Case Management &Health Information &IPTp &Mortality &Quality of Services Bill Brieger | 31 Oct 2018
Improving Malaria Care Project Contribution in Transforming Malaria Control for Vulnerable Populations in Burkina Faso
![]() Mathurin Dodo, Ousmane Badolo, Stanislas Nebie, Youssouf Sawadogo, Thierry Ouedraogo, Moumouni Bonkoungou, Youssouf Zongo, Maria Gouem, Danielle Burke, Gladys Tetteh, Lolade Oseni, Linda Fogarty, and William Brieger of Jhpiego and the USAID Improving malaria Care Project in Burkina Faso shared the status of malaria control efforts at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. The focus on vulnerable populations is shared below.
Mathurin Dodo, Ousmane Badolo, Stanislas Nebie, Youssouf Sawadogo, Thierry Ouedraogo, Moumouni Bonkoungou, Youssouf Zongo, Maria Gouem, Danielle Burke, Gladys Tetteh, Lolade Oseni, Linda Fogarty, and William Brieger of Jhpiego and the USAID Improving malaria Care Project in Burkina Faso shared the status of malaria control efforts at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. The focus on vulnerable populations is shared below.
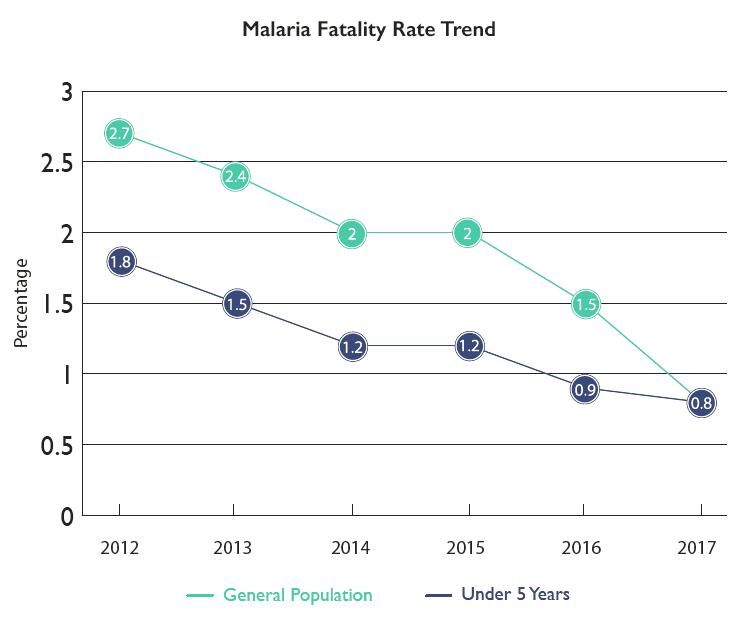
Burkina Faso in 2010-2012 experienced poor capacity in malaria prevention and control, Malaria fatality rate was high:
- Pregnant women: 0.71% in 2010 and 0.66% in 2012
- Children under 5: 2.8% in 2010 and 2.7% in 2012
Improving Malaria Care (IMC) Project funded by USAID/President’s Malaria Initiative, began in 2013. IMC supports National Malaria Control Program to improve prevention and case
Management. IMC’s Strategies include the following:
- Update national malaria prevention and case management guidelines
- Strengthen health care provider capacity
- Align malaria training package with revised guidelines
- Strengthen national malaria health management information system (HMIS)
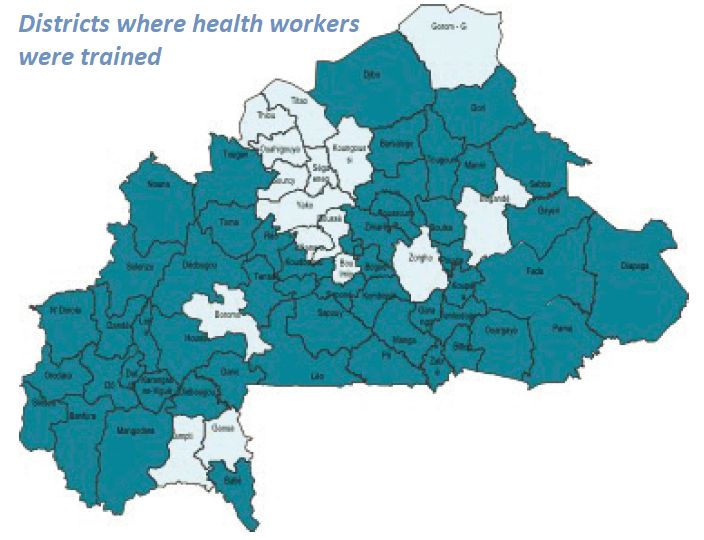 IMC together with the National Malaria Control Program has been strengthening Health Care Provider Capacity. 54 health districts have been covered by IMC direct support where 1819 providers were trained. Training reached 185 trainers/supervisors on revised training Modules who then trained 1,819 health care providers from 1,349 health facilities in 54 districts on new guidelines
IMC together with the National Malaria Control Program has been strengthening Health Care Provider Capacity. 54 health districts have been covered by IMC direct support where 1819 providers were trained. Training reached 185 trainers/supervisors on revised training Modules who then trained 1,819 health care providers from 1,349 health facilities in 54 districts on new guidelines
 After training 58 supervisors rolled out quality improvement (QI) systems. They oriented 897 providers from referral hospitals on new severe case management guidelines. Formative Supervision, Performance and Quality Improvement efforts were based on an improved malaria supervision guide and tools. Post-training supervision reached each provider. Specifically, malaria supervisions occurred twice a year.
After training 58 supervisors rolled out quality improvement (QI) systems. They oriented 897 providers from referral hospitals on new severe case management guidelines. Formative Supervision, Performance and Quality Improvement efforts were based on an improved malaria supervision guide and tools. Post-training supervision reached each provider. Specifically, malaria supervisions occurred twice a year.
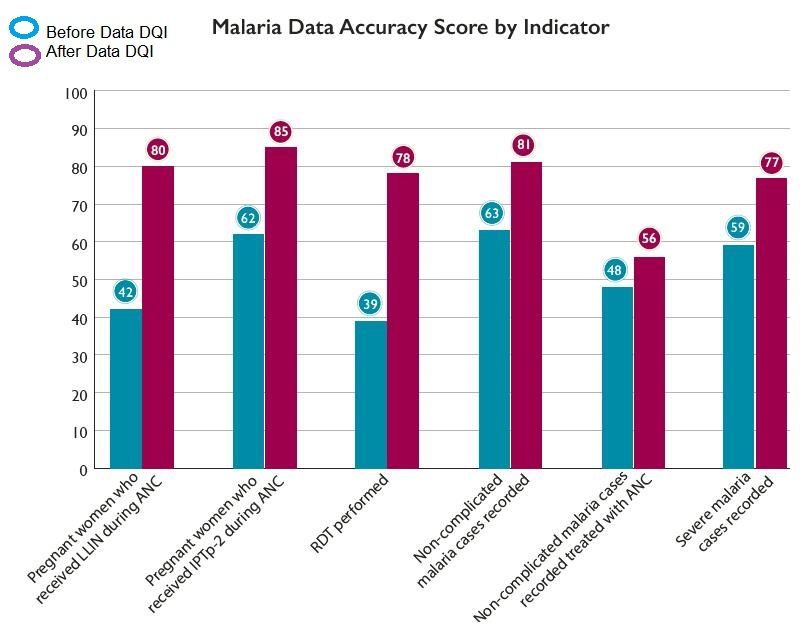
The quality improvement approach, SBM-R® (Standards-Based Management and Recognition) approach, was implemented in 6 regions, 28 districts. Organized data review and validation workshop in 67 districts were another aspect of quality improvement. To sustain quality improvement, IMC conducted 2-day quality assessments and guided developed DQI implementation plans.
 Social Behavior Change Communication was a central component of IMC. IMC conducted 13 regional advocacy workshops on malaria issues. The project developed and broadcast 2 malaria spots through 27 media, revised 5 diagnostic and case management job aids, distributed 7,440 job aids to health facilities, and reached 792,660 people through community activities and sensitization sessions
Social Behavior Change Communication was a central component of IMC. IMC conducted 13 regional advocacy workshops on malaria issues. The project developed and broadcast 2 malaria spots through 27 media, revised 5 diagnostic and case management job aids, distributed 7,440 job aids to health facilities, and reached 792,660 people through community activities and sensitization sessions
 IMC Strengthened National Malaria HMIS. This included training 1,300 (72%) health workers to enter data into monthly reporting forms. Also trained were 326 data managers on HMIS and data use for decisionmakers. The malaria data collection system was integrated into national HMIS using DHIS2. To facilitate this the national HMIS manual was revised and distributed. Data Quality was improved through malaria data review and validation at district levelUltimately these interventions resulted in Improved Malaria Services. More confirmed simple malaria cases received artemisinin-based combination therapy (65% in 2013 to 90% in 2017). More women received three doses of IPTp3 (14% in 2014 to 51% in June 2018). More suspected cases tested for malaria (65% in 2013 to 96% 2017). More women received insecticide-treated nets at antenatal care. There was Better accuracy in reporting of malaria key indicators.
IMC Strengthened National Malaria HMIS. This included training 1,300 (72%) health workers to enter data into monthly reporting forms. Also trained were 326 data managers on HMIS and data use for decisionmakers. The malaria data collection system was integrated into national HMIS using DHIS2. To facilitate this the national HMIS manual was revised and distributed. Data Quality was improved through malaria data review and validation at district levelUltimately these interventions resulted in Improved Malaria Services. More confirmed simple malaria cases received artemisinin-based combination therapy (65% in 2013 to 90% in 2017). More women received three doses of IPTp3 (14% in 2014 to 51% in June 2018). More suspected cases tested for malaria (65% in 2013 to 96% 2017). More women received insecticide-treated nets at antenatal care. There was Better accuracy in reporting of malaria key indicators.
 Improved services led to decreased national malaria fatality rate. In the General population there was a decrease in malaria deaths of 34% and a decrease in overall fatality rate by 47%. Among pregnant women there was a decrease in malaria deaths by 91% and a decrease in malaria fatality rate by 93%. For Children under 5 years of age, there was a decrease in malaria deaths by 34% and a decrease in fatality rate 48%
Improved services led to decreased national malaria fatality rate. In the General population there was a decrease in malaria deaths of 34% and a decrease in overall fatality rate by 47%. Among pregnant women there was a decrease in malaria deaths by 91% and a decrease in malaria fatality rate by 93%. For Children under 5 years of age, there was a decrease in malaria deaths by 34% and a decrease in fatality rate 48%
 In conclusion the IMC Project Contributed to Lives Saved in Burkina Faso. IMC supported health delivery sites in Burkina Faso (Jan 2014 -Sep 2017). As a result the health system was able to Distribute 33,566,671 courses of artemisinin-based combination therapy. IMC provided 2,175,648 pregnant women with intermittent preventive treatment 2nd dose and distributed 1,146,185 nets to pregnant women during antenatal care visit. These interventions averted estimated 150,390 malaria deaths and 12,866,271 DALYs (Disability-Adjusted Life Years calculated using PSI Impact calculator. 1 DALY=1 lost year of “healthy” life.)
In conclusion the IMC Project Contributed to Lives Saved in Burkina Faso. IMC supported health delivery sites in Burkina Faso (Jan 2014 -Sep 2017). As a result the health system was able to Distribute 33,566,671 courses of artemisinin-based combination therapy. IMC provided 2,175,648 pregnant women with intermittent preventive treatment 2nd dose and distributed 1,146,185 nets to pregnant women during antenatal care visit. These interventions averted estimated 150,390 malaria deaths and 12,866,271 DALYs (Disability-Adjusted Life Years calculated using PSI Impact calculator. 1 DALY=1 lost year of “healthy” life.)
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID) under Cooperative Agreement No. AID-624-A-13-00010 and the President’s Malaria Initiative (PMI). The contents are the responsibility of the authors and do not necessarily reflect the views of USAID, PMI or the United States Government.
Case Management &Health Information &Procurement Supply Management Bill Brieger | 30 Oct 2018
One SMS Saves Lives in Madagascar
 Haja Andriamiharisoa, Eliane Razafimandimby, Jean Pierre Rakotovao, Jean Eugene Injerona, Zo Harifetra, Lalanirina H. Ravony, Rado Randriamboavonjy, Jocelyn Razafindrakoto, and Laurent Kapesa have been working with the USAID Maternal and Child Survival Program. At the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene they presented their experiences on “Improving Procurement and Redeployment of Malaria Commodities Using SMS and Web Mapping at a District Level in Madagascar,” and are also sharing via this posting.
Haja Andriamiharisoa, Eliane Razafimandimby, Jean Pierre Rakotovao, Jean Eugene Injerona, Zo Harifetra, Lalanirina H. Ravony, Rado Randriamboavonjy, Jocelyn Razafindrakoto, and Laurent Kapesa have been working with the USAID Maternal and Child Survival Program. At the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene they presented their experiences on “Improving Procurement and Redeployment of Malaria Commodities Using SMS and Web Mapping at a District Level in Madagascar,” and are also sharing via this posting.
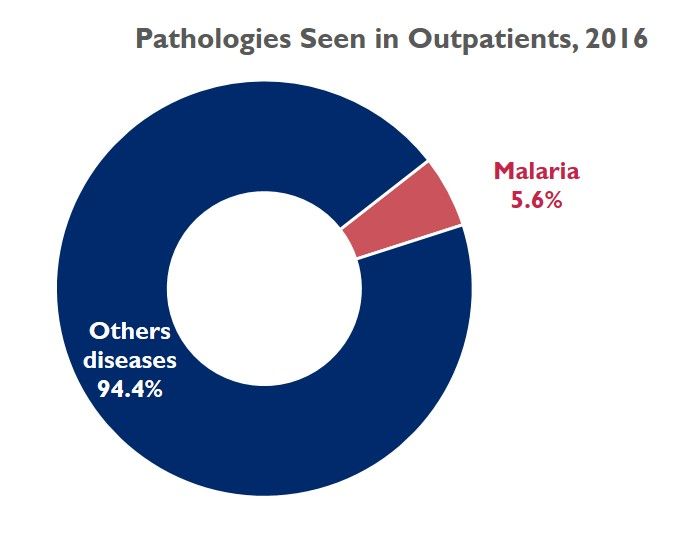 Malaria is a public health problem in Madagascar. In 2016, the frequency of diseases at health center level, places malaria at the 4th cause of hospital morbidity and mortality. Out of about 30 thirty diseases, malaria accounts for 5.6% of all cases.
Malaria is a public health problem in Madagascar. In 2016, the frequency of diseases at health center level, places malaria at the 4th cause of hospital morbidity and mortality. Out of about 30 thirty diseases, malaria accounts for 5.6% of all cases.
Health facilities often experience commodity stock-outs of products used for malaria prevention and case management. The existing logistics reporting system does not allow for macro or micro views of the monthly stock situation at the health facility level, which inhibits rapid decision-making.
 On January 2018, implementation of a fast data collection system and easy-to-use data visualization began. The tool was based on the use of SMS and web mapping to map the level of monthly keys stock of commodities. The data are sent by providers at facility level via structured SMS and are published by a web server by a web mapping process. Note that sending a monthly SMS costs 9 US cents per facility. Providers at 773 health facilities in 16 regions of Madagascar sent monthly SMS (each message cost $0.09) with ART, ACT, and ITN stock levels.
On January 2018, implementation of a fast data collection system and easy-to-use data visualization began. The tool was based on the use of SMS and web mapping to map the level of monthly keys stock of commodities. The data are sent by providers at facility level via structured SMS and are published by a web server by a web mapping process. Note that sending a monthly SMS costs 9 US cents per facility. Providers at 773 health facilities in 16 regions of Madagascar sent monthly SMS (each message cost $0.09) with ART, ACT, and ITN stock levels.
- Sample message: “Please send the quantity in stock at the end of month in: ART, ACT, ITN.”
- Structure like: “palu csbcode year month ART ACT ITN. Thank you.”
- Sample of answer received: “palu 520241031 D A 200 25 0”
 Thus was created an easy-to-use tool from data received. It was free to use, and no password was needed. The SMS is simple and short (of 40 forty characters, composed of:
Thus was created an easy-to-use tool from data received. It was free to use, and no password was needed. The SMS is simple and short (of 40 forty characters, composed of:
- “palu” diminutive of malaria so that the system is ready for data collection from other cases
- the health facility code : 520241031
- year : here D : as project has implemented sms data collecting system since 2015 = A
- month : here A that means January
- stock of Injectable Artesunate (ART) : 200
- stock of tablet for Artemisinin–based combination therapy (ACT) : 25
- stock of Insecticide Treated Nets (ITN) : 0
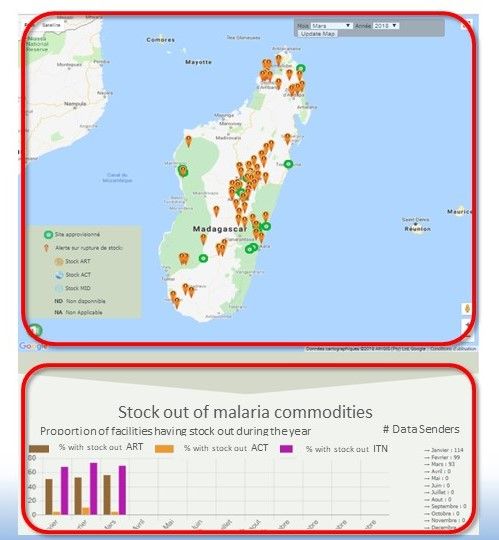
 Providers send SMS after completing the Monthly Activity Report. (CSB = Centre de Santé de Base, or basic health center). The received data are then displayed as web mapping on a Google map background, embedded on a web page. From this screen shot, The page displays a map of stock outs for the selected month, and monthly charts of the stock status of the three commodities. Accessing this website, is open, without restriction.
Providers send SMS after completing the Monthly Activity Report. (CSB = Centre de Santé de Base, or basic health center). The received data are then displayed as web mapping on a Google map background, embedded on a web page. From this screen shot, The page displays a map of stock outs for the selected month, and monthly charts of the stock status of the three commodities. Accessing this website, is open, without restriction.
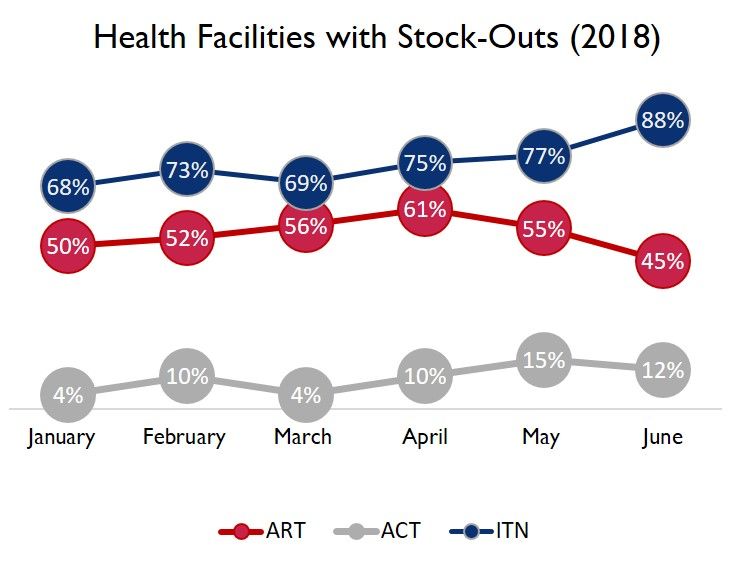
From the end of January to the end of June 2018, a hundred health facilities sent SMS each month. The data we received shows that on average:
- 75% Average stock-out of ITN
- 53% Average stock-out of ART
- 9% Average stock-out of ACT
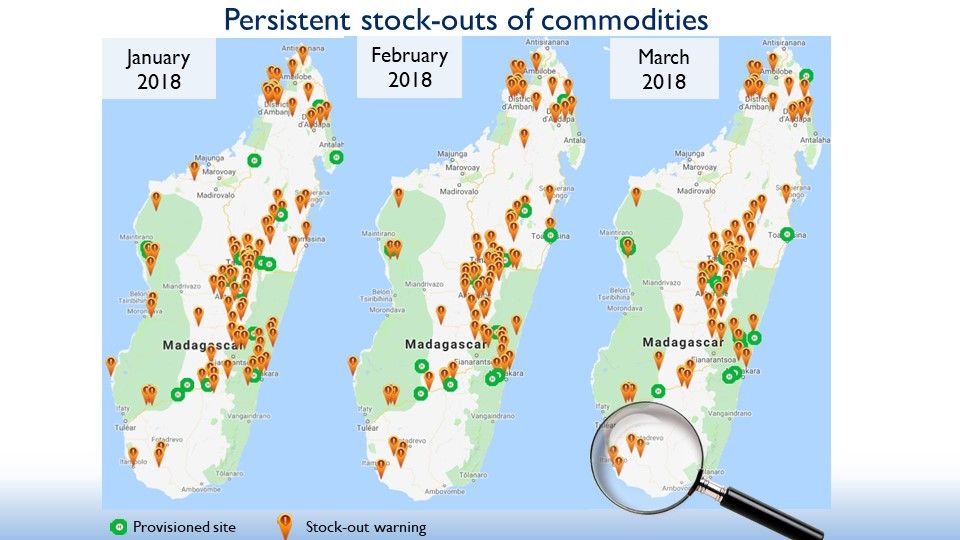 The attached three-map picture provides a broad view from three screenshots of the system, showing the evolution of stock-outs at a facility level
The attached three-map picture provides a broad view from three screenshots of the system, showing the evolution of stock-outs at a facility level
- Each point represents health facilities:
- When the dot is green, this means that the 03 commodities are available in stock
- When in brown, at least one of the 03 elements is unavailable
- At first sight, there are more stockouts than stock availability and a tendency of the reduction of green points over the months
- Appropriate decision-making would change the points of the map of the following months to green
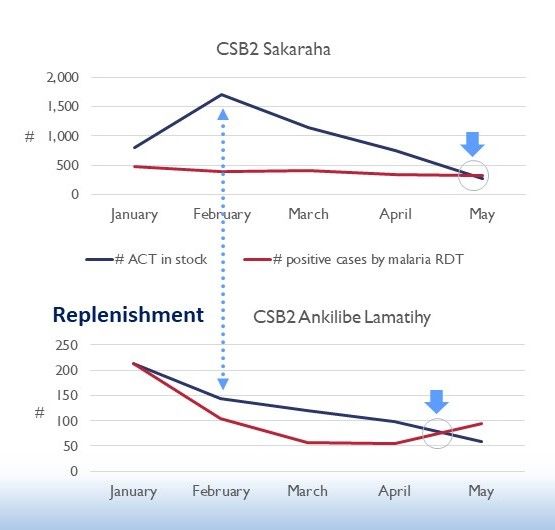 After this broad view of the country’s overall situation and given the large number of facilities with out of stock, an emergency supply for all districts was done for some medicine since February 2018. Based on maps and stats, we could improve our interventions at a CSB level through rapid and adequate decision-making as in the supply of ITN and ART.
After this broad view of the country’s overall situation and given the large number of facilities with out of stock, an emergency supply for all districts was done for some medicine since February 2018. Based on maps and stats, we could improve our interventions at a CSB level through rapid and adequate decision-making as in the supply of ITN and ART.
In conclusion, the use of SMS data collection to map stock-outs online can quickly improve input supply through simple spatial analysis. Sending SMSs to alert district-level officials about overstock in facilities at the same district level can solve many stock-out issues. All districts were restocked using this SMS and Web mapping system, but routing to the CSBs remains a challenge. Punctual stock-out reporting could significantly reduce the morbidity and mortality caused by malaria.
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A- 14-00028. The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government.
Case Management &CHW &Community &iCCM Bill Brieger | 29 Oct 2018
Performance of Community Health Workers in Providing Integrated Community Case Management (iCCM) Services in Eight Districts of Rwanda

During the first poster session at the 2018 Annual Meeting fo the American Society of Tropical Medicine and Hygiene, Noella Umulisa, Aline Uwimana, Cathy Mugeni, Beata Mukarugwiro, Stephen Mutwiwa, and Aimable Mbituyumuremyi of the Maternal and Child Survival Project (USAID)/Jhpiego and the Ministry of Health, Rwanda, presented findings from a review of community health workers in malaria case management. Their findings follow:
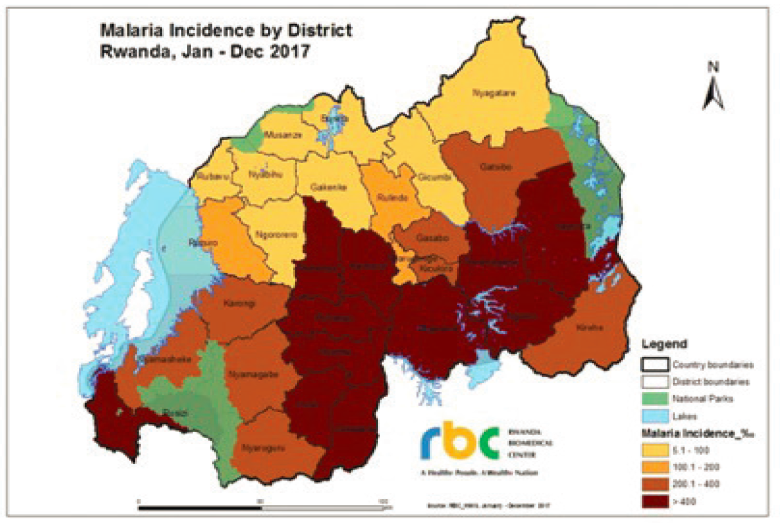 Rwanda has achieved near universal coverage of long-lasting insecticide nets, artemisinin-based combination therapy (ACT) and diagnosis, and targeted indoor residual spraying. Even so, there was an unprecedented increase in malaria cases from 2012-2017 despite optimal coverage of preventive and curative key interventions. The increase was caused by higher temperature, more rainfall, and increased resistance to insecticides.
Rwanda has achieved near universal coverage of long-lasting insecticide nets, artemisinin-based combination therapy (ACT) and diagnosis, and targeted indoor residual spraying. Even so, there was an unprecedented increase in malaria cases from 2012-2017 despite optimal coverage of preventive and curative key interventions. The increase was caused by higher temperature, more rainfall, and increased resistance to insecticides.
With more cases, the need for community case management (CCM) is crucial. Rwanda therefore trains, equips and supports community health providers to deliver high- impact treatment interventions and aims to supplement facility-based case management. Rwanda introduced integrated CCM 2008. Trained community health workers (CHWs) provide iCCM based on empirical diagnosis and treatment of pneumonia, diarrhea, and malaria. They also conduct malnutrition surveillance, comprehensive reporting and referral services.
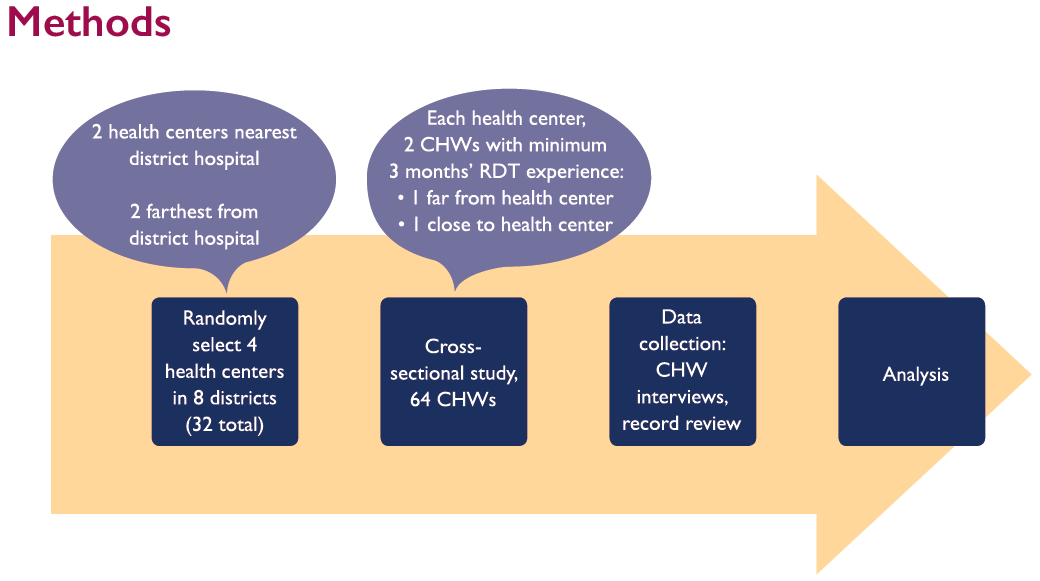 Given the changing status of malaria in the country, it was necessary to evaluate the performance of the CHWs. The evaluation aimed 1) to evaluate CHW performance in managing malaria, pneumonia and diarrhea in 8 districts of Rwanda based on national guidelines, and 2) to identify areas to reinforce and empower community health interventions. Using proximity (near/far) to hospitals and health centers, CHWs who had a minimum of 3 months experience using malaria rapid diagnostic tests (RDTs) were selected for interview. Slightly over half of CHWs were Males (56.2%). Most were over 40 years of age and nearly one-third were 50 years and older. Only 2% were between 25-29 years old.
Given the changing status of malaria in the country, it was necessary to evaluate the performance of the CHWs. The evaluation aimed 1) to evaluate CHW performance in managing malaria, pneumonia and diarrhea in 8 districts of Rwanda based on national guidelines, and 2) to identify areas to reinforce and empower community health interventions. Using proximity (near/far) to hospitals and health centers, CHWs who had a minimum of 3 months experience using malaria rapid diagnostic tests (RDTs) were selected for interview. Slightly over half of CHWs were Males (56.2%). Most were over 40 years of age and nearly one-third were 50 years and older. Only 2% were between 25-29 years old.
 Based on National Guidelines, CHWs were judged to have provided “adequate” treatment more frequently than “correct” treatment. Overall, 90% of cases were adequately treated; only 70% correctly treated. Among the three main conditions, malaria was most often adequately and correctly treated. Incorrect treatment was due to lack of adherence to guidelines. For malaria incorrect treatment often meant using the wrong does for age packet for treatment when the correct packet was not in stock.
Based on National Guidelines, CHWs were judged to have provided “adequate” treatment more frequently than “correct” treatment. Overall, 90% of cases were adequately treated; only 70% correctly treated. Among the three main conditions, malaria was most often adequately and correctly treated. Incorrect treatment was due to lack of adherence to guidelines. For malaria incorrect treatment often meant using the wrong does for age packet for treatment when the correct packet was not in stock.
 In conclusion, CHWs correctly treat 70% of children for all IMCI pathologies according to national guidelines. Malaria was the most seen/treated pathology; cases increased during study period. Overall, cases more often treated adequately than correctly. CHWs use complex tools thus lack adequate time to follow all steps correctly when providing services.
In conclusion, CHWs correctly treat 70% of children for all IMCI pathologies according to national guidelines. Malaria was the most seen/treated pathology; cases increased during study period. Overall, cases more often treated adequately than correctly. CHWs use complex tools thus lack adequate time to follow all steps correctly when providing services.
The study team recommends the need to strengthen iCCM commodities supply chain, especially at community level through supervision and mentorship conducted at health centers, district hospitals and central level. Also it is necessary to revise and simplify iCCM tools used by CHWs to decrease burden and improve quality of services.
 This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Announcement &Case Management &CHW &Community &Ebola &Infection Prevention &IPTp &Malaria in Pregnancy &Quality of Services Bill Brieger | 29 Oct 2018
Malaria Featured in Jhpiego Sessions at ASTMH 2018

Below is a list of Jhpiego Sessions at this week’s American Society of Tropical Medicine Annual Meeting in New Orleans (28 October-1 November). Please attend if you are at the conference:
![]() Poster Session A, Monday, October 29 (Posters in Marriott Grand Ballroom – 3rd Floor )
Poster Session A, Monday, October 29 (Posters in Marriott Grand Ballroom – 3rd Floor )
- Poster Number 098: Performance of community health workers in providing integrated community case management services (iCCM) in 8 districts of Rwanda
- Poster 380: Contribution of quarterly malaria data review and validation to data quality and malaria services Improvement
- Poster LB-5117: Community based health workers can enhance coverage of intermittent preventive treatment of malaria in pregnancy and promote antenatal attendance
Poster Session B, Tuesday 30 October
- Poster 1088: Assessing organizational capacity to deliver quality malaria services in rural Liberia
- Poster 1092: Contribution of IMC project in transforming the face of malaria control for vulnerable populations in Burkina Faso
- Poster 1093: Malaria response plan in times of high transmission: An approach to improving the quality of hospital malaria management
- Poster 1111: Setting the stage to introduce a ground breaking approach to prevent malaria in pregnancy in Sub-Saharan Africa: baseline-readiness assessment findings from Democratic Republic of Congo, Mozambique, Madagascar, and Nigeria
- Poster 1337: Institutionalizing infection prevention and control practices in health facilities in Liberia following the Ebola epidemic
 Scientific Session 87, Tuesday, 1:45 – 3:30 p.m. Marriott – La Galerie 1 & 2 – 2nd Floor: Improving procurement and redeployment of district level malaria commodities using SMS and web mapping in Madagascar
Scientific Session 87, Tuesday, 1:45 – 3:30 p.m. Marriott – La Galerie 1 & 2 – 2nd Floor: Improving procurement and redeployment of district level malaria commodities using SMS and web mapping in Madagascar
Poster Session C, Wednesday 31 October
- Poster 1816: Experiences and perceptions of care seeking for febrile illness among caregivers and providers in 8 districts of Madagascar
- Poster 1818: Improving adherence to national malaria treatment guidelines by village health workers in selected townships through a low-dose, high-frequency training approach
- Poster 1819: Improving malaria case management through national roll-out of Malaria Service and Data Quality Improvement (MSDQI): A Case study from Tanzania
- Poster 1820: Collaborative quality improvement framework to support data quality improvement, experience from 10 collaborative facilities in Uganda
- Poster 1821: Using malaria death audits to improve malaria case management and prevent future malaria related preventable deaths
- Poster 1833: Multiple approaches for malaria case management in the struggle to reach pre-elimination of malaria.
Scientific Session 182, Thursday, November 1, 10:15 am – 12:00 p.m. Marriott – Balcony I,J,K – 3rd Floor: Seasonal malaria chemoprevention, an effective intervention for reducing malaria morbidity and mortality
Case Management &Elimination &Epidemiology &Health Information &ITNs &Migration &Surveillance Bill Brieger | 20 Jul 2018
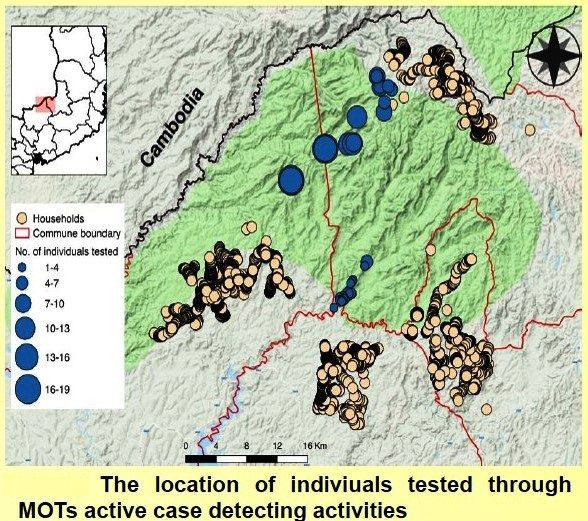
Establishing Mobile Outreach Teams (MOTs) for strengthening Active Case Detection with Mobile Populations in Vietnam 2016-2020
 Mobile migrant populations present a special challenge for malaria control and elimination efforts. Nguyen Ha Nam and colleagues* (Nguyen Xuan Thang, Gary Dahl, James O’Donnell, Vashti Irani, Sara Canavati, Jack Richards, Ngo Duc Thang, and Tran Thanh Duong) presented their study of this group at the recent Malaria World Congress. They are also sharing what they learned below.
Mobile migrant populations present a special challenge for malaria control and elimination efforts. Nguyen Ha Nam and colleagues* (Nguyen Xuan Thang, Gary Dahl, James O’Donnell, Vashti Irani, Sara Canavati, Jack Richards, Ngo Duc Thang, and Tran Thanh Duong) presented their study of this group at the recent Malaria World Congress. They are also sharing what they learned below.
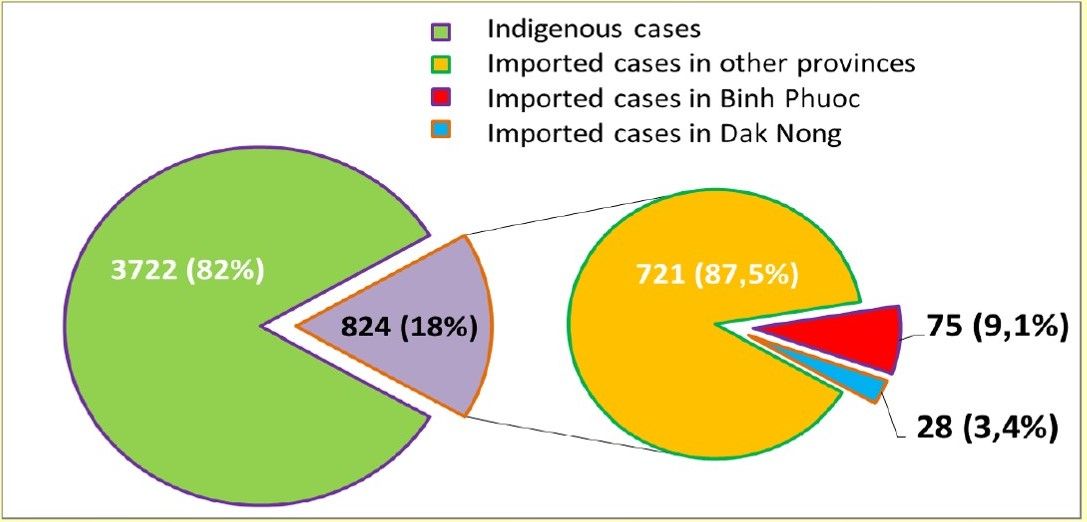
 Mobile Migrant Populations (MMPs) are a key population for containing the spread of malaria in the border areas between Cambodia and Vietnam. The number of imported cases in Viet Nam in 2017. 12,5% of such cases caught in Binh Phuoc and Dak Nong provinces and all of them came from Cambodia. The provinces bordering Cambodia and Vietnam have been had the highest malaria transmission intensity. This borders are frequented by MMPs who have proven difficult to target for surveillance and malaria control activities.
Mobile Migrant Populations (MMPs) are a key population for containing the spread of malaria in the border areas between Cambodia and Vietnam. The number of imported cases in Viet Nam in 2017. 12,5% of such cases caught in Binh Phuoc and Dak Nong provinces and all of them came from Cambodia. The provinces bordering Cambodia and Vietnam have been had the highest malaria transmission intensity. This borders are frequented by MMPs who have proven difficult to target for surveillance and malaria control activities.
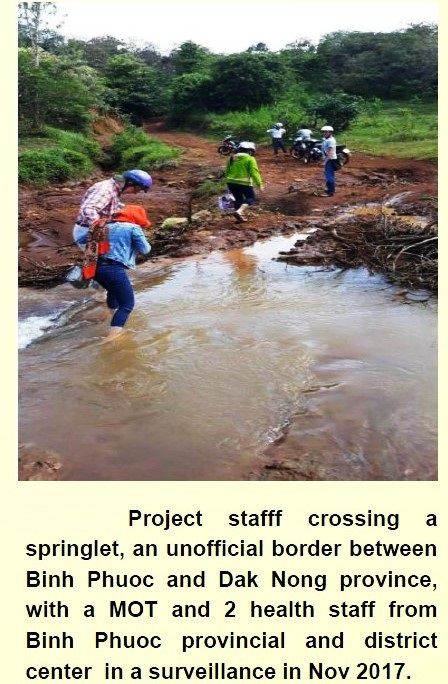
 Mobile Outreach Teams (MOTs) provide a potential approach to target malaria elimination activities for MMPs who may not be strongly supported by the regular village-based and clinic-based health services. This work describes the implementation of MOTs in Binh Phuoc and Dak Nong Provinces, which are high-risk regions along the Viet Nam-Cambodia border. These activities were conducted as part of the Regional Artemisinin-resistance Initiative (RAI) in 2017. Each MOT was comprised of 2 Commune Health Staff and 1 Village Health Worker (VHW) from the village nearest to the outreach area.
Mobile Outreach Teams (MOTs) provide a potential approach to target malaria elimination activities for MMPs who may not be strongly supported by the regular village-based and clinic-based health services. This work describes the implementation of MOTs in Binh Phuoc and Dak Nong Provinces, which are high-risk regions along the Viet Nam-Cambodia border. These activities were conducted as part of the Regional Artemisinin-resistance Initiative (RAI) in 2017. Each MOT was comprised of 2 Commune Health Staff and 1 Village Health Worker (VHW) from the village nearest to the outreach area.
In the first phase of the pilot, 3 communes of 2 districts in Binh Phuoc and 2 communes of 1 district in Dak Nong with highest malaria cases reported from NIMPE are selected as targeted areas. The Objectives were to …
- Design/tailor Mobile Outreach Information Education and Communication/Behaviour change communication (BCC/ IEC) Toolkit
- Intensify case detection and quality management by increasing the coverage of diagnostics and treatment for hard to reach populations
- Strengthen outreach to high-risk and under-served populations through MOT scouting activities to locate unreached Mobile Communities and map their locations
- Link MMPs with health facilities and Village Health Workers
 All MOT members were provided with smartphones and were trained on how to use the EpiCollect5 app to track malaria cases, record mapping information and upload real-time reports of these malaria cases. MOTs conducted 5-day outreach activities every month. These activities began with scouting out locations of the MMP communities.
All MOT members were provided with smartphones and were trained on how to use the EpiCollect5 app to track malaria cases, record mapping information and upload real-time reports of these malaria cases. MOTs conducted 5-day outreach activities every month. These activities began with scouting out locations of the MMP communities.
Once located, the MOTs geo-tagged the location of the community, conducted a short epidemiological survey on the community and screened for malaria using Rapid Diagnostic Tests and blood smear microscopy. Active malaria cases were provided with treatment according to the National guidelines, and Long Lasting Insecticidal Nets were distributed based on results of diagnosis and the survey.
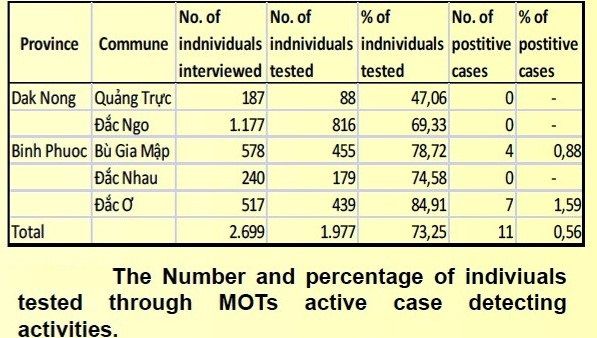 This action has led to increased diagnosis and treatment of hard to reach MMPs with increased access by those communities to malaria services. Improved understanding and increased use of malaria prevention practices hard to reach MMP communities/households. Mapped of previously unreached MMP Communities and unofficial border crossing points with malaria transmission hotspots and highly frequented crossing identified. The number of MMPs were monitored by MOTs were 2,699 accounting for 5.18% of the population in the project sites (2,699/52,095).
This action has led to increased diagnosis and treatment of hard to reach MMPs with increased access by those communities to malaria services. Improved understanding and increased use of malaria prevention practices hard to reach MMP communities/households. Mapped of previously unreached MMP Communities and unofficial border crossing points with malaria transmission hotspots and highly frequented crossing identified. The number of MMPs were monitored by MOTs were 2,699 accounting for 5.18% of the population in the project sites (2,699/52,095).
These screened MMPs were almost located along the border among project communes in Bu Gia Map National Forest where have a lot of unofficial border crossers, timber camp communities, and other revolving communities. 1,977 targeted people were tested for malaria. This number was achieved 73.25% of mobile migrant people (1,977/2,699). This work highlights how MOTs can target the previously unreached populations of MMPs to strengthen malaria surveillance and active case responses to reduce malaria transmission in Viet Nam.
 A system of real-time data collection of malaria cases from VHWs and MOTs using mobile phone uploads was established. Border screening and tracking hard to reach communities is a useful approach to implement to identify imported cases; however, it is labor-intensive, and misses subjects crossing at unofficial borders due to limited working time of MOTs (5 days a month).
A system of real-time data collection of malaria cases from VHWs and MOTs using mobile phone uploads was established. Border screening and tracking hard to reach communities is a useful approach to implement to identify imported cases; however, it is labor-intensive, and misses subjects crossing at unofficial borders due to limited working time of MOTs (5 days a month).
Positive cases in Binh Phuoc province are maintained for keeping track after receiving treatment due to no confirmed cases detected in targeted communes in Dak Ngo province, though these communes mainly have numerous transient timber camps moving in deep forests, and highly mobile border-crossers moving between regions and countries frequently. Future work will combine routine support from District health staff and expand the role of VHWs with motorbike provision for each MOT in order to not only to improve their quality outreach activities but also develop stronger Active Case Detection in the next phase of the project.
*Team members represent the National Institute of Malariology, Parasitology and Entomology, Hanoi, Viet Nam; Health Poverty Action, London, UK; and the Burnet Institute, Melbourne, Australia.
References
- Kheang ST, Lin MA, et al. Malaria Case Detection Among Mobile Populations and Migrant Workers in Myanmar: Comparison of 3 Service Delivery Approaches. 2018
- Shannon Takala-Harrison,a Christopher G. Jacob, et al. Independent Emergence of Artemisinin Resistance Mutations Among Plasmodium falciparum in Southeast Asia. 2014.
- Imwong M, Hien TT, et al. Spread of a single multidrug resistant malaria parasite lineage (PfPailin) to Vietnam. 2017.
- Richard J Maude,corresponding author Chea Nguon, et al. Spatial and temporal epidemiology of clinical malaria in Cambodia 2004–2013. 2014.
- Imwong M, Nguyen TN, et al.The epidemiology of subclinical malaria infections in South-East Asia: findings from cross-sectional surveys in Thailand–Myanmar border areas, Cambodia, and Vietnam. 2015.
- Hannah Edwards, Sara E. Canavati, et al. Novel Cross-Border Approaches to Optimise Identification of Asymptomatic and Artemisinin-Resistant Plasmodium Infection in Mobile Populations Crossing Cambodian Borders. 2015.
Advocacy &Case Management &Community &IPTp &ITNs Bill Brieger | 30 Apr 2018
Burkina Faso Celebrated World Malaria Day with Pledges to Defeat Malaria
 Burkina Faso celebrated World Malaria Day with pledges to Defeat Malaria on 25th April 2018. Dr Ousman Badolo. Technical Director of Jhpiego’s USAID/PMI Supported Improving Malaria Care (IMC) Project describes below the event in the village of Kamboinsin, not far from the capital, Ouagadougou. Ibrahim Sawadogo from IMC provided the photographs.
Burkina Faso celebrated World Malaria Day with pledges to Defeat Malaria on 25th April 2018. Dr Ousman Badolo. Technical Director of Jhpiego’s USAID/PMI Supported Improving Malaria Care (IMC) Project describes below the event in the village of Kamboinsin, not far from the capital, Ouagadougou. Ibrahim Sawadogo from IMC provided the photographs.
The day started with a proclamation of malaria day from Burkina Faso’s President, Roch Marc Christian Kaboré, to his assembled cabinet and the press. The president recognized that malaria is still a major public health issue in the country, and while deaths are decreasing, the incidence of malaria is not. The President called for a greater commitment of resources by all partners to insure that malaria can be defeated in Burkina Faso by 2030.
 Kamboinsin village in Sig-Noghin Health District was the site of further observances organized by the National Malaria Control Program, later that afternoon. This district was chosen because of having among the highest incidence rates for malaria in the region. Many partners set up booths to share their work in malaria with partners and citizens of the district. Included were three research centers (Centre Muraz, CNRFP and IRD), and three USAID programs supported by the President’s Malaria Initiative in Burkina Faso (Procurement and Supply Management [PSM], IMC and VectorLink), among others.
Kamboinsin village in Sig-Noghin Health District was the site of further observances organized by the National Malaria Control Program, later that afternoon. This district was chosen because of having among the highest incidence rates for malaria in the region. Many partners set up booths to share their work in malaria with partners and citizens of the district. Included were three research centers (Centre Muraz, CNRFP and IRD), and three USAID programs supported by the President’s Malaria Initiative in Burkina Faso (Procurement and Supply Management [PSM], IMC and VectorLink), among others.
 During the program both the Minister for Health and the US Ambassador spoke. The Minister highlighted the main strategies that Burkina Faso is employing to reduce and eliminate malaria including regular use of insecticide treated nets (ITN), seasonal malaria chemoprevention, Intermittent Preventive Treatment in Pregnancy (IPTp), Prompt and Appropriate Case Management and other Vector Control Strategies.
During the program both the Minister for Health and the US Ambassador spoke. The Minister highlighted the main strategies that Burkina Faso is employing to reduce and eliminate malaria including regular use of insecticide treated nets (ITN), seasonal malaria chemoprevention, Intermittent Preventive Treatment in Pregnancy (IPTp), Prompt and Appropriate Case Management and other Vector Control Strategies.
The US Ambassador shared a real-life story of a pregnant woman who during her current pregnancy decided to register early for Antenatal Care (ANC) as encouraged by the IMC project. She was able to get several doses of IPTp as required as well as obtain an ITN on her first visit, unlike in her previous pregnancies.
 Entertainment was provided by the comedian Hypolythe Wangrawa (alias M’ba Bouanga) who presented a sketch involving his ‘son’ who was not encouraging his wife to attend ANC and receive malaria prevention services. M’ba Bouanga chastised the son and an actor playing a midwife explained to the family the value of attending ANC and preventing malaria. Singers Maria Bissongo, Miss Oueora and Aicha Junior provided the audience with a song that embodied a variety of malaria prevention and care messages.
Entertainment was provided by the comedian Hypolythe Wangrawa (alias M’ba Bouanga) who presented a sketch involving his ‘son’ who was not encouraging his wife to attend ANC and receive malaria prevention services. M’ba Bouanga chastised the son and an actor playing a midwife explained to the family the value of attending ANC and preventing malaria. Singers Maria Bissongo, Miss Oueora and Aicha Junior provided the audience with a song that embodied a variety of malaria prevention and care messages.
 A highlight of the occasion was recognition of high performing health districts in the country. They were judged on criteria including good management of malaria commodity stocks, reduced case fatality rates, use of diagnostic tests to confirm malaria before treatment and coverage of at least three doses of IPTp. Four districts were given awards, Titao, Thyou, Boussouma and Batie, while Charles de Gaul Pediatric Hospital was also recognized.
A highlight of the occasion was recognition of high performing health districts in the country. They were judged on criteria including good management of malaria commodity stocks, reduced case fatality rates, use of diagnostic tests to confirm malaria before treatment and coverage of at least three doses of IPTp. Four districts were given awards, Titao, Thyou, Boussouma and Batie, while Charles de Gaul Pediatric Hospital was also recognized.
One can watch a video of the proclamation by the President on the National Facebook page. More details of the events are found in the following media: Lefaso.net and Paalga Observer.
World Malaria Day in Burkina Faso demonstrated the political will and commitment to “defeat malaria.” More and more national resources will be needed to reach the endline in 2030.
Advocacy &Case Management &Children &CHW &Community &Elimination &Funding &iCCM &Invest in Malaria Control &IPTp &ITNs Bill Brieger | 25 Apr 2018
On World Malaria Day the realities of resurgence should energize the call to ‘Beat Malaria’
 Dr Pedro Alonso who directed the World Health Organization’s Global Malaria Program, has had several opportunities in the past two weeks to remind the global community that complacency on malaria control and elimination must not take hold as there are still over 400,000 deaths globally from malaria each year. At the Seventh Multilateral Initiative for Malaria Conference (MIM) in Dakar, Dr Alonso drew attention to the challenges revealed in the most recent World Malaria Report (WMR). While there have been decreases in deaths, there are places where the number of actual cases is increasing.
Dr Pedro Alonso who directed the World Health Organization’s Global Malaria Program, has had several opportunities in the past two weeks to remind the global community that complacency on malaria control and elimination must not take hold as there are still over 400,000 deaths globally from malaria each year. At the Seventh Multilateral Initiative for Malaria Conference (MIM) in Dakar, Dr Alonso drew attention to the challenges revealed in the most recent World Malaria Report (WMR). While there have been decreases in deaths, there are places where the number of actual cases is increasing.
 Around twenty years ago the course of malaria changed with the holding of the first MIM, also in Dakar and the establishment of the Roll Bank Malaria (RBM) Partnership. These were followed in short order by the Abuja Declaration that set targets for 2010 and embodied political in endemic countries, as well as major funding mechanisms such as the Global Fund to fight AIDS, TB and Malaria. This spurred what has been termed a ‘Golden Decade’ of increasing investment and intervention coverage, leading to decreasing malaria morbidity and mortality. The Millennium Development Goals provided additional impetus to reduce the toll of malaria by 2015.
Around twenty years ago the course of malaria changed with the holding of the first MIM, also in Dakar and the establishment of the Roll Bank Malaria (RBM) Partnership. These were followed in short order by the Abuja Declaration that set targets for 2010 and embodied political in endemic countries, as well as major funding mechanisms such as the Global Fund to fight AIDS, TB and Malaria. This spurred what has been termed a ‘Golden Decade’ of increasing investment and intervention coverage, leading to decreasing malaria morbidity and mortality. The Millennium Development Goals provided additional impetus to reduce the toll of malaria by 2015.
 On Facebook Live yesterday Dr Alonso talked about that ‘Golden Decade.’ There was a 60% decrease in mortality and a 40% decreases in malaria cases. But progress slowing down and we may be stalled at a crossroads. He noted that history show unless accelerate efforts, malaria will come back with a vengeance. Not only is renewed political leadership and funding, particularly from affected countries needed, but we also need new tools. Dr Alonso explained that the existing tools allowed 7m deaths be diverted in that golden decade, but these tools are not perfect. We are reaching limits on these tools such that we need R&D for tools to enable quantum leap forward. Even old tools like nets are threatened by insecticide resistance, and research on alternative safe insecticides is crucial.
On Facebook Live yesterday Dr Alonso talked about that ‘Golden Decade.’ There was a 60% decrease in mortality and a 40% decreases in malaria cases. But progress slowing down and we may be stalled at a crossroads. He noted that history show unless accelerate efforts, malaria will come back with a vengeance. Not only is renewed political leadership and funding, particularly from affected countries needed, but we also need new tools. Dr Alonso explained that the existing tools allowed 7m deaths be diverted in that golden decade, but these tools are not perfect. We are reaching limits on these tools such that we need R&D for tools to enable quantum leap forward. Even old tools like nets are threatened by insecticide resistance, and research on alternative safe insecticides is crucial.
 Dr Alonso at MIM pointed to the worrying fact that investment in malaria overall peaked in 2013. Investment by endemic countries themselves has remained stable throughout and never gone reached $1 billion despite advocacy and leadership groups like the Africa Leaders Malaria Alliance. The 2017 WMR shows that while 16 countries achieved a greater that 20% reduction in malaria cases, 25 saw a greater that 20% increase in cases. The outnumbering of decreasing countries by increasing was 4 to 8 in Africa, the region with the highest burden of the disease. Overall 24 African countries saw increases in cases between 2015 and 2016 versus 5 that saw a decrease. A review of the Demographic and Health and the Malaria Information Surveys in recent years show that most countries continue to have difficulty coming close to the Abuja 2010 targets for Insecticide treated net (ITN) use, prompt and appropriate malaria case management and intermittent preventive treatment of malaria in pregnancy (IPTp).
Dr Alonso at MIM pointed to the worrying fact that investment in malaria overall peaked in 2013. Investment by endemic countries themselves has remained stable throughout and never gone reached $1 billion despite advocacy and leadership groups like the Africa Leaders Malaria Alliance. The 2017 WMR shows that while 16 countries achieved a greater that 20% reduction in malaria cases, 25 saw a greater that 20% increase in cases. The outnumbering of decreasing countries by increasing was 4 to 8 in Africa, the region with the highest burden of the disease. Overall 24 African countries saw increases in cases between 2015 and 2016 versus 5 that saw a decrease. A review of the Demographic and Health and the Malaria Information Surveys in recent years show that most countries continue to have difficulty coming close to the Abuja 2010 targets for Insecticide treated net (ITN) use, prompt and appropriate malaria case management and intermittent preventive treatment of malaria in pregnancy (IPTp).
 The coverage gap is real. The WMR shows that while there have been small but steady increase in 3 doses of IPTp, coverage of the first dose has leveled off. Also while ownership of a net by households has increased, less than half of households have at least one net for every two residents.
The coverage gap is real. The WMR shows that while there have been small but steady increase in 3 doses of IPTp, coverage of the first dose has leveled off. Also while ownership of a net by households has increased, less than half of households have at least one net for every two residents.
In contrast a new form of IPT – seasonal malaria chemoprevention (SMC) for children in the Sahel countries has taken off with over 90% of children receiving at least one of the monthly doses during the high transmission season. Community case management is taking off as is increased use of rapid diagnostic testing. Increased access to care may explain how in spite of increased cases, deaths can be reduced. This situation could change rapidly if drug resistance spreads.
 While some international partners are stepping up, we are far short of the investment needed. The Gates Foundation is pledging more for research and development to address the need for new tools as mentioned by Dr Alonso. A big challenge is adequate funding to sustain the implementation of both existing tools and the new ones when they come online. Even in the context of a malaria elimination framework, WHO stresses the need to maintain appropriate levels of intervention with case management, ITNs and other measures regardless of the stage of elimination at which a country or sub-strata of a country is focused.
While some international partners are stepping up, we are far short of the investment needed. The Gates Foundation is pledging more for research and development to address the need for new tools as mentioned by Dr Alonso. A big challenge is adequate funding to sustain the implementation of both existing tools and the new ones when they come online. Even in the context of a malaria elimination framework, WHO stresses the need to maintain appropriate levels of intervention with case management, ITNs and other measures regardless of the stage of elimination at which a country or sub-strata of a country is focused.
Twenty years after the formation of RBM and 70 years after the foundation of WHO, the children, families and communities of endemic countries are certainly ready to beat malaria. The question is whether the national and global partners are equally ready.
Case Management &Children Bill Brieger | 19 Apr 2018
Improved Malaria Case Management of Children under Age 5: The Experience of the MCSP Restoration of Health Services Liberia Project
Catherine Gbozee, Birhanu Getahun, Topian Zikeh, Anne Fiedler, and Allyson Nelson of the Maternal and Child Survival Program (Jhpiego and John Snow, Inc.) have presented experiences on improving malaria case management for children in Liberia at the 7th Multilateral Initiative for Malaria Conference in Dakar. Below are their findings.
 In malaria-endemic countries, malaria is the second leading cause of mortality for children under the age of 5 years. In Liberia Mortality rate for children under the age of 5 years was 94 per 1,000 in 2013. Malaria accounts for 31% of outpatient mortality for children under the age of 5 years and 51% of all outpatient consultations. Malaria among children under the age of 5 years accounts for 20.5% of all outpatient consultations in Liberia Health services weakened by the epidemic of Ebola virus disease. Over 40% of children under the age of 5 years have tested positive for malaria using malaria rapid diagnostic tests (mRDTs) since 2009 (see Figure 1)
In malaria-endemic countries, malaria is the second leading cause of mortality for children under the age of 5 years. In Liberia Mortality rate for children under the age of 5 years was 94 per 1,000 in 2013. Malaria accounts for 31% of outpatient mortality for children under the age of 5 years and 51% of all outpatient consultations. Malaria among children under the age of 5 years accounts for 20.5% of all outpatient consultations in Liberia Health services weakened by the epidemic of Ebola virus disease. Over 40% of children under the age of 5 years have tested positive for malaria using malaria rapid diagnostic tests (mRDTs) since 2009 (see Figure 1)
 Maternal and Child Survival Program (MCSP) Restoration of Health Services (RHS) Project Objectives for malaria include prevention at facilities, Strengthen infection prevention and control (IPC) practices at 77 health facilities through training, intensive supportive supervision, triage, improvement of waste management, and provision of essential IPC commodities and supplies, Increased utilization of and demand for maternal and child health services—Restore delivery of quality primary health care services through implementation of integrated reproductive, maternal, newborn, child, and adolescent health as part of the Essential Package of Health Services in 77 facilities.
Maternal and Child Survival Program (MCSP) Restoration of Health Services (RHS) Project Objectives for malaria include prevention at facilities, Strengthen infection prevention and control (IPC) practices at 77 health facilities through training, intensive supportive supervision, triage, improvement of waste management, and provision of essential IPC commodities and supplies, Increased utilization of and demand for maternal and child health services—Restore delivery of quality primary health care services through implementation of integrated reproductive, maternal, newborn, child, and adolescent health as part of the Essential Package of Health Services in 77 facilities.
 MCSP RHS supported health facilities in three counties
MCSP RHS supported health facilities in three counties
- Grand Bassa: 30 (91% of health facilities in county)
- Lofa: 17 (27% of health facilities in county)
- Nimba: 30 (46% of health facilities in county)
- Population coverage: 900,000 (20% of total population)
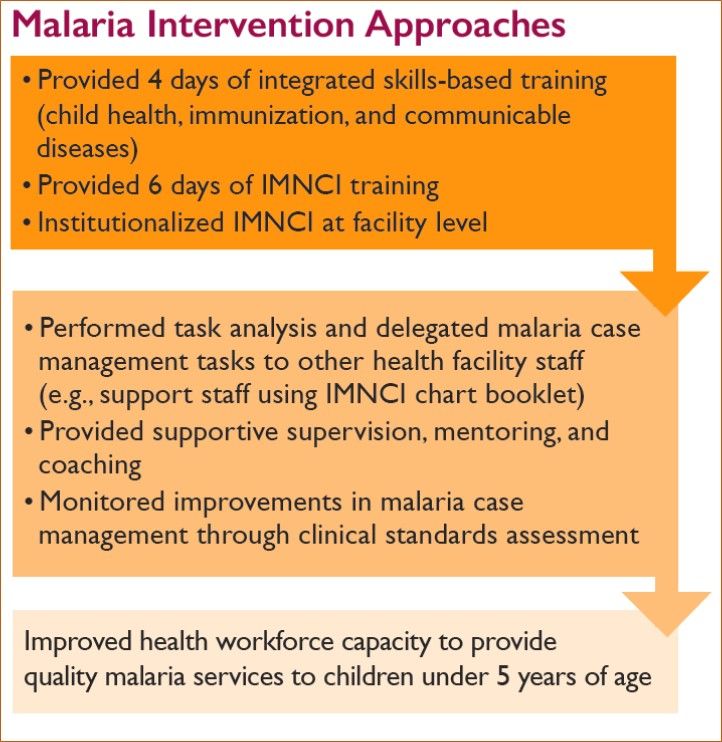 Liberia Malaria Indicator Survey 20164 showed that mRDT was done for only 43% and 44% of children with fever in North Central and South Central regions, respectively. Treatment with artemisinin-based combination therapy (ACT) improved from 43% to 81% from 2013 to 2016. Intervention approaches are outlined at the left.
Liberia Malaria Indicator Survey 20164 showed that mRDT was done for only 43% and 44% of children with fever in North Central and South Central regions, respectively. Treatment with artemisinin-based combination therapy (ACT) improved from 43% to 81% from 2013 to 2016. Intervention approaches are outlined at the left.
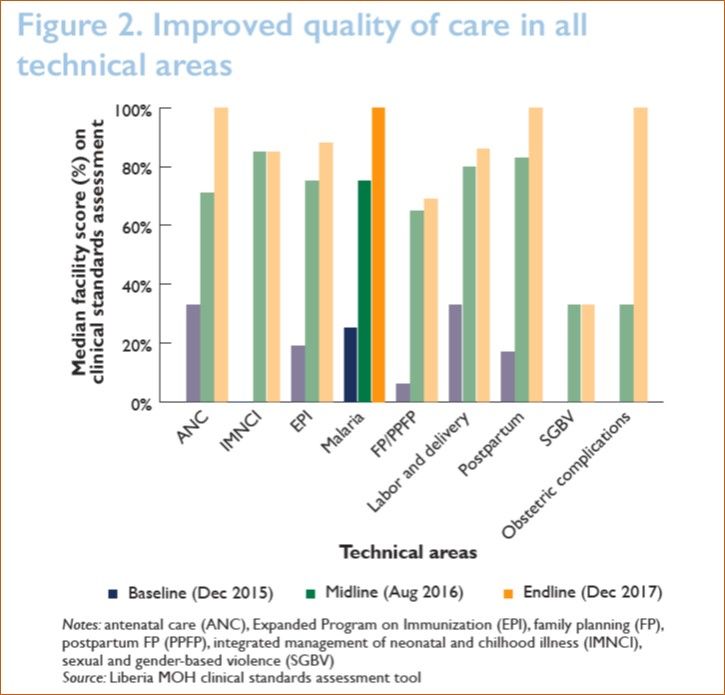
Scores for all technical areas, including malaria, improved
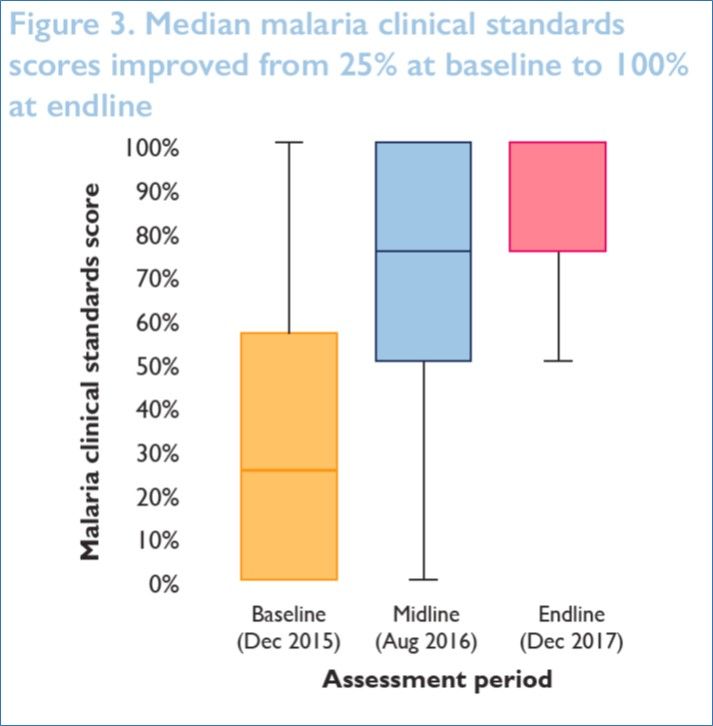
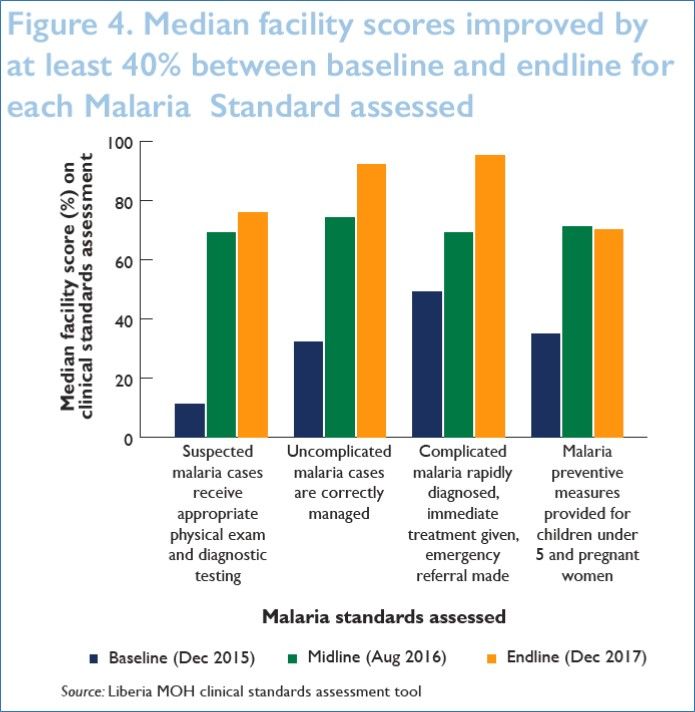
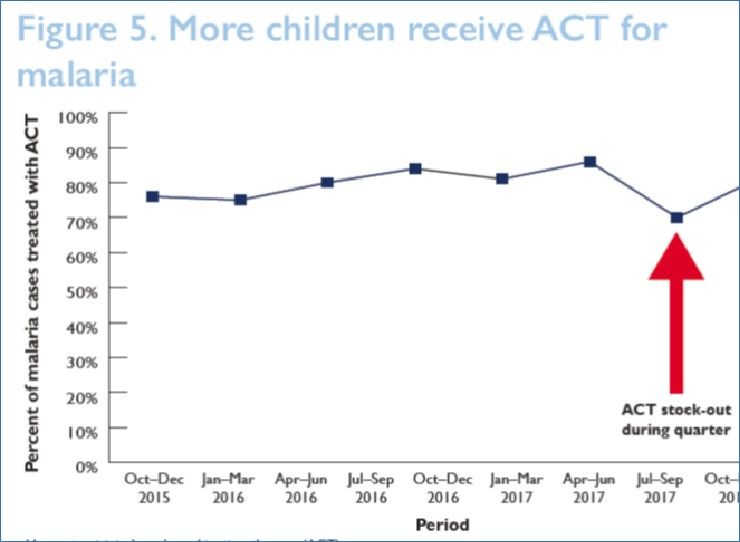
from baseline to endline (see Figure 2). Median facility scores for adherence to malaria clinical standards improved by 75% between baseline and endline in half of MCSP facilities sampled (see Figures 3 and 4). Percent of malaria cases in children under 5 years of age receiving ACT for malaria in MCSP-supported facilities improved from 76% to 82%, despite sporadic stock-outs of ACT (see Figure 5)
Challenges included Frequent stock-outs of mRDTs and ACT. There were Bad roads and broken bridges challenging for supportive supervision, malaria commodity distribution, and facility accessibility to users.
Lessons Learned included Task-shifting and comprehensive hands-on health workforce improvement approaches are essential for revamping and improving quality care provision in post-disaster settings such as Liberia. Uninterrupted and sustained supplies of mRDTs, ACT, and malaria commodities are key for quality malaria case management.
References
1. World Health Organization (WHO). 2015. MCEE-WHO methods and data sources for child causes of death 2000–2015. WHO website.
http://www.who.int/healthinfo/global_burden_disease/ChildCOD_method_2000_2015.pdf. Accessed April 2, 2018.
2. Liberia Institute of Statistics and Geo-Information Services (LISGIS), Ministry of Health and Social Welfare Liberia, National AIDS Control Program Liberia, et al. 2014.
Liberia demographic and health survey 2013. Demographic and Health Surveys Program website. https://dhsprogram.com/pubs/pdf/fr291/fr291.pdf. Accessed April 2, 2018.
3. Liberia Ministry of Health. Liberia Ministry of Health Annual Report 2015. Monrovia, Liberia: Ministry of Health.
4. National Malaria Control Program, Liberia Institute of Statistics and Geo-Information Services, and The DHS Program. 2017. Liberia Malaria Indicator Survey 2016.
The Demographic and Health Surveys Program website. http://dhsprogram.com/pubs/pdf/MIS27/MIS27.pdf. Accessed April 2, 2018.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Case Management Bill Brieger | 16 Apr 2018
Febrile Illness Case Management in Madagascar: Lessons from a Facility Provider Case Scenario Assessment
Rachel Favero, Jean Pierre Rakotovao, Lalanirina Ravony, Reena Sethi, Katherine Wolf, Barbara Rawlins, Eliane Razafimandimby, Andrianandraina Ralaivaomisa, Toky Rakotondrainibe, Mamy Razafimahatratra, Thierry Franchard, Sedera Mioramalala, Joss Razafindrakoto, and Catherine Dentinger of the Maternal and Child Survival Program/Jhpiego, the National Malaria Control Programme and the United States Agency for International Development/Madagascar examine malaria care seeking in Madagascar. Their findings were presented at the 7th Multilateral Initiative for Malaria Conference in Dakar and are shared below.
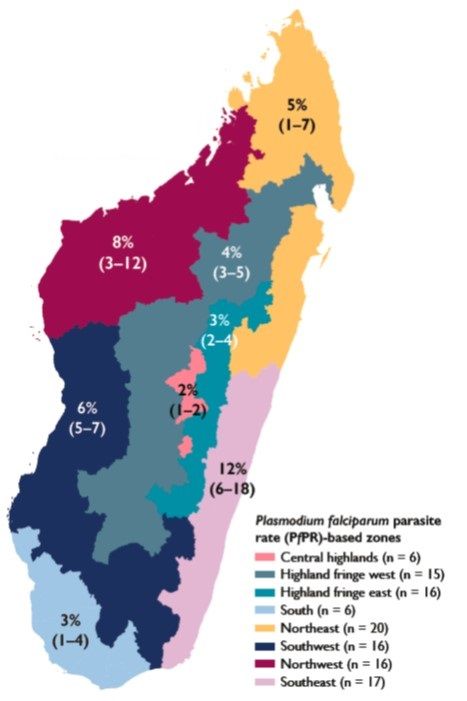 In 2016, malaria accounted for 5.9% of outpatient visits and 6.7% of all deaths in Madagascar. Care is often delayed and the recommended treatment protocols for management of febrile illness are not systematically applied. Children and adults do not always receive medication for febrile illness and when they do, it is not always the correct medication or dosage, as noted in MEDALI (Mission d’Etude des Déterminants de l’Accès aux Méthodes de Lutte antipaludique et de leur Impact) Quantitative and Qualitative 2014.
In 2016, malaria accounted for 5.9% of outpatient visits and 6.7% of all deaths in Madagascar. Care is often delayed and the recommended treatment protocols for management of febrile illness are not systematically applied. Children and adults do not always receive medication for febrile illness and when they do, it is not always the correct medication or dosage, as noted in MEDALI (Mission d’Etude des Déterminants de l’Accès aux Méthodes de Lutte antipaludique et de leur Impact) Quantitative and Qualitative 2014.
Study Goals aimed to Identify gaps, attitudes, and practices that may Prevent timely care seeking for febrile illness (within 24 hours after onset of fever) in the formal health system and Lead to nonadherence to national guidelines for malaria treatment. Key assessment questions included What strategies could be adopted to encourage pregnant women and caregivers of children under age 15 to use the formal health system as their primary resource for treatment of febrile illness? The study also asked What are the reasons that health providers do not systematically apply national malaria treatment guidelines?
 Study districts were sampled from eight malaria operational zones. In-depth interviews with the following groups (N = 90). Facility health care providers, both public and private were included as were Community health workers and Caregivers of children under age 15 and pregnant women. Focus group discussions were held with caregivers of children
Study districts were sampled from eight malaria operational zones. In-depth interviews with the following groups (N = 90). Facility health care providers, both public and private were included as were Community health workers and Caregivers of children under age 15 and pregnant women. Focus group discussions were held with caregivers of children
under the age of 15 years, including pregnant women (N = 16).
A Case scenario was reviewed with facility providers (N = 15). A case scenario is a description of a made-up situation involving a decision to be made or a problem to be solved. The case scenario used was febrile illness in children and pregnant women. This scenario allowed the study team to understand provider response. Provider responses to the scenarios are seen below.
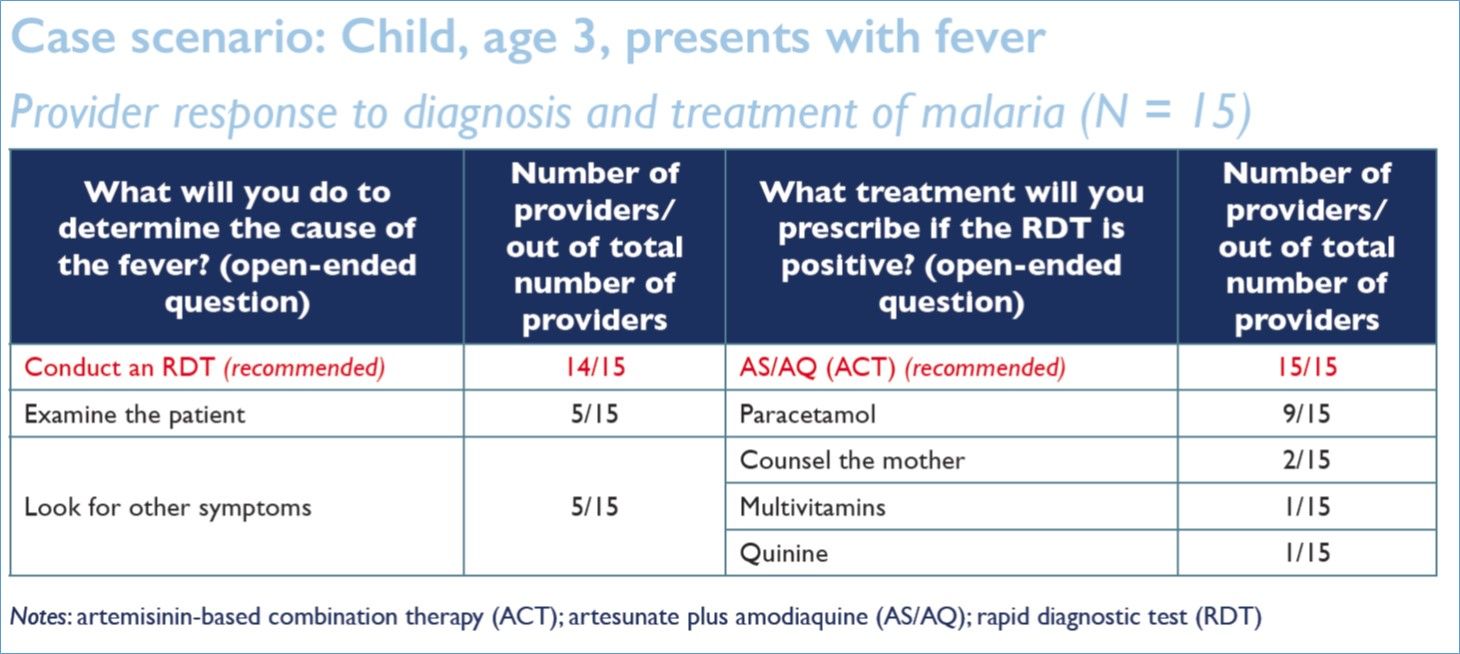
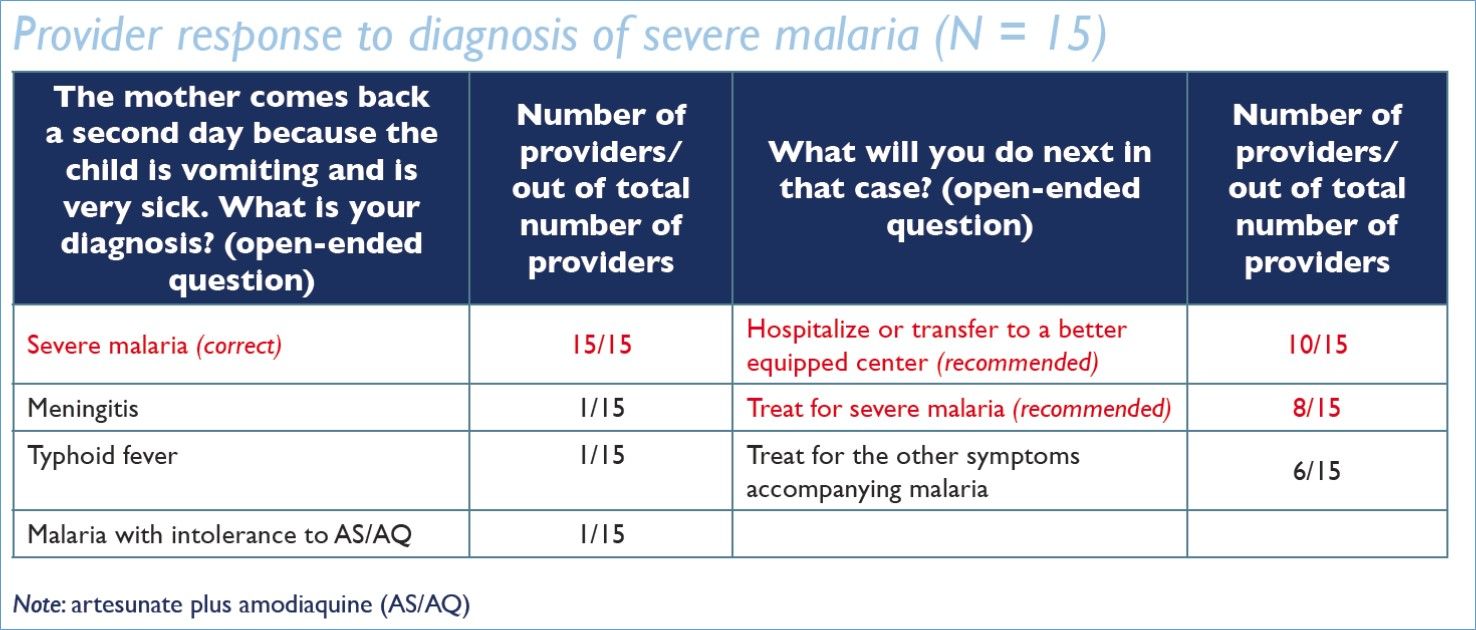

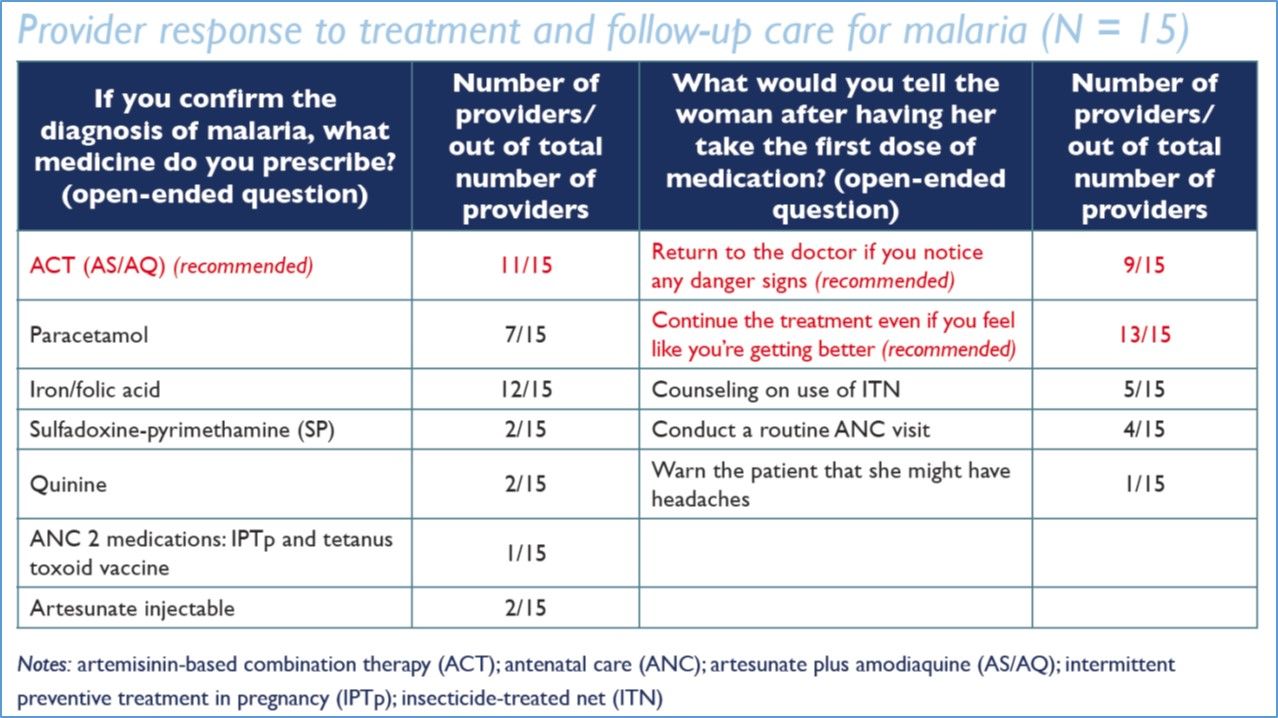
From the review of case studies one could see that Facility provider diagnosis and treatment of malaria does not always conform to national protocol. Therefore, Targeted efforts to improve provider knowledge and practice are needed. Effort must be made to Ensure that standards/protocols are available in the health facilities and that providers have received guidance on the standards/protocols. Finally, Supportive supervision should be provided to address gaps in knowledge and practice.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID, PMI, or the United States Government.
Case Management &CHW &IPTp &ITNs Bill Brieger | 14 Apr 2018
Community Health Volunteers Contribute to Improved Malaria Prevention and Management in Kribi, Cameroon
Kodjo Morgah, Eric Tchinda, and Naibei Mbaïbardoum of Jhpiego (a Johns Hopkins University Affiliate) in Cameroon are presenting a poster at the Multilateral Initiative for Malaria Conference in Dakar this week. Their findings, seen below, show how community health volunteers can contribute to improving the quality of malaria control services in Chad and Cameroon.

CHV Lilian Kubeh preparing to administer a rapid diagnostic test. Photo by Karen Kasmauski.
Project objectives focused overall on contributing to the reduction of malaria-related morbidity and mortality in Cameroon and Chad. It also aimed to strengthen community-based interventions through the use of community health volunteers (CHVs) to manage simple cases of malaria and conduct awareness-raising activities. The geographic scope of the project was Kribi District in the south of Cameroon. Thirty-two health facilities are supported by Jhpiego. Kribi District has an estimated population of 134,876.
Reports from the National Malaria Control Program show that malaria is the leading cause of morbidity in Cameroon—an estimated 1,500,000 cases occur each year. In 2016, it was the leading reason for medical consultations (23.6% of all medical consultations) and hospitalizations (46% of all hospitalizations). Among children under 5 years of age, malaria accounted for 41% of all medical consultations and 55% of all hospitalizations. Malaria is also a leading cause of mortality. In 2016, Cameroon had 2,639 deaths caused by malaria—12% of all deaths across all age groups and 28% of all deaths among children under 5 years of age were attributed to malaria.
 Project intervention strategies target the four levels of the health system. The CHV intervention was mobilized to support the strategy at the community level as seen in the attached diagram. In 2012 and 2014, 38 CHVs were selected by the community and received training to support areas in the district more than 10 km from a health center. (Note: 10 km was the measurement tool used to determine the geographic scope of each CHV for this project.) An initial donation of medications, data collection tools, and small equipment was made available to CHVs using funding from ExxonMobil Foundation. An evaluation of the training intervention was conducted by an external consultant in April 2016.
Project intervention strategies target the four levels of the health system. The CHV intervention was mobilized to support the strategy at the community level as seen in the attached diagram. In 2012 and 2014, 38 CHVs were selected by the community and received training to support areas in the district more than 10 km from a health center. (Note: 10 km was the measurement tool used to determine the geographic scope of each CHV for this project.) An initial donation of medications, data collection tools, and small equipment was made available to CHVs using funding from ExxonMobil Foundation. An evaluation of the training intervention was conducted by an external consultant in April 2016.

CHV Daniel Ze conducting an individual educational session on IPTp. Photo by Karen Kasmauski.
CHVs conduct outreach activities in their communities—via home visits and community education sessions—to provide health education on malaria transmission and prevention, use of long-lasting insecticidal nets, the importance of intermittent preventive treatment in pregnancy (IPTp), and the importance of promptly seeking medical care for suspected cases of malaria. CHVs also support national health campaigns and health promotion events, including World Malaria Day. In Cameroon, where CHVs are also able to test and treat patients, they administer rapid diagnostic tests (RDTs) and treat cases of uncomplicated malaria.
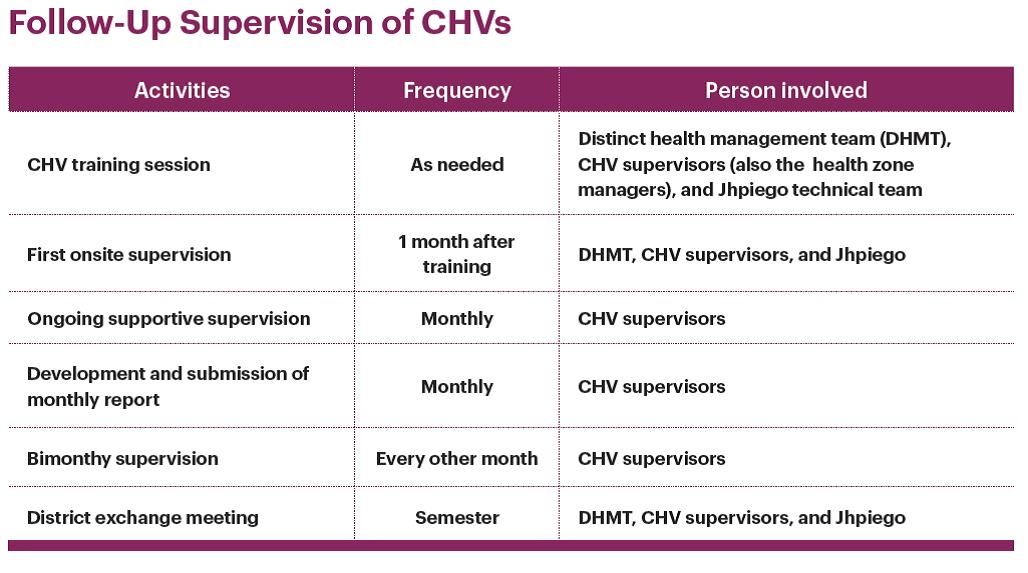 Motivation of CHVs included ongoing training and technical updates, regular replenishment of materials, CHVs are recognized and respected community leaders, provision of per diem and transport costs, and continued advocacy targeting district officials to provide CHV stipends to ensure sustainability. Attached are details of the supervisory activities that provided continual technical support to the CHVs to ensure that they retain knowledge and skills to carry out their activities and track their data.
Motivation of CHVs included ongoing training and technical updates, regular replenishment of materials, CHVs are recognized and respected community leaders, provision of per diem and transport costs, and continued advocacy targeting district officials to provide CHV stipends to ensure sustainability. Attached are details of the supervisory activities that provided continual technical support to the CHVs to ensure that they retain knowledge and skills to carry out their activities and track their data.
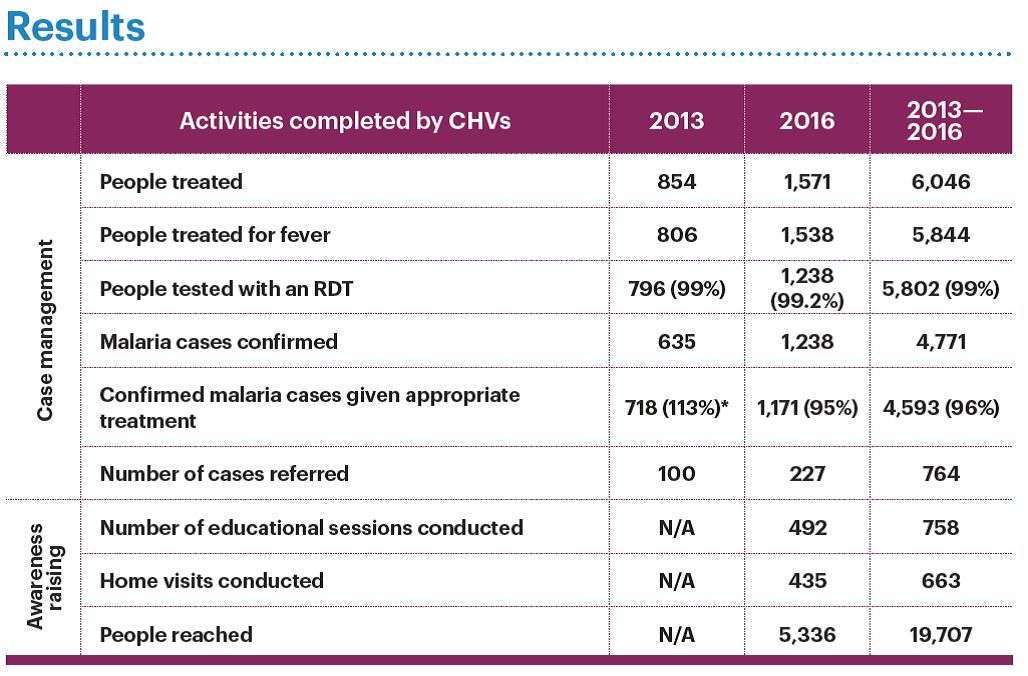 Between 2013 and 2016 CHVs in these communities were able to reach nearly 20,000 people with a variety of malaria services as seen in the attached table. The project paid close attention to data quality, which was reviewed with the CHVs on a regular basis, resulting in improved data quality. CHVs improved the accessibility of malaria prevention and care services for communities living in remote areas. Results from April 2016 external evaluation show these results. Knowledge of malaria prevention is significantly higher in households that did not receive CHV support (p = 0.001). Use of long-lasting insecticide-treated nets is higher in households that benefitted from CHV support (88%) than in households that did not benefit from CHV support (73%) (p = 0.023). There was an increase in the delivery of IPTp2, from 60% in 2012 to 70% in 2016.
Between 2013 and 2016 CHVs in these communities were able to reach nearly 20,000 people with a variety of malaria services as seen in the attached table. The project paid close attention to data quality, which was reviewed with the CHVs on a regular basis, resulting in improved data quality. CHVs improved the accessibility of malaria prevention and care services for communities living in remote areas. Results from April 2016 external evaluation show these results. Knowledge of malaria prevention is significantly higher in households that did not receive CHV support (p = 0.001). Use of long-lasting insecticide-treated nets is higher in households that benefitted from CHV support (88%) than in households that did not benefit from CHV support (73%) (p = 0.023). There was an increase in the delivery of IPTp2, from 60% in 2012 to 70% in 2016.
In conclusion CHVs have increased their communities’ access to health centers through referrals, health education on malaria prevention, IPTp, and treatment for simple and severe cases of malaria. Regular supervision of CHVs by their supervisors (the health zone managers) is essential to maintaining and strengthening CHV performance and motivation. Continuing advocacy efforts with local authorities is necessary to ensure that CHV activities are sustainable. The project team aims to establish a mechanism to improve documentation of its activities to better measure the impact on indicators at the community, facility, and district levels, and provide evidence for advocacy to sustain these efforts.