Community &IPTp &Malaria in Pregnancy Bill Brieger | 08 Nov 2017 11:16 am
Baseline for Coverage of Intermittent Preventive Treatment of Malaria in Pregnancy for Planning Community Interventions in Burkina Faso

Under supervision from health center Community Health Worker provides SP for IPTp to Pregnant Woman
Now that the World Health Organization recommends that pregnant women in high and stable malaria transmission areas receive three or more doses of Intermittent Preventive Treatment (IPTp) with Sulfadoxine-pyrimethamine, it is necessary to learn ways to reach more women with this intervention. William R. Brieger, Mathurin Dodo, Danielle Burke, Ousmane Badolo, Justin Tiendrebeogo, Kristen Vibbert, Susan J Youll, and Julie R Gutman conducted a baseline household survey of recently pregnant women in Burkina Faso to learn about the extent of current IPTp coverage and where improvements are needed. With support from the US President’s Malaria Initiative and the USAID Maternal and Child Survival Program Their findings were made available at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
The World Health Organization recommends intermittent preventive treatment (IPTp) to prevent the adverse effects of malaria in pregnancy in high burden settings; IPTp coverage has lagged behind international targets. In Burkina Faso, the 2014 Malaria Indicator Survey found that 22% of women received 3 or more doses of IPTp (IPTp3). In 2014, Burkina Faso’s IPTp policy was updated from recommending 2 doses to providing at least 3 doses of IPTp. Prior studies have suggested that use of community health workers to deliver IPTp can increase coverage.
 To improve IPTp coverage, we will pilot community delivery of IPTp within 3 southern districts: Po, Ouargaye, and Batie. Here we report results from a baseline assessment in the selected districts. Health Management Information System (HMIS) data for 2015 were collected in each district, and IPTp3 coverage was 37%. Four health facilities per district were randomly selected to participate in the pilot. In 2017, a baseline household survey was conducted among recently pregnant women in the catchment areas of these health facilities.
To improve IPTp coverage, we will pilot community delivery of IPTp within 3 southern districts: Po, Ouargaye, and Batie. Here we report results from a baseline assessment in the selected districts. Health Management Information System (HMIS) data for 2015 were collected in each district, and IPTp3 coverage was 37%. Four health facilities per district were randomly selected to participate in the pilot. In 2017, a baseline household survey was conducted among recently pregnant women in the catchment areas of these health facilities.
 Women were asked to recall the number of antenatal care (ANC) visits and IPTp doses they had received during their most recent pregnancy. The same information was extracted from their ANC cards. A total of 374 women were interviewed during the baseline survey.
Women were asked to recall the number of antenatal care (ANC) visits and IPTp doses they had received during their most recent pregnancy. The same information was extracted from their ANC cards. A total of 374 women were interviewed during the baseline survey.
ANC attendance was reported to be 98% for any visit, and 84% for four visits; these rates were 90% and 62% as documented on the ANC cards. Over 95% of women recalled receiving the first dose of IPTp, while over 80% of cards verified that the first dose was given.
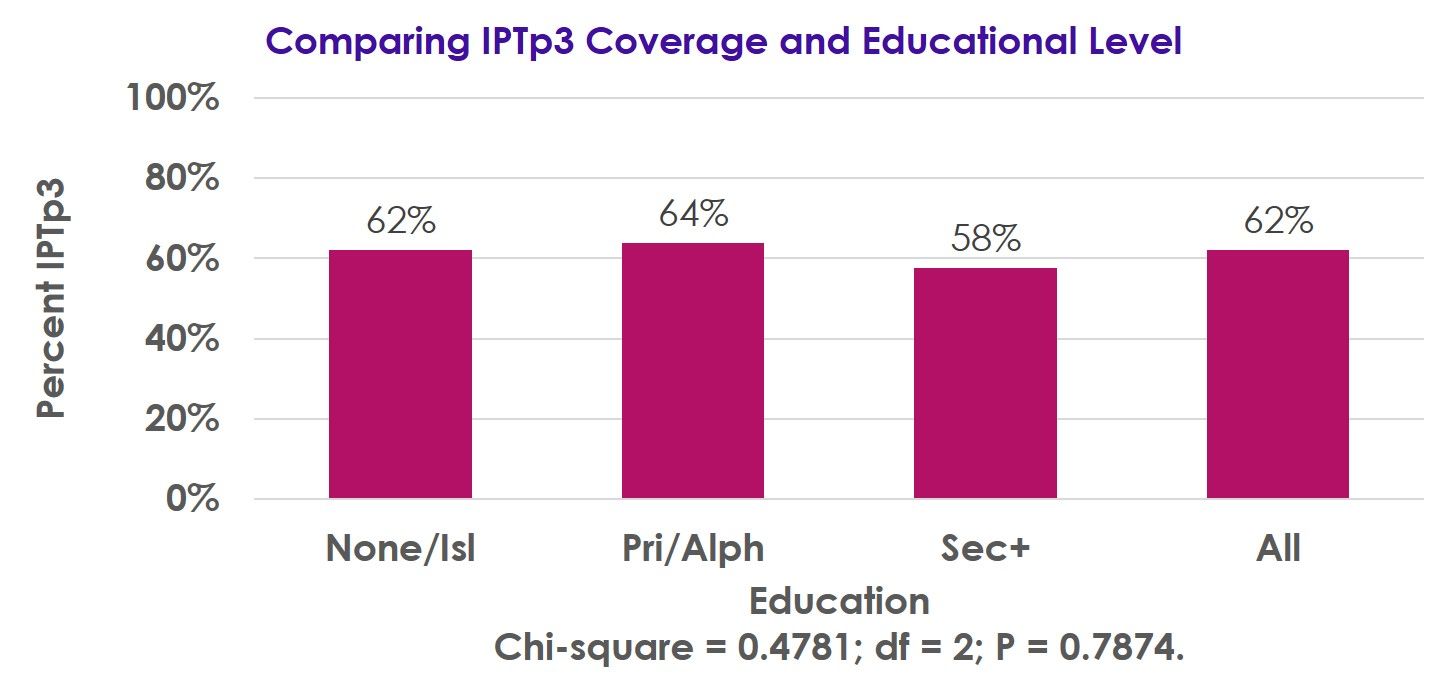 Receipt of the third IPTp dose was 62% by recall and 52% as recorded on the ANC cards, while receipt of 4 doses was 32% by recall and 19% per the ANC cards. IPTp3 coverage was not associated with parity or educational level.
Receipt of the third IPTp dose was 62% by recall and 52% as recorded on the ANC cards, while receipt of 4 doses was 32% by recall and 19% per the ANC cards. IPTp3 coverage was not associated with parity or educational level.
Following implementation of the revised IPTp policy, there has been a substantial improvement in IPTp coverage, though more work is needed to achieve the national 85% coverage target.
Our pilot will examine the impact that delivery of IPTp by community workers has on IPTp coverage, with endline surveys planned for 2018.