During a press conference prior to the release of the executive summary of 3-year study of trends and future projections for the factors and determinants that underpin malaria by its Strategic Advisory Group on Malaria Eradication (SAGme), WHO outlined some hopeful signs emanating from the SAGme including
Lack of biological barriers to malaria eradication
Recognition of the massive social and economic benefits that would provide a return on investment in eradication, and
Megatrends in the areas of factors such as land use, climate, migration, urbanization that could inhibit malaria transmission
Concerning the first point, the executive summary notes that, “We did not identify biological or environmental barriers to malaria eradication. In addition, our review of models accounting for a variety of global trends in the human and biophysical environment over the next three decades suggest that the world of the future will have much less malaria to contend with.”
The group did agree that, “using current tools, we will still have 11 million cases of malaria in Africa in 2050.” So one wonders whether there are biological barriers or not.
Interestingly the group did identify, “Potential biological threats to malaria eradication include development of insecticide and antimalarial drug resistance, vector population dynamics and altered vector behaviour. For example, Anopheles vectors might adapt to breeding in polluted water, and mosquito vector species newly introduced to Africa, such as Anopheles stephensi, could spread more widely into urban settings.”
Their further expansion on the biological issues using smallpox as an example is instructive. They noted that not only are humans essential for the life cycle of the organism, but that there was no other reservoir for the causative virus, and the virus could not amplify in the environment. In short, there were no vectors, as in the case of malaria. The relatively recent documentation of transmission of malaria between humans and other primates of different plasmodium species is another biological concern. At this point, Malaysia, for example, is reporting more cases of Plasmodium knowlesi in humans that either P vivax or P falciparum.
Another biological issue identified by Aylward and colleagues was the fact that smallpox had one effective and proven intervention, the vaccine. Application of the vaccine could be targeted using photograph disease recognition cards as the signs were quite specific to the disease. Malaria has several effective interventions, but most strategies emphasize the importance of using a combination of these, and implementation is met with a number of management and logistical challenges. The signs and symptoms of malaria are confused with a number of febrile illnesses.
Finally, two other issues raised concern. Insecticide resistance was recognized in the first malaria eradication effort, and is raising its head again, as pointed out by SAGme. Comparing smallpox and yaws, the challenge of latent or sub-clinical/asymptomatic infection was mentioned. Malaria too, is beleaguered with this problem.
Clearly, we must not lose momentum in the marathon (not a race) to eliminate malaria, but we must, as WHO stressed at the press conference, increase our research and development efforts to strengthen existing tools and develop new once to address the biological and logistical challenges.
As part of the course on Social and Behavioral Foundations in Primary Health Care, Rebecca Huebsch posted in the class blog. We have shared these thoughts below.
91,000 people die from cholera every year. Cholera is a burden which is carried by some of the poorest and most vulnerable people in the world. This disease, which puts about 1.4 billion people at risk annually, is most predominant in low-income nations. One of these nations is South Sudan. Since its independence in 2011, South Sudan has been plagued by ongoing conflict, displacements, poverty, and disease outbreaks. In South Sudan’s most recent cholera outbreak, there were already 20,000 cases before the outbreak could be brought under control.
Controlling a cholera outbreak requires a combination of approaches; water and sanitation, hygiene promotion, case management, and reactive vaccination campaigns. The oral cholera vaccine (OCV) revolutionized cholera responses and made it possible protect people from this dangerous disease. OCV campaigns are still incredibly resource intense and traditionally target each person with 2-doses of the vaccine. In places like South Sudan, even reaching these people once is difficult, finding them a second time requires a great deal of motivation, resources, and creativity. In the rainy season, large swaths of South Sudan are flooded and become swamps. This is also the time of year that people are most at risk of cholera. A vaccination campaign requires vaccination teams to literally walk through the swamps for hours, or even days, to reach the affected areas.
Fortunately, a more streamlined approach is possible, and has even been tested in emergency cholera responses in South Sudan. There is a growing body of evidence that supports a single-dose strategy for OCV campaigns. In settings where cholera is endemic, like South Sudan, a single dose of OCV can be as effective as 2 doses for controlling an outbreak. Adopting this strategy would allow the same amount of vaccine to protect double the amount of people. It would also save on the logistical costs of trying to reach each person twice. While a second dose of cholera vaccine makes sense for routine immunization programs because it provides prolonged coverage, it is costly and limiting to an emergency response. In a cholera outbreak, the State Ministries of Health may look to a single-dose strategy to more efficiently control the outbreak and protect their people.
As part of the course on Social and Behavioral Foundations in Primary Health Care, Muhammad N Asghar posted in the class blog. We have shared these thoughts below.
Pakistan is one of the three polio endemic countries and recent surge in cases shows that eradication of the disease demands an urgent change in strategy. A look at previous five year cases in Pakistan shows a positive progress in reduction of new polio cases; from 307(2014) to 12(2018), but new cases still appeared in almost every province. The reasons behind this country wide presence of disease can be attributed to internal displacement due to conflicts, weak health systems and operational and resource risks. But the alarming increase in number of new polio cases during 2019 has reversed the whole progress made so far as the number of new cases as of today stands at 53. 32 out of 53 cases are reported from KPK region, which had observed massive internal displacement during last decade but the number of IDPs has decreased from last two years due to stability in the region.
This recent surge in polio cases in the the province is mainly due to increase in vaccine refusals due to rumors regarding side effects caused by the vaccine on social media. Official sources reported that after rumors refusals to vaccinate increased by 85% in the province. But high number of cases in other provinces when compared with last year cases indicate that multiple factors are hindering the progress towards containment and eradication of the polio virus disease from the country, which can be attributed to homelessness and poor sanitation, operational issues for vaccine delivery, conflicts, cross border movement etc.
This situation demands urgent review of existing strategy for polio eradication as number of new cases are increasing rapidly. There is a need to work on multiple aspects to make the anti-polio drive successful; some key aspects include detailed geo-mapping of the population at basic level and identification of missed areas to ensure every child is vaccinated, involving community and religious leaders, NGOs, CSOs for confidence building and education of the community, expansion of partnership with nutrition, hygiene, water sectors, and robust rebuttal of rumors and strict action against those involved in such heinous activities etc. There is a new political government of helm, which is sensitive to the social sector issues and taking measures to provide homes, health facilities and education to the disadvantaged sections. International agencies (GPEI, WHO) shall coordinate with the political government to review the existing strategy for revamping it, so that not only the current surge can be contained but the disease can be eradicated from the country to achieve the target of polio free world.
This posting focuses on Malaria and Ebola, both of which have been the recent focus of some disturbing news. The malaria community has been disturbed by the clear documentation of resistance to drugs in Southeast Asia. Those working to contain Ebola in the northeast of the Democratic Republic of Congo saw a change in political leadership even in light of continued violence and potential cross-border spread.
Malaria Drug Resistance
Several sources reported on studies in the Lancet Infectious Diseases concerning the spread of Multidrug-Resistant Malaria in Southeast Asia. Reuters explained that by sing genomic surveillance, researchers concurred that “strains of malaria resistant to two key anti-malarial medicines are becoming more dominant” and “spread aggressively, replacing local malaria parasites,” becoming the dominant strains in Vietnam, Laos and northeastern Thailand.”
The focus was on “the first-line treatment for malaria in many parts of Asia in the last decade has been a combination of dihydroartemisinin and piperaquine, also known as DHA-PPQ,” and resistance had begun to spread in Cambodia between 2007 and 2013. Authors of the study noted that while, “”Other drugs may be effective at the moment, but the situation is extremely fragile, and this study highlights that urgent action is needed.” They further warned of an 9impending Global Health Emergency.
NPR notes that “Malaria drugs are failing at an “alarming” rate in Southeast Asia” and provided some historical context about malaria drug resistance arising in this region since the middle of the 20th century. “Somehow antimalarial drug resistance always starts in that part of the world,” says Arjen Dondorp, who leads malaria research at the Mahidol Oxford Tropical Medicine Research Unit in Bangkok and who was a lead author of the report about the randomized trial. Ironically, “one reason could have something to do with the relatively low levels of malaria there. When resistant parasites emerge, they are not competing against a dominant nonresistant strain of malaria and are possibly able to spread easier.
When we are talking about monitoring resistance in low resource and logistically and politically challenging areas, we need to think of appropriate diagnostic tools at the molecular level. Researchers in Guinea-Bissau conducted a proof of concept study and used malaria rapid diagnostic tests applied for parallel sequencing for surveillance of molecular markers. While they noted that, “Factors such as RDT storage prior to DNA extraction and parasitaemia of the infection are likely to have an effect on whether or not parasite DNA can be successfully analysed … obtaining the necessary data from used RDTs, despite suboptimal output, becomes a feasible, affordable and hence a justifiable method.”
A Look at Insecticide Treated Nets
On a positive note, Voice of America provides more details on the insecticide treated net (ITN) monitoring tool developed called “SmartNet” by Dr Krezanoski in collaboration with the Consortium for Affordable Medical Technologies in Uganda. The net uses strips of conductive fabric to detect when it’s in use. Dr. Krezanoski was happy to find that people given the net used it no differently that if they were not being observed. The test nets made it clear who what using and not using this valuable health investment and when it was in use. Such fine tuning will be deployed to design interventions to educate net users based on their real-life use patterns.
Another important net issue is local beliefs that may influence use. We can find out when people use nets, but we also need to determine why. In Tanzania, researchers found that people think mosquitoes that bite in the early evening when people are outside relaxing are harmless. As one community member said, “I only fear those that bite after midnight. We’ve always been told that malaria is spread by mosquitoes that bite after midnight.”
Even if people do use their ITNs correctly, we still need to worry about insecticide resistance. A study in Afghanistan reported that, “Resistance to different groups of insecticides in the field populations of An. stephensi from Kunar, Laghman and Nangarhar Provinces of Afghanistan is caused by a range of metabolic and site insensitivity mechanisms.” The authors conclude that vector control programs need to be better prepared to implement insecticide resistance management strategies.
Ebola Crisis Becomes (More) Political
Headlines such as “Congo health minister resigns over response to Ebola crisis” confronted the global health community this week. this happened after the DRC’s relatively new president took control of the response. The President set up a new government office to oversee the response to an outbreak outside of the Ministry of Health which was managing the current outbreak and the previous ones. The new board was set up without the knowledge of the Minister who was traveling to the effected provinces at the time.
The former Minister, Dr Oly Ilunga stated on Twitter that, “Suite à la décision de la @Presidence_RDC. de gérer à son niveau l’épidémie d’#Ebola, j’ai remis ma démission en tant que Ministre de la Santé ce lundi. Ce fut un honneur de pouvoir mettre mon expertise au service de notre Nation pendant ces 2 années importantes de notre Histoire. (Following the decision of the @Presidence_RDC to manage the # Ebola outbreak, I resigned as Minister of Health on Monday. It was an honor to be able to put my expertise at the service of our Nation during these two important years of our History.)
The former Minister also warned that the “Multisectoral Ebola Response Committee would interfere with the ongoing activities of national and international health workers on the ground in North Kivu and Ituri provinces.” Part of the issue may likely have been “pressure to approve a new vaccine in addition to one that has already been used to protect more than 171,000 people.” People had warned about the potential confusion to the public as well as ethical issues if a second vaccine was used, especially one that did not have the strong accumulated evidence from both the current outbreak as well as the previous one in West Africa.
One might have thought that this would be a time when stability was needed since “The WHO earlier this month declared the outbreak a Public Health Emergency of International Concern, a rare step meant to highlight the urgency of the moment that has been used only four times before.” In addition, “the World Bank said it would release $300 million from a special fund set aside for crises like viral outbreaks to help cover the cost of the response.”
Unfortunately one of the msain impediments to successful Ebola control, violence in the region, continues. CIDRAP stated that. “the Allied Democratic Forces (ADF), a rebel group, attacked two villages near Beni, killing 12 people who live in the heart of the Democratic Republic of the Congo’s (DRC’s) ongoing Ebola outbreak. The terrorists killed nine in Eringeti and three in Oicha, according to Reuters. ADF has not publicly pledged allegiance to the Islamic state (ISIL), but that hasn’t stopped ISIL from claiming responsibility for the attacks.” It will take more than a change of structure in Kinshasa to deal with the realities on the ground.
CIDRAP also observed that since the resignation of the Health Minister, “DRC officials have provided no update on the outbreak, including statistics on the number of deaths, health workers infected, or suspected cases.” The last was seen on 21 July 2019.
ReliefWeb reports that, “Adding to the peril, the Ebola-affected provinces share borders with Rwanda and Uganda, with frequent cross-border movement for personal travel and trade, increasing the chance that the virus could spread beyond the DRC. There have already been isolated cases of Ebola reported outside of the outbreak zone.”
These are troubling times when parasites and mosquitoes are becoming more resistant to our interventions and when governments and communities are resistant to a clear and stable path to disease containment and control.
In the past week more attention was drawn to the apparently never-ending year-long Ebola outbreak in the northeast of the Democratic Republic of the Congo. Regarding other diseases, there is new information on the RTS,S malaria vaccine, river prawns have been found to play a biological control role in schistosomiasis, and an update from the World Health Organization on essential medicines and diagnostics. New malaria vector control technologies are discussed.
Second Largest Ebola Outbreak One Year On
Ronald A. Klain and Daniel Lucey in the Washington Post observed raised concern that, “the disease has since crossed one border (into Uganda) and continues to spread. In the absence of a trajectory toward extinguishing the outbreak, the opposite path — severe escalation — remains possible. The risk of the disease moving into nearby Goma, Congo — a city of 1 million residents with an international airport.”
They added their voices to a growing number of experts who are watching this second biggest Ebola outbreak in history and note that, “As the case count approaches 2,500 with no end in sight, it is time for the WHO to declare the outbreak a public health emergency of international concern — a ‘PHEIC’ — to raise the level of global alarm and signal to nations, particularly the United States, that they must ramp up their response.” They call for three actions: 1) improved security for health workers in the region, 2) stepped up community engagement and 3) extended health care beyond Ebola treatment. The inability to adequately respond to malaria, diarrheal diseases and maternal health not only threated life directly, but also threated community trust, putting health workers’ lives at risk.
Olivia Acland, a freelance journalist based in DRC, reporting for the New Humanitarian describes the insecurity and the recent “wave of militia attacks in the Democratic Republic of Congo’s northeastern Ituri province has left hundreds dead and roughly 300,000 displaced in recent weeks, triggering a new humanitarian crisis in a region.” Specifically, “Ituri, a fertile region rich in gold deposits, has been an epicentre of conflict in Congo for decades. Between 1999 and 2003, around 60,000 people were killed here, as a power struggle between rebel groups escalated into ethnic violence,” related to traditional tensions between Hema cattle herders and Lendu farmers with roots in Belgian colonization.
Updates from the DRC Ministry of Health report on average 11 new Ebola cases per day in the past week. So far over 160,000 people have been vaccinated, and yet the spread continues. The Ministry also describes new protocol contains three vaccinations strategies that can be used depending on the environment in which confirmed cases are found including:
Classic Ring: The classic strategy of vaccinating contacts of confirmed cases and contact contacts.
Enlarged ring: It is also possible to vaccinate all inhabitants of houses within 5 meters around the outbreak of a confirmed case.
Geographical Ring: In an area where team safety can not be guaranteed, they can vaccinate an entire village or neighborhood.
Malaria Vaccines, Essential Drugs and New Vector Control Technologies
Halidou Tinto and colleagues enrolled two age groups of children in a 3-year extension of the RTS,S/AS01 vaccine efficacy trial: 1739 older children (aged 5–7 years) and 1345 younger children (aged 3–5 years). During extension, they reported 66 severe malaria cases. Overall they found that, “severe malaria incidence was low in all groups, with no evidence of rebound in RTS,S/AS01 recipients, despite an increased incidence of clinical malaria in older children who received RTS,S/AS01 compared with the comparator group in Nanoro. No safety signal was identified,” as seen in The Lancet.
WHO has updated the global guidance on medicines and diagnostic tests to address health challenges, prioritize highly effective therapeutics, and improve affordable access. Section 6.5.3 presents antimalarial medicines including curative treatment (14 medicines) for both vivax and falciparum and including tablets and injectables. Prophylaxis includes 6 medicines including those for IPTp and SMC. The latest guidance can be downloaded at WHO.
Paul Krezanoski reports on a new technology to monitor bednet use and tried it out in Ugandan households. As a result. “Remote bednet use monitors can provide novel insights into how bednets are used in practice, helping identify both households at risk of malaria due to poor adherence and also potentially novel targets for improving malaria prevention.
In another novel technological approach to vector control, Humphrey Mazigo and co-researchers tested malaria mosquito control in rice paddy farms using biolarvicide mixed with fertilizer in Tanzanian semi-field experiments. The intervention sections (with biolarvicide) had lowest mean mosquito larvae abundance compared to control block and did not affect the rice production/harvest.
Prawns to the Rescue in Senegal Fighting Schistosomiasis and Poverty
The researchers in Senegal said that, “market analysis in Senegal had shown there was significant interest among restaurant owners and farmers in introducing prawns to the diet.” The prawn could also for the basis of aquaculture in rice paddies and remove the threat of schistosomiasis from the rice workers.
—- Thank you for reading this week’s summary. These weekly abstractings have replaced our occasional mailings on tropical health issues due to fees introduced by those maintaining the listserve website. Also continue to check the Tropical Health Twitter feed, which you can see running on this page.
For almost 20 years we have been maintaining an email list where current news and articles have been shared with those interested in tropical health and malaria. The listserve host we have been using is changing to a paid model. While there are still some free listserve options, these are cumbersome to produce. Since we are already maintaining this blog, we thought it best to provide a weekly summary of key news events through this medium.
Mapping Plasmodium Vivax
The Malaria Atlas Project has published in The Lancet a global burden of Plasmodium Vivax mapping study. The authors describe the contribution of this study as: “Our study highlights important spatial and temporal patterns in the clinical burden and prevalence of P vivax. Amid substantial progress worldwide, plateauing gains and areas of increased burden signal the potential for challenges that are greater than expected on the road to malaria elimination. These results support global monitoring systems and can inform the optimisation of diagnosis and treatment where P vivax has most impact.”
Ebola Spread from DRC to Uganda
Since the major ongoing outbreak of Ebola Virus Disease in North Kivu and Ituri Provinces of the Democratic Republic of Congo (DRC) started nearly a year ago, there has been concern that the disease might spread to neighboring countries like Uganda, Rwanda, South Sudan and the Central African Republic. This fear same true recently when a family affected by Ebola crossed from DRC into Uganda to connect with relatives in Kasese District Uganda. Uganda has had many years’ experience dealing with Ebola and was able to contain the situation.
A press release this week noted that, “As of today (21 June 2019), Uganda has not registered any new confirmed Ebola Virus Disease (EVD) case in Kasese District or any other part of Uganda since the last registered case one week ago. There are no new suspect cases under admission. Currently, 110 contacts to the confirmed Ebola cases in Kagando and Bwera are being followed up daily. A total of 456 individuals have been vaccinated against EVD using the Ebola-rVSV vaccine in Kasese District, Western Uganda.”
Although many people expected that the meeting of the “International Health Regulations (2005) Emergency Committee} for Ebola virus disease in the Democratic Republic of the Congo would finally declare the current outbreak a Public Health Emergency of International Concern (PHEIC) because it crossed a border, the result was noting that the challenge was still an emergency only for DRC. WHO did note that there were serious funding gaps and support from other countries for the DRC’s predicament. Ironically, such gaps make it more likely that Ebola can spread more widely.
As of 21 June 2019, the DRC reported a total of 2,211 cases since the start of the epidemic last year, of which 2,117 have been confirmed and 94 are probable. There have been 1,489 deaths. To date 139,027 persons have been vaccine with the Merck rVSV-ZEBOV vaccine.
Progress toward Eliminating Malaria – the E-2020 Countries
The process of eliminating malaria from the world needs to start in a step-by-step fashion. WHO explained that, “Creating a malaria-free world is a bold and important public health and sustainable development goal. It is also the vision of the Global technical strategy for malaria 2016-2030, which calls for the elimination of malaria in at least 10 countries by the year 2020.”
Actually, WHO identified 21 countries, spanning 5 regions, that could defeat malaria by 2020. The progress report charts the effort. During the recent World Health Assembly two countries received recognition for being certified malaria-free, Argentina and Algeria. This week WHO also announced that 5 more countries have not had malaria cases in the past year. There was also release of a downloadable report on progress toward the 2020 target for selected countries.
Reconsidering Yaws Eradication
In the 1950s and 1960s the world focused on the possibility of eradicating Yaws through screening and treatment interventions. Like the early malaria eradication programs from the same period, the Yaws effort slowed, stopped and experienced a resurgence. The Telegraph reported that, “Between 1952 and 1964, Unicef and the WHO screened some 300 million people for the illness, in a coordinated programme which treated more than 50 million cases. Yaws was on the brink of being wiped out and reports of the disease dropped by 95 per cent.” WHO continues to work on treatment strategies with azithromycin and for resistant cases, benzathine benzylpenicillin injection.
WHO noted that there were 80,472 cases reported in 2018, although this figure is likely to be much higher in actuality. The challenge of case detection exists but may be overcome, according to the Telegraph with a new molecular rapid diagnostic test which detects yaws within 30 minutes, and thus could allow on-the-spot diagnosis in remote regions.
Measles Cases Continue to Increase
The problem of measles in the DRC may not be receiving much attention because of the Ebola epidemic. Ironically, Outbreak News Today reports that, “In a follow-up on the measles outbreak in the Democratic Republic of the Congo (DRC), UN health officials report an additional 7500 suspect cases in the past 2 weeks, bringing the total cases since the beginning of the year to 106,870. The death toll due to the measles outbreak has reached 1815 deaths (case fatality ratio 1.7%).”
Vaccine coverage challenges in the DRC result from health systems weaknesses. Unfortunately, a global study has shown that increasing cases in the Global North are not due to weak systems, but ‘vaccine hesitancy.’ The Guardian reports that a global survey has revealed the scale of the crisis of confidence in vaccines in Europe, “showing that only 59% of people in western Europe and 50% in the east think vaccines are safe, compared with 79% worldwide.” The Guardian observes that, “In spite of good healthcare and education systems, in parts of Europe there is low trust in vaccines. France has the highest levels of distrust, at 33%.”
For more news and daily updates check our other services, a closed/private Facebook Group and a Twitter feed. For those who do not use social media, please check here each weekend to find a summary of some of the stories we have shared during the week.
Erin Fleming has recently posted a perspective on the new malaria vaccine intervention testing at “Social, Cultural & Behavioral Issues in PHC & Global Health.” See her observations below.
Malaria is one of the world’s deadliest diseases. In Malawi, it is endemic across 95 percent of the country and is one of the leading causes of morbidity and mortality across all ages, and has a disproportionate impact on children under 5. In collaboration with many international partners such as the Centers for Disease Control and Prevention (CDC), the Global Fund to Fight AIDS, Tuberculosis and Malaria, the United States Agency for International Development (USAID), and Gavi, the Vaccine Alliance, the Malawian Ministry of Health’s Malaria Control Program has been combating malaria for years by scaling up distribution of artemisinin-based combination therapies (ACTs), intermittent preventive treatment for pregnant women (IPTp) using sulfoxide-pyrimethamine (SP), and insecticide-treated net (ITNs) based on the World Health Organization’s (WHO) malaria guidelines and national level policies. But now, they may potentially have another tool to add to their existing package of services, a malaria vaccine!
Moms waiting for the malaria vaccine for their children in Malawi.
On April 23, 2019, Malawi, 1 of 3 countries selected for the Malaria Vaccine Implementation Programme (MVIP) pilot rolled out RTS,S/AS01 (RTS,S) – also known as Mosquirix , as part of their routine immunization for children under 5. It has been met with great excitement, as early speculation is that the vaccine could be a gamechanger in the fight against malaria. But there is still a way to go, four years to be exact after the completion of the pilot and research, before we know for sure. IF the pilot findings present positive results, i.e. higher levels of efficacy and effectiveness, does not have any severe adverse health effects, and can be incorporated into national immunization programs, then yes, we may have on our hands a new control to help reduce severe malaria morbidity and mortality in children under 5 in a significant way.
Now, despite my excitement regarding the potential impact RTS,S could have on malaria on childhood morbidity and mortality, it is too soon to tell. I am supportive of the vaccine pilot and the potential inclusion into policies and see the life changing benefits for patients, but with reservations. And, perhaps I am taking a more conservative stance based on my experience working and living in sub-Saharan Africa, seeing firsthand some of the systemic issues (i.e. lack of human resources, funding, poor infrastructure – in particular supply chain management, and government commitment) that continue to plague the efforts being made to improve health service delivery – all of which directly impacts routine immunization programs. That said, I’m eager to see what the pilot results yield, in particular as it relates to the economic and operational feasibility of implementation in low-income countries who are the hardest hit by malaria.
But while we wait, we must not lose track of continuing to implement existing prevention approaches and enforcing adherence to treatment guidelines, especially as we know malaria is on the rise again in Malawi, and around the world. There still needs to be significant increases of support and investment from cooperating governments and international stakeholders in improved surveillance systems and research on some of the challenges we’re encountering with existing methodologies, i.e. increased insecticide and anti-malarial drug resistance, and the biggest “unknown” of them all, how climate change will impact the mosquito burden and potentially increase the reach of this deadly disease globally.
Ramatsobane Johanna Ledwaba provides us with a guest blog to address the need to reach more school aged girls with vaccines for human papilloma (HPV) virus in South Africa and in the process prevent cervical cancer. Her blog originally appeared in Social, Cultural & Behavioral Issues in PHC & Global Health.
Cervical cancer is the first most common cancer in women and the first leading cancer related-deaths among South African women, aged 15-44 years. More that 12,000 women are diagnosed with cervical cancer annually, of which 5,500 die from cancer— age-specific incidence rate (15-44 years) of 41.8 per 100,000 women per year and age-specific mortality rate (15-44 years) of 11,7 per 100,000 women per year. Reasons for such a high mortality rate include, low screening coverage of 19.3%, and late presentation with an advanced stage compounded by the high HIV epidemic. The World Health Organization recommends a 2-dose HPV vaccination among girls of 9-13 years.
In 2014, the South African National Department of Health introduced a school-based HPV vaccination policy— using 2-dose Cervarix vaccine, as prevention for cervical cancer among girls aged 9 and above in grade 4 attending public schools. The policy aimed to vaccinate 500, 000 young girls from 18,000 public schools before their sexual debut.
HPV vaccine campaign poster distributed by the Department of Health. Source: Government Communication and Information SystemPreliminary data showed that 91% of schools were reached and 87% age eligible grade 4 girls were vaccinated, however there is a high dropout rate in the second dose.
Although the programme seems a success thus far, there is a need for expanded coverage of the vaccine to include higher grades that could potentially house girls of ages 11-13 years. In addition, the vaccine must be widely available at public health facilities for girls who were missed at school because they changed schools or dropped out.
Girls attending private schools are presumed to access HPV vaccine through the private health sector, however the HPV vaccine coverage in the private health sector remains low due to high costs and lack of awareness— which suggest that there is low coverage in private schools. Therefore, the vaccine must be expanded to include private schools. This gap may lead to poor coverage of HPV vaccination and may also increase perceptions or hesitancy against the vaccine because it is not widely available for all girls of targeted age. No girl must be left behind.
Newer malaria interventions are coming on board, and whether these will be used of a large scale or targeted to certain epidemiological contexts remains to be seen. In each case, one will need to examine if in each context one can measure whether the intervention is universally accessible to and used by the intended population or subgroup.
WHO explains that, “The malaria vaccine pilot aims to reach about 360,000 children per year across the three countries. Ministries of health will determine where the vaccine will be given; they will focus on areas with moderate-to-high malaria transmission, where the vaccine can have the greatest impact.” There will be a strong monitoring component to identify coverage levels as well as any implementation challenges and adverse effects that may only become visible in a larger scale intervention that the typical efficacy trials. Implementation is occurring in areas with a relatively strong existing malaria control effort, with an intent to learn how a vaccine can complement a total control package.
Mass Drug Administration (MDA, also known as preventive chemotherapy) has been a successful strategy for controlling and eliminating neglected tropical diseases with special reference to onchocerciasis, lymphatic filariasis, trachoma, soil transmitted helminths and schistosomiasis. MDA use in malaria has been limited due to a number of financial and logistical challenges, not the least of which is the need to achieve high coverage over several periods of distribution. This is why WHO recommends, “Use of MDA for the elimination of P. falciparum malaria can be considered in areas approaching interruption of transmission where there is good access to treatment, effective implementation of vector control and surveillance, and a minimal risk of re-introduction of infection.”
Another link with MDA for a different disease, onchocerciasis, has pointed to a potential new malaria intervention. Around ten years ago it was observed that after ivermectin treatment for onchocerciasis in Senegal survivorship of malaria vectors was reduced. Subsequently the potential effect of ivermectin has been intentionally researched with the outcome that, “Frequently repeated mass administrations of ivermectin during the malaria transmission season can reduce malaria episodes among children without significantly increasing harms in the populace.” Mathematical models for onchocerciasis control have predicted the need to achieve annual coverage targets below what could be called universal levels. Using ivermectin for mosquito control would require more frequent dosing and higher coverage.
Although not defined as ‘new’ it is important to include mention of additional vector interventions like larviciding and indoor residual spraying, as these present technical and coverage challenges. For example, larviciding interventions either chemical or biological, do not cover individuals. These focus on breeding sites in communities. This may require better use of the concept of geographical coverage as has been used in onchocerciasis control wherein the proportion of endemic villages reached is monitored.
For example, in Mali the NTD program aimed to achieve 80% program coverage of individuals eligible for preventive chemotherapy and 100% geographical coverage yearly. This means all villages should be reached. In reality, the program achieved 85% geographical coverage for lymphatic filariasis and over 90% for onchocerciasis.
In conclusion, we have seen that defining as well as achieving universal coverage of malaria interventions is a challenging prospect. For example, do we base our monitoring on households, villages, or populations? Do we have the funds and technical capacity to implement and sustain the level of coverage required to have an impact on malaria transmission and move toward elimination? Are we able to introduce new, complimentary and appropriate interventions as a country moves closer to elimination?
Njabuliso Lukhele of the Ministry of Health Swaziland shared Swaziland’s experiences in Vaccine Procurement at the recent Regional Immunization Technical Advisory Group (RITAG) Meeting, Johannesburg, South Africa, 05-08 December 2017. A summary of his presentation appears below.
As a Lower Middle Income Country (MIC), Swaziland is not and has never been eligible to receive financial support for its immunization programs through the GAVI Alliance. Therefore, 83% of the health care budget is financed through domestic sources, and only 17% comes from from WHO and UNICEF.
Swaziland has a comprehensive Multi-Year plan (cMYP) that drives investment in immunization covering the period 2017–2021. The Government of Swaziland has been fully funding 100% of vaccine costs and average 96% of routine immunization costs over the last years. The Government of Swaziland procures vaccines and distribute to all service providers (government, regional referral and mission hospitals, public as well as private sector clinics and health facilities).
The vaccine Procurement Process begins as Requisitions are sent by Expanded Program of Immunizations (EPI) unit to the procurement unit through the chief pharmacist through documented minutes. This Minute is approved by the Financial Controller (FC) acknowledging availability of funds to furnish the procurement of the vaccines. Then a Tender document is drafted by both the EPI and procurement unit. Advertisement of tender document then takes place. Tender runs for 30 days as per procurement policy. Procurement of vaccines is done through open tender.
The 5 top vaccines (PCV, IPV, OPV, Rota, Penta) in Swaziland represented 98% of the total costs in 2015-16. While this is a major internal financial obligation, Vaccine procurement for the relatively small population of Swaziland represents approximately 0.2 percent of the overall African market by volume and about 0.4 percent by value. This puts smaller countries at a disadvantage in terms of getting good pricing and negotiating with suppliers.
Swaziland was one of the first countries for the Middle Income Country (MIC) strategy mission The MIC strategy mission recommended the need on generating efficiencies in the management of the programme, in particular in the area of procurement, with a need to explore pooled procurement as well as other options with the aim of maximizing savings on the high costs of vaccines. Government desires to achieve economic efficiency in procurement and consideration of pool procurement mechanism.
The current supplier charged 81,256,196.50 Swaziland Lilangeni (SZL) or roughly $5.8 million for the total package of vaccines needed in 2016. If UNICEF were to provide the same package it would cost SZL 62,215,336.34. or $4.5 million. While commercial suppliers can be paid on delivery, UNICEF requires approval from Ministry of Finance for the advance payment with the need to make sure the funds are sufficient for full payment.
This comparative information had valuable advocacy effect. Earlier this year (2017) a MOU signed between MOH and UNICEF. A commitment letter was sent to UNICEF supply division. Now Swaziland has a more reliable supplier and a more affordable cost, enhancing the Ministry’s capacity to save lives of its citizens. Swaziland can also serve as an example for the many other MICs and countries who are ‘graduating’ from GAVI support.
Sign up for daily or weekly articles from Bill highlighting the most noteworthy developments in newspapers and scientific journals. Click here to register.
 Concerning the first point, the executive summary notes that, “We did not identify biological or environmental barriers to malaria eradication. In addition, our review of models accounting for a variety of global trends in the human and biophysical environment over the next three decades suggest that the world of the future will have much less malaria to contend with.”
Concerning the first point, the executive summary notes that, “We did not identify biological or environmental barriers to malaria eradication. In addition, our review of models accounting for a variety of global trends in the human and biophysical environment over the next three decades suggest that the world of the future will have much less malaria to contend with.”


 Pakistan is one of the three polio endemic countries and recent surge in cases shows that eradication of the disease demands an urgent change in strategy. A look at previous five year cases in Pakistan shows a positive progress in reduction of new polio cases; from 307(2014) to 12(2018), but new cases still appeared in almost every province. The reasons behind this country wide presence of disease can be attributed to internal displacement due to conflicts, weak health systems and operational and resource risks. But the alarming increase in number of new polio cases during 2019 has reversed the whole progress made so far as the number of new cases as of today stands at 53. 32 out of 53 cases are reported from KPK region, which had observed massive internal displacement during last decade but the number of IDPs has decreased from last two years due to stability in the region.
Pakistan is one of the three polio endemic countries and recent surge in cases shows that eradication of the disease demands an urgent change in strategy. A look at previous five year cases in Pakistan shows a positive progress in reduction of new polio cases; from 307(2014) to 12(2018), but new cases still appeared in almost every province. The reasons behind this country wide presence of disease can be attributed to internal displacement due to conflicts, weak health systems and operational and resource risks. But the alarming increase in number of new polio cases during 2019 has reversed the whole progress made so far as the number of new cases as of today stands at 53. 32 out of 53 cases are reported from KPK region, which had observed massive internal displacement during last decade but the number of IDPs has decreased from last two years due to stability in the region. This recent surge in polio cases in the the province is mainly due to increase in vaccine refusals due to rumors regarding side effects caused by the vaccine on social media. Official sources reported that after rumors refusals to vaccinate increased by 85% in the province. But high number of cases in other provinces when compared with last year cases indicate that multiple factors are hindering the progress towards containment and eradication of the polio virus disease from the country, which can be attributed to homelessness and poor sanitation, operational issues for vaccine delivery, conflicts, cross border movement etc.
This recent surge in polio cases in the the province is mainly due to increase in vaccine refusals due to rumors regarding side effects caused by the vaccine on social media. Official sources reported that after rumors refusals to vaccinate increased by 85% in the province. But high number of cases in other provinces when compared with last year cases indicate that multiple factors are hindering the progress towards containment and eradication of the polio virus disease from the country, which can be attributed to homelessness and poor sanitation, operational issues for vaccine delivery, conflicts, cross border movement etc.
 The focus was on “the first-line treatment for malaria in many parts of Asia in the last decade has been a combination of dihydroartemisinin and piperaquine, also known as DHA-PPQ,” and resistance had begun to spread in Cambodia between 2007 and 2013. Authors of the study noted that while, “”Other drugs may be effective at the moment, but the situation is extremely fragile, and this study highlights that urgent action is needed.” They further warned of an 9impending Global Health Emergency.
The focus was on “the first-line treatment for malaria in many parts of Asia in the last decade has been a combination of dihydroartemisinin and piperaquine, also known as DHA-PPQ,” and resistance had begun to spread in Cambodia between 2007 and 2013. Authors of the study noted that while, “”Other drugs may be effective at the moment, but the situation is extremely fragile, and this study highlights that urgent action is needed.” They further warned of an 9impending Global Health Emergency.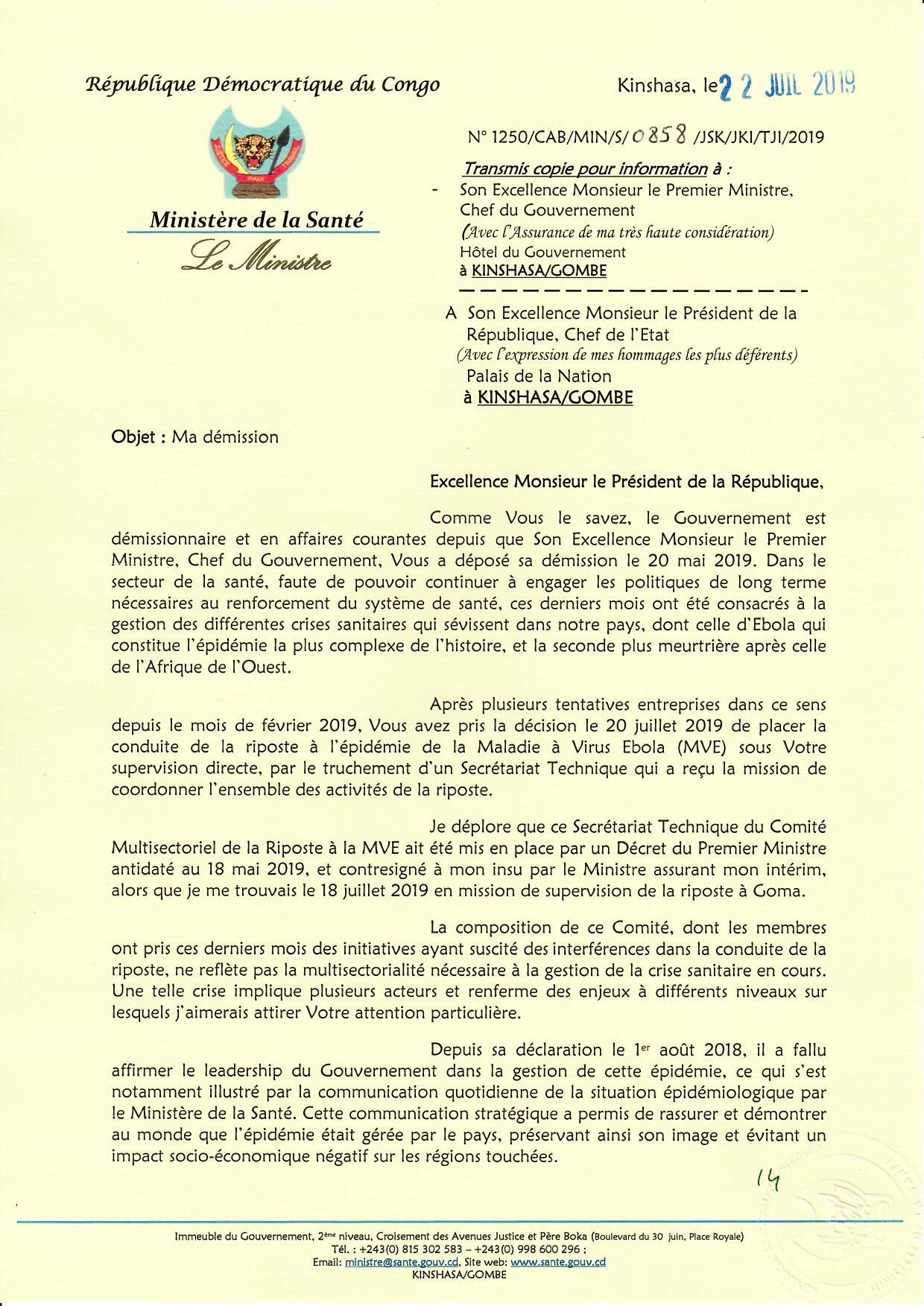 The former Minister, Dr Oly Ilunga stated on Twitter that, “Suite à la décision de la @Presidence_RDC. de gérer à son niveau l’épidémie d’#Ebola, j’ai remis ma démission en tant que Ministre de la Santé ce lundi. Ce fut un honneur de pouvoir mettre mon expertise au service de notre Nation pendant ces 2 années importantes de notre Histoire. (Following the decision of the @Presidence_RDC to manage the # Ebola outbreak, I resigned as Minister of Health on Monday. It was an honor to be able to put my expertise at the service of our Nation during these two important years of our History.)
The former Minister, Dr Oly Ilunga stated on Twitter that, “Suite à la décision de la @Presidence_RDC. de gérer à son niveau l’épidémie d’#Ebola, j’ai remis ma démission en tant que Ministre de la Santé ce lundi. Ce fut un honneur de pouvoir mettre mon expertise au service de notre Nation pendant ces 2 années importantes de notre Histoire. (Following the decision of the @Presidence_RDC to manage the # Ebola outbreak, I resigned as Minister of Health on Monday. It was an honor to be able to put my expertise at the service of our Nation during these two important years of our History.) The former Minister also warned that the “Multisectoral Ebola Response Committee would interfere with the ongoing activities of national and international health workers on the ground in North Kivu and Ituri provinces.” Part of the issue may likely have been “pressure to approve a new vaccine in addition to one that has already been used to protect more than 171,000 people.” People had warned about the potential confusion to the public as well as ethical issues if a second vaccine was used, especially one that did not have the strong accumulated evidence from both the current outbreak as well as the previous one in West Africa.
The former Minister also warned that the “Multisectoral Ebola Response Committee would interfere with the ongoing activities of national and international health workers on the ground in North Kivu and Ituri provinces.” Part of the issue may likely have been “pressure to approve a new vaccine in addition to one that has already been used to protect more than 171,000 people.” People had warned about the potential confusion to the public as well as ethical issues if a second vaccine was used, especially one that did not have the strong accumulated evidence from both the current outbreak as well as the previous one in West Africa. CIDRAP also observed that since the resignation of the Health Minister, “DRC officials have provided no update on the outbreak, including statistics on the number of deaths, health workers infected, or suspected cases.” The last was seen on 21 July 2019.
CIDRAP also observed that since the resignation of the Health Minister, “DRC officials have provided no update on the outbreak, including statistics on the number of deaths, health workers infected, or suspected cases.” The last was seen on 21 July 2019.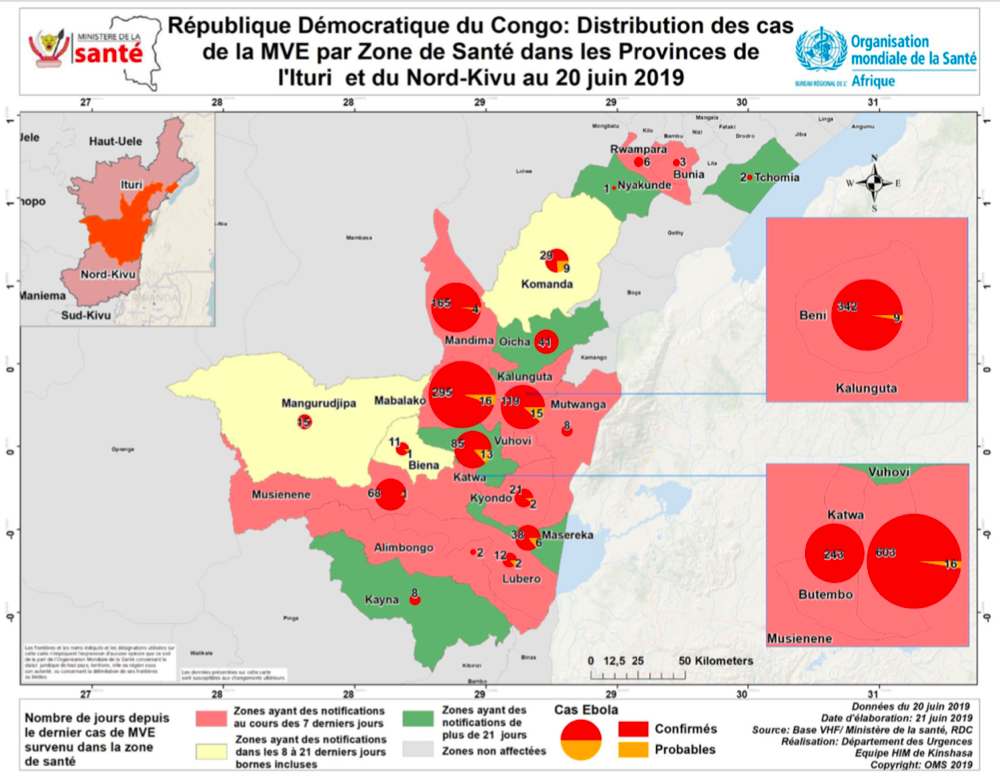 Since the major ongoing outbreak of Ebola Virus Disease in North Kivu and Ituri Provinces of the Democratic Republic of Congo (DRC) started nearly a year ago, there has been concern that the disease might spread to neighboring countries like Uganda, Rwanda, South Sudan and the Central African Republic. This fear same true recently when a family affected by Ebola crossed from DRC into Uganda to connect with relatives in Kasese District Uganda. Uganda has had many years’ experience dealing with Ebola and was able to contain the situation.
Since the major ongoing outbreak of Ebola Virus Disease in North Kivu and Ituri Provinces of the Democratic Republic of Congo (DRC) started nearly a year ago, there has been concern that the disease might spread to neighboring countries like Uganda, Rwanda, South Sudan and the Central African Republic. This fear same true recently when a family affected by Ebola crossed from DRC into Uganda to connect with relatives in Kasese District Uganda. Uganda has had many years’ experience dealing with Ebola and was able to contain the situation. The process of eliminating malaria from the world needs to start in a step-by-step fashion. WHO explained that, “Creating a malaria-free world is a bold and important public health and sustainable development goal. It is also the vision of the Global technical strategy for malaria 2016-2030, which calls for the elimination of malaria in at least 10 countries by the year 2020.”
The process of eliminating malaria from the world needs to start in a step-by-step fashion. WHO explained that, “Creating a malaria-free world is a bold and important public health and sustainable development goal. It is also the vision of the Global technical strategy for malaria 2016-2030, which calls for the elimination of malaria in at least 10 countries by the year 2020.”

 After 30 years of research and testing, a malaria vaccine is ready to go through implementation testing in Malawi, Ghana and Kenya. This pilot of the vaccine, known as RTS,S, will be made available to children up to 2 years of age with the Malawi launching first during the week of World Malaria Day.
After 30 years of research and testing, a malaria vaccine is ready to go through implementation testing in Malawi, Ghana and Kenya. This pilot of the vaccine, known as RTS,S, will be made available to children up to 2 years of age with the Malawi launching first during the week of World Malaria Day. Mass Drug Administration (MDA, also known as preventive chemotherapy) has been a successful strategy for controlling and eliminating neglected tropical diseases with special reference to onchocerciasis, lymphatic filariasis, trachoma, soil transmitted helminths and schistosomiasis. MDA use in malaria has been limited due to a number of financial and logistical challenges, not the least of which is the need to achieve high coverage over several periods of distribution. This is why WHO recommends, “Use of MDA for the elimination of P. falciparum malaria can be considered in areas approaching interruption of transmission where there is good access to treatment, effective implementation of vector control and surveillance, and a minimal risk of re-introduction of infection.”
Mass Drug Administration (MDA, also known as preventive chemotherapy) has been a successful strategy for controlling and eliminating neglected tropical diseases with special reference to onchocerciasis, lymphatic filariasis, trachoma, soil transmitted helminths and schistosomiasis. MDA use in malaria has been limited due to a number of financial and logistical challenges, not the least of which is the need to achieve high coverage over several periods of distribution. This is why WHO recommends, “Use of MDA for the elimination of P. falciparum malaria can be considered in areas approaching interruption of transmission where there is good access to treatment, effective implementation of vector control and surveillance, and a minimal risk of re-introduction of infection.”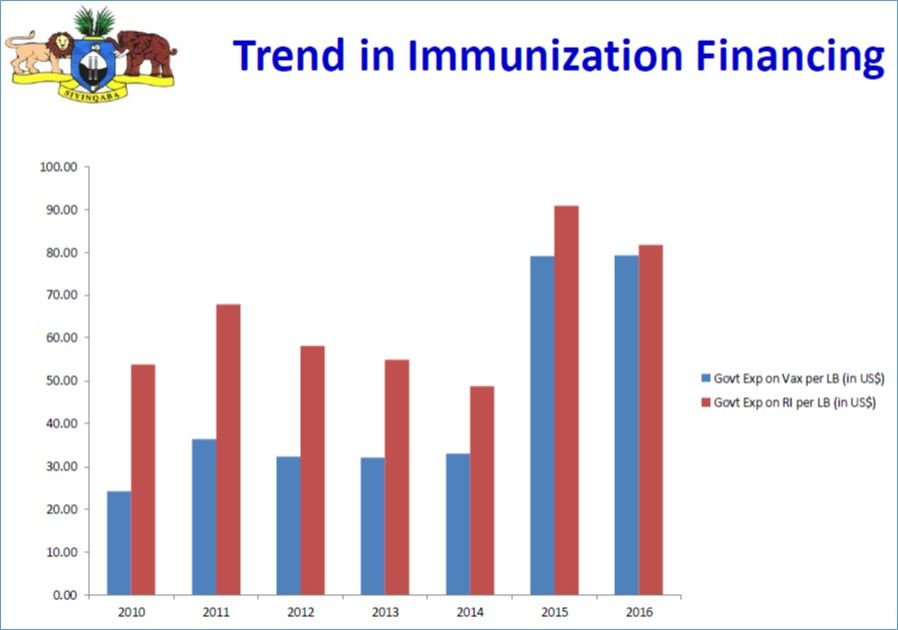 As a Lower Middle Income Country (MIC), Swaziland is not and has never been eligible to receive financial support for its immunization programs through the GAVI Alliance. Therefore, 83% of the health care budget is financed through domestic sources, and only 17% comes from from WHO and UNICEF.
As a Lower Middle Income Country (MIC), Swaziland is not and has never been eligible to receive financial support for its immunization programs through the GAVI Alliance. Therefore, 83% of the health care budget is financed through domestic sources, and only 17% comes from from WHO and UNICEF.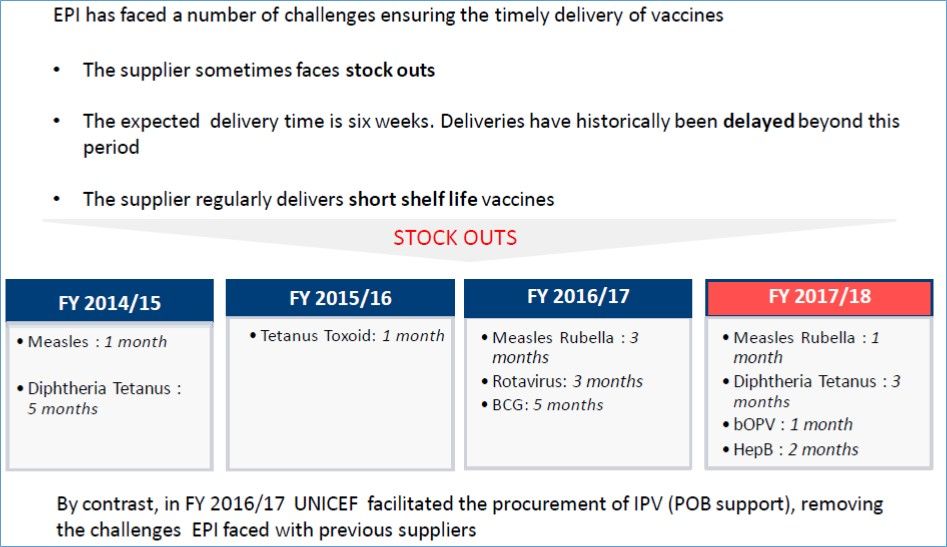 The 5 top vaccines (PCV, IPV, OPV, Rota, Penta) in Swaziland represented 98% of the total costs in 2015-16. While this is a major internal financial obligation, Vaccine procurement for the relatively small population of Swaziland represents approximately 0.2 percent of the overall African market by volume and about 0.4 percent by value. This puts smaller countries at a disadvantage in terms of getting good pricing and negotiating with suppliers.
The 5 top vaccines (PCV, IPV, OPV, Rota, Penta) in Swaziland represented 98% of the total costs in 2015-16. While this is a major internal financial obligation, Vaccine procurement for the relatively small population of Swaziland represents approximately 0.2 percent of the overall African market by volume and about 0.4 percent by value. This puts smaller countries at a disadvantage in terms of getting good pricing and negotiating with suppliers.