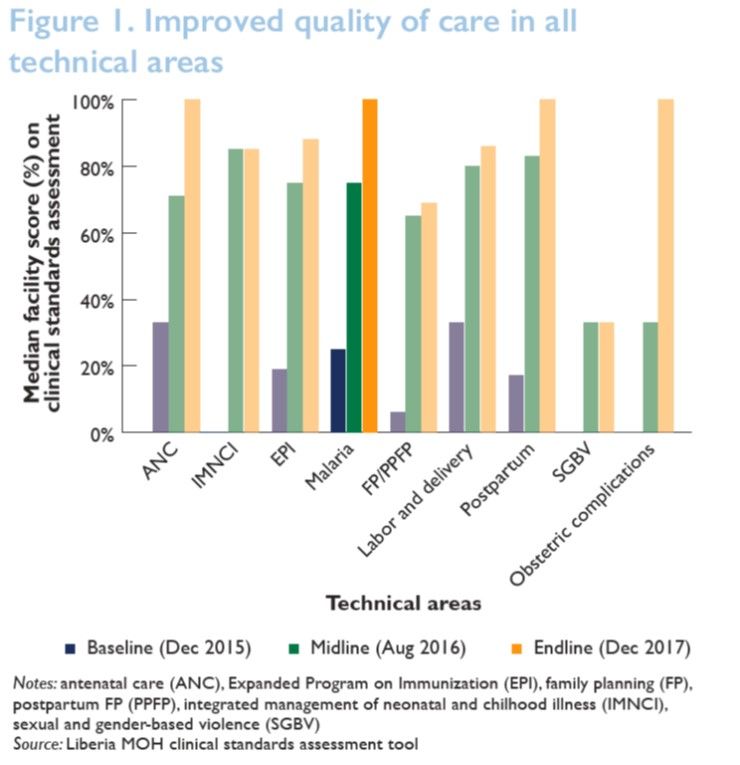 Several achievements were documented. Adherence to malaria clinical standards improved from 25% at baseline to 100% at endline in 39 MCSP-supported facilities—sampled at endline (see Figure 1). Adherence to malaria clinical standards improved substantially from baseline to endline in 39 MCSP-supported facilities—sampled at endline (see Figure 2). Increasing uptake of IPT2+ in the 77 RHS facilities has been observed since the inception of the project (see Figure 3).
Several achievements were documented. Adherence to malaria clinical standards improved from 25% at baseline to 100% at endline in 39 MCSP-supported facilities—sampled at endline (see Figure 1). Adherence to malaria clinical standards improved substantially from baseline to endline in 39 MCSP-supported facilities—sampled at endline (see Figure 2). Increasing uptake of IPT2+ in the 77 RHS facilities has been observed since the inception of the project (see Figure 3).
 The project met and dealt with several challenges. Health facilities were sporadically stocked with SP and mosquito nets (another component of malaria in pregnancy services). Bad roads prevented travel to field during rainy seasons. This affected distribution of malaria supplies and provision of mentorship and supervision for quality service. Clients had huge difficulty accessing health facilities.
The project met and dealt with several challenges. Health facilities were sporadically stocked with SP and mosquito nets (another component of malaria in pregnancy services). Bad roads prevented travel to field during rainy seasons. This affected distribution of malaria supplies and provision of mentorship and supervision for quality service. Clients had huge difficulty accessing health facilities.
 Among the lessons learned were that close collaboration and involvement of key actors, especially MOH (National Malaria Control Program) and country health team at all levels, is an effective and efficient approach for project implementation. Regular mentorship and coaching during supportive supervision improves the quality of care provided for malaria in pregnancy. Ensuring availability of IPTp drugs and long-lasting insecticidal nets at health facilities are key to preventing malaria in pregnancy.
Among the lessons learned were that close collaboration and involvement of key actors, especially MOH (National Malaria Control Program) and country health team at all levels, is an effective and efficient approach for project implementation. Regular mentorship and coaching during supportive supervision improves the quality of care provided for malaria in pregnancy. Ensuring availability of IPTp drugs and long-lasting insecticidal nets at health facilities are key to preventing malaria in pregnancy.
In conclusion the project met IPC objectives and achieved 80% Safe, Quality, Health Services score. Thus there was improved service delivery utilization.
The poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Case Management &CHW &Elimination &Malaria in Pregnancy Bill Brieger | 11 Apr 2018
Multilateral Initiative for Malaria (MIM) – Jhpiego Presents in Dakar
 The 7th Pan African Malaria Conference holds from 15-20 April 2017, Dakar, Senegal. The conference celebrates 20 years since the initial establishment of the Multilateral Initiative on Malaria (MIM) by the Tropical Disease Research Program and partners.
The 7th Pan African Malaria Conference holds from 15-20 April 2017, Dakar, Senegal. The conference celebrates 20 years since the initial establishment of the Multilateral Initiative on Malaria (MIM) by the Tropical Disease Research Program and partners.
During the conference next week, staff from Jhpiego malaria projects in Burkina Faso, Liberia, Nepal, Madagascar and Cameroon will share oral and poster presentations to highlight their work. Below is a list along with the location numbers.
- Application d’un Audit de la Qualité des données (DQA) du paludisme dans le District Sanitaire de Kribi, Cameroun, SS-13 Oral
- Contribution des Agent de Santé Communautaire (ASC) à l’amélioration de la prévention et la prise en charge du paludisme dans le district de Kribi, Cameroun, B-40 Poster
- MOH’s effort in developing and implementing Quality Assurance plan (QAP) for Global Fund-supported antimalarial drugs: A case study of Nepal in the context of malaria elimination, C-107 Poster
- Community-Based Health Workers in Burkina Faso: Are they ready to take on a larger role to prevent malaria in pregnancy? D-115 Poster

- Contribution of Community-Based Health Workers (CBHWs) to Improving Prevention of Malaria in Pregnancy in Burkina Faso: Review of health worker perceptions from the baseline study D-118 Poster
- Malaria in Pregnancy: The Experience of MCSP in Liberia, D-140 Poster
- Improved Malaria Case Management of Under-Five Children: The Experience of MCSP-Restoration of Health Liberia project D-141 Poster
- Experiences and perceptions of care seeking for febrile illness among caregivers, pregnant women and health providers in eight districts of Madagascar D-142 Poster

 Abstracts will be shared here on the day of each presentation for those unable to attend MIM. Also check Jhpiego at Exhibit Booth 148.
Abstracts will be shared here on the day of each presentation for those unable to attend MIM. Also check Jhpiego at Exhibit Booth 148.