Community &Private Sector &Treatment Bill Brieger | 03 Nov 2014
Ghana at ASTMH: Mapping out of antimalarial drugs on stock at the market in a rural districts of Ghana
The first Poster Session of the American Society of Tropical Medicine and Hygiene (Monday noon) will feature a study on availability of malaria medicines in rural Ghana. “Mapping out of antimalarial drugs on stock at the market in a rural districts of Ghana” was developed by Alexander A. Nartey, Evelyn K. Ansah, Patricia Akweongo, Gloria A. Nartey, Mary A. Pomaa, Doris Sarpong, Clement Narh, and Margaret Gyapong of the Dodowa Health Research Centre.
American Society of Tropical Medicine and Hygiene (Monday noon) will feature a study on availability of malaria medicines in rural Ghana. “Mapping out of antimalarial drugs on stock at the market in a rural districts of Ghana” was developed by Alexander A. Nartey, Evelyn K. Ansah, Patricia Akweongo, Gloria A. Nartey, Mary A. Pomaa, Doris Sarpong, Clement Narh, and Margaret Gyapong of the Dodowa Health Research Centre.
 Antimalarial drugs are a very important component of any policy for effective reduction of morbidity and mortality related to the malaria disease. The availability of efficacious and high quality antimalarials and their correct use can mitigate the risk of morbidity and mortality among the people of sub-Saharan Africa who have the highest risk of contracting and dying
Antimalarial drugs are a very important component of any policy for effective reduction of morbidity and mortality related to the malaria disease. The availability of efficacious and high quality antimalarials and their correct use can mitigate the risk of morbidity and mortality among the people of sub-Saharan Africa who have the highest risk of contracting and dying
from malaria.
Chemical (medicine) shops are major source of care for most developing countries where anti-malarial drugs can be purchase at the counter. The paper seeks to identify the different kinds of anti-malarial drugs on the market for malaria treatment in a rural district in Ghana.
 A structured questionnaire was used during two seasons (peak and low malaria transmission seasons) to collect information on anti-malarial drugs from all 58 chemical shops within the Dangme West district now (Shai Osudoku and Ningo Prampram districts). Pictures of the anti-malarial drugs were taken,
A structured questionnaire was used during two seasons (peak and low malaria transmission seasons) to collect information on anti-malarial drugs from all 58 chemical shops within the Dangme West district now (Shai Osudoku and Ningo Prampram districts). Pictures of the anti-malarial drugs were taken,
The active ingredients, and also the source of the drugs documented. GIS locations of the shops were also recorded to ascertain the proximity of the shops to households in the communities. Majority (72.0%) of the chemical and pharmacy shop owners are males. Only 7.0% of the shops are pharmacy while the remainder is licensed chemical shops.
 The total numbers of antimalarial drugs counted were forty nine (49). Among the stock, 4.2% were quinine, 31.9% of them were monotherapies such as artemether, Amodiaquine, Artesunate etc. Altogether, 59.4% of the artemisinin combination therapies (ACTs) were artemether + Lumefantrine, 25.0% were Artesunate + Amodiaquine.
The total numbers of antimalarial drugs counted were forty nine (49). Among the stock, 4.2% were quinine, 31.9% of them were monotherapies such as artemether, Amodiaquine, Artesunate etc. Altogether, 59.4% of the artemisinin combination therapies (ACTs) were artemether + Lumefantrine, 25.0% were Artesunate + Amodiaquine.
Other antimalarials observed were 9.4% Sulfadoxine + Pyrimethamine and 3.1% of of Artesunate + Sulfamethoxypyrazine + Pyrimethamine. About 47% of the anti-malarial drugs were pediatric formulations.
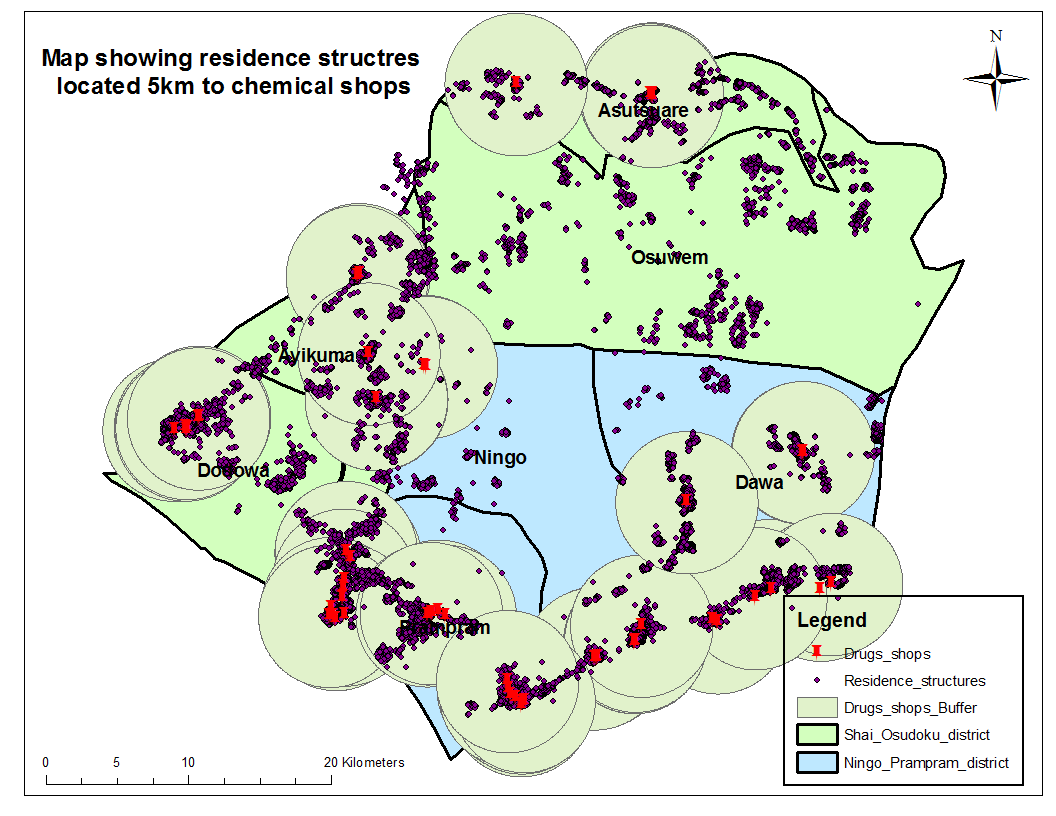 GIS mapping shows that majority of the households are within a periphery of 5km to a chemical shop.
GIS mapping shows that majority of the households are within a periphery of 5km to a chemical shop.
The national antimalarial drug policy recommends the use of ACTs for malaria treatment however; all sorts of anti-malarial drugs which are not ACTs are in stock at the chemical shops in Ghana. Chemical shops are closer to households and play a very important role in the treatment of malaria hence there is the need to train chemical sellers to stock and administer the recommended antimalarials.
Health Systems &Human Resources &IPTp &Malaria in Pregnancy &Monitoring Bill Brieger | 03 Nov 2014
Jhpiego at ASTMH: Performance Quality Improvement for IPTp in Kenya
Monday afternoon (3 October 2014) at the American Society for Tropical Medicine and Hygiene Annual Meeting in New Orleans, Jhpiego and USAID/PMI are sponsoring a panel on “Integrating and Innovating: Strengthening Care for Mothers and Children with Infectious Diseases.” If you are at the meeting please attend to learn more about our Malaria activities in Kenya.
 One of the panel presentations is “Performance Quality Improvement Lending to Corrected Documented Outcomes for Intermittent Preventive Treatment in Kenya,” by Jhpiego staff Muthoni Kariuki, Augustine Ngindu Isaac Malonza, and Sanyu Kigondu, who are working with USAID’s Maternal & Child Health Integrated Project (MCHIP).
One of the panel presentations is “Performance Quality Improvement Lending to Corrected Documented Outcomes for Intermittent Preventive Treatment in Kenya,” by Jhpiego staff Muthoni Kariuki, Augustine Ngindu Isaac Malonza, and Sanyu Kigondu, who are working with USAID’s Maternal & Child Health Integrated Project (MCHIP).
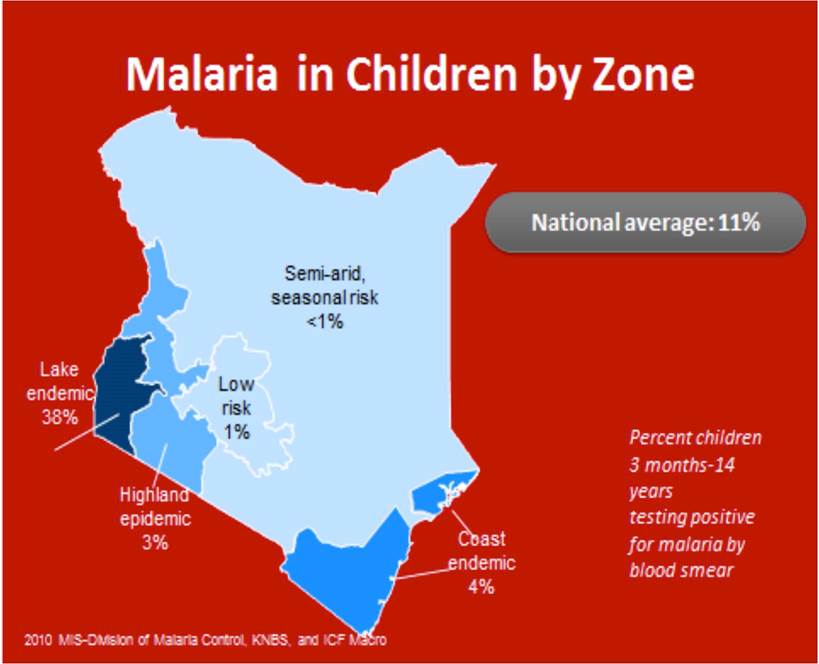
According to Malaria policy in Kenya all pregnant women in malaria endemic areas receive free intermittent preventive treatment with SP have access to free malaria diagnosis and treatment when presenting with fever have access to LLINs (National Malaria Strategy (NMS) 2009–2017).
By 2013 80% of people living in malaria risk areas should be using appropriate malaria preventive interventions. Intermittent Preventive Treatment of malaria in pregnancy using Sulfadoxine Pyrimethamine (IPTp-SP) intervention is recommended for use in malaria endemic region.
 MCHIP broadly implemented Capacity Development and service delivery and improvement interventions that also had impact on the delivery of malaria in pregnancy services through collaboration with the Ministry of Health divisions/units at national level: (malaria, reproductive health, community health).
MCHIP broadly implemented Capacity Development and service delivery and improvement interventions that also had impact on the delivery of malaria in pregnancy services through collaboration with the Ministry of Health divisions/units at national level: (malaria, reproductive health, community health).
At county level scale up provision of IPTp at facility level took place in 14 malaria endemic counties. This included 8 counties in the lake endemic region including Bondo sub-county (the MCHIP model sub-county) and 6 in the coastal endemic region.
Quality Improvement through Performance Quality Improvement (PQI) process was instituted to enhance service delivery. The MCHIP era in Bondo Strengthened ANC Services using the following:
- Development of MIP Standards-Based Management and Recognition (SBM-R) standards
- Orientation of facility in-charges, supervisors and service providers on the standards
- Monitoring of IPTp uptake using DHIS2 data
- Feedback to facility in-charges and supervisors on DHIS2 findings
- Collection of ANC data from ANC registers (2011-2013)
- Feedback to facility in-charges and supervisors on ANC data
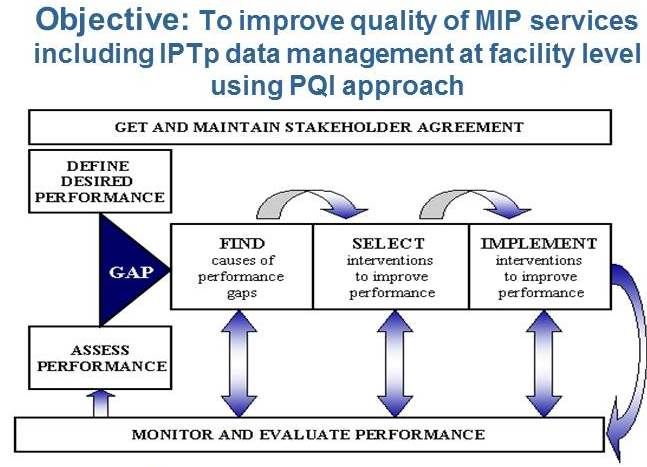
Quality improvement in the malaria in pregnancy component was undertaken with the objective to improve quality of MIP services including IPTp data management at facility level using PQI approach. An Example of a MIP SBM-R standard is seen below.
 In-service training focused on orientation of facility in-charges on PQI who then continued orientation at Facility Level. Overall we oriented 1200 facility in-charges and 100 supervisors on the standards. Facility in-charges cascaded orientation to 2,441 service providers.
In-service training focused on orientation of facility in-charges on PQI who then continued orientation at Facility Level. Overall we oriented 1200 facility in-charges and 100 supervisors on the standards. Facility in-charges cascaded orientation to 2,441 service providers.
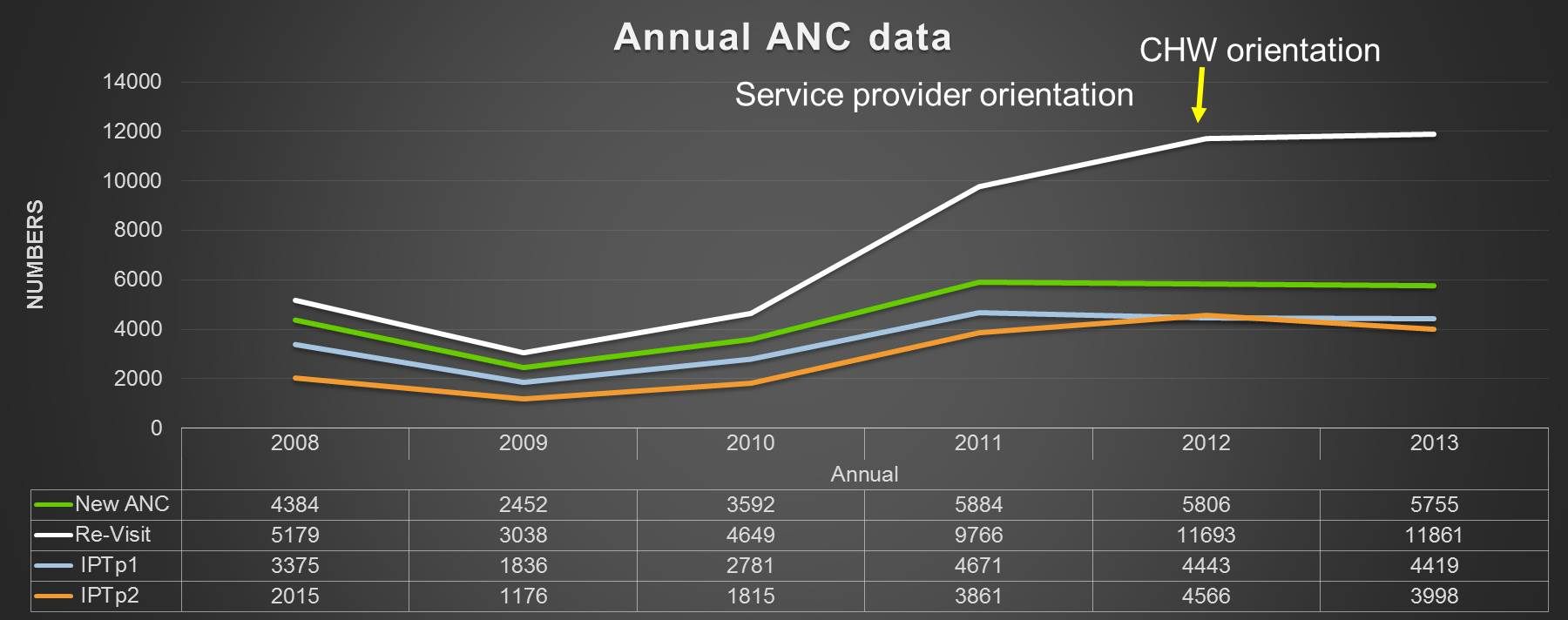 We then analysed ANC data from DHIS (2011-2013) indicated proportion of pregnant women receiving IPTp2 was higher than IPTp1 (IPTp2+ doses reported as IPTp2 dose). We helped improve reporting by service providers not oriented on use of the ANC register in order to reduce data errors.
We then analysed ANC data from DHIS (2011-2013) indicated proportion of pregnant women receiving IPTp2 was higher than IPTp1 (IPTp2+ doses reported as IPTp2 dose). We helped improve reporting by service providers not oriented on use of the ANC register in order to reduce data errors.
In conclusion, PQI is a best practice in provision of MIP services. Standardization of knowledge among service providers is essential in provision of quality MIP services. Development of facility in-charges as mentors in the facility to ensure continued orientation of new service providers.
Use of appropriate monitoring tools is necessary to assist in assessment of quality of services provided including data management. Feedback to service providers is one of the performance rewards and encourages participation in knowledge acquisition
Health Systems &Human Resources &Integration &Malaria in Pregnancy Bill Brieger | 02 Nov 2014
Improved Malaria Services in Malawi: Jhpiego and USAID at ASTMH
 Monday afternoon (3 October 2014) at the American Society for Tropical Medicine and Hygiene Annual Meeting in New Orleans, Jhpiego and USAID/PMI are sponsoring a panel on “Integrating and Innovating: Strengthening Care for Mothers and Children with Infectious Diseases.” If you are at the meeting please attend to learn more about our Malaria activities in Malawi.
Monday afternoon (3 October 2014) at the American Society for Tropical Medicine and Hygiene Annual Meeting in New Orleans, Jhpiego and USAID/PMI are sponsoring a panel on “Integrating and Innovating: Strengthening Care for Mothers and Children with Infectious Diseases.” If you are at the meeting please attend to learn more about our Malaria activities in Malawi.
One of the panel presentations is “Improving Malaria Outcomes in Malawi: Focusing on Integration of Services at all Levels” presented by John Munthali, Senior Technical Advisor, Jhpiego/Malawi. John works with Support for Service Delivering Integration-Services (SSDI-S), a USAID bilateral program (2011-2016) with Partnerships in 15 Districts involving the Ministry of Health, Jhpiego, Save the Children International, Care Malawi and Plan International.
 SSDI-Services focuses on Malawi’s Essential Health Package (EHP) Focal Areas with particular emphasis on Maternal Health, Newborn and Child Health, Family Planning and Reproductive Health, HIV/AIDS and TB, Nutrition and Malaria. Aspects of the Malaria Component include Intermittent Preventive Treatment and Insecticide Treated Bed Nets
SSDI-Services focuses on Malawi’s Essential Health Package (EHP) Focal Areas with particular emphasis on Maternal Health, Newborn and Child Health, Family Planning and Reproductive Health, HIV/AIDS and TB, Nutrition and Malaria. Aspects of the Malaria Component include Intermittent Preventive Treatment and Insecticide Treated Bed Nets
SSDI-S is based on Promotion of the continuum of care from household to hospital. Health Facility Approaches address Improved Technical Capacity of Health Workers, Functional Health Facility, and Data-informed Decision Making. Community Approaches involve Improved Technical Capacity of CHWs, Functional Village Clinics, and Community Mobilization. Integration is a major concern such that there are no missed opportunities of EHP services at all levels.
Positive Trends since have been seen since Inception. Malaria in Pregnancy interventions supported the National Malaria Control program to review the Malaria in Pregnancy guidelines and training manuals to adopt the new WHO policy recommendations. 74 Trainers were trained in all 15 districts. MNCH services were established in selected districts. 344 HSAs were trained. 70 community-based Core Groups oriented on MNCH. SSDI supported ongoing MNCH activities through review meetings and distribution of reporting forms.
 As a result of these integrated high impact interventions there has been a remarkable increase in the uptake of IPTp 2 (16% in June 2012 to 64% in Sept. 2013) by pregnant women in the SSDI-services focus districts. Central to this increase is the integration of services at the facility level where malaria has been highly integrated into maternal, newborn and child health. The project has also seen IPTp 1 uptake maintained at above 91% in all the 15 districts
As a result of these integrated high impact interventions there has been a remarkable increase in the uptake of IPTp 2 (16% in June 2012 to 64% in Sept. 2013) by pregnant women in the SSDI-services focus districts. Central to this increase is the integration of services at the facility level where malaria has been highly integrated into maternal, newborn and child health. The project has also seen IPTp 1 uptake maintained at above 91% in all the 15 districts
Malaria Care capacity building has resulted in improved iCCM services delivered by Health Surveillance Assistants (HSAs) at village clinics. iCCM is serving as the foundation for community-based treatment of malaria by HSAs while at facility level IMCI provides an integrated approach to manage childhood illnesses including malaria.
In conclusion, it is feasible to integrate MNCH programs at all levels using SBCC and Systems Strengthening. Having an integrated project looking at the whole spectrum of health services (system strengthening, service delivery and behavior change) can help improve programming & service delivery.
Diagnosis Bill Brieger | 02 Nov 2014
Fyodor UMT Researchers at ASTMH
Recently we shared the news that Fyodor Biotechnologies’ new Urine Malaria Test (UMT) has been approved by Nigeria’s food and drug agency. The research team from the University of Lagos and Fyodor will be at the American Society of Tropical Medicine and Hygiene Annual Meeting.
The poster abstract is outlined below, but please visit the actual poster on Tuesday at #882 Poster Session B starting at noon, to learn more from the researchers and discuss the implications for the future of malaria case management.
———–>
Effective case management of malaria requires prompt diagnosis and treatment within 24 hours. Despite current policy guidelines that mandate confirmed parasitological diagnosis before treatment, access to diagnostic testing remains low in sub-Saharan Africa.
Today, malaria diagnosis is only by blood-tests (microscopy and rapid diagnostic tests, RDTs), which are invasive, multistep and therefore relatively complex to perform, require technical expertise, and not available in most public and private sector healthcare settings where more than 65% of the population seek care.
 Here, we report the results of a multicenter pivotal clinical trial of Fyodor Urine Malaria Test (UMT) – a simple (one-step, no blood, no reagents, no equipment) dipstick test that detects Plasmodium falciparum parasite proteins shed in the urine of febrile malaria patients. A total of 1,893 participants (?2 years) with fever (axillary temperature ?37.5°C) or history of fever in the last 48 hours were enrolled at 6 primary healthcare centers in rural and suburban communities in Lagos State, Nigeria, over a 7-month period that covered both rainy and dry seasons.
Here, we report the results of a multicenter pivotal clinical trial of Fyodor Urine Malaria Test (UMT) – a simple (one-step, no blood, no reagents, no equipment) dipstick test that detects Plasmodium falciparum parasite proteins shed in the urine of febrile malaria patients. A total of 1,893 participants (?2 years) with fever (axillary temperature ?37.5°C) or history of fever in the last 48 hours were enrolled at 6 primary healthcare centers in rural and suburban communities in Lagos State, Nigeria, over a 7-month period that covered both rainy and dry seasons.
Matched patient urine and fingerprick blood sample were tested using the UMT, Binax NOW (Inverness) (HRP-2/pLDH) test, and microscopy. A total of 358 participants (18.9%) had confirmed malaria by microscopy; Fyodor UMT, 450 (23.8%); Binax NOW (pLDH), 386 (20.4%) and Binax NOW RDT (HRP-2), 731 (38.6%).
Statistical data analyses to determine test performance characteristics are ongoing and will be made available within a month. The UMT has the potential of expanding access to malaria diagnosis especially in settings where blood test is not possible.
Authors: Wellington A. Oyibo, Nnenna Ezeigwe, Godwin Ntadom, William Brieger, Wendy O’Meara, Anne Derrick, Bao Lige, Oladosu Oladipo, Eddy C. Agbo
Health Systems &Malaria in Pregnancy Bill Brieger | 01 Nov 2014
Jhpiego Malaria Team at the American Society of Tropical Medicine & Hygiene Conference
Jhpiego’s Malaria Team is co-hosting a symposium on Malaria in Pregnancy and presenting several posters at the upcoming ASTMH 2014 annual meeting in New Orleans, 2-6 November. Below is an outline of these events for those who may be in attendance. Jhpiego also will have a booth in the Exhibition area – please visit it.
Symposium: Integrating and Innovating: Strengthening Care for Mothers and Children with Infectious Diseases, 1:45 – 3:30 p.m., Marriott – Mardi Gras Ballroom D (Third Floor): Co-Faciliators: Elaine Roman, Jhpiego | Erin Eckert, USAID/ PMI
- Improving Malaria Outcomes in Malawi: Focusing on Integration of Services at all Levels, John Munthali, Jhpiego, Malawi
- Performance Quality Improvement Lending to Corrected Documented Outcomes for Intermittent Preventive Treatment in Kenya, Muthoni Kariuki, Jhpiego, Kenya
- The provision of HIV and IPTp Services in Antenatal Care in Malawi: Views of Health Care Providers from a Qualitative Study, P. Stanley Yoder
- Mothers and Mycobacteria: Implications of the Intersection of TB, Pregnancy, and Maternal and Newborn Health, Charlotte Colvin
- Wrap-up: The Growing Role of Infectious Disease in Maternal Mortality Reduction: How to Attain the Post-MDG targets, Allisyn Moran
![]()
Poster Sessions:
Poster Session A: Monday 12:00 – 1:45 p.m., Marriott Grand Ballroom (Third Floor)
- Quality Inspired Project – A Key to Achieving Results with Malaria Interventions, Grace Qorro, Jhpiego Tanzania
- Prevention of Malaria in Pregnancy: Community Health Volunteers (CHVs) Promote Community-based Activities to Increase Uptake of Intermittent Preventive Treatment of Malaria in Pregnancy (IPTp) in Kenya, Augustine Ngindu, Jhpiego Kenya
Poster Session B: Tuesday 12:00 – 1:45 p.m., Marriott Grand Ballroom (Third Floor)
- Improving Maternal and Neonatal Health: Complementary Role of the Private Sector Increasing Uptake of Intermittent Preventive Treatment for Malaria in Pregnancy in Kenya, Augustine Ngindu, Jhpiego, Kenya
Poster Session C: Wednesday 12:00 – 1:45 p.m., Marriott Grand Ballroom (Third Floor)
- Expanding Health Ministry Capacity to Deliver Malaria and Other Health Commodities at the Community Level in Nigeria, Bright Orji, Jhpiego, Nigeria