Case Management &Essential Medicines Bill Brieger | 26 Dec 2018
The Essential Health Service Package in Nigeria
When examining the service delivery building block of a health system we much ask what, how and where? “What” addresses the package of services, “How” describes the mechanisms and personnel who do the delivery, and “Where” considers making services accessible in or very near the community. These are the issues explored in this case study on Nigeria. As USAID notes, “An Essential Package of Health Services (EPHS) can be defined as the package of services that the government is providing or is aspiring to provide to its citizens in an equitable manner. Essential packages are often expected to achieve multiple goals: improved efficiency, equity, political empowerment, accountability, and altogether more effective care.”[i]
Although Nigeria has held Primary Health Care as the official foundation of its national health policy since 1986, it took nearly 30 years to give legal backing to a standard service package with the legislative passage and presidential signing of the National Health Bill in 2014. The law says that “all citizens shall be entitled to a basic minimum package of health services…” defined as “the set of health services as may be prescribed from time to time by the Minister after consultation with the National Council on Health” (National Health Bill, 2014 (SB. 215)).1
Up until that time one could infer the existence of an essential medicines list for primary care through the “Standing Orders” service provision algorithms.[ii] These algorithms guide front line health staff known as community health extension workers (CHEWs) in providing quality and accurate treatment and prevention for common illnesses. The Standing Orders also form the basis for training for CHEWs. For each area, “there is a set of actions including health education, further investigation, treatment, and follow-up necessary for good client’s care.”
As an example of essential medicines, the section of an algorithm for fever management below indicates that Artemisinin-Based Combination Treatment (ACT) malaria medicines and Long-Lasting Insecticide-Treated Nets (LLINS) for malaria prevention should be part of the basic package found at the front line.

USAID describes the official service delivery system in Nigeria as organized in three tiers. Tertiary facilities operated by the Federal Ministry of Health are the highest level of health care and serve as referral centers for patients. State Ministries of Health manage secondary facilities, which provide some specialized health services. Local Government Area (LGA) PHC Departments manage primary facilities, which provide the most basic entry point to the health care system-health centers, clinics, and dispensaries. It is at the LGA level in frontline PHC clinics where the CHEWs mentioned above function and deliver the basic package. Volunteer CHW programs exist and are often run by NGOs and are poorly coordinated, although efforts in recent years have aimed at standardizing their training and activities.
In reality, Nigerians at the community level face a mosaic of health service delivery mechanisms ranging from LGA clinics and dispensaries, patent medicine shops, private clinics often run by nurses and licensed to physicians living in the city, and a range of indigenous practitioners (herbalists, bone setters) and faith healers (based in all major religious groups).[iii]

The USAID report on Nigeria’s essential services shows major challenges in health equity.1
- Coverage is low for reproductive health, maternal health, and immunization varies widely and is strongly associated with wealth, education level, and rural versus urban place of residence.
- On some measures, health services coverage among populations with urban residence is more than double the coverage among populations with rural residence.
- Only about 30% of women in the poorest households receive at least one antenatal care visit, compared to over 90 percent of woman in the wealthiest households, with service coverage steeply increasing along with wealth.
- Coverage of most key preventive and curative health services is relatively low with large disparities in geopolitical zones, between rural and urban zones, and with regard to socioeconomic status; the poorest fifth of the population are much less likely to receive medical services than their counterparts in the wealthiest 20 percent of the population.
USAID’s Health Financing and Governance Project,1 helped group the Essential Package of Care into three “service delivery modes”:
- family-oriented, community-based services that can be delivered on a daily basis by trained community health, nutrition or sanitation promoters with periodic supervision from skilled health staff;
- population- oriented, schedulable services that require health workers with basic skills (e.g. auxiliary nurses/midwives and other paramedical staff) and that can be delivered either by outreach or in health facilities in a scheduled way; and
- individually oriented clinical services that require health workers with advanced skills (such as registered nurses, midwives or physicians) available on a permanent basis.
These modes come along with recommended actions which could
be interventions like safe water for the family or drugs like antibiotics for
child pneumonia. Therefore, at present the package focuses more on essential
interventions (than essential medicines) for groups such as adolescents,
pregnant women, women in childbirth, and infants and children among other
populations to be reached with of RMNCH services (reproductive, maternal,
neonatal, and child health).
In conclusion, Nigeria has articulated its PHC
service delivery in terms of what, how and where, but has some ways to go in
articulating a clear essential package across the life span and ensuring
equitable access to and provision of these services across the country and
among all income groups.
[i] Wright, Jenna (2016), ESSENTIAL PACKAGE OF HEALTH SERVICES COUNTRY SNAPSHOT: NIGERIA. United States Agency for International Development (USAID), Health Finance and Governance Project (Abt Associates). https://www.hfgproject.org/essential-package-of-health-services-country-snapshot-nigeria/
[ii] National Primary Health Care Development Agency (2015) NATIONAL STANDING ORDERS FOR COMMUNITY HEALTH OFFICERS/COMMUNITY HEALTH EXTENSION WORKERS, Revised By CHPRBN IN COLLABORATION WITH NPHCDA. Nigeria Federal Ministry of Health, Abuja.
[iii] Brieger WR. PHC: in search of a system that works. Africa Health 1987; 10: 30 31,26.
Case Management &Drug Quality &Essential Medicines Bill Brieger | 24 Dec 2018
Burkina Faso Ensures Essential Medicines Reach the Front Line
Meike Schleiff of the Department of International Health, The JHU Bloomberg School of Public Health has explored how Burkina Faso manages to get essential medicines, including those for malaria, to the front line health services. She explains that the World Health Organization (WHO) has determined essential medicines to be, “those that satisfy the priority health care needs of the population. They are selected with due regard to public health relevance, evidence on efficacy and safety, and comparative cost-effectiveness.”(WHO, 2018) These medicines should be available as part of health systems functioning to all persons at appropriate amounts, affordable costs, quality standards and sufficient information assured to consumers. Every country develops an essential drug list,

In Burkina Faso, approval of modern medicines (specialty and generic), traditional pharmacopoeial drugs, medical consumables and medical biology reagents is assigned to the Drug Regulatory Directorate (DRP).
Essential Medicines in Burkina Faso are purchased and distributed primarily through the Centrale d’Achats des Médicaments Essentiels (CAMEG), or Central Purchasing of Essential Drugs system.(CAMEG, 2018) This CAMEG system operates with two agencies in Ouagadougou, and then has seven additional agencies in other zones of the country (see map). From the zonal agencies, the CAMEG supplies 67 District Dispatching Depots (DRDs), and also supplies University Hospital Centers, regional hospitals, and additional services provided by the Ministry of Health. For the private sector, the CAMEG manages supplies for NGOs, faith-based organizations, medical laboratories, pharmaceutical companies, and the Global Fund for HIV, tuberculosis, and malaria.(CAMEG, 2018)
Before the CAMEG was created, access to essential medicines and supplies was very difficult, particularly for rural and other hard to reach populations. This was due to geographical access as well as high prices for specialty drugs, limited availability of generic drugs, and prohibitive regulations against the introduction of generic medicines. In response to this situation, the CAMEG was created under a presidential decree in 1992 and commenced activities in 1994. In 1997, an evaluation was carried out to determine the impact of the CAMEG and decide whether to continue the activities through a long-term structure; the results of this evaluation proposed establishing a legally and financially autonomous non-profit entity to carry forward the work of the CAMEG.(CAMEG, 2018) Today, the CAMEG manages the selection of drug suppliers for the country, ensures compliance with WHO and national regulations on price and quality, and facilitates distribution and storage of drugs across the country. A full product list of the drugs managed by the CAMEG can be found on their website (www.cameg.com).

Community Level
The availability of essential generic medicines at health and social welfare centres in Burkina Faso is 74.5%, compared with an average of 40% across the African region and less than 60% globally.(World Health, 2016, Ministry of Health, 2010) For hospitals, rates are slightly lower with 61% of generics available and regional hospital centers and 39% at university hospital centers (Saouadogo and Compaore, 2010), but only 1.2% of branded medicines; this situation results in patients who are referred to hospitals from lower level facilities often being forced to purchase medicines from more expensive private pharmacies in order to receive the necessary care at higher levels of the health system.(Vervoort, 2012)
While immense progress has been made in ensuring affordability and accessibility of essential medicines in Burkina Faso, mark-ups at different points along the supply chain still result in prohibitively high prices at final points of sale; patients still pay for 37% of the cost of essential medicines and remain the single greatest healthcare cost for households in Burkina and a burden for the majority of the population who still live on less than $1.25 per day.(Vervoort, 2012)
References
CAMEG 2018. Centrale d’Achats des Médicaments Essentiels. Ouagadougou, Burkina Faso.
Ministry of Health 2010. Measuring the Price, Availability, Financial Accessibility, and Price Composition of Medicines in Burkina Faso. Ouagadougou, Burkina Faso: Ministry of Health of Burkina Faso.
Saouadogo, H. and Compaore, M. (2010) ‘Essential Medicines Access Survey in Public Hospitals in Burkina Faso’, 4(6), pp. 373-380.
Vervoort, K. 2012. Ensuring the Availability of Essential Medicines in Burkina Faso: A Shared Responsibility.
WHO 2018. Essential Medicines. Geneva, Switzerland.
World Health, O. (2016) Burkina Faso: Country Cooperation Strategy. Available at: http://apps.who.int/iris/bitstream/handle/10665/136973/ccsbrief_bfa_en.pdf (Accessed: May).
Case Management &Funding &Insurance &Uncategorized Bill Brieger | 17 Dec 2018
Community Based Health Insurance Can Fight Malaria
Community-Based Health Insurance (CBHI) is seen as a way to promote universal health coverage and protect vulnerable populations from catastrophic financial effects of illness. Malaria can be such an illness is not treated in a timely manner, and having insurance can help prevent delays.

In countries including Rwanda, Burkina Faso and Senegal a particular CBHI scheme known as mutuelles has taken root. For Rwanda USAID (2018) reports that …
The 2014–2015 DHS showed that insurance coverage has remained stable since the 2010DHS and that 79 percent of the households have at least one family member with health insurance and that among those insured 97 percent have community health insurance (mutuelles). Early ANC attendance is also encouraged by providing targeted SBCC, combined with innovative community- and facility-level performance-based financing and high enrollment in community health insurance schemes (mutuelles). The MoH, with the support of partners, has worked to improve the quality of services for case management at health facilities through training and capacity building efforts at national and district levels.
A study looked at health care seeking for children below 5years of age in Rwanda in 2005 to 2010 and found that, “In both years,under-five children with Mutuelles were more likely to use medical care than uninsured children. Children in 2010 had a higher probability of using medical care … regardless of the children’s poverty or Mutuelles status.” The study provides an example of how pre-payment CBHI can not only increase universal health coverage but also address challenges of equity (Mejía-Guevara et al., 2015).
Below is a chart showing the fee structure in Rwanda (Tashobya, 2017). [The trainer should ask participants about fees for CBHIs or other national health insurance schemes in their countries if such exist and how participation in CHBI helps achieve UHC.]
| Fees in Rwanda’s community insurance scheme, Mutuelles | ||
| Ubudehe/Social Category | Annual Rwandan Francs per Household Member | Approximate US Dollars |
| 1 | 0 (Paid by government) | 0 |
| 2 | 2,000 | 2.25 |
| 3 | 3,000 | 3.35 |
| 4 | 4,000 | 7.85 |
Now The East African reports that, “With more than 90 per cent of Rwandans covered under the community-based health insurance scheme locally known as Mutuelle de Santé, Rwanda is one of the few developing countries in the world that have successfully achieved universal healthcare” (Kagire, 2018) This was achieved by addressing enrollment, quality of cane and transferring management of the scheme to the Rwanda Social Security Board (RSSB). Now more than ever, no one needs to die from malaria in Rwanda.
- Kagire, Edmund (2018). Rwanda Has Achieved Universal Healthcare. The East African. 15 December 2018. https://allafrica.com/stories/201812150128.html
- Mejía-Guevara I, Hill K, Subramanian SV, Lu C. (2015). Service availability and association between Mutuelles and medical care usage for under-five children in rural Rwanda: a statistical analysis with repeated cross-sectional data. BMJ Open. 2015 Sep 8;5(9):e008814. doi: 10.1136/bmjopen-2015-008814.
- Tashobya, Athan (2017). Mutuelle Month: Govt targets 100% subscription. The New Times. Published : April 03, 2017. https://www.newtimes.co.rw/section/read/210035
- USAID/President’s Malaria Initiative (2018) Rwanda Malaria Operational Plan FY19. https://www.pmi.gov/docs/default-source/default-document-library/malaria-operational-plans/fy19/fy-2019-rwanda-malaria-operational-plan.pdf?sfvrsn=3
Case Management &Monitoring &Mortality Bill Brieger | 04 Nov 2018
Malaria Death Audits: A tool to help improve severe malaria case management and prevent malaria related deaths in Mashona East, Zimbabwe
Anthony Chisada, Paul Matsvimbo, Munekayi Padingani, Tsitsi Siwela of Jhpiego,the USAID ZAPIM Project, Harare, Zimbabwe, and the Zimbabwe Ministry of Health and Child Welfare, Harare, Zimbabwe presented their experiences using death audits at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings follow.
 Nearly 50% of the Zimbabwean population is at risk for malaria. Total numbers of malaria related deaths have remained almost constant over the past 5 years. The National Malaria Control Program’s National Malaria Strategic Plan aims to reduce malaria-related deaths by 90% from 2015 levels (462 deaths) by 2020.
Nearly 50% of the Zimbabwean population is at risk for malaria. Total numbers of malaria related deaths have remained almost constant over the past 5 years. The National Malaria Control Program’s National Malaria Strategic Plan aims to reduce malaria-related deaths by 90% from 2015 levels (462 deaths) by 2020.
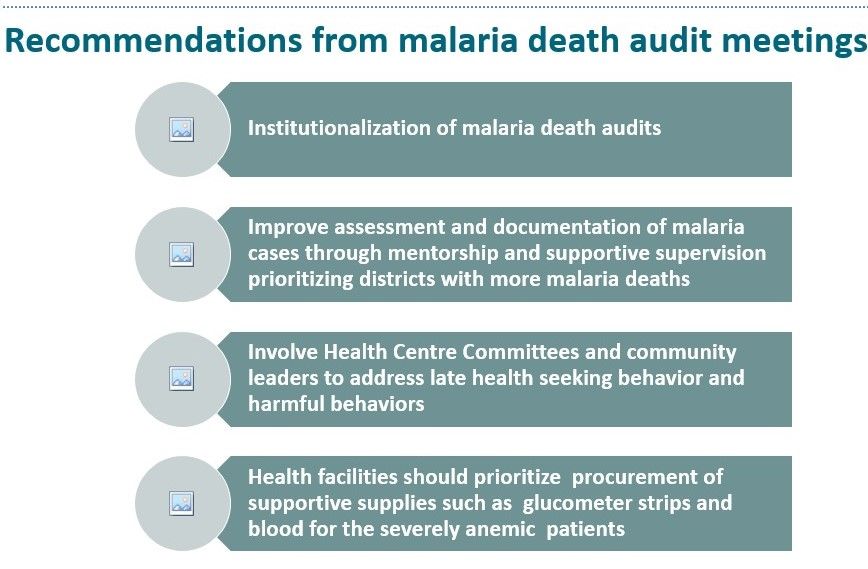
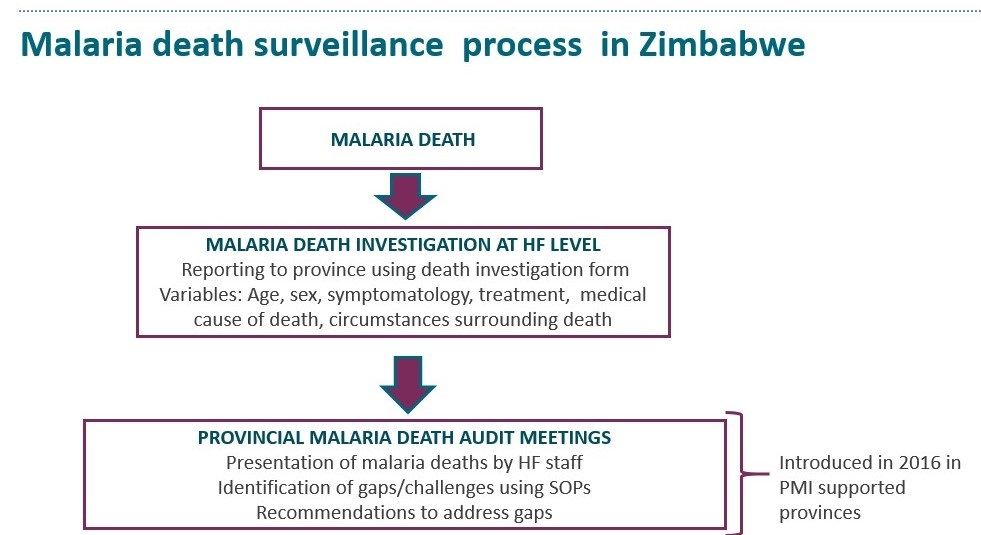 To improve severe malaria care and reduce mortality, NMCP documents and investigates all malaria deaths to ascertain the cause of the death and understand if and how it was avoidable. Malaria death audit meetings are held quarterly with health facility staff using a standard death investigation form and case management notes and form a learning platform to look at qualitative and quantitative data related to the deaths.
To improve severe malaria care and reduce mortality, NMCP documents and investigates all malaria deaths to ascertain the cause of the death and understand if and how it was avoidable. Malaria death audit meetings are held quarterly with health facility staff using a standard death investigation form and case management notes and form a learning platform to look at qualitative and quantitative data related to the deaths.
 The audits also examine the quality of care offered as per treatment guidelines and seek to identify ways to prevent future malaria deaths based on omissions and errors in presented cases.
The audits also examine the quality of care offered as per treatment guidelines and seek to identify ways to prevent future malaria deaths based on omissions and errors in presented cases.
This review examines the findings from death audit meetings facilitated by the  PMI-funded Zimbabwe Assistance Program in Malaria project in the Zimbabwean provinces of Mashonaland Central, Mashonaland East and Matabeleland North. Six death audit meetings were conducted over an 18-month period, resulting in a total of 80 deaths audited. The audited deaths were purposely sampled for the potential learning value they offered and to diversify lessons learned.
PMI-funded Zimbabwe Assistance Program in Malaria project in the Zimbabwean provinces of Mashonaland Central, Mashonaland East and Matabeleland North. Six death audit meetings were conducted over an 18-month period, resulting in a total of 80 deaths audited. The audited deaths were purposely sampled for the potential learning value they offered and to diversify lessons learned.
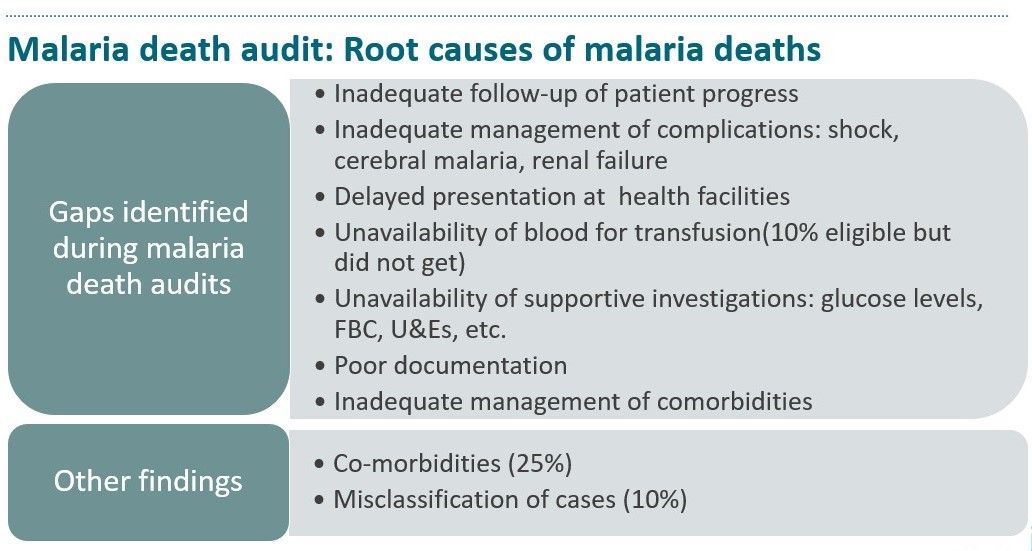
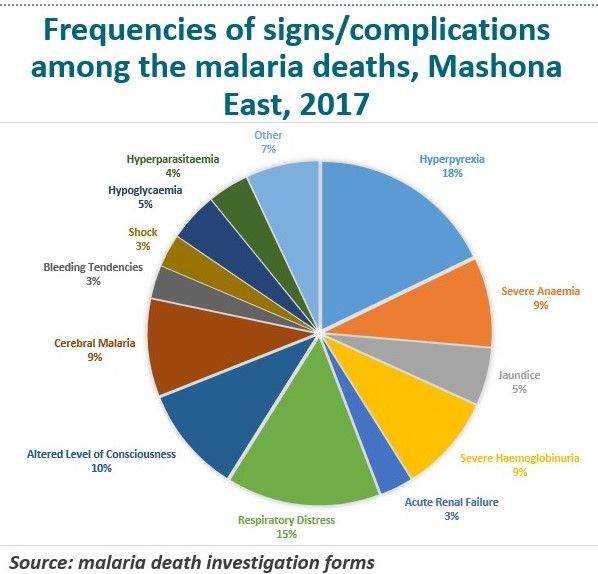 According to audit reports, the main contributing factors to malaria deaths included: delayed presentation by patients, lack of comprehensive assessment and documentation of cases, inadequate care for patients with reduced level of consciousness and shock, inadequate follow-up of patient progress, lack of supportive investigations, and lack of access to renal replacement therapy/dialysis and blood transfusion.
According to audit reports, the main contributing factors to malaria deaths included: delayed presentation by patients, lack of comprehensive assessment and documentation of cases, inadequate care for patients with reduced level of consciousness and shock, inadequate follow-up of patient progress, lack of supportive investigations, and lack of access to renal replacement therapy/dialysis and blood transfusion.
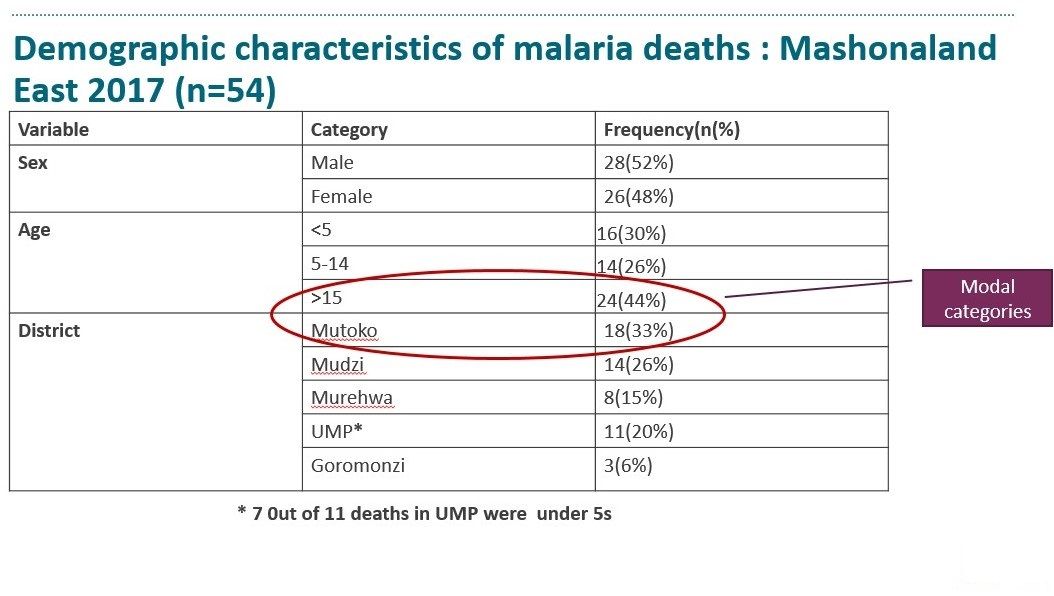
 Most deaths in age groups: under 5s(30%) and over 15(44%). Children are at risk of dying from malaria because of underdeveloped immunity, women taking children to gardens at night, delayed presentation since mothers are busy. Problem most pronounced in UMP. People over 15 years also at risk of dying: Suggestive of exposure as they indulge in outdoor activities without any protection from mosquito bites.
Most deaths in age groups: under 5s(30%) and over 15(44%). Children are at risk of dying from malaria because of underdeveloped immunity, women taking children to gardens at night, delayed presentation since mothers are busy. Problem most pronounced in UMP. People over 15 years also at risk of dying: Suggestive of exposure as they indulge in outdoor activities without any protection from mosquito bites.
 Death audits reapportion delays (3rd delay increased from 8% to 28%). First delay remains the major contributory factor- need for strengthening SBCC efforts. Malaria death audit meetings enhances the usefulness of the malaria death surveillance system and provides an opportunity for identification and discussion of health system challenges. Some challenges identified are rectifiable thus mitigating deaths. These enable holistic patient care: Identification and management of co-morbidities is critical. Findings contributed to justification of introduction malaria clinical mentorship for improving QoC.
Death audits reapportion delays (3rd delay increased from 8% to 28%). First delay remains the major contributory factor- need for strengthening SBCC efforts. Malaria death audit meetings enhances the usefulness of the malaria death surveillance system and provides an opportunity for identification and discussion of health system challenges. Some challenges identified are rectifiable thus mitigating deaths. These enable holistic patient care: Identification and management of co-morbidities is critical. Findings contributed to justification of introduction malaria clinical mentorship for improving QoC.
 The introduction of malaria death audit meetings has added an active, learning platform to complement the use of the malaria death investigation form and also served as a useful learning tool within Zimbabwe’s clinical mentorship program. Regular malaria death audit meetings are potentially useful in improving malaria care and reducing malaria related deaths.
The introduction of malaria death audit meetings has added an active, learning platform to complement the use of the malaria death investigation form and also served as a useful learning tool within Zimbabwe’s clinical mentorship program. Regular malaria death audit meetings are potentially useful in improving malaria care and reducing malaria related deaths.

Case Management &Children &Health Workers &IPTp &Malaria in Pregnancy &Quality of Services Bill Brieger | 04 Nov 2018
Improving Malaria through National Rollout of Malaria Service and Data Quality Improvement: A Case Study from Tanzania
Jasmine Chadewa, Chonge Kitojo, Goodluck Tesha, Naomi Kaspar, Lusekelo Njoge, Zahra Mkomwa, Dunstan Bishanga, George Greer, Abdallah Lusasi, and Sigsbert Mkude of the USAID Boresha Afya Project, the US President’s Malaria Initiative, the National Malaria Control Program, and the Community Development, Gender, Elderly and Children (Tanzanian Ministry of Health) shared how malaria data quality could be improved at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. Below are their findings.
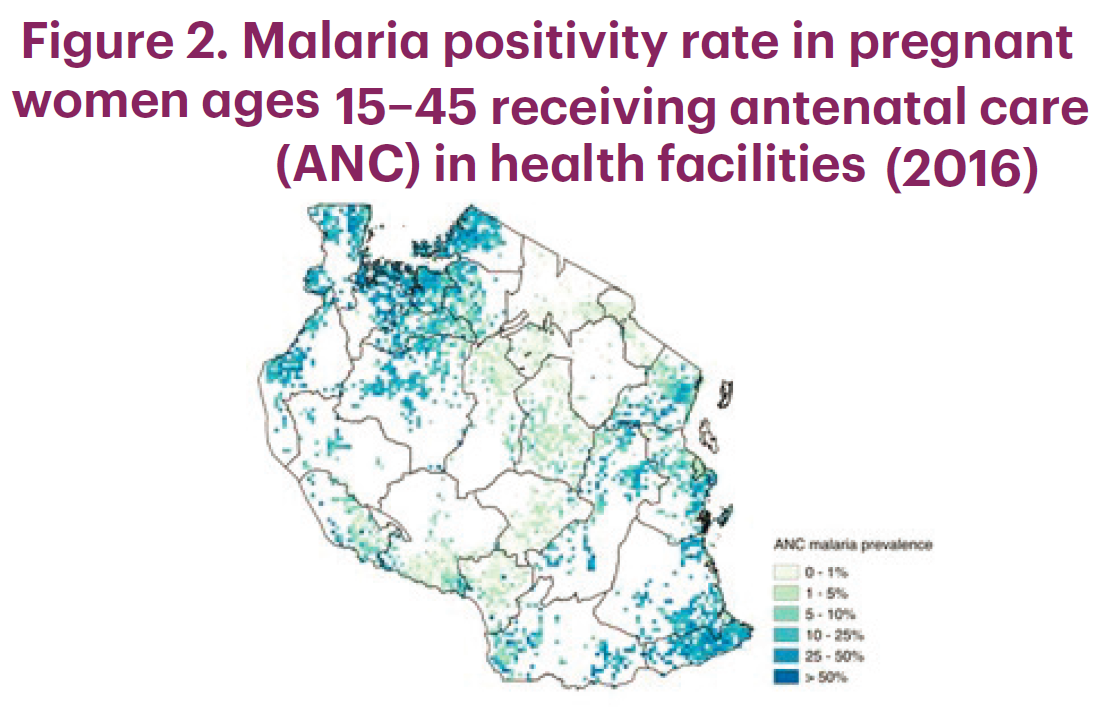
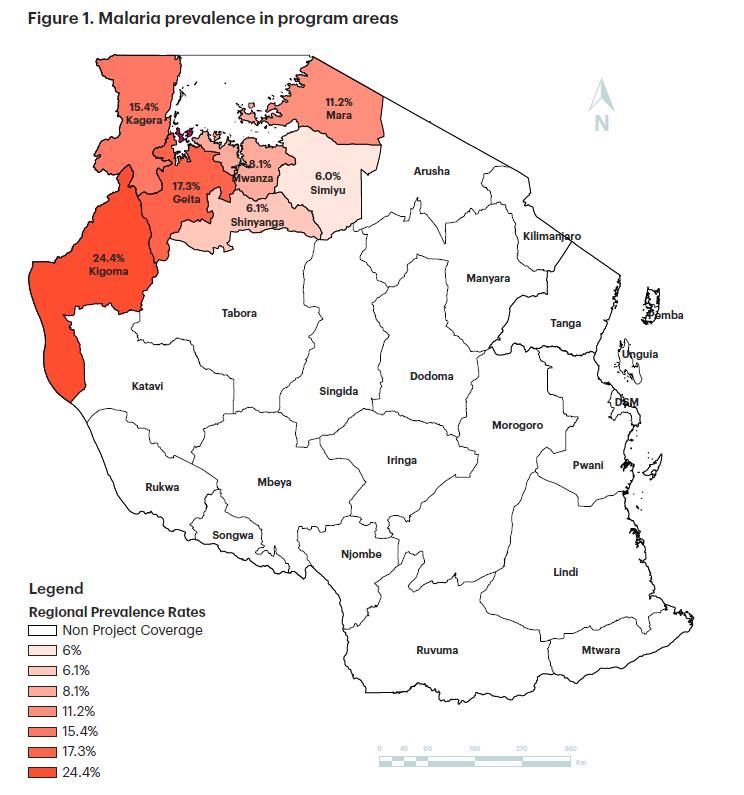 Tanzania has a high malaria burden (see Figure 1) and is facing an increased demand for health services. The Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) developed the Malaria Service and Data Quality Improvement (MSDQI) checklist to guide supportive supervision teams in evaluating the quality of malaria case management (MCM) services at facility level. MSDQI helps with the collection, monitoring, and evaluation of facility-based malaria performance indicators at all levels of service delivery that provide timely, accurate information and data for decision-making at district, regional, and national levels.
Tanzania has a high malaria burden (see Figure 1) and is facing an increased demand for health services. The Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) developed the Malaria Service and Data Quality Improvement (MSDQI) checklist to guide supportive supervision teams in evaluating the quality of malaria case management (MCM) services at facility level. MSDQI helps with the collection, monitoring, and evaluation of facility-based malaria performance indicators at all levels of service delivery that provide timely, accurate information and data for decision-making at district, regional, and national levels.
 USAID Boresha Afya conducted MSDQI assessments in 1,222 health facilities in the Lake and Western zones in outpatient departments (OPDs) and during antenatal care (ANC). The program disseminates malaria and ANC guidelines, tablets, job aids, and standard operating procedures. It also continues to facilitate supportive
USAID Boresha Afya conducted MSDQI assessments in 1,222 health facilities in the Lake and Western zones in outpatient departments (OPDs) and during antenatal care (ANC). The program disseminates malaria and ANC guidelines, tablets, job aids, and standard operating procedures. It also continues to facilitate supportive  supervision and mentorship through the MSDQI tool to build providers’ capacity in identified areas.
supervision and mentorship through the MSDQI tool to build providers’ capacity in identified areas.
Among the challenges reported, Supervisors need to be trained in more than one module to reduce cost. There is turnover of MSDQI supervisors. Cases that come back positive for diseases other than malaria are not investigated further. The use of Android smartphones sometimes  interfered with data collection and the reporting system. • Regions/districts depend on donor support to implement MSDQI activities.
interfered with data collection and the reporting system. • Regions/districts depend on donor support to implement MSDQI activities.
In conclusion, effective implementation of the MSDQI tool requires regions, districts, and facilities to be well informed and given clear instruction so they can form supportive supervision teams. This should be done by:
- Orienting teams on roles and responsibilities
- Training teams on relevant competencies, resource allocation, and tablet
use for data collection
The team learned that MCM improved in OPDs and during ANC as a result of the MSDQI assessment. Improved access to quality MCM (diagnosis) nationwide. Frequency of malaria testing increased during the first ANC contact. Testing increased from 87% in April–June 2017 to 96% April–June 2018, a 9% change (see Figure 3). Second doses of intermittent preventive treatment of malaria in pregnancy (IPTp2) coverage increased by 15% on average in Boresha Afya-supported regions between October 2016 and June 2018 (see Figure 4).
![]() This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of USAID Boresha Afya and do not necessarily reflect the views of USAID or the United States government.
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of USAID Boresha Afya and do not necessarily reflect the views of USAID or the United States government.
Case Management &CHW &Primary Health Care &Private Sector Bill Brieger | 04 Nov 2018
Experiences and Perceptions of Care Seeking for Febrile Illness among Caregivers and Health Providers in Eight Districts of Madagascar
 Andrianandraina Ralaivaomisa, Eliane Razafimandimby, Jean Pierre Rakotovao, Lalanirina Ravony Harintsoa, Sedera Aurélien Mioramalala, Rachel Favero, Katherine Wolf, Patricia Gomez, Jocelyn Razafindrakoto, and Laurent Kapesa of MCSP/Jhpiego (Johns Hopkins University Affiliate), the Madagascar Ministry of Public Health and USAID presented their findings about febrile illness care seeking in Madagascar at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. Details follow below.
Andrianandraina Ralaivaomisa, Eliane Razafimandimby, Jean Pierre Rakotovao, Lalanirina Ravony Harintsoa, Sedera Aurélien Mioramalala, Rachel Favero, Katherine Wolf, Patricia Gomez, Jocelyn Razafindrakoto, and Laurent Kapesa of MCSP/Jhpiego (Johns Hopkins University Affiliate), the Madagascar Ministry of Public Health and USAID presented their findings about febrile illness care seeking in Madagascar at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. Details follow below.
 Malaria Care and Treatment in Madagascar is hampered by low perception of malaria risk among caregivers. There is use of self-medication and a lack of health provider knowledge about malaria prevention and treatment in pregnant women. Low-quality care in primary health facilities is another concern (Source: WHO. 2015. Guidelines for the treatment of malaria, 3rd ed.).
Malaria Care and Treatment in Madagascar is hampered by low perception of malaria risk among caregivers. There is use of self-medication and a lack of health provider knowledge about malaria prevention and treatment in pregnant women. Low-quality care in primary health facilities is another concern (Source: WHO. 2015. Guidelines for the treatment of malaria, 3rd ed.).
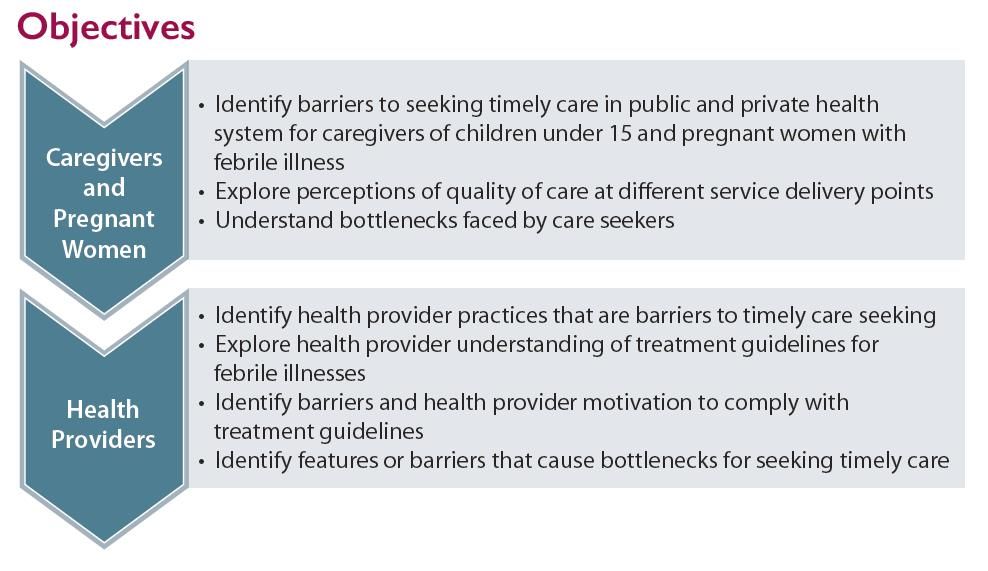
As seen in the attached, Study Objectives focus on Caregivers and Pregnant Women as well as Health Providers to determine barriers to effective care seeking of febrile illnesses.
 Both Qualitative and Quantitative Approaches were used. Among care seekers we conducted 16 focus group discussion sessions with 128 caregivers and pregnant women. There were also in-depth interviews with 32 pregnant women and 16 caregivers of children under 15. For Health Providers we conducted in-depth interview with 32 public and private health providers and administered 16 knowledge tests and case studies to health providers. We also reviewed logistic management information system records with 16 health
Both Qualitative and Quantitative Approaches were used. Among care seekers we conducted 16 focus group discussion sessions with 128 caregivers and pregnant women. There were also in-depth interviews with 32 pregnant women and 16 caregivers of children under 15. For Health Providers we conducted in-depth interview with 32 public and private health providers and administered 16 knowledge tests and case studies to health providers. We also reviewed logistic management information system records with 16 health
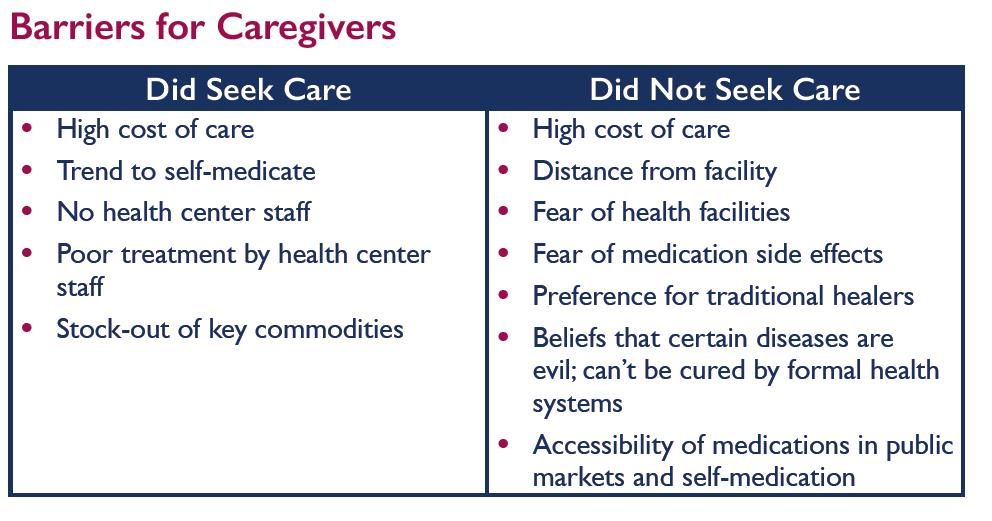
 Barriers for Caregivers are seen in the attached table. Barriers were faced by both care seekers and those who did not seek care, but were more common among non-seekers.
Barriers for Caregivers are seen in the attached table. Barriers were faced by both care seekers and those who did not seek care, but were more common among non-seekers.
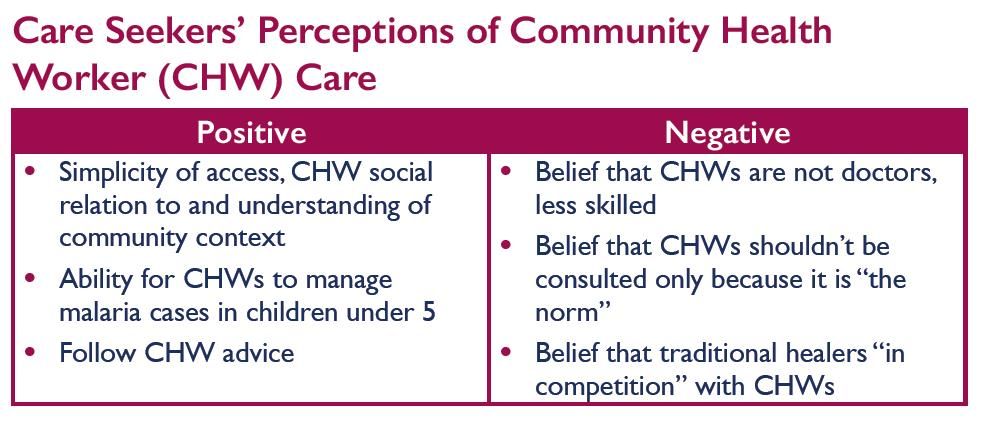
Three tables follow that show perceptions of public sector providers, private providers and community health workers. 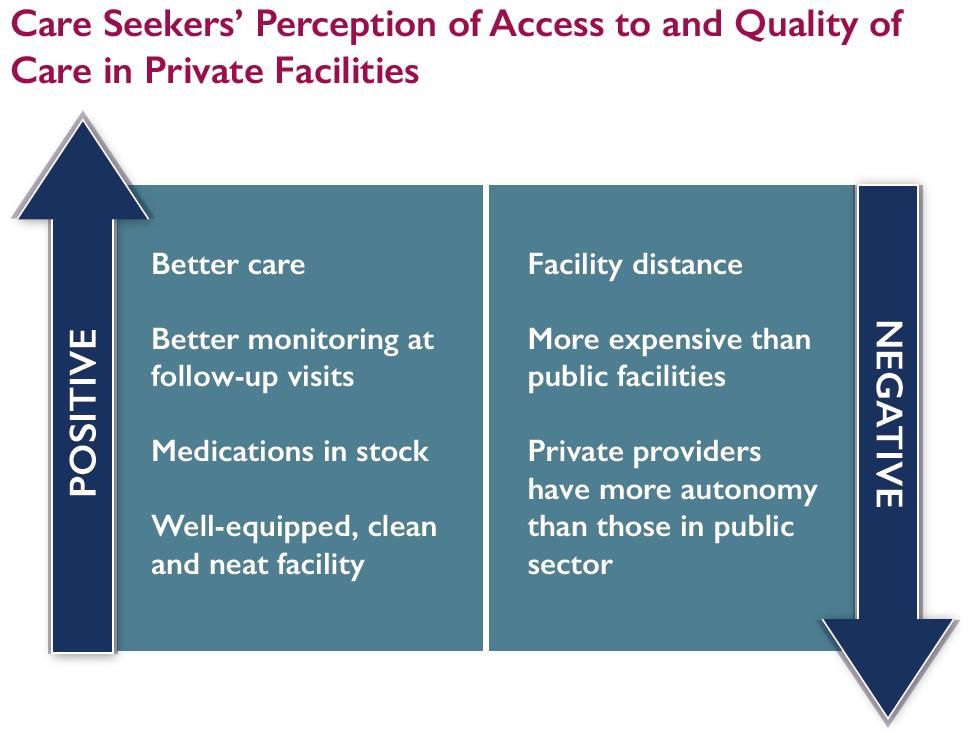 There were positive and negative perceptions of each group of providers.
There were positive and negative perceptions of each group of providers.
Health Provider Practices were also studied. They had low adherence to national guidelines for fever and malaria case management. Health workers reported high stock-outs rates of critical commodities (artemisinin-based combination therapy, artesunate). There was also lack of respectful care. Fortunately health provider diagnostic practices included 100% compliance with rapid diagnostic testing in cases of fever. They took temperatures and did physical exams appropriate to client’s symptoms and used microscopy at centers with local laboratory
 General Bottlenecks to Timely Care Seeking still existed. There was insecurity due to political situation in some regions. Inability to pay for care or medications was common. Alternative health behaviors included seeking care with traditional healers, and self-medication. There was fear by clients of going to health facilities and inaccurate perceptions of care provided by formal health care system
General Bottlenecks to Timely Care Seeking still existed. There was insecurity due to political situation in some regions. Inability to pay for care or medications was common. Alternative health behaviors included seeking care with traditional healers, and self-medication. There was fear by clients of going to health facilities and inaccurate perceptions of care provided by formal health care system
Recommendations start with the need to train providers and CHWs on national treatment guidelines for managing fever in all age groups and in pregnant women. Efforts are needed to strengthen onsite provider mentoring and supportive supervision and improve respectful care of clients, especially in public sector. Since care seeking still based on cultural norms, there is need to strengthen community/family education about febrile illness dangers and advantages of timely care seeking. Communities can also consider forming “mutuelle” community insurance schemes to relieve cost of care burden.
 This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Case Management &Elimination Bill Brieger | 03 Nov 2018
Multiple Approaches for Malaria Case Management in the Struggle to Reach Pre-Elimination of Malaria
![]() Goodluck Tesha, Zahra Mkomwa, Jasmine Chadewa, Lusekelo Njoge, Abdallah Lusasi, Dunstan Bishanga, Chonge Kitojo, Erik Reaves, George Greer of the USAID Boresha Afya Project, the Tanzanian Ministry of Health, and the US President’s Malaria Initiative shared experiences on the role of malaria case management in pre-elimination efforts at the 2018 Annual Meeting of the American Society of Tropical medicine and Hygiene. Their results are seen below.
Goodluck Tesha, Zahra Mkomwa, Jasmine Chadewa, Lusekelo Njoge, Abdallah Lusasi, Dunstan Bishanga, Chonge Kitojo, Erik Reaves, George Greer of the USAID Boresha Afya Project, the Tanzanian Ministry of Health, and the US President’s Malaria Initiative shared experiences on the role of malaria case management in pre-elimination efforts at the 2018 Annual Meeting of the American Society of Tropical medicine and Hygiene. Their results are seen below.
 The 5-year USAID Boresha Afya project works in 1,817 facilities in the seven regions of the Lake/Western Zone, where malaria prevalence is high. Since 2016, Boresha Afya has collaborated with the National Malaria Control Program to support the goal of reducing the malaria case fatality rate to below 1% by 2020 by:
The 5-year USAID Boresha Afya project works in 1,817 facilities in the seven regions of the Lake/Western Zone, where malaria prevalence is high. Since 2016, Boresha Afya has collaborated with the National Malaria Control Program to support the goal of reducing the malaria case fatality rate to below 1% by 2020 by:
- Promoting universal access to early diagnosis and prompt treatment
- Providing preventive therapies to vulnerable groups
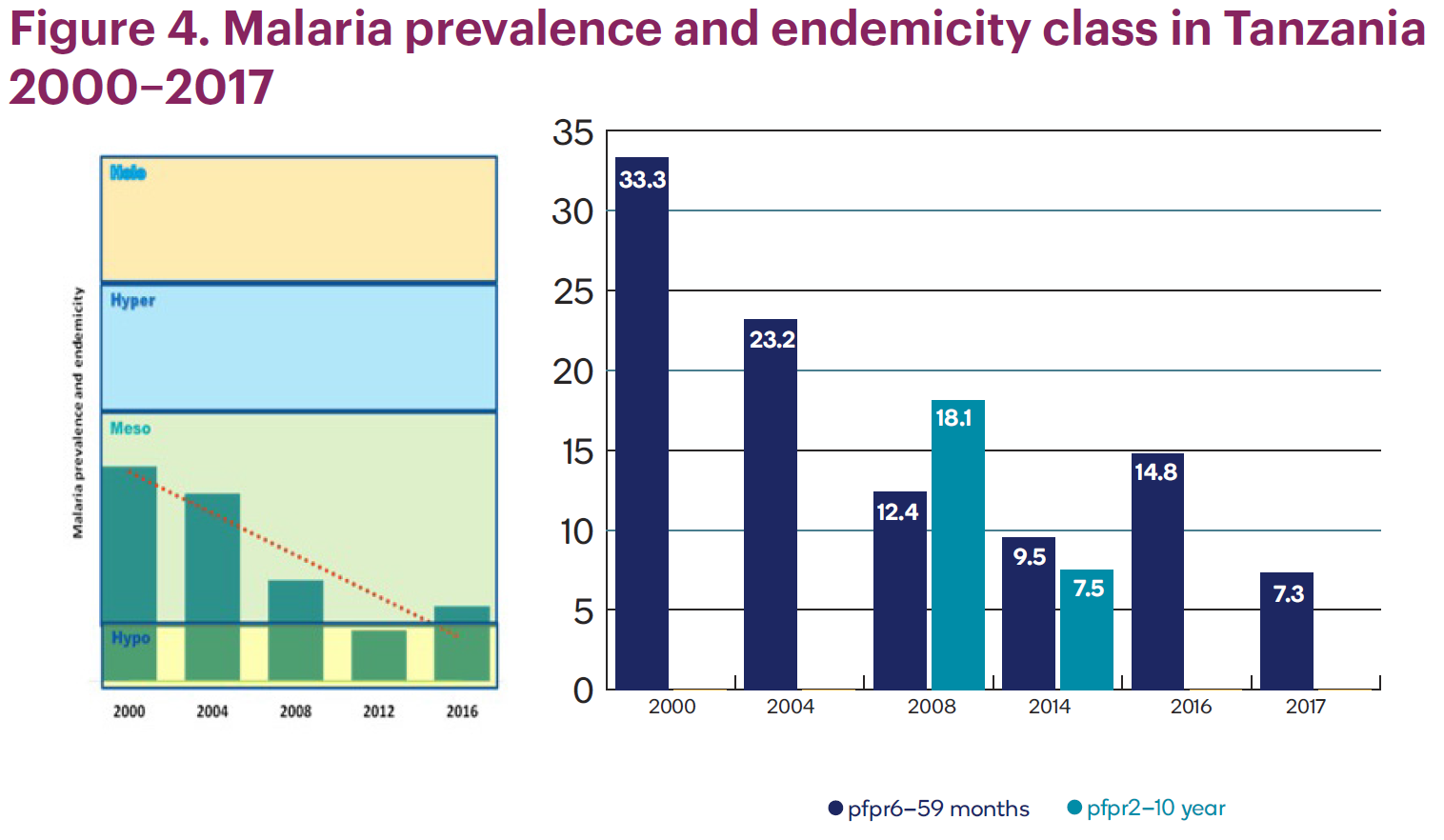
 In the last 15 years, malaria transmission has been cut in half, dropping from about 33% to less than 7.5%. Over the last three malaria indicator surveys, the number of regions with extremely low malaria prevalence (<1%) increased from one (2008) to seven (2016). The percentage of the population living in low-transmission areas (<10% prevalence) increased from 31% in 2000 to 49% in 2015.
In the last 15 years, malaria transmission has been cut in half, dropping from about 33% to less than 7.5%. Over the last three malaria indicator surveys, the number of regions with extremely low malaria prevalence (<1%) increased from one (2008) to seven (2016). The percentage of the population living in low-transmission areas (<10% prevalence) increased from 31% in 2000 to 49% in 2015.
 The intervention trained providers on quality testing using malaria rapid diagnostic tests (mRDTs). Training focused on conducting quality malaria microscopy examinations.
The intervention trained providers on quality testing using malaria rapid diagnostic tests (mRDTs). Training focused on conducting quality malaria microscopy examinations.
In addition, the team stratified malaria burden using GIS mapping and introduced malaria service and data quality improvement through a malaria dashboard. Community outreach programs were formed in remote areas.
 Due to mRDT availability, more suspected malaria cases are tested before malaria treatment is administered. Per national guidelines, all pregnant women should be tested for malaria on their first visit to the clinic. All project regions have met or exceeded the national 80% testing rate target (see Figure 5).
Due to mRDT availability, more suspected malaria cases are tested before malaria treatment is administered. Per national guidelines, all pregnant women should be tested for malaria on their first visit to the clinic. All project regions have met or exceeded the national 80% testing rate target (see Figure 5).
 In conclusion, to move toward malaria elimination, Boresha Afya will focus on ensuring more suspected cases are tested at facility level. Prompt treatment positive cases will then follow. Performing more community outreach should increase access to malaria case management in remote areas. Using GIS mapping will rapidly target services.
In conclusion, to move toward malaria elimination, Boresha Afya will focus on ensuring more suspected cases are tested at facility level. Prompt treatment positive cases will then follow. Performing more community outreach should increase access to malaria case management in remote areas. Using GIS mapping will rapidly target services.
 This poster is made possible by the support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of Jhpiego and do not necessarily reflect the views of USAID or the United States Government.
This poster is made possible by the support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of Jhpiego and do not necessarily reflect the views of USAID or the United States Government.
Case Management &Health Information &Quality of Services Bill Brieger | 02 Nov 2018
Using the collaborative quality improvement approach to increase adherence to the test, treat, and track malaria case management framework: Experiences from 10 health facilities in Uganda
Thomson Ngabirano, Espilidon Tumukurate, Innocent Atukunda, Emily Katarikawe, Jimmy Opigo, Martin Muhire, Emily Goodwin, Sam Gudoi, Kassahun Belay, Peter Thomas, James Tibenderana have been working with the following partners in Uganda to improve malaria  case management: Jhpiego, United States Agency for International Development’s (USAID) Malaria Action Program for Districts (MAPD) Project, Uganda National Malaria Control Program, Ministry of Health, University Research Co., the USAID ASSIST Project, Malaria Consortium, US President’s Malaria Initiative, and the US Centers for Disease Control and Prevention, Uganda. Their work, seen below, was presented at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene.
case management: Jhpiego, United States Agency for International Development’s (USAID) Malaria Action Program for Districts (MAPD) Project, Uganda National Malaria Control Program, Ministry of Health, University Research Co., the USAID ASSIST Project, Malaria Consortium, US President’s Malaria Initiative, and the US Centers for Disease Control and Prevention, Uganda. Their work, seen below, was presented at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Malaria has a 19 percent parasite prevalence in Uganda and is a leading cause of morbidity and mortality in Uganda and in 2014 was responsible for:
- 30-50 percent of outpatient visits
- 15-20 percent of hospital admissions
- 20 percent of inpatient deaths.[1]
 In an effort to reduce its malaria burden, in 2016 the Ministry of Health in Uganda incorporated a number of World Health Organization recommendations into its National Malaria Policy Guidelines. The main elements in these guidelines implemented by health workers were:
In an effort to reduce its malaria burden, in 2016 the Ministry of Health in Uganda incorporated a number of World Health Organization recommendations into its National Malaria Policy Guidelines. The main elements in these guidelines implemented by health workers were:
- testing all suspected malaria cases with malaria rapid diagnostic tests (mRDT) or microscopy before treatment
- using artemisinin-based combination therapy (ACT) to treat only positive malaria cases
- providing at least three doses of intermittent preventive treatment in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP).
However, a number of challenges for malaria service delivery were encountered during
implementation, including incomplete, inaccurate, and inconsistent malaria records and reports; health workers not adhering to the malaria test, treat, and track policy; and malaria causing high caseloads at outpatient and inpatient service points.
To overcome these issues, and in particular to improve adherence to the malaria test, treat and track policy and strengthen the quality of data collection and recording, USAID’s Malaria Action Program for Districts (MAPD) implemented a collaborative quality improvement approach (CQI).
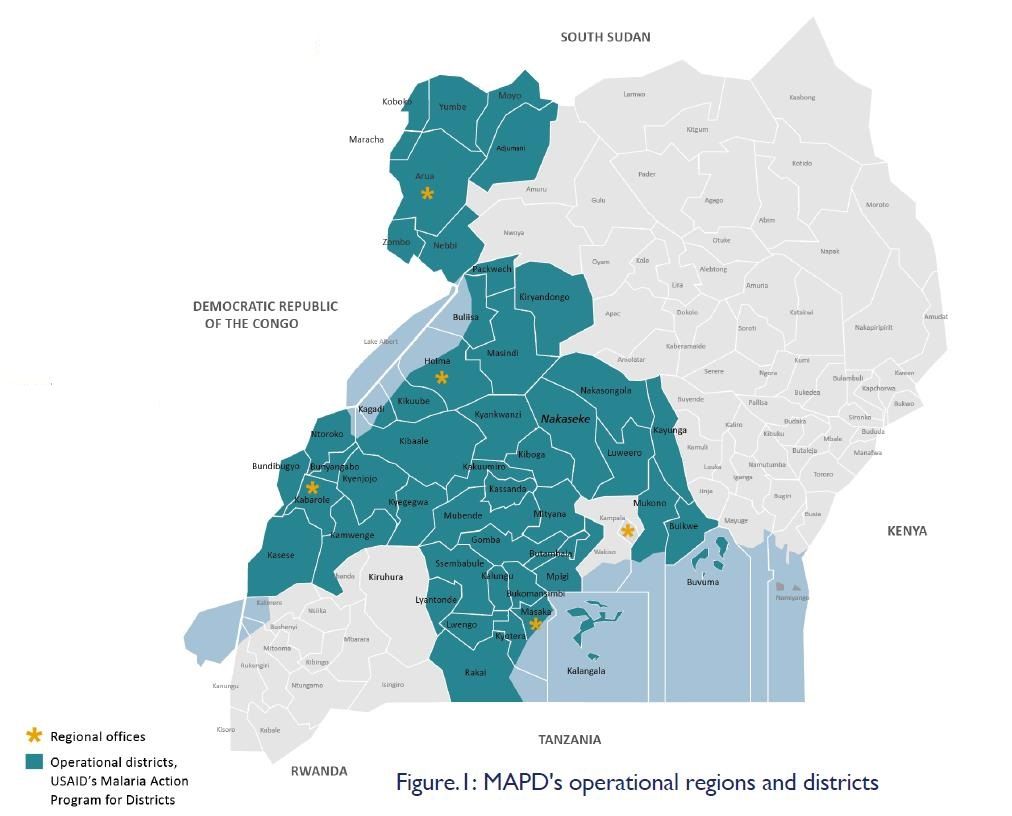
 A CQI approach was introduced to MAPD in November 2017 and implemented using both qualitative and quantitative methods. These included reviewing malaria indicators on the District Health Information System, identifying 10 high-volume facilities across MAPD’s five operational regions with poor malaria indicators (see Figure 1), holding entry meetings with the district health teams, conducting collaborative data reviews and problem analysis with health facility staff, and presenting the results of data reviews to health facility staff to identify inaccurate reporting and non-compliance with the test, treat and track policy. Interventions also included working with health facility staff to identify potential solutions and interventions, implementing agreed interventions and reviewing indicators, monitoring progress using documentation journals, holding learning sessions led by a CQI coach, agreeing on new actions.
A CQI approach was introduced to MAPD in November 2017 and implemented using both qualitative and quantitative methods. These included reviewing malaria indicators on the District Health Information System, identifying 10 high-volume facilities across MAPD’s five operational regions with poor malaria indicators (see Figure 1), holding entry meetings with the district health teams, conducting collaborative data reviews and problem analysis with health facility staff, and presenting the results of data reviews to health facility staff to identify inaccurate reporting and non-compliance with the test, treat and track policy. Interventions also included working with health facility staff to identify potential solutions and interventions, implementing agreed interventions and reviewing indicators, monitoring progress using documentation journals, holding learning sessions led by a CQI coach, agreeing on new actions.
Malaria data indicators reviewed include accuracy and completeness of cases in lab register and OPD, number of fever cases tested for malaria using mRDT or microscopy, number of malaria-negative cases treated with ACTs, number of malaria-positive cases treated with ACTs, and number of pregnant women receiving three or more doses of IPTp-SP.
In a sample of 300 cases from a June 2018 lab register, taken eight months after the CQI approach was introduced, all 300 (100 percent) were recorded in the respective OPD register. This represents a 108 percent increase from when an equivalent sample was first reviewed in November 2017. In a sample of 300 patients that were treated using ACTs in June 2018, all patients were tested for malaria using mRDTs or microscopy and no patients were treated that had tested negative. This represents an 89 percent decrease from November 2017 when 27 (nine percent) malaria-negative cases were incorrectly treated using ACTs.
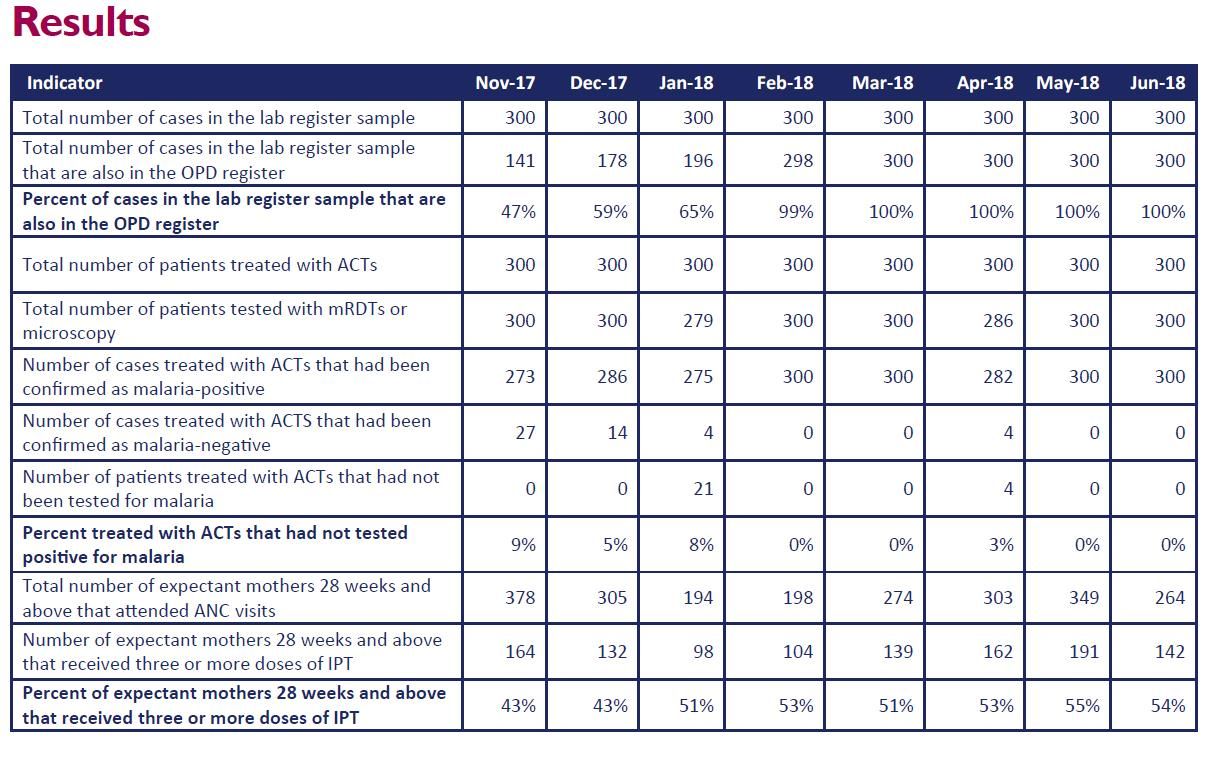
Of the total 264 expectant mothers (who were 28 weeks pregnant and above) that attended ANC visits in July 2018, 142 (54 percent) received three or more doses of IPTp-SP. This is a marked increase on the 43 percent of pregnant women who received three or more doses in November 2017.
Feedback from discussions with health workers in facility meetings and regional learning sessions showed that health teams now accept that there is a need for accurate and complete data and understand the importance of adhering to the National Malaria Policy Guidelines. In conclusion … The CQI approach was found to promote accurate data collection and improve adherence to the malaria test, treat, and track policy among health workers at 10 health facilities in five regions of Uganda.
[1] Reference: Uganda Bureau of Statistics (UBOS) and ICF International. Uganda Malaria Indicator Survey 2014-15. Kampala, Uganda and Rockville, Maryland, USA: UBOS and ICF International; 2015. Available at https://dhsprogram.com/pubs/pdf/mis21/mis21.pdf
MAPD is a project (running from 2016-2021), funded by the US President’s Malaria Initiative, USAID, UK aid, and the government of Uganda, which aims to improve the health status of the Ugandan population by reducing malaria-related morbidity and mortality among children and pregnant women. This poster was made possible by the support of the American and British People through the United States Agency for International Development and UK aid from the UK government. The contents of this poster are the sole responsibility of USAID Malaria Action Program for Districts and do not necessarily reflect the views of USAID or the United States Government and do not necessarily reflect the UK government’s official policies. For more information, please contact; 1. Dr Thomson Ngabirano, Malaria in Pregnancy Specialist Thomson.Ngabirano@Jhpiego.org 2. Dr Sam Siduda Gudoi, Chief of Party s.gudoi@malariaconsortium.org
Case Management &Health Workers &Planning &Severe Malaria &Training Bill Brieger | 01 Nov 2018
Malaria Response Plan in Times of High Transmission: An Approach to Improving the Quality of Hospital Malaria Management
Ousmane Badolo, Stanislas Nebie, Youssouf Sawadogo, Thierry Ouedraogo, Moumouni Bonkoungou, Mathurin Dodo, Danielle Burke, William Brieger, and Gladys Tetteh of Jhpiego and the Improving Malaria Care Project (USAID) in Burkina Faso presented a poster on helping hospitals develop a malaria response plan. Their findings are shared below.
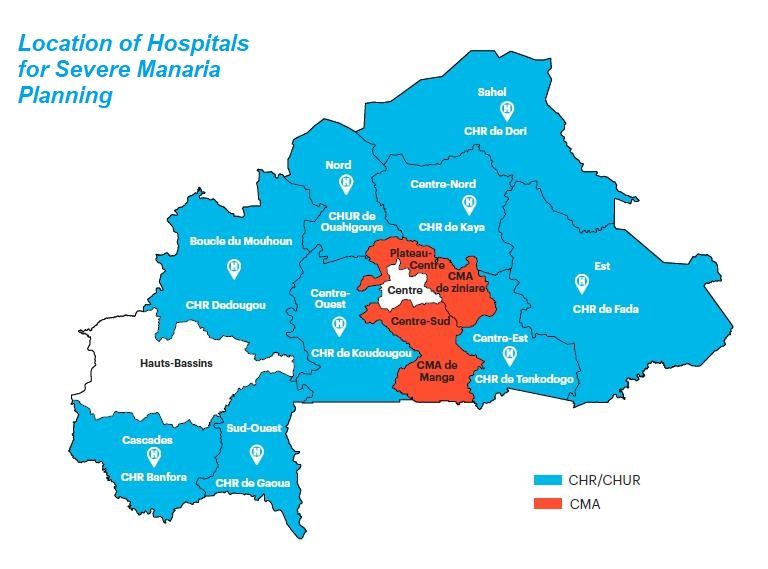 In Burkina Faso Malaria cases peak from June-September (rainy season), exceeding hospital capacity and causing high number of deaths, especially in children under 5 years of age. The Improving Malaria Care Project, funded by USAID/President’s Malaria Initiative, provided support to National Malaria Control Program to develop and implement malaria preparedness and response plans in all 11 regional hospitals
In Burkina Faso Malaria cases peak from June-September (rainy season), exceeding hospital capacity and causing high number of deaths, especially in children under 5 years of age. The Improving Malaria Care Project, funded by USAID/President’s Malaria Initiative, provided support to National Malaria Control Program to develop and implement malaria preparedness and response plans in all 11 regional hospitals
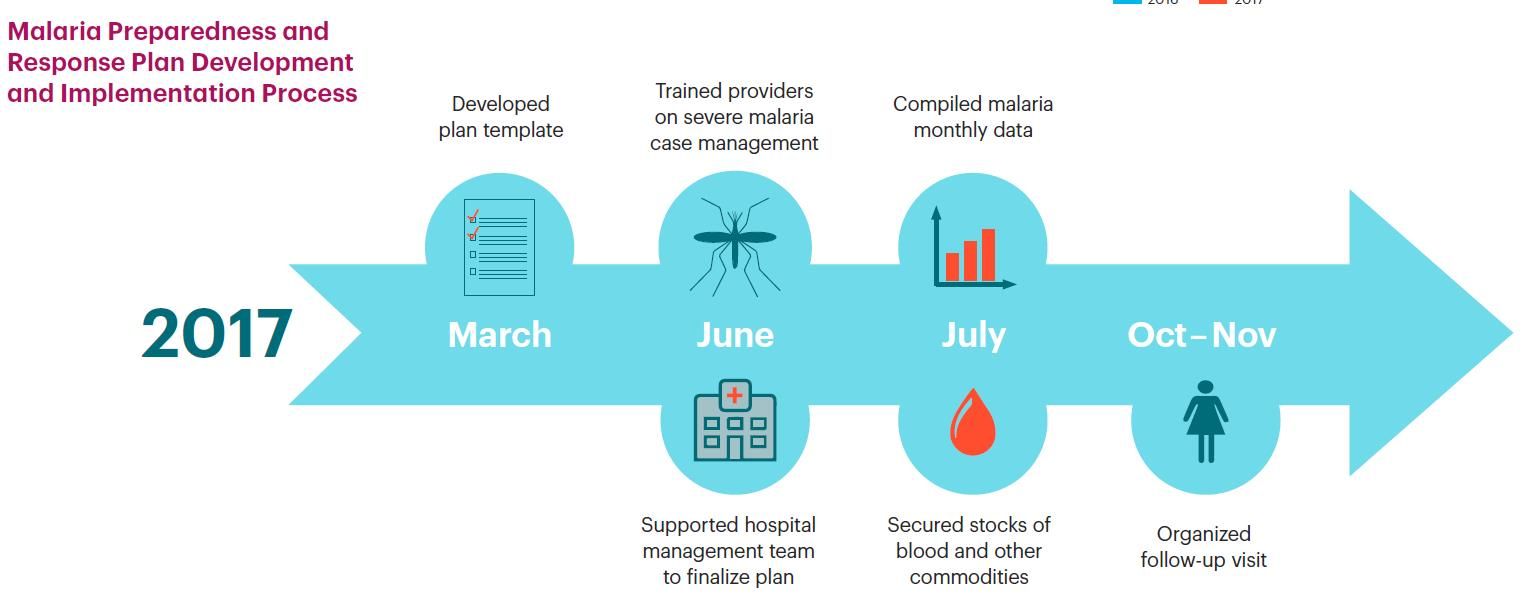 The Objectives of this effort aimed to describe development and implementation of malaria preparedness and response plan. From this the project planned to share lessons learned and challenges Malaria Preparedness and Response Plan Development and Implementation Process is seen in the attached chart.
The Objectives of this effort aimed to describe development and implementation of malaria preparedness and response plan. From this the project planned to share lessons learned and challenges Malaria Preparedness and Response Plan Development and Implementation Process is seen in the attached chart.
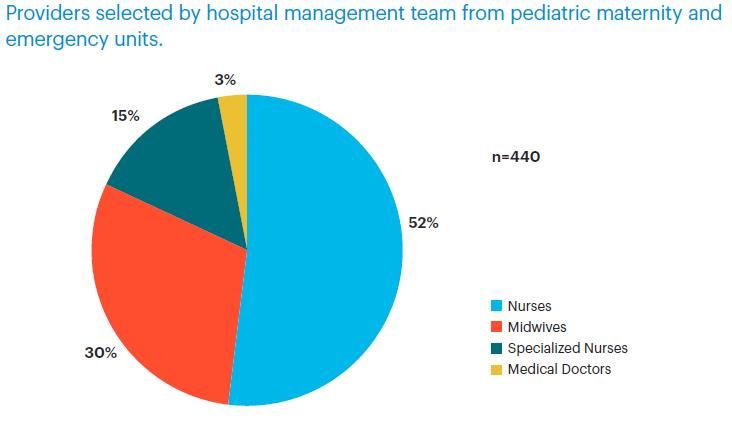 In preparation of hospital staff for planning, the training reached Nurses and midwives were largest groups of trained providers at 52% and 30%, respectively. Providers were selected by hospital management team from pediatric maternity and emergency units.
In preparation of hospital staff for planning, the training reached Nurses and midwives were largest groups of trained providers at 52% and 30%, respectively. Providers were selected by hospital management team from pediatric maternity and emergency units.
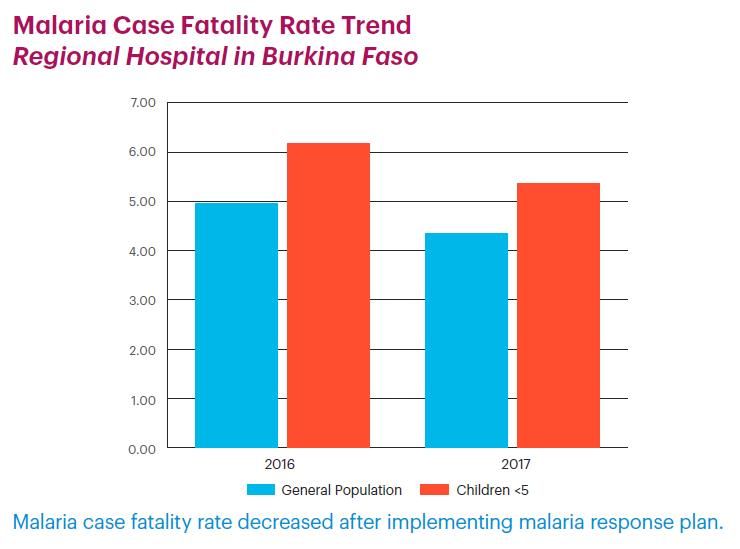
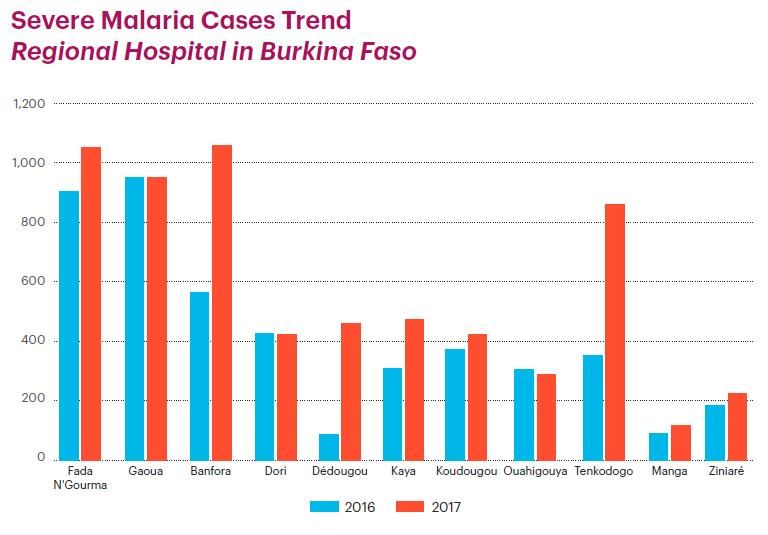 Severe Malaria Cases Trend Regional Hospital in Burkina Faso is seen in the attached graph. In a second graph, Malaria Case Fatality Rate Trend at Regional Hospitals in Burkina Faso is shown. Even though there were more cases of severe malaria in 2017, Malaria case fatality rate decreased after implementing malaria response plan.
Severe Malaria Cases Trend Regional Hospital in Burkina Faso is seen in the attached graph. In a second graph, Malaria Case Fatality Rate Trend at Regional Hospitals in Burkina Faso is shown. Even though there were more cases of severe malaria in 2017, Malaria case fatality rate decreased after implementing malaria response plan.
 Challenges faced by the hospitals included Lack of funding for response plan activities, which were not included in the routine hospital work plan. Also there was a Lack of beds in some hospital rooms, especially in pediatric unit. Timing of clients coming to hospital posed a challenge as many do not come early and sometimes come when only complications start.
Challenges faced by the hospitals included Lack of funding for response plan activities, which were not included in the routine hospital work plan. Also there was a Lack of beds in some hospital rooms, especially in pediatric unit. Timing of clients coming to hospital posed a challenge as many do not come early and sometimes come when only complications start.
Lessons learned from the intervention include the fact that On-the-job training is opportunity to improve providers’ skills. Response plans must consider that providers’ refreshment, and securing blood and other commodities may improve severe malaria case management. Monthly data collection and analysis may highlight progress in malaria planning through case management and orient decision-making. Follow-up visits strengthened provider engagement on severe malaria case Management
 In Conclusion, Response plans may provide a way to reduce malaria mortality. Each hospital should consider incorporating response plan into its annual work plan
In Conclusion, Response plans may provide a way to reduce malaria mortality. Each hospital should consider incorporating response plan into its annual work plan
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID) under Cooperative Agreement No. AID-624-A-13-00010 and the President’s Malaria Initiative (PMI). The contents are the responsibility of the authors and do not necessarily reflect the views of USAID, PMI or the United States Government.
Case Management &CHW &Training Bill Brieger | 31 Oct 2018
Improving Adherence to National Malaria Treatment Guidelines through a Low-Dose, High-Frequency Approach Targeting Village Malaria Workers in Selected Townships in Myanmar
 Ni Ni Aye, May Aung Lin, Saw Lwin, Khin Than Win, Kyan Khaing, Nu Nu Khin, Kyaw Myint Tun who are colleagues from Jhpiego, PMI Defeat Malaria Project, University Research Co., Myanmar Nurses and Midwives Association; and the USAID/US President’s Malaria Initiative, Myanmar
Ni Ni Aye, May Aung Lin, Saw Lwin, Khin Than Win, Kyan Khaing, Nu Nu Khin, Kyaw Myint Tun who are colleagues from Jhpiego, PMI Defeat Malaria Project, University Research Co., Myanmar Nurses and Midwives Association; and the USAID/US President’s Malaria Initiative, Myanmar  presented their experiences training village malaria workers on national malaria treatment guidelines at the 2018 Annual Meeting of the American Society of Tropical Medicine an Hygiene. Below are their findings.
presented their experiences training village malaria workers on national malaria treatment guidelines at the 2018 Annual Meeting of the American Society of Tropical Medicine an Hygiene. Below are their findings.
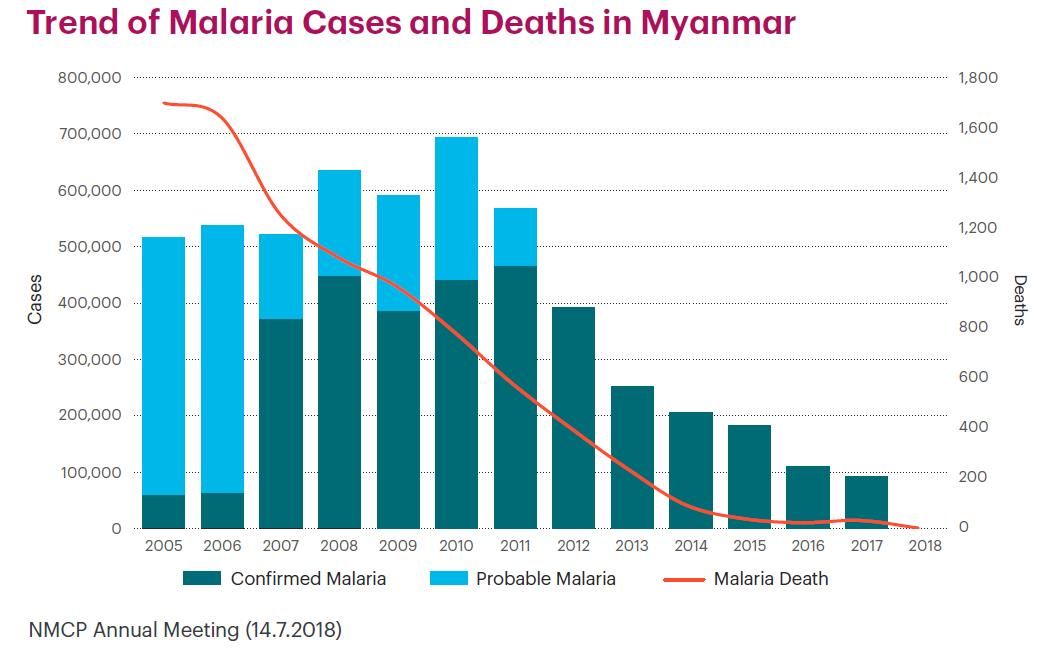
The Trend of Malaria Cases and Deaths in Myanmar has been steadily decreasing. PMI Defeat Malaria Project (October 2016–September 2021) wants to ensure that this trend continues.
 Project goals include reduce malaria burden, control artemisinin-resistant malaria in target area, and eliminate malaria in Myanmar. Specific Objectives are:
Project goals include reduce malaria burden, control artemisinin-resistant malaria in target area, and eliminate malaria in Myanmar. Specific Objectives are:
- Achieve universal coverage of at-risk populations
- Strengthen malaria surveillance system
- Enhance provider technical capacity
- Promote community and public and private-sector involvement in malaria control and elimination
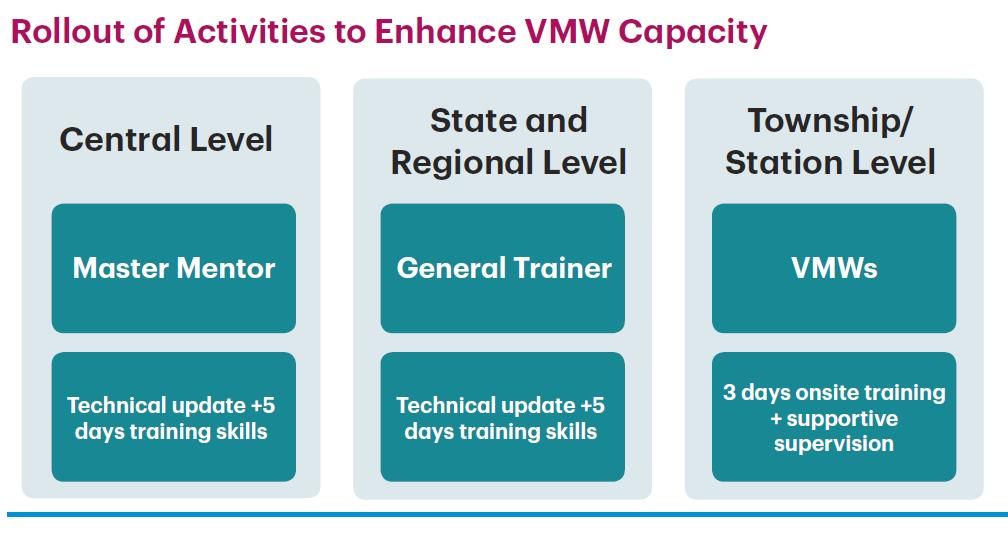 Capacity Development Strategy for Village Malaria Workers (VMWs) focused on Two townships with low adherence to National Malaria Treatment Guidelines (NTGs): Palaw Township with 38 Village Malaria Workers (VMWs) and Gwa Township with 39 VMWs. The project used a Competency-based low-dose, high-frequency (LDHF) training approach. There were Three sessions, one day/month during June, July, and August 2017.
Capacity Development Strategy for Village Malaria Workers (VMWs) focused on Two townships with low adherence to National Malaria Treatment Guidelines (NTGs): Palaw Township with 38 Village Malaria Workers (VMWs) and Gwa Township with 39 VMWs. The project used a Competency-based low-dose, high-frequency (LDHF) training approach. There were Three sessions, one day/month during June, July, and August 2017.
 Post-training follow-up used a Clinical audit result review during supportive supervision and monitoring visits. Data quality assessment and verification was performed by field teams and monthly reports examined.
Post-training follow-up used a Clinical audit result review during supportive supervision and monitoring visits. Data quality assessment and verification was performed by field teams and monthly reports examined.
The project also Conducted refresher training using LDHF approach for at least two doses followed by on-the-job training and regular supervision and monitoring. They Formulated culturally appropriate materials for areas like Palaw Township where different languages are spoken. A Job Aid on Benefits of Adherence to Antimalarial Drug was developed.
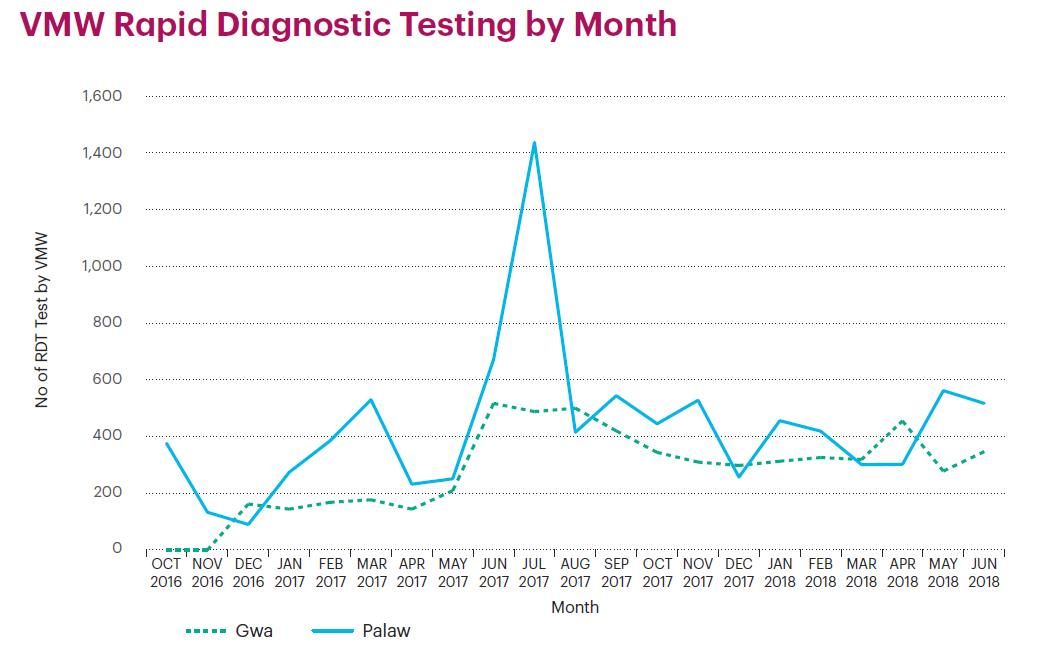 VMW Rapid Diagnostic Testing was observed by Month. There was an Improvement in VMW Knowledge Assessment Scores with a positive Post-training Assessment Knowledge of Malaria.
VMW Rapid Diagnostic Testing was observed by Month. There was an Improvement in VMW Knowledge Assessment Scores with a positive Post-training Assessment Knowledge of Malaria.
Post-training Assessment for RDT Competency also took place. 85-90% of 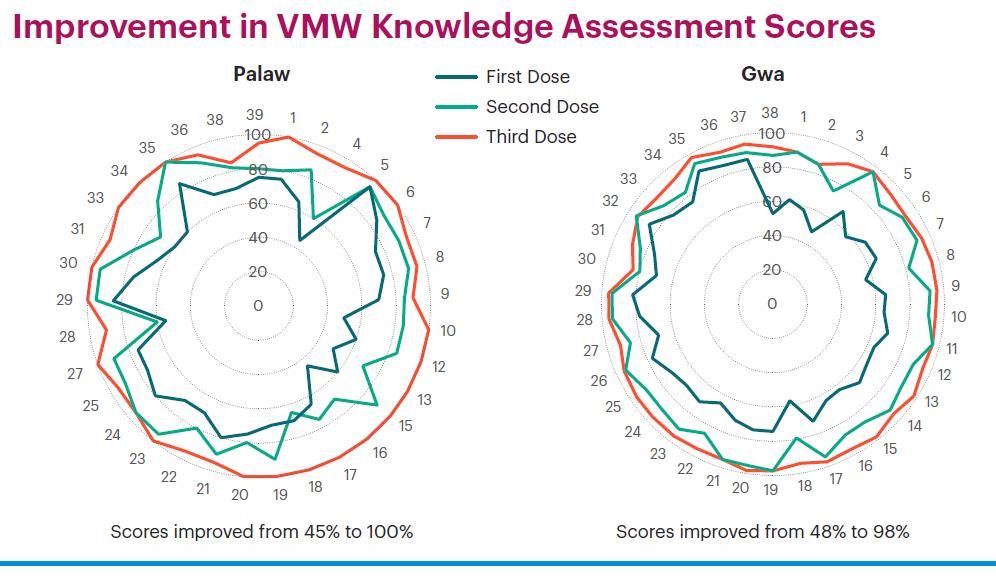 VMWs Told clients about blood testing and provided emotional support. 70-80% of VMWs Conducted RDT testing according to standards. 95-98% of VMWs Performed hand hygiene before and after rapid diagnostic test. 80-90% of VMWs Disposed used lancet immediately into safety box after use. 85-90% of VMWs Gave health education. Finally 80-90% Disposed of contaminated items appropriately and recorded test in malaria register, and 80% Used job aids/manual and provided correct treatment according to National Training Guidelines (NTGs).
VMWs Told clients about blood testing and provided emotional support. 70-80% of VMWs Conducted RDT testing according to standards. 95-98% of VMWs Performed hand hygiene before and after rapid diagnostic test. 80-90% of VMWs Disposed used lancet immediately into safety box after use. 85-90% of VMWs Gave health education. Finally 80-90% Disposed of contaminated items appropriately and recorded test in malaria register, and 80% Used job aids/manual and provided correct treatment according to National Training Guidelines (NTGs).
 In Conclusion, Improvement was seen in adherence to NTGs assessed as percent of uncomplicated malaria cases that received correct antimalarial treatment. VMWs Adhered to NTGs. In Gwa thus Increased from 72% to 100% and remained high. In Palaw this Stayed at 91% – 92% after training period. Therefore, the LDHF approach was appropriate for
In Conclusion, Improvement was seen in adherence to NTGs assessed as percent of uncomplicated malaria cases that received correct antimalarial treatment. VMWs Adhered to NTGs. In Gwa thus Increased from 72% to 100% and remained high. In Palaw this Stayed at 91% – 92% after training period. Therefore, the LDHF approach was appropriate for 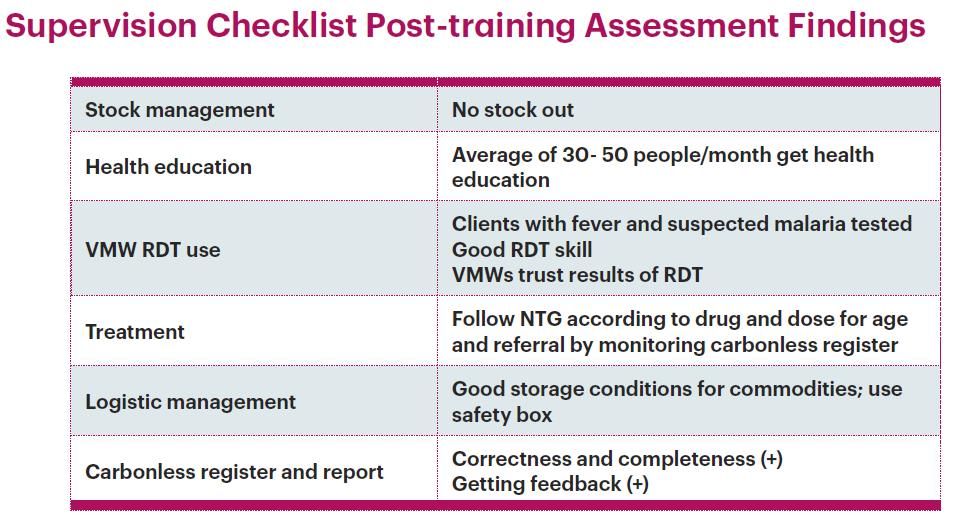 VMW capacity-building on protocol adherence in Gwa Township where there was no language barrier.
VMW capacity-building on protocol adherence in Gwa Township where there was no language barrier.
Next Steps include Conducting refresher training using LDHF approach for at least two doses followed by on-the-job training and regular supervision and monitoring. The project will Formulate culturally appropriate materials for areas like Palaw Township where different languages are spoken.