CHW &Community &IPTp &Malaria in Pregnancy Bill Brieger | 29 Oct 2018 05:58 am
Community Health Workers Can Enhance Coverage of Intermittent Preventive Treatment of Malaria in Pregnancy and Promote Antenatal Attendance
Among the poster presentations on malaria from Jhpiego, the President’s Malaria Initiative and partners at the 2018 ASTMH Annual Meeting, WR Brieger, J Tiendrebeogo, O Badolo, M Dodo, D Burke, K Vibbert, SJ Youll, and JR Gutman shared the findings from a 15-month intervention that tested the ability of community health workers to deliver intermittent preventive treatment of malaria in pregnancy in 3 districts in Burkina Faso. Please check out the poster and talk to one of the co-investigators at Poster Session A on Monday 29 October. Their results are found below.
Malaria in pregnancy is responsible for a substantial proportion of low-birthweight and stillborn infants in sub-Saharan Africa. To prevent this, the World Health Organizatio n (WHO) recommends that pregnant women receive intermittent preventive treatment of malaria in pregnancy (IPTp) using sulfadoxine-pyrimethamine. Specifically, WHO recommends an optimal three or more doses (e.g., IPTp3, IPTp4).
n (WHO) recommends that pregnant women receive intermittent preventive treatment of malaria in pregnancy (IPTp) using sulfadoxine-pyrimethamine. Specifically, WHO recommends an optimal three or more doses (e.g., IPTp3, IPTp4).
In stable malaria endemic countries, IPTp coverage remains unacceptably low, at around 19% for IPTp3. Community IPTp might provide an answer. Community delivery can improve coverage as seen in previous study in Nigeria and Malawi, but its effects on antenatal care (ANC) attendance have been mixed. Additional data are needed to determine whether delivery of IPTp-SP by community health workers (CHWs) is effective and does not detract from ANC attendance. Hence the Burkina Faso intervention was designed and implemented
The study piloted community delivery of IPTp (c-IPTp) in three districts of Burkina Faso  with high malaria transmission: Po, Ouargaye, and Batie. Four health facilities per district were randomly selected to participate (two intervention and two control).
with high malaria transmission: Po, Ouargaye, and Batie. Four health facilities per district were randomly selected to participate (two intervention and two control).
In 2017, following a baseline household survey of women who recently became pregnant, implementation of c-IPTp began in intervention areas by existing CHWs trained and supervised by health staff. At Baseline in each of the three study districts, four health centers (CSPSs) and the villages in their catchment areas were selected—two as intervention and two as control. A random sample of 374 women who had been pregnant within the last 9 months were interviewed in CSPS catchment villages. There were no significant differences in ANC attendance (ANC1=90%, ANC4=62%) or IPTp coverage between intervention and control areas:
- IPTp3 was 81% (intervention) and 86% (control).
- IPTp4 was 22% (intervention) and 16% (control).
 The Intervention consisted of building on Burkina Faso’s existing CHWs. They were trained and monitored by clinic staff. The CHWs encouraged women to attend the first ANC visit to obtain IPTp1. Then the CHWs provided monthly doses of IPTp, submitted monthly reports, and continued to promote ANC. ANC attendance and IPTp uptake were monitored through monthly clinic and CHW reports. The catchment area populations were roughly the same, and monitoring showed that the additional provision of IPTp by CHWs resulted in more women being reached while at the same time ANC attendance remained high.
The Intervention consisted of building on Burkina Faso’s existing CHWs. They were trained and monitored by clinic staff. The CHWs encouraged women to attend the first ANC visit to obtain IPTp1. Then the CHWs provided monthly doses of IPTp, submitted monthly reports, and continued to promote ANC. ANC attendance and IPTp uptake were monitored through monthly clinic and CHW reports. The catchment area populations were roughly the same, and monitoring showed that the additional provision of IPTp by CHWs resulted in more women being reached while at the same time ANC attendance remained high.
An endline su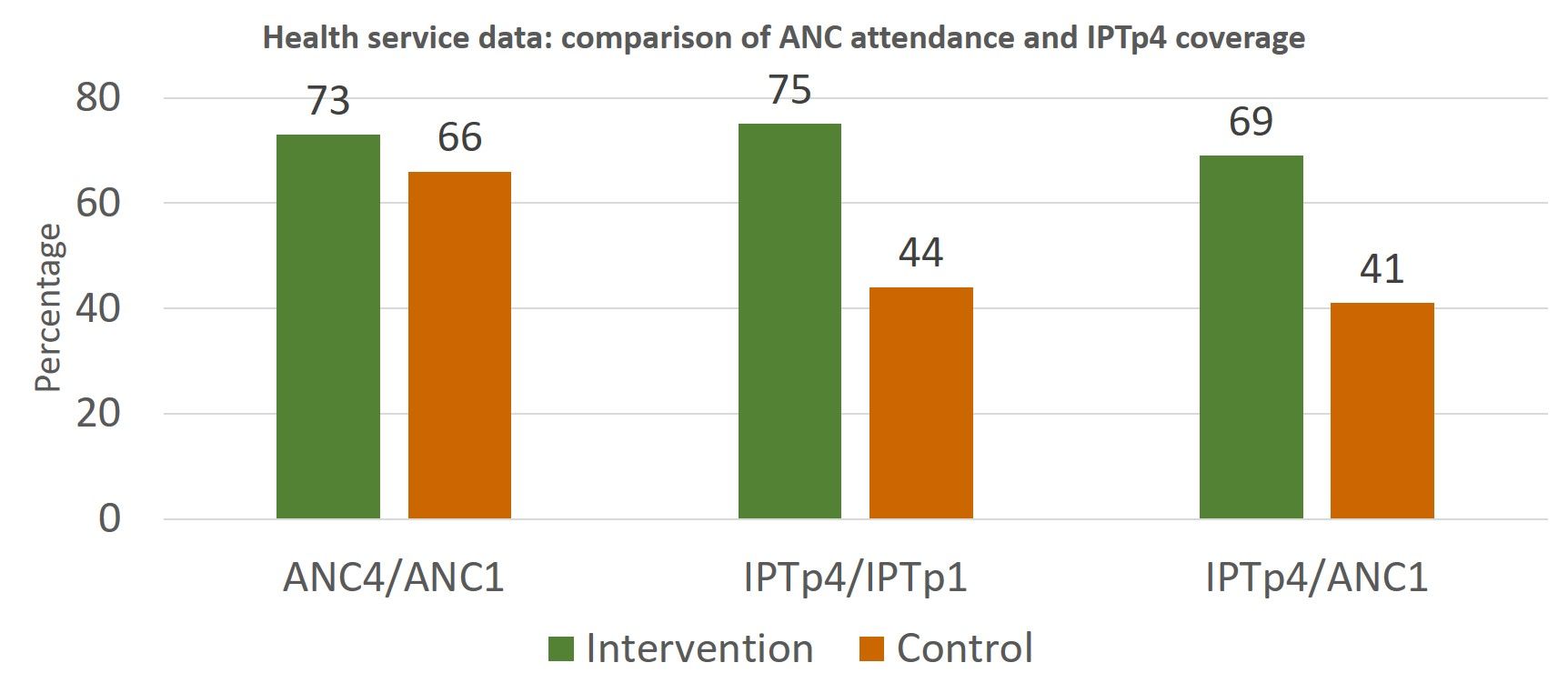 rvey was conducted after 18 months of implementation. Changes over time were compared between baseline and endline in intervention versus control villages. Attendance at ANC1 and ANC4 increased in both groups between baseline and endline but was significantly better for the intervention group. Likewise, coverage of IPTp3 and IPTp4 increased between baseline and endline for intervention and control women, but the difference was significant only in the intervention areas.
rvey was conducted after 18 months of implementation. Changes over time were compared between baseline and endline in intervention versus control villages. Attendance at ANC1 and ANC4 increased in both groups between baseline and endline but was significantly better for the intervention group. Likewise, coverage of IPTp3 and IPTp4 increased between baseline and endline for intervention and control women, but the difference was significant only in the intervention areas.
 Monthly monitoring of CHW and ANC registers and the household surveys both documented that community delivery of IPTp resulted in the desired increased uptake of services without detracting from ANC attendance. Community IPTp may be a promising strategy to improve coverage of IPTp.
Monthly monitoring of CHW and ANC registers and the household surveys both documented that community delivery of IPTp resulted in the desired increased uptake of services without detracting from ANC attendance. Community IPTp may be a promising strategy to improve coverage of IPTp.
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.