ITNs &Universal Coverage &Vector Control &Zero Malaria Bill Brieger | 25 Apr 2019 07:37 am
Zero Malaria Starts with Universal Coverage: Part 1 Nets
WHO says, “Malaria elimination and universal health coverage go hand in hand,” at a special event during the 72st World Health Assembly. To achieve zero malaria, the goal of involving everyone from the policy maker to the community member must have a focus on achieving universal health coverage (UHC) of all malaria interventions ranging from insecticide treated bednets (ITNs) to appropriate provision of malaria diagnostics and medicines. Many of the studies to date have focused on ITNs, which include long-lasting insecticide treated nets (LLINs), but nationwide monitoring through the Demographic and Health Surveys (DHS), the Malaria Indicator Surveys (MIS) and the Multi-Indicator Cluster Surveys (MICS).
UNICEF’s website provides a data repository that includes the most recent DHS, MIS and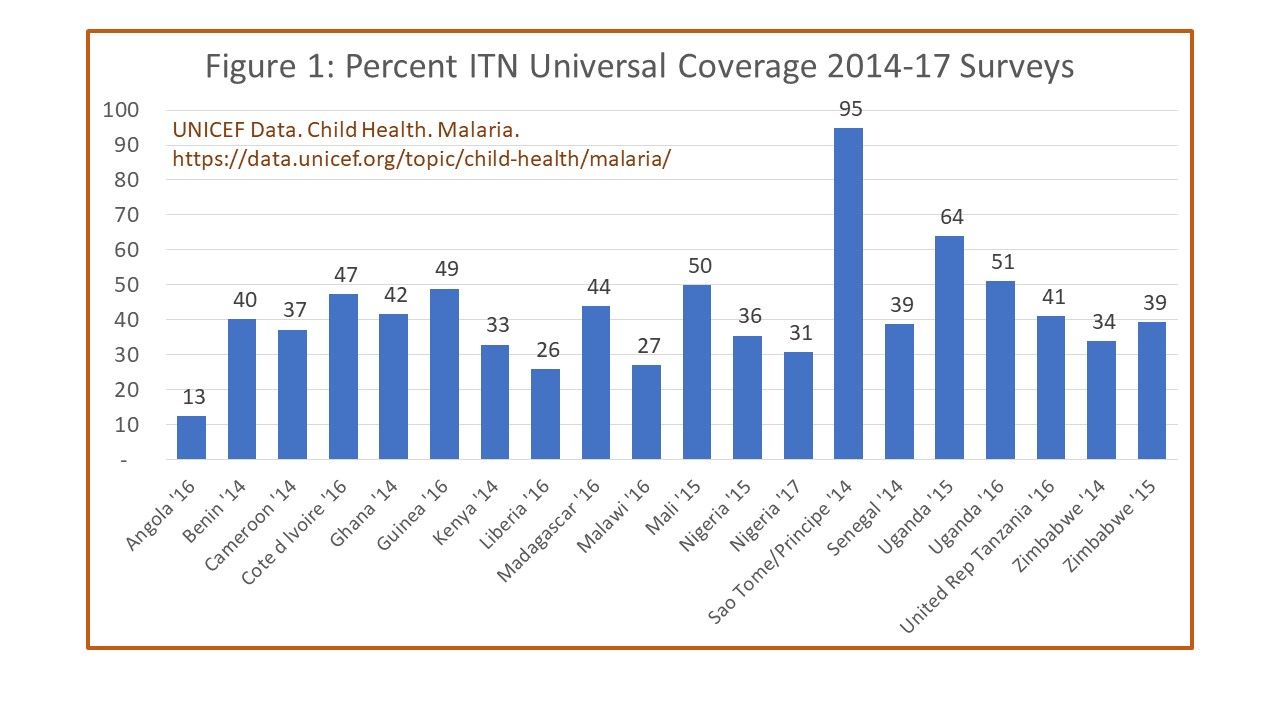 MICS survey data per country between 2014 and 2017. For the indicator of one ITN per to people in a household, shows Angola at only 13%, most countries for which recent data are available reached between 40-50%. Only two achieved above 60% on a point-in-time survey, Uganda at 62% and Sao Tome and Principe at 95%. The website shows information that where there were multiple surveys in a country during the period, there were variations, sometimes quite wide, over the years. Aside from the fact that the surveys may have had slightly different procedures, the problem remains of achieving and sustaining UHC for ITNs.
MICS survey data per country between 2014 and 2017. For the indicator of one ITN per to people in a household, shows Angola at only 13%, most countries for which recent data are available reached between 40-50%. Only two achieved above 60% on a point-in-time survey, Uganda at 62% and Sao Tome and Principe at 95%. The website shows information that where there were multiple surveys in a country during the period, there were variations, sometimes quite wide, over the years. Aside from the fact that the surveys may have had slightly different procedures, the problem remains of achieving and sustaining UHC for ITNs.
Another factor that affects maintaining UHC for ITNs, assuming the target can be met is the durability of nets. The physical integrity as well as the insecticide efficacy can decline over time. Intact nets may lose their insecticide through improper washing and drying, yet still prevent mosquito bites to the individual sleeping under them. Nets with holes may still maintain a minimal level of effective insecticide and may not fully prevent bites but ultimately kill the mosquito that flies through. Researchers in Senegal have been grappling with these challenges.
 Program managers must themselves grapple with whether such compromised nets count toward universal coverage as well as how often to conduct net replacement campaigns. A report from community surveys in Uganda during 2017 found that, “Long-lasting insecticidal net ownership and coverage have reduced markedly in Uganda since the last net distribution campaign in 2013/14.” UHC for ITNs is always a moving target.
Program managers must themselves grapple with whether such compromised nets count toward universal coverage as well as how often to conduct net replacement campaigns. A report from community surveys in Uganda during 2017 found that, “Long-lasting insecticidal net ownership and coverage have reduced markedly in Uganda since the last net distribution campaign in 2013/14.” UHC for ITNs is always a moving target.
A frequently unaddressed issue in seeking to improve ITN coverage is whether it makes a difference in malaria disease. A study in Malawi reported that although ITNs per household increased from 1.1 in 2012 to 1.4 in 2014, the prevalence of malaria in children increased over the period from 28% to 32%. The authors surmised that factors such as insecticide resistance, irregular ITN use and inadequate coordinated use of other malaria control interventions may have influenced the results. This shows that UHC for ITNs cannot be viewed in isolation.
This brings up the issue of the role of the many different vector control measures available. Researchers in Côte d’ Ivoire examined the use of eave nets and window screening. At present eave nets are mainly deployed in research contexts but use of window and door screening and netting are a commercially available interventions that households employ on their own. One wonders then whether UHC should focus on how the household and the people therein are protected by any malaria vector intervention.
 Here the discussion should focus on the question raised by colleagues in the USAID/PMI Vectorworks Project. WHO declared a goal of universal ITN coverage in 2009 using the target f one ITN/LLIN for every two household members. Vectorworks found that a decade on only one instance of a country briefly achieving 80% of this UHC net target, whereas no others reached above 60%. In fact, the bigger the household, the less chance there was of meeting the two people for one ITN target. Just because people live in a household that has the requisite number of nets, does not guarantee the actual target for sleeping under a net can be achieved because of practical or cultural realities in a household. Neither the minimal indicator of having at least one net in a household, or the ideal or ‘perfect’ indicator of UHC are satisfactory for judging population protection.
Here the discussion should focus on the question raised by colleagues in the USAID/PMI Vectorworks Project. WHO declared a goal of universal ITN coverage in 2009 using the target f one ITN/LLIN for every two household members. Vectorworks found that a decade on only one instance of a country briefly achieving 80% of this UHC net target, whereas no others reached above 60%. In fact, the bigger the household, the less chance there was of meeting the two people for one ITN target. Just because people live in a household that has the requisite number of nets, does not guarantee the actual target for sleeping under a net can be achieved because of practical or cultural realities in a household. Neither the minimal indicator of having at least one net in a household, or the ideal or ‘perfect’ indicator of UHC are satisfactory for judging population protection.
The Vectorworks team suggests that, “Population ITN access indicator is a far better indicator of ‘universal coverage’ because it is based on individual people,” and can be compared to, “The proportion of the population that used an ITN the previous night, which enables detailed analysis of specific behavioral gaps nationally as well as among population subgroups.” Population access to ITNs therefore, provides a batter basis for more realistic policies and strategies.
We have seen that defining as well as achieving universal coverage of malaria interventions is a challenging prospect. For example, do we base our monitoring on households or populations? Do we have the funds and technical capacity to implement and sustain the level of coverage required to have an impact on malaria transmission and move toward elimination? Are we able to introduce new, complimentary and appropriate interventions as a country moves closer to elimination?
A useful perspective would be determination if households and individuals even benefit from any part of the malaria package, even if everyone does not have access and utilize all components. This may be why zero malaria has to start with each person living in endemic areas.
on 27 Apr 2019 at 4:59 am 1.Zero Malaria Starts with Universal Coverage: Part 1 Nets said …
[…] See the article here: Zero Malaria Starts with Universal Coverage: Part 1 Nets […]