Community &Private Sector &Treatment Bill Brieger | 03 Nov 2014
Ghana at ASTMH: Mapping out of antimalarial drugs on stock at the market in a rural districts of Ghana
The first Poster Session of the American Society of Tropical Medicine and Hygiene (Monday noon) will feature a study on availability of malaria medicines in rural Ghana. “Mapping out of antimalarial drugs on stock at the market in a rural districts of Ghana” was developed by Alexander A. Nartey, Evelyn K. Ansah, Patricia Akweongo, Gloria A. Nartey, Mary A. Pomaa, Doris Sarpong, Clement Narh, and Margaret Gyapong of the Dodowa Health Research Centre.
American Society of Tropical Medicine and Hygiene (Monday noon) will feature a study on availability of malaria medicines in rural Ghana. “Mapping out of antimalarial drugs on stock at the market in a rural districts of Ghana” was developed by Alexander A. Nartey, Evelyn K. Ansah, Patricia Akweongo, Gloria A. Nartey, Mary A. Pomaa, Doris Sarpong, Clement Narh, and Margaret Gyapong of the Dodowa Health Research Centre.
 Antimalarial drugs are a very important component of any policy for effective reduction of morbidity and mortality related to the malaria disease. The availability of efficacious and high quality antimalarials and their correct use can mitigate the risk of morbidity and mortality among the people of sub-Saharan Africa who have the highest risk of contracting and dying
Antimalarial drugs are a very important component of any policy for effective reduction of morbidity and mortality related to the malaria disease. The availability of efficacious and high quality antimalarials and their correct use can mitigate the risk of morbidity and mortality among the people of sub-Saharan Africa who have the highest risk of contracting and dying
from malaria.
Chemical (medicine) shops are major source of care for most developing countries where anti-malarial drugs can be purchase at the counter. The paper seeks to identify the different kinds of anti-malarial drugs on the market for malaria treatment in a rural district in Ghana.
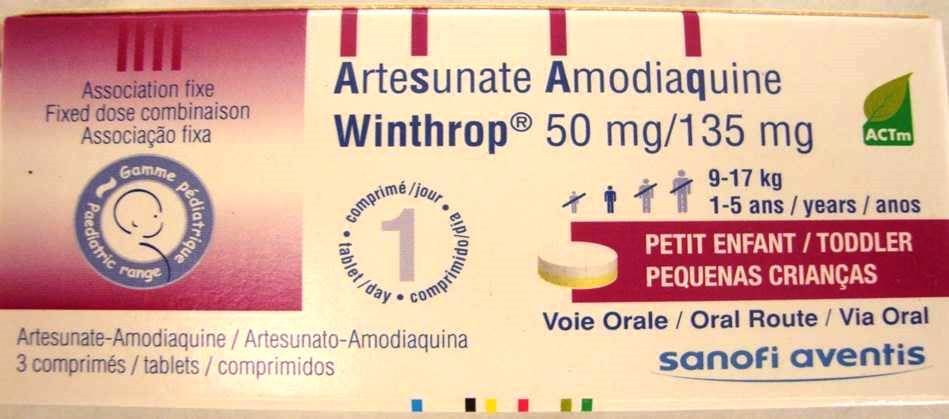
 A structured questionnaire was used during two seasons (peak and low malaria transmission seasons) to collect information on anti-malarial drugs from all 58 chemical shops within the Dangme West district now (Shai Osudoku and Ningo Prampram districts). Pictures of the anti-malarial drugs were taken,
A structured questionnaire was used during two seasons (peak and low malaria transmission seasons) to collect information on anti-malarial drugs from all 58 chemical shops within the Dangme West district now (Shai Osudoku and Ningo Prampram districts). Pictures of the anti-malarial drugs were taken,
The active ingredients, and also the source of the drugs documented. GIS locations of the shops were also recorded to ascertain the proximity of the shops to households in the communities. Majority (72.0%) of the chemical and pharmacy shop owners are males. Only 7.0% of the shops are pharmacy while the remainder is licensed chemical shops.
 The total numbers of antimalarial drugs counted were forty nine (49). Among the stock, 4.2% were quinine, 31.9% of them were monotherapies such as artemether, Amodiaquine, Artesunate etc. Altogether, 59.4% of the artemisinin combination therapies (ACTs) were artemether + Lumefantrine, 25.0% were Artesunate + Amodiaquine.
The total numbers of antimalarial drugs counted were forty nine (49). Among the stock, 4.2% were quinine, 31.9% of them were monotherapies such as artemether, Amodiaquine, Artesunate etc. Altogether, 59.4% of the artemisinin combination therapies (ACTs) were artemether + Lumefantrine, 25.0% were Artesunate + Amodiaquine.
Other antimalarials observed were 9.4% Sulfadoxine + Pyrimethamine and 3.1% of of Artesunate + Sulfamethoxypyrazine + Pyrimethamine. About 47% of the anti-malarial drugs were pediatric formulations.
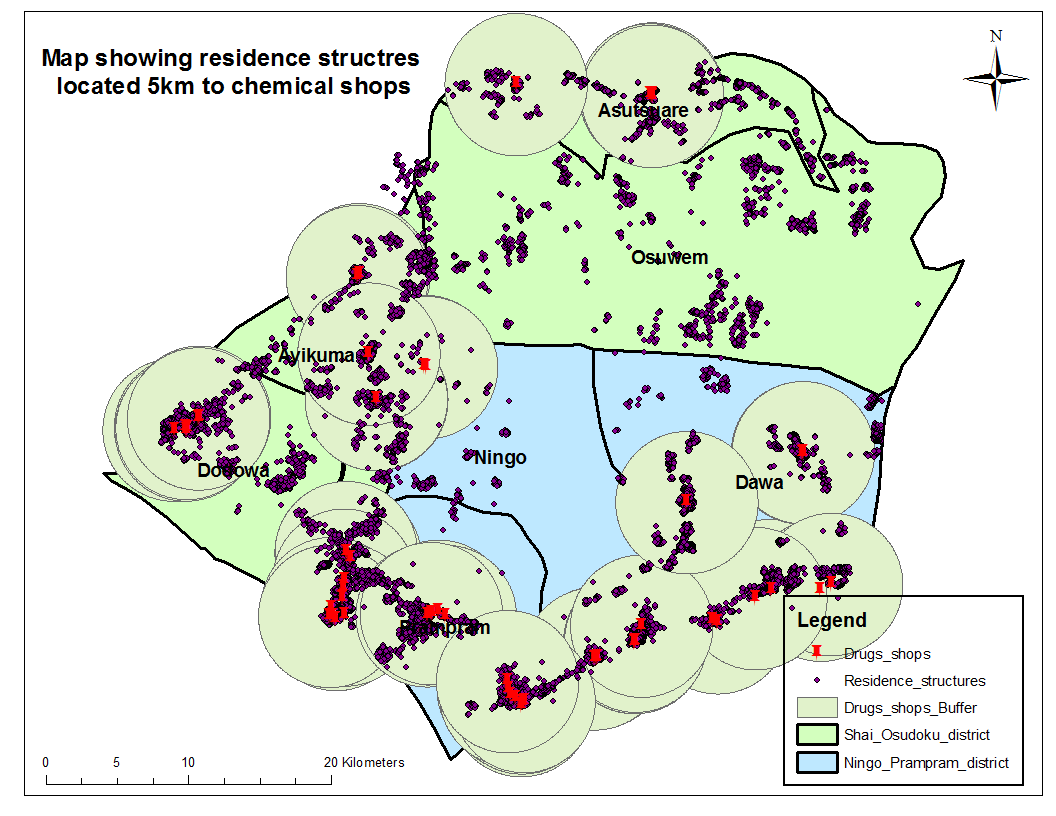 GIS mapping shows that majority of the households are within a periphery of 5km to a chemical shop.
GIS mapping shows that majority of the households are within a periphery of 5km to a chemical shop.
The national antimalarial drug policy recommends the use of ACTs for malaria treatment however; all sorts of anti-malarial drugs which are not ACTs are in stock at the chemical shops in Ghana. Chemical shops are closer to households and play a very important role in the treatment of malaria hence there is the need to train chemical sellers to stock and administer the recommended antimalarials.
Community &Drug Quality &Private Sector &Treatment Bill Brieger | 08 Oct 2014
Registered drug shops are preferred for treating acute febrile illness in rural Uganda
The recently concluded Global Health Systems Research Symposium in Cape Town featured a number of abstracts that touched directly or indirectly on malaria. Malaria services and movement toward malaria elimination cannot be achieved in a country without a strong health system that involves both communities, program staff and policy makers.
 Below is an abstract by Freddy Kitutu, Chrispus Mayora, Phyllis Awor, Forsberg Birger, Stefan Peterson, and Henry Wamani of Makerere University and the Karolinska Institute on use of medicine shops in Uganda.
Below is an abstract by Freddy Kitutu, Chrispus Mayora, Phyllis Awor, Forsberg Birger, Stefan Peterson, and Henry Wamani of Makerere University and the Karolinska Institute on use of medicine shops in Uganda.
“Under-five child mortality in Uganda is still high and majority is caused by easily treatable pneumonia, malaria and diarrhoeal diseases among the poorest people. One of the reasons for these deaths is the lack of timely access to proven life saving medicines. This hinders progress towards attainment of MDG 4 target by 2015.
“To increase access to quality medicines and diagnostics for child febrile illnesses, Makerere University School of Public Health (MakSPH) in collaboration with WHO Alliance for Health Policy and Systems Research, is doing a project to assess the potential to deliver quality integrated care for malaria, pneumonia and diarrhoea using integrated community case management (iCCM) strategies and tools. Hence, an assessment was conducted to determine baseline care seeking preferences.
“A baseline household survey interviewed caregivers of children under-five years. The study protocol and data collection tools had been reviewed and approved by Research and Ethics Committees at WHO, MakSPH and Uganda National Council of Science and Technology.
“A total of 2606 households were surveyed. The main childhood diseases reported included fever (70%), cough (77%), and diarrhoea (40%) convulsions (16%) Most households use private drug shops to purchase medicines to manage these illnesses. Use of drug shops was attributed to long distances to public health facilities, availability and reliability of drug stocks at drug shops, perceived high quality of services, and options for credit.
“Interventions that target public health facilities are likely to miss many healthcare seekers especially the poor in rural distant areas. Conclusion: Drug shops are the convenient and preferred outlets for rural poor communities, and therefore need to be included in interventions such as iCCM strategy.
“Significance for the selected field-building dimension: This abstract presents findings from the baseline assessment prior to introducing a health system intervention in drug shops to improve access to and quality of care for under-five children.”
Private Sector &Procurement Supply Management &Treatment Bill Brieger | 05 Oct 2014
Licensed chemical sellers and antimalarial prices in northern Ghana under the affordable medicines facility
The recently concluded Global Health Systems Research Symposium in Cape Town featured a number of abstracts that touched directly or indirectly on malaria. Malaria services and movement toward malaria elimination cannot be achieved in a country without a strong health system that involves both communities, program staff and policy makers.
Below is an abstract by Heather Lanthorn of the Harvard School of Public Health on the AMFm program testing in Ghana. Other abstracts will appear subsequently.
“The Affordable Medicines Facility – malaria (AMFm) represents an important experiment in using private retail chains to improve access to medicines in low- and middle-income countries. AMFm aimed to make quality-assured artemisinin-based combination therapies (QA.ACTs) accessible at the variety of outlets where citizens treat fevers. In Ghana, where ACTs are legally sold over the counter, Licensed Chemical Sellers (LCS) are a key antimalarial provider.
“I use a framework adapted from industrial organization to study a unique, geo-coded data set of 250 LCSs in and around Tamale, Ghana collected explicitly for this study. Through well-integrated quantitative (multiple logistic regression) and qualitative (open thematic analysis) approaches, I analyze: the experiences of LCSs with AMFm; LCS reported compliance with recommended retail prices (RRPs); LCS economic and social explanations for compliance; and associations between LCS objective characteristics – including geo-location – and RRP compliance.
“We find high stocking of subsidized QA.ACTs and high RRP compliance. 18% of LCSs report selling above the RRP. The majority of non-compliers cite rising prices from their supplier as the major determinant of their own pricing. The majority of non-compliers sold at USD 1.5 rather than the RRP, USD 1.0. Indeed, in the quantitative analysis, RRP compliance is most clearly associated with the distributor prices and with LCS reputation (years in business).
 “A driving motivation for experimentally piloting AMFm was to learn whether the QA.ACT subsidy would be passed on to end-line private retailers and, in turn, to consumers. We find that, largely, it is. By considering LCSs both as economic agents and community members, the present analyses accord with, complement and innovate on the large, independent evaluation of AMFm, which focused on prices but neither objective nor perceptual explanations for price-compliance.”
“A driving motivation for experimentally piloting AMFm was to learn whether the QA.ACT subsidy would be passed on to end-line private retailers and, in turn, to consumers. We find that, largely, it is. By considering LCSs both as economic agents and community members, the present analyses accord with, complement and innovate on the large, independent evaluation of AMFm, which focused on prices but neither objective nor perceptual explanations for price-compliance.”
Advocacy &Coordination &Partnership &Private Sector Bill Brieger | 11 Sep 2014
UN General Assembly Resolves to Fight Malaria
 GhanaWeb reported this morning that, “The United Nations General Assembly at its 68th Session, adopted Resolution A/68/L.60, “Consolidating Gains and Accelerating Efforts to Control and Eliminate Malaria in Developing Countries, Particularly in Africa, by 2015” by consensus.”
GhanaWeb reported this morning that, “The United Nations General Assembly at its 68th Session, adopted Resolution A/68/L.60, “Consolidating Gains and Accelerating Efforts to Control and Eliminate Malaria in Developing Countries, Particularly in Africa, by 2015” by consensus.”
Likewise the UN itself issued a press release confirming that in a final act the Assembly adopted this resolution in order to call for increased support for the implementation of international commitments and goals pertaining to the fight to eliminate malaria. GhanaWeb reiterated the UN’s message that, “with just less than 500 days until the 2015 deadline of the MDGs, the adoption of this resolution by the General Assembly reiterates the commitment of UN Member States to keep malaria high on the international development agenda.”
The UN Press Release explained that, “The resolution urged malaria-endemic countries to work towards financial sustainability to increase national resources allocated to controlling that disease, while also working with the private sector to improve access to quality medical services. Further, the resolution called upon Member States to establish or strengthen national policies, operational plans and research, with a view to achieving internationally agreed malaria targets for 2015.”
 This effort is consistent with moves two years ago in the 66th General Assembly when it called for “accelerated efforts to eliminate malaria in developing countries, particularly Africa, by 2015, in consensus resolution” (document A/66/L.58) where the “Consolidating Gains …” document was first shared. The draft of the 2012 resolution, according to the UN Press release was sponsored by Liberia on behalf of the African Group, and called on Member States, particularly malaria-endemic countries, to strengthen national policies and operational plans, with a view to scaling up efforts to achieve internationally agreed malaria targets for 2015.
This effort is consistent with moves two years ago in the 66th General Assembly when it called for “accelerated efforts to eliminate malaria in developing countries, particularly Africa, by 2015, in consensus resolution” (document A/66/L.58) where the “Consolidating Gains …” document was first shared. The draft of the 2012 resolution, according to the UN Press release was sponsored by Liberia on behalf of the African Group, and called on Member States, particularly malaria-endemic countries, to strengthen national policies and operational plans, with a view to scaling up efforts to achieve internationally agreed malaria targets for 2015.
The sad irony of Liberia’s current predicament wherein the Ebola epidemic is rendering it nearly impossible to provide malaria services should give us pause. According to Reuters, “Treatable diseases such as malaria and diarrhea are left untended because frightened Liberians are shunning medical centers, and these deaths could outstrip those from the Ebola virus by three or four fold.”
The new resolution (A/68/L.60) in calling for increases national resources allocated to controlling that disease from public and private sources demonstrates the importance of national commitment to sustain and advance malaria control into the era of malaria elimination. It is now up to local malaria advocates to ensure that their governments, as well as private sector and local NGO partners, follow through to guarantee the needed quantity and quality of malaria services.
Private Sector &Treatment &Universal Coverage Bill Brieger | 25 Apr 2014
Malaria and febrile illness care seeking in Bauchi State, Nigeria
World Malaria Day 2014 was observed at the Johns Hopkins Bloomberg School of Public Health. Admiral Tim Ziemer, the Coordinator of the US President’s Malaria Initiative was keynote speaker. Other speakers from the NGO and faith based organization community also talked about the importance of partnership in fighting a disease that still claims 600,000 lives annually. In addition 21 posters were presented.
Below is the abstract of one poster representing our work with USAID’s Targeted States High Impact Project in Nigeria.
Malaria and febrile illness care seeking in Bauchi State, Nigeria: context for improving case management at the primary level
Seeking of appropriate and q uality care for childhood illnesses is a major challenge in much of Africa including Bauchi State, Nigeria. In advance of an intervention to improve available care in the most common points of service (POS), government primary health care centers (PHCs) and patent medicine vendors (PMV), a survey was done of child caregivers in four districts concerning responses to febrile illness, suspected malaria, acute respiratory disease and diarrhea. The ethical review committee in the Bauchi State Ministry of Health approved of the study.
uality care for childhood illnesses is a major challenge in much of Africa including Bauchi State, Nigeria. In advance of an intervention to improve available care in the most common points of service (POS), government primary health care centers (PHCs) and patent medicine vendors (PMV), a survey was done of child caregivers in four districts concerning responses to febrile illness, suspected malaria, acute respiratory disease and diarrhea. The ethical review committee in the Bauchi State Ministry of Health approved of the study.
A total of 3077 children below the age of five were identified in the households sampled. Their mothers, fathers or other caregivers consented and were interviewed. Among the children 74% had any Illness, 57% had fever, 26% had cough, and 15% had diarrhoea. Only 8.7% of 1186 febrile children had their blood tested.
Care seeking from PMVs varied from 45% with fever, 40% with cough to 36% with diarrhoea. Care from public sector POS varied from 26-33%. Treatment that might be considered ‘appropriate’ for each also varied with 30% receiving antimalarial drugs for suspected malaria, 20% getting oral rehydration solution for diarrhoea and 50% being given an antibiotic for a suspected acute respiratory illness.
The results show that providing quality integrated case management with appropriate commodities through PHCs and PMVs can improve the illness care of a majority of children in Bauchi State, and interventions are currently being planned to do this.
Poster by … William R. Brieger, MPH, CHES, DrPH 1, Bright Orji, MPH 2, Masduk Abdulkarim 3, (1) International Health, Bloomberg School of Public Health, The John Hopkins University, 615 N Wolfe St, Baltimore, MD 21205 (and Jhpiego). (2) Jhpiego, Thames St, Baltimore, MD 21231`. (3) Targeted States High Impact Project USAID Nigeria, Bauchi, Nigeria.
Drug Quality &Private Sector &Treatment Bill Brieger | 05 Oct 2013
Patent Medicine Vending: vendors’ perspectives on business and health
Patent medicine vendors (PMVs) , also known as medicine shop owners, are a major source of malaria medicines. This qualitative examination of how PMVs perceive their business was conducted by Kabiru Salami, Bill Brieger and Stephen Kodish.
 Access to high-quality, affordable medicines is a global concern but manifests in distinctly local ways. In Nigeria, patent medicine vendors (PMVs) are a major source of medicines. Criticism of PMVs focuses on drug quality, dispensing practices, and their lack of formal health care training.
Access to high-quality, affordable medicines is a global concern but manifests in distinctly local ways. In Nigeria, patent medicine vendors (PMVs) are a major source of medicines. Criticism of PMVs focuses on drug quality, dispensing practices, and their lack of formal health care training.
This qualitative investigation approached PMVs as small business people and sought their business perspectives in comparison with views of other small business owners in Igbo-Ora, Nigeria. This study utilized an iterative approach to data collection among 51 entrepreneurs.
In-depth interviews about participants’ businesses were collected from PMVs (16), Food (7), Clothing (7), Provisions (9), Motor Parts (n7), and others (n5). A codebook containing 27 themes was inductively developed from emergent data and combined into broader themes for interpretation using Atlas.ti v7.1.
Accounts from participants reveal differences between PMVs and other businesses including amount of education necessary to learn the trade, as well as the level of professionalism and cleanliness required to operate successfully. Unlike other groups, PMVs routinely are asked for highly technical information at point of purchase.
PMVs work largely under strong trade associations due to more controls imposed by regulatory agencies. Although selling medicine is a small-scale enterprise, the purveyors of the trade see their work differently from other small business people. Their business model is based on having adequate knowledge about their products and maintaining standards. PMVs can increase human resources for health because they want to improve both their work and business prospects.
Private Sector Bill Brieger | 11 Mar 2013
Invest in the Future: How Corporations Can Impact Malaria
The word “invest†in the new World Malaria Day theme encourages us to focus our attention on the role of the corporate community.
A recent study completed on behalf of the Roll Back Malaria partnership by Malaria No more and McKinsey and Company, reviewed the potential impact of future business investment on malaria control. They found that, “According to the McKinsey report, if business were to invest approximately $10.9 billion over 5 years, we’d be able to achieve full coverage of prevention and treatment measures in the most affected African countries.â€
 ExxonMobil, has contributed broadly to malaria control programs and research both from the headquarters level as well as through its national affiliates. ExxonMobil Foundation, the company’s philanthropic arm, has committed $110 million worldwide since 2000 to its Malaria Initiative. For example, with ExxonMobil Foundation support, Jhpiego conducted proof of concept interventions in Akwa Ibom State, Nigeria that showed how community directed interventions (CDI – the foundation approach for onchocerciasis control in Africa) could be adapted to increasing coverage of insecticide treated nets, intermittent preventive treatment for pregnant women and community case management for malaria, diarrhea and pneumonia.
ExxonMobil, has contributed broadly to malaria control programs and research both from the headquarters level as well as through its national affiliates. ExxonMobil Foundation, the company’s philanthropic arm, has committed $110 million worldwide since 2000 to its Malaria Initiative. For example, with ExxonMobil Foundation support, Jhpiego conducted proof of concept interventions in Akwa Ibom State, Nigeria that showed how community directed interventions (CDI – the foundation approach for onchocerciasis control in Africa) could be adapted to increasing coverage of insecticide treated nets, intermittent preventive treatment for pregnant women and community case management for malaria, diarrhea and pneumonia.
Corporate contributions do not have to be direct financing. Corporations have certain skills and mechanisms that can be applied to public health challenges. In a press release The Coca-Cola Company and the Global Fund to Fight AIDS, Tuberculosis and Malaria “announced they will expand a project leveraging the Company’s expansive global distribution system and core business expertise to help government and non-governmental organizations deliver critical medicines to remote parts of the world, beginning in rural Africa.†This has been dubbed “Project Last Mile.â€
AngloGold Ashanti in Ghana provides another model of corporate involvement. Starting in 2005, AngloGold began indoor residual spraying (IRS) of all houses in Obuasi District. Within a few years there was a noticeable drop of 74% in malaria cases in the district health facilities.  Bringing its experience managing a large program in Obuasi, AngloGold as “AngloGold Ashanti Malaria Control Limited,†has become the Principal Recipient of a Global Fund grant in Ghana to conduct IRS in 40 districts.
Corporate involvement in social programs generally and malaria control specifically is obviously not completely without controversy, especially in countries where corporations need to interact with governments that have questionable human rights records.
What is of importance in considering corporate investment in malaria control may not necessarily be the scale of investment, but its quality. Corporate activities can demonstrate good management practices that should be adopted by other major players in the malaria control arena. Corporate supported projects may provide proof of new concepts that can be taken to scale by national malaria control programs to increase their coverage. Finally corporate contributions set an example and serve as an advocacy point to encourage national governments to fulfill their own obligations to their citizens.
A longer version of this article will appear in the March 2013 edition of Africa Health.
Drug Quality &Private Sector &Treatment Bill Brieger | 10 Mar 2013
Revisiting the AMFm Controversy
Paul Kartchner contributes this guest blog via the SBFPHC Policy Advocacy Blog.For years, a major obstacle to controlling malaria in developing countries has been the high cost of effective medications. Yet in recent years a coalition of public health agencies and organizations are targeting this problem by subsidizing the most effective medications. Called the Affordable Medicines Facility – malaria (AMFm), the project hopes to make these medications more available and affordable to hospitals, physicians, and local pharmacies in developing countries.
Photo shows Workers load AFMm medications in Abuja, Nigeria (courtesy Novartis International AG)
Yet even though the project has been found to increase the supply of medications, criticisms have been raised regarding the program’s long-term benefits. A recent report by Oxfam, an international aid group, claims that although these medications are now broadly available, they are not being used appropriately to treat patients with malaria. They also claim that many patients that do need these medications, including women and children, still do not have access to them.
Another aid group, Doctors without Borders/Médecins Sans Frontières (MSF), claims that a project like AMFm cannot be successful if it is not carefully integrated into a larger strategy to combat malaria. Instead MSF recommends a plan whereby not only the medication but also treatment by knowledgeable providers is subsidized.
These criticisms raise important questions about the nature of complex global diseases such as malaria. Focusing efforts and resources on a particular aspect of a problem without considering the larger context may not only fail to improve the situation, but potentially make it worse.
Private Sector Bill Brieger | 20 Nov 2012
Corporations weigh in on solving the malaria challenge
The Corporate Alliance on Malaria in Africa announces a Member Meeting that will take place on December 3, 2012 from 10 am – 4 pm in Houston, Texas. They have shared their invitation with us to let interested colleagues know how to take part.

The Corporate Alliance on Malaria in Africa (CAMA) is a unique coalition of companies that share a vision to reduce the incidence of malaria by promoting private sector cooperation in sub-Saharan Africa. Founded by Marathon Oil in 2007, CAMA serves as a platform for private sector collaboration with country governments and other major stakeholders in the global response against malaria.
CAMA’s three principal objectives include –
- building country-level capacity for effective malaria control and its eventual elimination;
- providing a forum to exchange knowledge and current best practices in malaria control; and
- facilitating the establishment of effective multi-sector partnerships to increase the scale and impact of malaria control interventions.
GBCHealth is the implementing partner and secretariat of CAMA.A special Member Meeting will be held Monday, December 3, 2012, in Houston, Texas, to discuss the accomplishments of the past year and to develop the CAMA engagement strategy for 2013. As CAMA transitions into a fully integrated GBCHealth flagship initiative, this CAMA member meeting will be open to all current and prospective GBCHealth members interested in contributing to global malaria efforts.
The meeting will cover the importance of social and behavioral change programs for controlling malaria at the country level and provide a great networking opportunity for companies to meet key malaria stakeholders from academia, business and non-profits.
RSVP by clicking this link.
Advocacy &Private Sector Bill Brieger | 15 Oct 2012
Healthy workers can be malaria champions in their communities
Emmanuel Fiagby of the VOICES for a Malaria-Free Future in Ghana shares a recent workshop of the Ghana Revenue Authority at Kpetoe, Volta Region, Ghana. Below are his experiences.
 The Ghana Revenue Authority has made a giant stride in the implementation of its Employee Wellbeing Program (EWP) by initiating a program which will result in the development and implementation of a Malaria Control Strategy and Program of Action for the Authority. A total of 45 officials of the GRA mostly EWP Focal Persons participated in the program.
The Ghana Revenue Authority has made a giant stride in the implementation of its Employee Wellbeing Program (EWP) by initiating a program which will result in the development and implementation of a Malaria Control Strategy and Program of Action for the Authority. A total of 45 officials of the GRA mostly EWP Focal Persons participated in the program.
Launching the program at the Customs Excise and Preventive Services (CEPS) Academy here, the Commissioner General of the GRA Mr. George Blankson stated that the GRA has since its establishment shown tremendous commitment towards the welfare, health and wellbeing of its staff who are its most valued asset and therefore finds the theme for its Malaria Control strategy development exercise, “Turning Revenue Makers in to Malaria champions; a true demonstration of corporate social responsibility,†an apt reflection of what the GRA stands for.
Mr. Blankson emphasized that, the aim of the GRA in setting up its EWP of which malaria is becoming a key component is to set the pace as a leading healthy workplace in Ghana where staff and management work together to protect and promote the health, safety and wellbeing of its over 7,000 staff and almost 30,000 community members on a sustainable basis. “Today we stand at the threshold of expanding the frontiers of the Employee Wellbeing Program (EWP) to encompass malaria control programs for our staff and the wider community which GRA serves. I am extremely certain that this effort will lead to the total obliteration of the 25% absenteeism of our workforce attributed to malaria and the random deaths this disease wrecks on our institution,†the Commissioner General reiterated. He called on all officers selected to lead the malaria program and noted that by becoming champions for malaria control, they will be “contributing to sustaining a stronger workforce, a stronger community and therefore a more productive and taxpaying community.â€
In her key note remarks, Dr. Kezia Malm, Deputy Manager of the National Malaria Control Program (NMCP) stressed that Ghana has made tremendous progress in the fight against malaria and it’s only through the collaborative efforts of parastatal institutions such as the GRA and others that the country would be able to sustain the gains. “Our journey to eliminating malaria can only end successfully if the support of every sector of our development effort – the public sector, private sector, NGOs, and the donor community is sustained,†she concluded.
The two day GRA Malaria Control Strategy development and action plan development program was organized by the Johns Hopkins University Center for Communication Programs Voices Project in collaboration with the Ghana Revenue Authority and the National Malaria Control Program. In setting the stage for the program, the Country Director of the Voices for a Malaria-free Future Project, Mr. Emmanuel Fiagbey pointed out that the GRA, a non-health institution becoming a champion for malaria control should be an effort worth emulating by other powerful parastatal institutions. “That the ‘Revenue Makers’ our tax officials have become malaria advocates and mentors for their colleagues should not only result in preserving the health of the GRA Workforce against malaria, it must also lead to speedy action on malaria commodities and their documentation that come to the tables of the tax officials in the course of their work,†Mr. Fiagbey emphasized.
The Ghana Revenue Authority is a major parastatal institution in Ghana made up of the Customs Excise and Preventive Service, the Internal Revenue Service and the VAT Service. Fifteen senior officers of the Authority including Mr. K. E. Enyimayew the Deputy Commissioner HR, Deputy Directors of the three arms of the Authority, Service Commanders/Commissioners and the Director of the CEPS Academy also participated in the opening activities of the program.
Malaria is often a major cause of absenteeism – either for the sick worker or the worker who has to stay home with a sick child or relative. The GRA sets a great example how malaria training for members of the workforce can improve occupational, family and community health.