IPTi &Malaria in Pregnancy &Procurement Supply Management Bill Brieger | 15 Nov 2016
Improving IPTp uptake and mitigating Stock-outs in Bungoma County, Kenya
A poster entitled “Improving Pregnancy Outcomes: Alleviating Stock-Outs of Sulfadoxine-Pyrimethamine in Bungoma, Kenya” was presented by Augustine Ngindu, Gathari Ndirangu, Waqo Ejersa, David Omoit, and Mildred Mudany from Jhpiego’s Kenya Team at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
 WHO recommends intermittent preventive treatment of malaria in pregnancy using sulfadoxine pyrimethamine (IPTp-SP) to be provided at antenatal care (ANC) clinic. The Malaria Policy in Kenya requires that All pregnant women in malaria-endemic areas receive free intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine (IPTp-SP), have access to free malaria diagnosis and treatment when presenting with fever, and have access to long-lasting insecticidal nets.
WHO recommends intermittent preventive treatment of malaria in pregnancy using sulfadoxine pyrimethamine (IPTp-SP) to be provided at antenatal care (ANC) clinic. The Malaria Policy in Kenya requires that All pregnant women in malaria-endemic areas receive free intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine (IPTp-SP), have access to free malaria diagnosis and treatment when presenting with fever, and have access to long-lasting insecticidal nets.
Kenya’s Strategic Direction between 2014–2018 was revised to reflect the following:
- All pregnant women in the 14 malaria-endemic counties shall receive at least three doses of IPTp-SP
- Annual quantification of SP based on consumption to ensure adequate supplies
- Training, retraining and supervision of health care workers
- Dissemination of appropriate IPTp messages and materials
 Ministry of Health (MOH) used to procure SP until 2013 when health services were devolved to counties and procurement of became the responsibility of county governments. This presented a major challenge as counties had not factored SP in their budgets. Consequently, counties experienced SP stock-outs from October 2014. In Bungoma County the number of pregnant women receiving IPTp dropped by 51% from 7,845 in October 2014 to 3,865 in February 2015.
Ministry of Health (MOH) used to procure SP until 2013 when health services were devolved to counties and procurement of became the responsibility of county governments. This presented a major challenge as counties had not factored SP in their budgets. Consequently, counties experienced SP stock-outs from October 2014. In Bungoma County the number of pregnant women receiving IPTp dropped by 51% from 7,845 in October 2014 to 3,865 in February 2015.
To alleviate the situation (MOH) at national level requested counties to procure SP. Advocacy efforts with Bungoma County by the Maternal and Child Survival Program focused on prioritization of SP procurement at least once every quarter. As a result of this intervention, Bungoma County procured SP from February to July 2015.
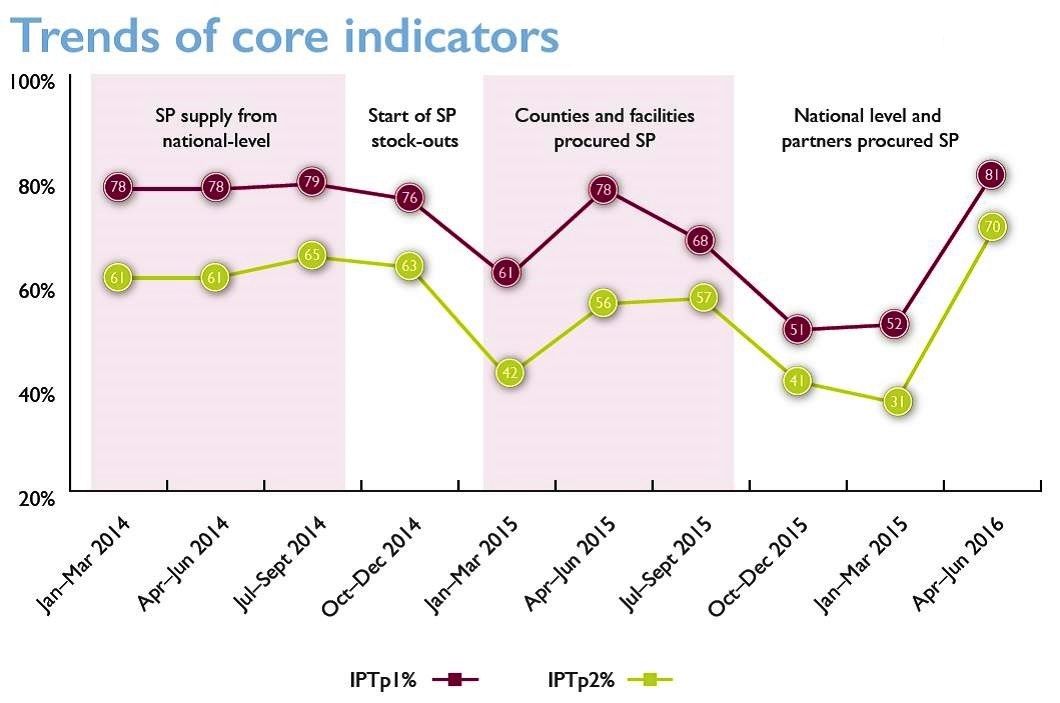 The county advised health facilities to procure additional SP doses if the supplied stocks ran out. The procurement led to a 117% increase in the number of pregnant women receiving IPTp; from 3,865 in February to 8,404 in July 2015.
The county advised health facilities to procure additional SP doses if the supplied stocks ran out. The procurement led to a 117% increase in the number of pregnant women receiving IPTp; from 3,865 in February to 8,404 in July 2015.
The fiscal year ended in June 2015 and no funds were available to procure additional SP until October 2015. This contributed to a 33% decrease in the number of pregnant women receiving IPTp from 8,404 in July to 5,672 in October 2015. As a response to support counties, MOH at national level procured 2.24 million SP doses in November/December for 14 MIP-focus counties which were received at health facilities in February 2016.
In conclusion, Bungoma County applied feasible mitigation measures including county level procurement of SP, supplemented by additional procurement at health facility and national levels. This is a practice which is replicable in other counties to ensure continued availability of SP to protect pregnant women from effects of malaria in pregnancy.
IPTp &Malaria in Pregnancy &Procurement Supply Management Bill Brieger | 11 Nov 2016
Kenya: Tackling stock-outs of medicines for intermittent preventive treatment of malaria in pregnancy
Augustine Ngindu of Jhpiego/MCSP Kenya shared with the Jhpiego Malaria Team at their pre-ASTMH 2016 Annual Meeting retreat the experience in Kenya of drug stock-outs and efforts to combat this.
 Kenya has experienced periods of Sulfadoxine-Pyrimethamine (SP) stock-outs thus threatening the coverage of intermittent preventive treatment to prevent malaria in pregnant women (IPTp). The situation has stabilized from March 2016 through efforts by Jhpiego and the USAID Maternal and Child Survival Program (MCSP) in collaboration with Kenyan health authorities and partners at national, county and facility levels.
Kenya has experienced periods of Sulfadoxine-Pyrimethamine (SP) stock-outs thus threatening the coverage of intermittent preventive treatment to prevent malaria in pregnant women (IPTp). The situation has stabilized from March 2016 through efforts by Jhpiego and the USAID Maternal and Child Survival Program (MCSP) in collaboration with Kenyan health authorities and partners at national, county and facility levels.
Jhpiego’s key interventions focused at several levels. At the national level technical assistance was provided to relevant Ministry of Health (MOH) departments (e.g. malaria, reproductive health and community strategy). In particular the situation on the ground has been used for advocacy with decision makers and managers on prioritizing procurement of SP.
At the County level Jhpiego is building capacity of counties in provision of MIP services by developing clinical mentors. Again advocacy was carried out on prioritizing inclusion of budget ite m for SP.
m for SP.
At the health facility level Jhpiego is strengthening the capacity of health facilities to provide MIP services. These activities include training of health care workers and monitoring their performance in terms of maintaining, ordering and redistribution of SP stocks. In addition Jhpiego worked with the MOH to establish malaria in pregnancy (MIP) service standards to enhance the provision of quality services in 336 facilities providing ANC services.
Then at the community level Jhpiego and partners promote MIP service utilization at community level by sensitizing pregnant women to start IPTp early in second trimester. Community health volunteers sensitize pregnant women to start IPTp early in second trimester. Hopefully increased demand will also pressure program managers to supply regular SP stocks.
Concerning the service standards, baseline data collected after immediately training found that 50% of facilities were maintaining SP stocks. A second assessment done during supportive supervision 3 months after training found 86% of facilities now met the standard. As a result of county level advocacy, redistribution of SP was done from over-stocked to under-stocked health facilities.
In conclusion, advocacy is a powerful tool in getting things done as evidenced by responses of County Directors of Health, national government and health development partners on prioritizing procurement of SP. This led to availability of adequate SP stocks to last the country up to 2019.
Community &iCCM &Procurement Supply Management &Treatment Bill Brieger | 06 Aug 2015
RSAP Themed Issue on Pharmaceutical Logistics for integrated Community Case Management (iCCM) – Call for Papers
 A themed issue for Research in Social and Administrative Pharmacy (RSAP at http://www.journals.elsevier.com/research-in-social-and-administrative-pharmacy/) will feature the challenges of guaranteeing regular and adequate pharmaceutical supplies and commodities for integrated Community Case Management (iCCM). iCCM can be described as a comprehensive approach to providing essential health services in and by the community. iCCM relies on having basic commodities like Rapid Diagnostic Tests (RDTs) and artemisinin-based combination therapy (ACT) medicines for malaria, oral rehydration solution (ORS) packets and zinc for diarrhea, in addition to appropriate antibiotics like amoxicillin and cotrimoxazole for pneumonia available in the community.
A themed issue for Research in Social and Administrative Pharmacy (RSAP at http://www.journals.elsevier.com/research-in-social-and-administrative-pharmacy/) will feature the challenges of guaranteeing regular and adequate pharmaceutical supplies and commodities for integrated Community Case Management (iCCM). iCCM can be described as a comprehensive approach to providing essential health services in and by the community. iCCM relies on having basic commodities like Rapid Diagnostic Tests (RDTs) and artemisinin-based combination therapy (ACT) medicines for malaria, oral rehydration solution (ORS) packets and zinc for diarrhea, in addition to appropriate antibiotics like amoxicillin and cotrimoxazole for pneumonia available in the community.
Early successes describing the documentation of need and initial procurement of these essential therapies in developing nations have been published; however, this themed issue will share original research, models, and expert commentaries on ensuing stages in procurement and supply chain management (PSM) that will sustain iCCM.
PSM/logistical success for iCCM can occur in countries that have a department or unit that focuses on community health promotion and supports standardized training and equipping of Community Health Workers (CHWs) even in small villages. Unfortunately, most programs lack adequate procurement and supply management systems, especially planning and forecasting. Front-line health center staff who train and supervise village-based iCCM volunteers express concern about the difficulty in acquiring enough medicines for their own clinical needs, let alone supplies for volunteer community health workers.
 Other programs reserve iCCM only for selected communities in a catchment area based on distance or availability of community health extension/auxiliary workers. There are also examples of iCCM that are narrowly focused on one or two health problems, while others take a more comprehensive approach. Clearly each has different logistical concerns such as the generic issues of forecasting, procurement, shipping and storage, while others experience the difficulty obtaining funding support when many disease control programs have vertical financial streams.
Other programs reserve iCCM only for selected communities in a catchment area based on distance or availability of community health extension/auxiliary workers. There are also examples of iCCM that are narrowly focused on one or two health problems, while others take a more comprehensive approach. Clearly each has different logistical concerns such as the generic issues of forecasting, procurement, shipping and storage, while others experience the difficulty obtaining funding support when many disease control programs have vertical financial streams.
There are various models for providing medicines at the community level. One is the pioneering work of the World Health Organization’s (WHO’s) Tropical Disease Research (TDR) program in promoting Community-Directed Treatment with Ivermectin (CDTI) for River Blindness Control, which evolved into the Community Directed Intervention (CDI) approach for delivering basic health commodities by the community, itself.[1] …
Policymakers, health organizations, and front-line clinicians often say, “no product, no program.” This themed issue will share the experiences and lessons of iCCM, both successes and challenges, to help the global health community see the need for more systematic planning of PSM for iCCM. International agencies and donors clearly recognize that alternative forms of essential health service delivery are needed to achieve coverage targets and save lives. The community as a source of care has a solid foundation as established at the International Conference on Primary Health Care, which produced global guidance through the Alma Ata Primary Health Care Declaration of 1978,[2] but in all those years, actualization of this ideal has been difficult for logistical reasons. This RSAP themed issue should not only help us understand the present challenges, but map a way forward to better access to essential health commodities in communities throughout the developing world.
The themed issue will include various contributions such as:
- Commentary/Overview from the World Health Organization staff who have spearheaded the iCCM movement
- Implementation/intervention research on:
- The link between front-line clinics and community health workers/distributors in guaranteeing iCCM commodities
- The challenge of providing iCCM commodities for use by nomadic populations
- Provision of iCCM commodities by different types community workers
- Successes and challenges in maintaining supplies and commodities for large-scale and national community primary health care programs
- Comparative lessons from other community based programs such as family planning commodity distribution and home-based care for people living with HIV
- Documented program experiences including:
- The challenges of maintaining iCCM supplies and logistics in emergency situations, as with disaster refugee and outbreak situations
- The role of donors and non-governmental organizations (NGOs) in providing commodities.
We are still seeking additional contributions. If you have a paper or idea for one or more, please contact the guest editors. Papers must be submitted on the Elsevier RSAP platform at http://ees.elsevier.com/rsap/ by February 1, 2016 for publication in fall of 2016.
Guest Editors:
- William R Brieger, MPH, DrPH, Professor, Department of International Health, Bloomberg School of Public health, The Johns Hopkins University; Senior Malaria Specialist, Jhpiego; RSAP Editorial Board Member. <bbbrieger@yahoo.com>
- Maria KL Eng, MPH, PhD, Departmental Associate, Department of International Health, Bloomberg School of Public health, The Johns Hopkins University; Instructor for “Pharmaceuticals Management for Under-Served Populations” <meng@jhu.edu>
[1] http://www.who.int/bulletin/volumes/88/7/09-069203/en/
[2] http://www.who.int/dg/20080915/en/
Private Sector &Procurement Supply Management &Treatment Bill Brieger | 05 Oct 2014
Licensed chemical sellers and antimalarial prices in northern Ghana under the affordable medicines facility
The recently concluded Global Health Systems Research Symposium in Cape Town featured a number of abstracts that touched directly or indirectly on malaria. Malaria services and movement toward malaria elimination cannot be achieved in a country without a strong health system that involves both communities, program staff and policy maker s.
s.
Below is an abstract by Heather Lanthorn of the Harvard School of Public Health on the AMFm program testing in Ghana. Other abstracts will appear subsequently.
“The Affordable Medicines Facility – malaria (AMFm) represents an important experiment in using private retail chains to improve access to medicines in low- and middle-income countries. AMFm aimed to make quality-assured artemisinin-based combination therapies (QA.ACTs) accessible at the variety of outlets where citizens treat fevers. In Ghana, where ACTs are legally sold over the counter, Licensed Chemical Sellers (LCS) are a key antimalarial provider.
“I use a framework adapted from industrial organization to study a unique, geo-coded data set of 250 LCSs in and around Tamale, Ghana collected explicitly for this study. Through well-integrated quantitative (multiple logistic regression) and qualitative (open thematic analysis) approaches, I analyze: the experiences of LCSs with AMFm; LCS reported compliance with recommended retail prices (RRPs); LCS economic and social explanations for compliance; and associations between LCS objective characteristics – including geo-location – and RRP compliance.
“We find high stocking of subsidized QA.ACTs and high RRP compliance. 18% of LCSs report selling above the RRP. The majority of non-compliers cite rising prices from their supplier as the major determinant of their own pricing. The majority of non-compliers sold at USD 1.5 rather than the RRP, USD 1.0. Indeed, in the quantitative analysis, RRP compliance is most clearly associated with the distributor prices and with LCS reputation (years in business).
 “A driving motivation for experimentally piloting AMFm was to learn whether the QA.ACT subsidy would be passed on to end-line private retailers and, in turn, to consumers. We find that, largely, it is. By considering LCSs both as economic agents and community members, the present analyses accord with, complement and innovate on the large, independent evaluation of AMFm, which focused on prices but neither objective nor perceptual explanations for price-compliance.”
“A driving motivation for experimentally piloting AMFm was to learn whether the QA.ACT subsidy would be passed on to end-line private retailers and, in turn, to consumers. We find that, largely, it is. By considering LCSs both as economic agents and community members, the present analyses accord with, complement and innovate on the large, independent evaluation of AMFm, which focused on prices but neither objective nor perceptual explanations for price-compliance.”
Advocacy &Funding &Health Systems &Procurement Supply Management &Universal Coverage Bill Brieger | 25 Apr 2013
Appreciating Many Years of Malaria Partnerships and Investment
 While today it technically the sixth World Malaria Day, one should actually trace the origins back 13 years to the first Africa Malaria Day (AMD) in 2001, held to encourage progress based on the Africa malaria Summit in Abuja just one year before. And since the Abuja summit and its resulting declaration were backed by the Roll Back Malaria Partnership, which formed in 1998, one could say the world has 15 years to considering in judging progress in and plans for partner investments in ridding the world of malaria.
While today it technically the sixth World Malaria Day, one should actually trace the origins back 13 years to the first Africa Malaria Day (AMD) in 2001, held to encourage progress based on the Africa malaria Summit in Abuja just one year before. And since the Abuja summit and its resulting declaration were backed by the Roll Back Malaria Partnership, which formed in 1998, one could say the world has 15 years to considering in judging progress in and plans for partner investments in ridding the world of malaria.
In 2001 organizers of Malaria Day events were encouraged to feature a ‘new’ medicine that WHO said could save 100,000 child healths annually in Africa. artimisinin-based combination therapy (ACT) drugs are now the front line treatment in most all endemic countries, and deaths have declined somewhat on the order of 400,000. At that time there was only one major manufacturer of ACTs. Investments by pharmaceutical companies in generic ACTs now means that there are at least nine companies that produce prequalified ACTs. What is needed is more indigenous African pharmaceutical companies approved to invest in ACT production.
![]() The first AMD stressed the risk of malaria to pregnant women and recommended widespread use of Intermittent Preventive Treatment in pregnancy (IPTp). This recommendation has been adopted in countries with stable falciparum malaria transmission, but has lagged in terms of implementation, and coverage still lags below the 80% target set at the 2000 Abuja Summit. There are missed opportunities to provide IPTp at antenatal clinics due to stock-outs, provider attitudes, and client beliefs. Weak health information systems mean that even when services are provided, reporting may not accurately reflect true coverage of IPTp.
The first AMD stressed the risk of malaria to pregnant women and recommended widespread use of Intermittent Preventive Treatment in pregnancy (IPTp). This recommendation has been adopted in countries with stable falciparum malaria transmission, but has lagged in terms of implementation, and coverage still lags below the 80% target set at the 2000 Abuja Summit. There are missed opportunities to provide IPTp at antenatal clinics due to stock-outs, provider attitudes, and client beliefs. Weak health information systems mean that even when services are provided, reporting may not accurately reflect true coverage of IPTp.
In the meantime resistance is growing to sulphadoxine-pyrimethamine (SP), the drug used for IPTp in part due to the inability or unwillingness of country drug authorities to curb its inappropriate use for case management. WHO now recommends more that the original two IPTp doses and suggests that pregnant women get SP at each ANC visit after quickening. In the meantime research is underway to find substitutes for SP.
The first AMD addressed the role of insecticide treated nets (ITNs) in helping halve the world’s malaria burden by 2010. Major progress came in 2008 when the whole United Nations community and of course companies invested in net production got behind universal coverage. In addition the advent of the long lasting insecticide-treated net with insecticide infused in the fabric from point of production pointed the way to success.
These three core interventions – ACTs, IPTp and ITNs – have been strengthened with better diagnostics and a variety of other vector control measures, Hopes for a vaccine still remain a dream, though an achievable one. While we have high expectations for eradication, we can see that some of the health systems challenges that thwarted the first malaria eradication effort are still with us including weak procurement and supply management, inadequate human resources and gaps in health information systems.
The foregoing implies that we need at least two forms of future investment in malaria. First is investment by governments in strengthening the health system that deliver malaria services. The second investment is in continued biomedical research in order to fend off resistance by mosquitoes and parasites and of course social research to address issues of behavior, adoption of innovations and program management practices. Let’s hope that when World Malaria Day 2014 rolls around, we can measure these increases investments.
Funding &Procurement Supply Management &Treatment Bill Brieger | 21 May 2012
Stock-outs: how can we achieve malaria treatment goals?
Of twenty-two malaria endemic countries in Africa that receive support from both USAID/PMI and the Global Fund, eleven reported gaps in malaria medicine funding in the 2011 Road Maps countries prepare for Roll Back Malaria. Likewise, 16 of these countries reported gaps in RDT financing and supplies.
 These stock and procurement problems arise from many causes including ability to forecast need, poor donor coordination and leadership, and lack of adherence to new guidelines that require diagnostic verification of malaria before treatment among others. We are well past the 2010 RBM target date to achieve 80% treatment coverage, but the most recent DHS and MIS results from the 22 countries for appropriate treatment of children below five years of age show that the country with the highest achievement of ACT coverage in this age group was Malawi with only 36.2%. The median among these 22 countries was 16.5%.
These stock and procurement problems arise from many causes including ability to forecast need, poor donor coordination and leadership, and lack of adherence to new guidelines that require diagnostic verification of malaria before treatment among others. We are well past the 2010 RBM target date to achieve 80% treatment coverage, but the most recent DHS and MIS results from the 22 countries for appropriate treatment of children below five years of age show that the country with the highest achievement of ACT coverage in this age group was Malawi with only 36.2%. The median among these 22 countries was 16.5%.
Therefore, it was not surprising that The Citizen newspaper reported from Dar es Salaam that, “Thousands of Tanzanians have continued to die from malaria annually due to lack of medicines despite massive investment by the government and donors towards improved supply of relevant drugs in health facilities.” Apparently programs like SMS for Life and AMFm have not had their desired effects.
The Citizen lamented that, “Phone calls to the CEO of Medical Stores Department (MSD), which is charged with responsibility of distributing drugs in the country, went unanswered.” Other malaria implementation partners gave their own views that the problem was due to lack of professionalism among health officials and a lack of commitment to implementing the malaria program.
If we cannot even achieve malaria treatment targets by 2010, what hope do we have of reducing mortality by 2015 – let alone head toward elimination? Technical assistance may be needed, but cannot succeed if there is a lack of will on the part of program implementation partners from the endemic countries.
Communication &Monitoring &Procurement Supply Management Bill Brieger | 24 Jul 2011
Malaria and Mobiles – Hacking or Helping
Surprise – the latest in the Rupert Murdoch scandal concerns malaria. Yesterday Metro Online headlined a story: “Cheryl Cole’s ‘phone hacked while she was suffering from malaria.'” The claims are still at the level of rumors, and thus investigators are still “looking into claims that her voicemails were hacked while she was hospitalised.”
A year ago when Ms Cole’s bout with malaria hit the news, The News of the World was mentioned as a source. One online posting noted that Ms Cole, “is believed to have lost half a stone during her battle with malaria. A source told the News of the World that the Girls Aloud beauty is now just over 7 stone. The insider told the newspaper that medics have said that it could be six months before Cole is allowed to perform her strenuous dance routines.”
Similarly another website reported last year that, “A source told the News of the World: “We nearly lost her and the battle is far from over. She is so weak and this horrible illness has taken complete hold of her. ‘It got so bad she was literally only hours from death’s door. Thank goodness she was diagnosed in time.'”
 Now a year later MTV UK published that, “Cheryl’s lawyers are investigating claims by a former News of the World journalist, who stated that the Geordie’s voicemails were listened to “while she underwent treatment for malaria.”
Now a year later MTV UK published that, “Cheryl’s lawyers are investigating claims by a former News of the World journalist, who stated that the Geordie’s voicemails were listened to “while she underwent treatment for malaria.”
Fortunately most use of mobile phone technology these days helps promote malaria control and elimination. In Nigeria for example, mobile phone SMS has been used to track bednet distribution. A UNICEF spokesperson who is involved in promoting such innovations explained that …
In Africa, we are finding there are systemic failures in public health and supply in terms of getting reliable information quickly from the field. Ninety percent of the developing world has access to a cell phone, so we’re experimenting with the use of instant messaging to make a difference. We’re finding that we can train people in villages to be data collectors and help us by using cell phones to text information to central authorities; we and governments can then respond faster to specific needs. In some places, it takes months just to get a piece of paper from the field. Mobile phones and SMS technology can help surmount that hurdle.
Recently the Business Standard reported that, “The University of Glasgow has received a grant from the Bill & Melinda Gates Foundation to further help in the diagnosis of malaria. The $100,000 award would go towards developing a device which uses mobile-phone derived technology to detect and separate red blood cells infected with malaria parasites.”
A study by Caroline Asiimwe and colleagues in Uganda has shown SMS improves the timeliness in reporting of specific, time-sensitive information on RDT positivity rates and ACT stockouts at modest cost, while by-passing current bottlenecks in the flow of data. Likewise in Tanzania “A multinational computer, technology and IT consulting company, IBM, in partnership with Novartis and Vodafone, together with Roll Back Malaria and Tanzania’s Ministry of Health and Social Welfare have reaped from the technology dubbed ‘SMS for Life’. The system tracks movement and the supply of anti-malaria drugs in sub-Saharan Africa.”
People have argued that technology itself is ethically neutral – it is how people use it that has ethical ramifications. In the case of malaria hopefully we will see more uses that help save lives instead of illegally spying on and disrupting them.
Burden &Procurement Supply Management Bill Brieger | 26 May 2011
Population Growth and Malaria Elimination
A major challenge in successful malaria control programming is correctly estimating the numbers of commodities needed and ensuring their timely delivery. It is not clear the extent to which this forecasting process accounts for population growth.
Therefore, when the International Herald Tribune (IHT) reports on population growth in the region with the heaviest burden of malaria, we take notice … “What is most striking, though, is the unabated demographic swelling of Africa. Africa’s population has almost doubled between 1975 and 2000, growing from 416 to 811 million; it will add another 75 percent to reach 1.4 billion people in 2025, and presumably another 55 percent to reach the staggering figure of 2.2 billion by mid-century.”
 One wonders whether successful efforts to reach 2015 targets of reduced malaria morbidity and mortality might offset the need for more and more LLINs, ACTs and other commodities? In some countries moving close to elimination, this might be true, but the high burden countries – high because of their large populations and challenging logistics – remain a concern. As the IHT observed, “countries such as Nigeria (230 million in 2025, 390 million in 2050); Ethiopia (110 million and 145 million) and Congo (95 million and 148 million) have since long been identified as the demographic giants of sub-Saharan Africa.”
One wonders whether successful efforts to reach 2015 targets of reduced malaria morbidity and mortality might offset the need for more and more LLINs, ACTs and other commodities? In some countries moving close to elimination, this might be true, but the high burden countries – high because of their large populations and challenging logistics – remain a concern. As the IHT observed, “countries such as Nigeria (230 million in 2025, 390 million in 2050); Ethiopia (110 million and 145 million) and Congo (95 million and 148 million) have since long been identified as the demographic giants of sub-Saharan Africa.”
We already know that universal coverage was not achieved by 31 December 2010 as many endemic countries are still sourcing and distributing nets and other commodities in the hopes of reaching the target in 2011. All the while, population does not remain static.
We also know that there has been strong competition for nets and drugs among endemic countries because of the low number of manufacturers of approved products. A lesson from the field is that rapid diagnostic test supplies are not close to catching up with supplies of artemisinin-based combination therapy (ACT) medicines, and long lasting insecticide treated nets (LLINs) are not as long lasting as once thought. Will we be able to get enough nets in 2013-14 to replace those distributed in 2010-11?
So in the short run as population increases, need for malaria control commodities will also increase. And, one wonders can donor support be counted on?
Ironically even as fertility decreases (though is still high), population grows because of the success in disease control programs and reduced mortality. Also as UNFPA explains, the fact that the majority of people in developing countries are young means that the bulk of the population still has many years of reproductive life ahead, hence population in the foreseeable future will increase even if fertility of lower.
Of course, even when people survive malaria episodes they experience personal costs that holds back the national economy. The question is whether we can get enough malaria commodities on the scene and in people’s hands before population doubles?
Procurement Supply Management &Universal Coverage Bill Brieger | 15 May 2011
Redrawing Roadmaps – can we get there from here?
The Roll Back Malaria Partnership guided countries to develop 2010 roadmaps for major malaria commodity and support service availability and gaps. The aim was to aid planning to reach universal coverage by the end of 2010. Forty-seven countries/locations on the African Continent and surrounding islands completed the analysis and started moving down the road to success.
In the case of 36 countries the road became a little longer than anticipated. Part of the challenge was international – there are only a few manufacturers of long lasting insecticide-treated nets, for example. Some of the barriers were internal, inadequate estimates of the logistical costs to distribute commodities, even if they were in hand. Now we have 2011 roadmaps in an effort to meet up with the original 2010 goals of 80% coverage with essential malaria commodities.
 At least one-quarter of countries that actually targeted a specific intervention in 2010, did not meet the 80% goals. Of particular concern is the fact that Rapid Diagnostic test use is both off target and not keeping up with ACTs.
At least one-quarter of countries that actually targeted a specific intervention in 2010, did not meet the 80% goals. Of particular concern is the fact that Rapid Diagnostic test use is both off target and not keeping up with ACTs.
Meeting procurement and distribution targets is one step, but getting people to use malaria control interventions is another challenge. As the director of a prominent Nigerian NGO recently said, “… ‘though about 35.6 million nets have been distributed across the country, it is highly under utilized,’ which according to him is responsible for the high death rate associated with malaria.”
Nigeria provides an instructive case. The roadmap for 2010 called for 62.9m LLINs of which 4.4m were already in place and pledges were set for 49.4m. This left a gap of 9.2m. While the RBM 2010 roadmap analysis shows that Nigeria met its LLIN target, the implication is that the target did not include the gap. Now the 2011 roadmap for Nigeria now shows that resources are in hand for both the 9.2m gap from the 2010 campaign plus an additional 8.2 m for routine distribution in clinics as a keep-up measure.
The gross figures do not fully reflect the fact that of the 36 states (plus one capital territory), campaign distribution of LLINs continued from 2010 into 2011 in 17 states. So far 9 or the 17 have completed distribution, but by carrying the campaign into 2011 additional delays were met in the remainder due to national elections, delayed local funding for the effort, and distribution logistics. So again while the roadmaps help identify commodity gaps, they do not always identify the challenges at the level of distribution and use.
The roadmap process is an important planning tool. It needs to be supplemented with plans for logistical support and health education to encourage use of the malaria commodities and services that are eventually distributed. For example, Nigeria estimates that it needs close to $17m for Monitoring and Evaluation and Information. Education and Communication. We can see from the Nigerian roadmaps that this planning needs to be a continuous process – not only is annual resupply of ACTs, RDTs and SP for IPTp needed, but also continuous stocks of nets for routine, keep-up services.
Malaria in Pregnancy &Procurement Supply Management Bill Brieger | 14 Dec 2010
SP Stock-Outs – What’s the Problem?
 In today’s guest report, Michelle Wallon from Jhpiego’s Zambia office discusses the challenges of maintaining stocks of sulphadoxine-pyrimethamine (SP) for use in Intermittent Preventive Treatment for pregnant women (IPTp) that arose during recent Roll Back Malaria meetings in Livingstone and Lusaka:
In today’s guest report, Michelle Wallon from Jhpiego’s Zambia office discusses the challenges of maintaining stocks of sulphadoxine-pyrimethamine (SP) for use in Intermittent Preventive Treatment for pregnant women (IPTp) that arose during recent Roll Back Malaria meetings in Livingstone and Lusaka:
The effects of malaria in pregnancy are many and the interventions, simple. Intermittent Preventive Treatment (IPTp), insecticide-treated bed nets, and timely case management can reduce effects including maternal anemia, low birth weight, and maternal and fetal mortality. Yet, when speaking to clinicians and public health experts across Africa about prevention and control of malaria in pregnancy (MIP), there is a common theme – stock-outs of SP, the drug used for IPTp, commonly inhibit the effectiveness of MIP interventions.
IPTp is relatively straight-forward and SP, is an inexpensive drug. Furthermore, at the time that the IPTp recommendations were adopted via the Abuja Declaration in 2000, many countries were still procuring SP as the first-line treatment for the general population (For example, Nigeria did not officially switch to ACTs as firstline malaria drugs until 2005).
SP supplies were abundant when it was still recommended as treatment. What then is the problem now?
Although SP stock-outs are formally documented in only a few African countries, including Zambia, Tanzania, and Malawi, the problem can be inferred by most of the recent Demographic and Health Survey and Malaria Indicator Survey reports (e.g. Liberia, Nigeria, Uganda, Senegal) showing low coverage of the recommended two doses of IPTp. MIP experts readily and repeatedly identify a handful of culprits for the SP stock-out phenomenon.
- Provider mistrust of RDTs coupled with policies that ACTs be provided only after positive diagnosis via RDT or microscopy
- Real or perceived high incidences of malaria
- Strong correlation in the community between fever and malaria with high expectations for malaria treatment
- Weak clinical skills in the appropriate diagnosis and management of fever
- Lack of skilled providers and high client loads
Inaccurate SP quantification based on population rather than consumption data and/or quantification failing to account for irrational use also create stock problems. Weak logistics systems with bottlenecks between central-level drug stores and receiving facilities result in stock-outs of both SP and ACTs.
These problems are not new and neither are the solutions. MIP has a potential advantage in that it falls under both reproductive health and national malaria control programs, and yet the persistence of SP stock-outs indicates that this is often used less as an opportunity for collaboration than as an excuse to pass the buck.
As the public health community moves towards more integrated programming, we must seize the opportunity to bridge the programmatic gap.