Case Management &Funding &Insurance &Uncategorized Bill Brieger | 17 Dec 2018
Community Based Health Insurance Can Fight Malaria
Community-Based Health Insurance (CBHI) is seen as a way to promote universal health coverage and protect vulnerable populations from catastrophic financial effects of illness. Malaria can be such an illness is not treated in a timely manner, and having insurance can help prevent delays.

In countries including Rwanda, Burkina Faso and Senegal a particular CBHI scheme known as mutuelles has taken root. For Rwanda USAID (2018) reports that …
The 2014–2015 DHS showed that insurance coverage has remained stable since the 2010DHS and that 79 percent of the households have at least one family member with health insurance and that among those insured 97 percent have community health insurance (mutuelles). Early ANC attendance is also encouraged by providing targeted SBCC, combined with innovative community- and facility-level performance-based financing and high enrollment in community health insurance schemes (mutuelles). The MoH, with the support of partners, has worked to improve the quality of services for case management at health facilities through training and capacity building efforts at national and district levels.
A study looked at health care seeking for children below 5years of age in Rwanda in 2005 to 2010 and found that, “In both years,under-five children with Mutuelles were more likely to use medical care than uninsured children. Children in 2010 had a higher probability of using medical care … regardless of the children’s poverty or Mutuelles status.” The study provides an example of how pre-payment CBHI can not only increase universal health coverage but also address challenges of equity (Mejía-Guevara et al., 2015).
Below is a chart showing the fee structure in Rwanda (Tashobya, 2017). [The trainer should ask participants about fees for CBHIs or other national health insurance schemes in their countries if such exist and how participation in CHBI helps achieve UHC.]
| Fees in Rwanda’s community insurance scheme, Mutuelles | ||
| Ubudehe/Social Category | Annual Rwandan Francs per Household Member | Approximate US Dollars |
| 1 | 0 (Paid by government) | 0 |
| 2 | 2,000 | 2.25 |
| 3 | 3,000 | 3.35 |
| 4 | 4,000 | 7.85 |
Now The East African reports that, “With more than 90 per cent of Rwandans covered under the community-based health insurance scheme locally known as Mutuelle de Santé, Rwanda is one of the few developing countries in the world that have successfully achieved universal healthcare” (Kagire, 2018) This was achieved by addressing enrollment, quality of cane and transferring management of the scheme to the Rwanda Social Security Board (RSSB). Now more than ever, no one needs to die from malaria in Rwanda.
- Kagire, Edmund (2018). Rwanda Has Achieved Universal Healthcare. The East African. 15 December 2018. https://allafrica.com/stories/201812150128.html
- Mejía-Guevara I, Hill K, Subramanian SV, Lu C. (2015). Service availability and association between Mutuelles and medical care usage for under-five children in rural Rwanda: a statistical analysis with repeated cross-sectional data. BMJ Open. 2015 Sep 8;5(9):e008814. doi: 10.1136/bmjopen-2015-008814.
- Tashobya, Athan (2017). Mutuelle Month: Govt targets 100% subscription. The New Times. Published : April 03, 2017. https://www.newtimes.co.rw/section/read/210035
- USAID/President’s Malaria Initiative (2018) Rwanda Malaria Operational Plan FY19. https://www.pmi.gov/docs/default-source/default-document-library/malaria-operational-plans/fy19/fy-2019-rwanda-malaria-operational-plan.pdf?sfvrsn=3
Burden &Funding &Health Education &Health Systems &Invest in Malaria Control &ITNs &Management Bill Brieger | 19 Nov 2018
Malaria funding may never be enough, but better program management should be possible
 The World Malaria Report shows that malaria cases are up, and even though there are fewer reported cases in 2017 than 2010, the number is greater than 2016. So once again high burden countries are being targeted. Today this focus is on “High Burden to High Impact”, but in 2012-13 it was the “Malaria Situation Room” that also focused on 10 high burden countries.
The World Malaria Report shows that malaria cases are up, and even though there are fewer reported cases in 2017 than 2010, the number is greater than 2016. So once again high burden countries are being targeted. Today this focus is on “High Burden to High Impact”, but in 2012-13 it was the “Malaria Situation Room” that also focused on 10 high burden countries.
Progress was being made up to around 2015-16, it then started to reverse. The challenge was not just funding. As the WHO Director General noted in the foreword to the 2018 World Malaria Report (WMR), “Importantly, ‘High burden to high impact’ calls for increased funding, with an emphasis on domestic funding for malaria, and better targeting of resources. The latter is especially pertinent because many people who could have benefited from malaria interventions missed out because of health system inefficiencies.”
 Over the years there have never been enough pledged funds to fully achieve targets, but as funding has never reached desired levels, attention is now being drawn more and more to the source of that funding (more emphasis on domestic/endemic countries) and especially how the health system functions to use the funds that are made available. In 1998 during one of the early meetings establishing the Roll Back Malaria Partnership, a speaker stressed that malaria control could not succeed without concomitant health systems strengthening and reform. That 20-year-old thought was prescient for today’s dilemma.
Over the years there have never been enough pledged funds to fully achieve targets, but as funding has never reached desired levels, attention is now being drawn more and more to the source of that funding (more emphasis on domestic/endemic countries) and especially how the health system functions to use the funds that are made available. In 1998 during one of the early meetings establishing the Roll Back Malaria Partnership, a speaker stressed that malaria control could not succeed without concomitant health systems strengthening and reform. That 20-year-old thought was prescient for today’s dilemma.
First, what is the funding situation? As outlined in the World Malaria Report …
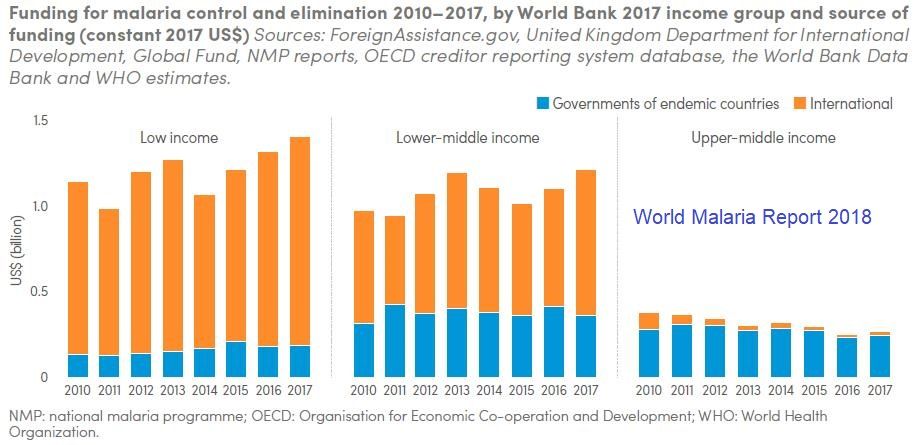
- In 2017, an estimated US$ 3.1 billion was invested in malaria control and elimination efforts globally by governments of malaria endemic countries and international partners – an amount slighter higher than the figure reported for 2016.
- Governments of endemic countries contributed 28% of total funding (US$ 900 million) in 2017, a figure unchanged from 2016.
- Funding for malaria has remained relatively stable since 2010
- To reach the Global Technical Strategy 2030 targets, it is estimated that annual malaria funding will need to increase to at least US$ 6.6 billion per year by 2020
 The question remains – does investment lead to results. The WMR shows, for example, that “Between 2015 and 2017, a total of 624 million insecticide-treated mosquito nets (ITNs/LLINs), were reported by manufacturers as having been delivered globally. This represents a substantial increase over the previous period 2012–2014, when 465 million ITNs were delivered globally”.
The question remains – does investment lead to results. The WMR shows, for example, that “Between 2015 and 2017, a total of 624 million insecticide-treated mosquito nets (ITNs/LLINs), were reported by manufacturers as having been delivered globally. This represents a substantial increase over the previous period 2012–2014, when 465 million ITNs were delivered globally”.
At the same time the report states that, “Households with at least one ITN for every two people doubled to 40% between 2010 and 2017. However, this figure represents only a modest increase over the past 3 years, and remains far from the target of universal coverage.” Is it simply a matter of funding to reach the other 60% of households, or are there serious management problems on the ground?
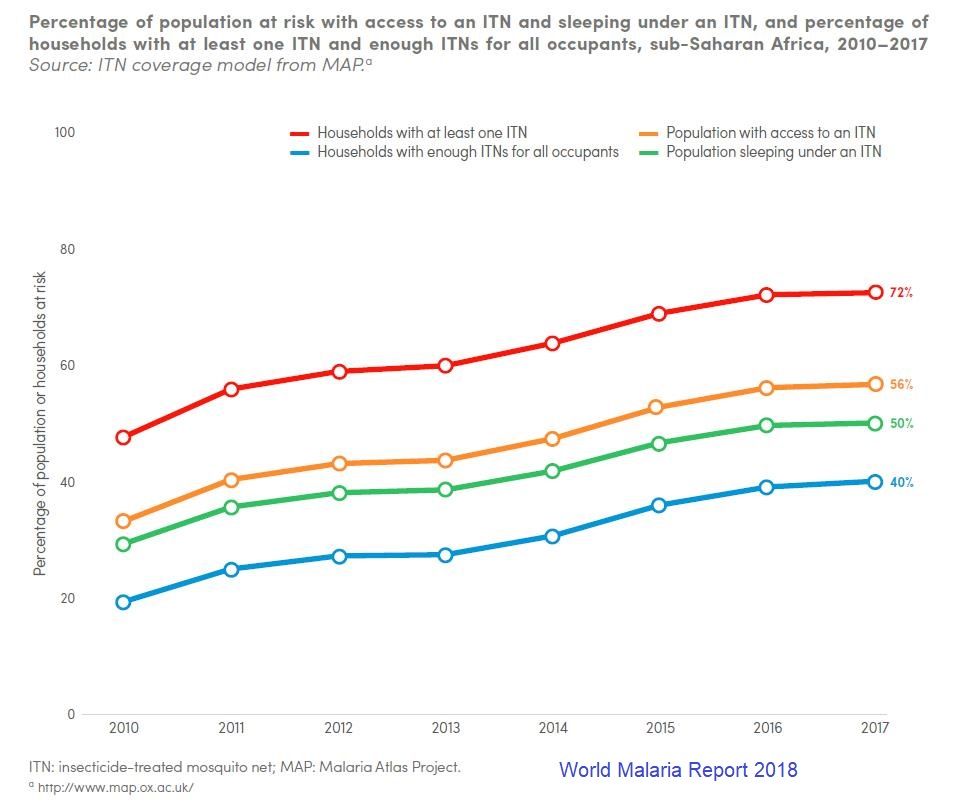 Then there is the issue of using nets. The WMR traces new ownership and use from 2010 to 2017, and we can see that overall the proportion of the population at risk who slept under a net increased from around 30% to 50%, but only 56% of those with access to a net were sleeping under them. This can be attributed in part but not completely to the adequacy of nets in a household.
Then there is the issue of using nets. The WMR traces new ownership and use from 2010 to 2017, and we can see that overall the proportion of the population at risk who slept under a net increased from around 30% to 50%, but only 56% of those with access to a net were sleeping under them. This can be attributed in part but not completely to the adequacy of nets in a household.
We should ask are enough nets getting to the right places, and also are efforts in place to promote their use. Behavior change efforts should be a major component of malaria program management. Even the so called biological challenges to malaria control have a human element. Monkey malaria transmission to people results from deforestation. Malaria parasite resistance to medicines comes from poor drug management on individual and systems levels.
The target year 2030 will be here before we know it. Will malaria still be here, or will countries and donors get serious about malaria financing AND program management?
Advocacy &Case Management &Children &CHW &Community &Elimination &Funding &iCCM &Invest in Malaria Control &IPTp &ITNs Bill Brieger | 25 Apr 2018
On World Malaria Day the realities of resurgence should energize the call to ‘Beat Malaria’
 Dr Pedro Alonso who directed the World Health Organization’s Global Malaria Program, has had several opportunities in the past two weeks to remind the global community that complacency on malaria control and elimination must not take hold as there are still over 400,000 deaths globally from malaria each year. At the Seventh Multilateral Initiative for Malaria Conference (MIM) in Dakar, Dr Alonso drew attention to the challenges revealed in the most recent World Malaria Report (WMR). While there have been decreases in deaths, there are places where the number of actual cases is increasing.
Dr Pedro Alonso who directed the World Health Organization’s Global Malaria Program, has had several opportunities in the past two weeks to remind the global community that complacency on malaria control and elimination must not take hold as there are still over 400,000 deaths globally from malaria each year. At the Seventh Multilateral Initiative for Malaria Conference (MIM) in Dakar, Dr Alonso drew attention to the challenges revealed in the most recent World Malaria Report (WMR). While there have been decreases in deaths, there are places where the number of actual cases is increasing.
 Around twenty years ago the course of malaria changed with the holding of the first MIM, also in Dakar and the establishment of the Roll Bank Malaria (RBM) Partnership. These were followed in short order by the Abuja Declaration that set targets for 2010 and embodied political in endemic countries, as well as major funding mechanisms such as the Global Fund to fight AIDS, TB and Malaria. This spurred what has been termed a ‘Golden Decade’ of increasing investment and intervention coverage, leading to decreasing malaria morbidity and mortality. The Millennium Development Goals provided additional impetus to reduce the toll of malaria by 2015.
Around twenty years ago the course of malaria changed with the holding of the first MIM, also in Dakar and the establishment of the Roll Bank Malaria (RBM) Partnership. These were followed in short order by the Abuja Declaration that set targets for 2010 and embodied political in endemic countries, as well as major funding mechanisms such as the Global Fund to fight AIDS, TB and Malaria. This spurred what has been termed a ‘Golden Decade’ of increasing investment and intervention coverage, leading to decreasing malaria morbidity and mortality. The Millennium Development Goals provided additional impetus to reduce the toll of malaria by 2015.
 On Facebook Live yesterday Dr Alonso talked about that ‘Golden Decade.’ There was a 60% decrease in mortality and a 40% decreases in malaria cases. But progress slowing down and we may be stalled at a crossroads. He noted that history show unless accelerate efforts, malaria will come back with a vengeance. Not only is renewed political leadership and funding, particularly from affected countries needed, but we also need new tools. Dr Alonso explained that the existing tools allowed 7m deaths be diverted in that golden decade, but these tools are not perfect. We are reaching limits on these tools such that we need R&D for tools to enable quantum leap forward. Even old tools like nets are threatened by insecticide resistance, and research on alternative safe insecticides is crucial.
On Facebook Live yesterday Dr Alonso talked about that ‘Golden Decade.’ There was a 60% decrease in mortality and a 40% decreases in malaria cases. But progress slowing down and we may be stalled at a crossroads. He noted that history show unless accelerate efforts, malaria will come back with a vengeance. Not only is renewed political leadership and funding, particularly from affected countries needed, but we also need new tools. Dr Alonso explained that the existing tools allowed 7m deaths be diverted in that golden decade, but these tools are not perfect. We are reaching limits on these tools such that we need R&D for tools to enable quantum leap forward. Even old tools like nets are threatened by insecticide resistance, and research on alternative safe insecticides is crucial.
 Dr Alonso at MIM pointed to the worrying fact that investment in malaria overall peaked in 2013. Investment by endemic countries themselves has remained stable throughout and never gone reached $1 billion despite advocacy and leadership groups like the Africa Leaders Malaria Alliance. The 2017 WMR shows that while 16 countries achieved a greater that 20% reduction in malaria cases, 25 saw a greater that 20% increase in cases. The outnumbering of decreasing countries by increasing was 4 to 8 in Africa, the region with the highest burden of the disease. Overall 24 African countries saw increases in cases between 2015 and 2016 versus 5 that saw a decrease. A review of the Demographic and Health and the Malaria Information Surveys in recent years show that most countries continue to have difficulty coming close to the Abuja 2010 targets for Insecticide treated net (ITN) use, prompt and appropriate malaria case management and intermittent preventive treatment of malaria in pregnancy (IPTp).
Dr Alonso at MIM pointed to the worrying fact that investment in malaria overall peaked in 2013. Investment by endemic countries themselves has remained stable throughout and never gone reached $1 billion despite advocacy and leadership groups like the Africa Leaders Malaria Alliance. The 2017 WMR shows that while 16 countries achieved a greater that 20% reduction in malaria cases, 25 saw a greater that 20% increase in cases. The outnumbering of decreasing countries by increasing was 4 to 8 in Africa, the region with the highest burden of the disease. Overall 24 African countries saw increases in cases between 2015 and 2016 versus 5 that saw a decrease. A review of the Demographic and Health and the Malaria Information Surveys in recent years show that most countries continue to have difficulty coming close to the Abuja 2010 targets for Insecticide treated net (ITN) use, prompt and appropriate malaria case management and intermittent preventive treatment of malaria in pregnancy (IPTp).
 The coverage gap is real. The WMR shows that while there have been small but steady increase in 3 doses of IPTp, coverage of the first dose has leveled off. Also while ownership of a net by households has increased, less than half of households have at least one net for every two residents.
The coverage gap is real. The WMR shows that while there have been small but steady increase in 3 doses of IPTp, coverage of the first dose has leveled off. Also while ownership of a net by households has increased, less than half of households have at least one net for every two residents.
In contrast a new form of IPT – seasonal malaria chemoprevention (SMC) for children in the Sahel countries has taken off with over 90% of children receiving at least one of the monthly doses during the high transmission season. Community case management is taking off as is increased use of rapid diagnostic testing. Increased access to care may explain how in spite of increased cases, deaths can be reduced. This situation could change rapidly if drug resistance spreads.
 While some international partners are stepping up, we are far short of the investment needed. The Gates Foundation is pledging more for research and development to address the need for new tools as mentioned by Dr Alonso. A big challenge is adequate funding to sustain the implementation of both existing tools and the new ones when they come online. Even in the context of a malaria elimination framework, WHO stresses the need to maintain appropriate levels of intervention with case management, ITNs and other measures regardless of the stage of elimination at which a country or sub-strata of a country is focused.
While some international partners are stepping up, we are far short of the investment needed. The Gates Foundation is pledging more for research and development to address the need for new tools as mentioned by Dr Alonso. A big challenge is adequate funding to sustain the implementation of both existing tools and the new ones when they come online. Even in the context of a malaria elimination framework, WHO stresses the need to maintain appropriate levels of intervention with case management, ITNs and other measures regardless of the stage of elimination at which a country or sub-strata of a country is focused.
Twenty years after the formation of RBM and 70 years after the foundation of WHO, the children, families and communities of endemic countries are certainly ready to beat malaria. The question is whether the national and global partners are equally ready.
Advocacy &Borders &Children &Conflict &Costs &Epidemiology &Funding &Human Resources &Leadership &Monitoring &Mortality &NTDs &Partnership &Surveillance Bill Brieger | 03 Feb 2018
African Leaders Malaria Alliance Recognizes Country Achievements, Adds NTDs to its Scorecard
 The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
 For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
The scorecard will now “report progress for the 47 NTD-affected countries in sub-Saharan Africa in their strategies to treat and prevent the five most common NTDs: lymphatic filariasis, onchocerciasis, schistosomiasis, soil-transmitted helminths and trachoma. By adding NTDs to the scorecard, African leaders are making a public commitment to hold themselves accountable for progress on these diseases.”
 In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
The combination is based on the logic that NTDs and malaria are both diseases of poverty. Malaria and several NTDs are also vector-borne. Also community platforms are a foundation for delivering needed drugs and supplies to tackle these diseases. Ultimately the decision shows that Heads of State are holding themselves accountable for progress in eliminating these diseases.
 At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
 The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
H.E . Dr. Barnabas Sibusiso Dlamini, the Prime Minister of the Kingdom of Swaziland, whose King and Head of State is the current chair of ALMA, warned all endemic countries that, “When we take our eyes off malaria, the cost for our countries is huge. Yet if we increase our efforts to control and eventually eliminate malaria, the yield we get from it is tremendous. It is time that we dig deep into our pockets and provide malaria programmes with the needed resources.”
 Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
IRIN concludes that, “For now, the biggest challenge for Zambia will be closing the gap in its malaria elimination strategy, which will cost around $160 million a year and is currently only about 50 percent funded – two thirds from international donors and one third from the Zambian government. Privately, international donors say the government must spend more money on its malaria programme if it is to succeed.” Cross-border transmission adds to the problem.
Internal strife is another challenge to malaria success. “The recent nurses’ strike which lasted for five months may have cost Kenya a continental award in reducing the prevalence of malaria during the 30th African Union Summit in Ethiopia on Sunday.” John Muchangi in the Star also noted that, “However, Kenya lost momentum last year and a major malaria outbreak during the prolonged nurses’ strike killed more than 30 people within two weeks in October.”
 Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Fortunately ALMA is equipped with the monitoring and advocacy tools to ensure that its members recognize and respond to such challenges. The Scorecards will keep the fight against the infectious diseases of poverty on track.
Elimination &Epidemiology &Funding &IPTp &ITNs &Procurement Supply Management &Treatment Bill Brieger | 20 May 2017
Ghana – spotlight on malaria indicators
 The Demographic and Health Surveys has released a brief on key indicators from the Ghana Malaria Indicator Survey of 2016. While much of the malaria community is discussing the elimination framework and processes, the reality is that many high burden countries are still trying to scale up basic interventions to achieve universal coverage.
The Demographic and Health Surveys has released a brief on key indicators from the Ghana Malaria Indicator Survey of 2016. While much of the malaria community is discussing the elimination framework and processes, the reality is that many high burden countries are still trying to scale up basic interventions to achieve universal coverage.
The overall prevalence across the country in children aged 6-59 months at the time of the survey was 27% using Rapid Diagnostic test and 20% using microscopy. Among children reporting fever in the previous two weeks care/advice was sought for only 72%. Although only only 30% received some sort of blood based diagnostic test, 61% of the febrile children were given the antimalarial artemisinin-based combination therapy drugs.
 Children are still being treated without the benefit of parasitological testing, a key procedure highlighted in WHO case management guidelines. Presumptive treatment for malaria without testing means that a child could inappropriately receive antimalarial drugs and die of another underlying febrile illness. Appropriate testing and adherence to test results is one of the main areas of focus of Ghana’s grants from the US President’s Malaria Initiative. Improved testing is also an important element in Ghana’s current Global Fund support. Clearly more value for money is needed from these inputs.
Children are still being treated without the benefit of parasitological testing, a key procedure highlighted in WHO case management guidelines. Presumptive treatment for malaria without testing means that a child could inappropriately receive antimalarial drugs and die of another underlying febrile illness. Appropriate testing and adherence to test results is one of the main areas of focus of Ghana’s grants from the US President’s Malaria Initiative. Improved testing is also an important element in Ghana’s current Global Fund support. Clearly more value for money is needed from these inputs.
Preventive measures as documented in the MIS fare somewhat better., but at present only 73% of households own an insecticide treated bednet. When considering the recommended 1 net for every 2 household members, the indicator drops to 50%. Concerning the typical ‘vulnerable’ populations, we see that only 52% of children below the age of 5 years slept under an ITN the night before the survey; only 50% of pregnant women did likewise.
 Malaria prevention in pregnancy results reflect the fact that Ghana has promoted at least three IPTp doses for around ten years. Most pregnant women (78% ) had received the previously recommended minimum of two doses, and now 60% have received at least three doses.
Malaria prevention in pregnancy results reflect the fact that Ghana has promoted at least three IPTp doses for around ten years. Most pregnant women (78% ) had received the previously recommended minimum of two doses, and now 60% have received at least three doses.
One of the important issues stressed in WHO’s new malaria elimination framework is stratifying the country by prevalence to the lowest level possible in order to plan appropriate interventions. Fortunately the Ghana 217 MIS key indicator brief does stratify prevalence and intervention coverage by region. Prevalence through RDT testing ranges from nearly 5% in the urbanized greater Accra area to 44% in the Central Region. Interestingly ITN use is nearly 20% higher in Central than greater Accra.
Hopefully future planning in Ghana will build on this stratification. Better mobilization of donor, national and private sector resources will address likely issues of stock-outs and increase the likelihood of universal coverage of basic interventions that is needed to move the country along the road to malaria elimination.
Funding Bill Brieger | 12 Feb 2017
What are national governments willing to pay for malaria control?
In 2013 national/domestic funding accounted for 20.4% of the US$2.6 billion in global support used to control and eliminate malaria, although it is not clear whether this is governmental, private or a mix.[i] The 2016 World Malaria Report (WMR) reports that, “Total funding for malaria control and elimination in 2015 is estimated at US$ 2.9 billion.[ii] This total represents just 46% of the Global Technical Strategy for Malaria 2016–2030 (GTS) 2020 milestone of US$ 6.4 billion.”
 If domestic funding at the previous rate were to meet this milestone, endemic countries would need to put forward $US1.3 billion themselves, not to mention the fact that domestic funding may be needed even more as uncertainties increase in bilateral and multi-lateral sources. Of the coming from governments, US$ 612 million was direct expenditures through national malaria control programmes (NMCPs) while US$ 332 million was expenditures on malaria patient care. While domestic funding for malaria in African countries has increased in absolute terms over the years, it still remains a smaller proportion of total funding.[iii]
If domestic funding at the previous rate were to meet this milestone, endemic countries would need to put forward $US1.3 billion themselves, not to mention the fact that domestic funding may be needed even more as uncertainties increase in bilateral and multi-lateral sources. Of the coming from governments, US$ 612 million was direct expenditures through national malaria control programmes (NMCPs) while US$ 332 million was expenditures on malaria patient care. While domestic funding for malaria in African countries has increased in absolute terms over the years, it still remains a smaller proportion of total funding.[iii]
Governments in endemic countries characterized by a large portion of the poor, may in fact not contribute a fair share of malaria expenditure. Households are often said to bear the brunt of malaria financing through out-of-pocket expenditure for both treatment and prevention. While we do not have specific figures for malaria, we note that the overall out-of-pocket (OPP) expenditure by households in Nigeria for health care averaged 69.3% between 2010 and 2014.[iv]
Ghana has a national health insurance scheme that may reach up to two-thirds of the population. Costs of fever/malaria episodes therefore should covered by membership, although one is required to pay annual premiums.[v] Still a large portion of the population still pays out-of-pocket.
Although malaria funding from all sources has been increasing over the years, it has recently stagnated at a level approximately 45% of that level targeted to eventually eliminate the disease. In many countries households still bear the brunt of malaria costs, both for treatment and prevention.
Benefits of investments in interventions like community health workers do help bring malaria care closer to the community at a cost people can afford.[vi] More financial support is needed to scale these up, especially by mobilizing in-country governmental, corporate and non-governmental resources.
[i] Kates J and Wexler A. Global Financing for Malaria: TRENDS & FUTURE STATUS.
Kaiser Family Foundation, December 2014 http://kff.org/report-section/global-financing-for-malaria-introduction/
[ii] World Health Organization. World Malaria Report 2016. ISBN 978-92-4-151171-1. Geneva: World Health Organization, 2016
[iii] Korenromp EL, Hosseini M, Newman RD, Cibulskis RE. Progress towards malaria control targets in relation to national malaria programme funding. Malaria Journal 2013, 12:18 Page 2 of 9 http://www.malariajournal.com/content/12/1/18
[iv] World Health Organization. Global Health Expenditure Database: Nigeria. Accessed 6 February 2017. http://apps.who.int/nha/database/Key_Indicators_by_Country/Index/en?COUNTRYKEY=84700
[v] Tawiah T, Asante KP, Dwommoh RA, Kwarteng A, Gyaase S, Mahama E, Abokyi L, Amenga-Etego S, Hansen K, Akweongo P, Owusu-Agyei S. Economic costs of fever to households in the middle belt of Ghana. Malar J. 2016 Feb 6;15:68. doi: 10.1186/s12936-016-1116-x.
[vi] Sunguya BF, Mlunde LB, Ayer R, Jimba M.. Towards eliminating malaria in high endemic countries: the roles of community health workers and related cadres and their challenges in integrated community case management for malaria: a systematic review. Malar J. 2017 Jan 3;16(1):10. doi: 10.1186/s12936-016-1667-x.
Funding &Invest in Malaria Control &Procurement Supply Management Bill Brieger | 19 Dec 2016
Malaria Funding Allocations by the Global Fund and the Need to Mitigate Risk
The Global Fund Observer (aidspan) has provided information on the 2017-19 allocations by the Global Fund to Fight AIDS, TB and Malaria. Here we take a closer look at the malaria component.
Overall malaria grants account for $US 3.3b or 32% of total funding for the period. This includes 71 countries as follows:
- 41 countries in WHO’s Africa Region
- 6 in the Eastern Mediterranean Region
- 7 in the Americas
- 10 in Southeast Asia
- 7 in the Western Pacific

2017-2019 GFATM Allocation
The Global Fund Observer also noted that the GFATM board is very much aware of risks to these grants. An example comes from the management pharmaceuticals. Risks can be found along the whole supply chain process. The GFATM found that, “artemisinin-based combination therapies (ACTs) are more commonly targeted for theft or illegal diversion than are antiretrovirals (ARVs) or medicines for opportunistic infections (OIs).”
In fact the GFATM has identified 40 high or very high risk countries, most of which overlap with the list receiving current grant allocations. Therefore while we praise the provision of needed malaria funds for the upcoming three years, we also call on the Global Fund managers, country coordinating mechanisms, grant recipients and watchdogs in civil society and the media to ensure these grants continue to save lives from malaria.
Funding &Research Bill Brieger | 24 Jun 2016
Malaria Plus Brexit – let’s hope no Malexit
 No one knows for certain the full implications of Britain’s narrow vote to leave the European Union (EU). Since Britain has been a major player in malaria research and development aid, questions naturally arise of whether the British exit (Brexit) from the EU will affect development aid and global research generally and malaria aid and research specifically.
No one knows for certain the full implications of Britain’s narrow vote to leave the European Union (EU). Since Britain has been a major player in malaria research and development aid, questions naturally arise of whether the British exit (Brexit) from the EU will affect development aid and global research generally and malaria aid and research specifically.
Earlier this week the Brookings Institution examined the ways that a Brexit could affect Africa. Here are some of the possibilities adapted to malaria –
- Volatility in the global economic market will affect not only the British economy but also those of malaria endemic countries, possibly reducing the reducing available funds for national contributions to malaria control at home, a major goal for sustaining malaria control and elimination
- Britain specifically may not be able to sustain its financial contributions to malaria aid through the Global Fund, bilateral malaria programs and of course it would no longer contribute to the European Development Fund which currently stands at nearly 15% of its total.
- The British economy which like all modern nations depends on trade would be affected by the need to renegotiate hundreds of trade agreements around the world. Less trade likely means less income and less development aid.
In both 2014 and 2015 the United Kingdom contributed 8% of the total contributions received by the Global Fund to fight HIV, TB and Malaria. In addition “UK’s official development assistance (ODA) is expected to rise to £11.3bn when it hits the 0.7% target. With a population of about 63 million, the figure works out at roughly £137 per Brit.” In 2012 the malaria component was estimated at 2%.
Patrick Vallance and Tim Wells examine the importance of global collaboration on malaria research. This requires the free flow of researchers and their needed supplies across national borders, especially malaria research that has had to date a pan-European character. They describe the collaboration needed “between commercial and non-profit organizations, and between academic science and medicine. Without such partnerships, advances in fighting this deadly disease would not have been possible.”
Vallance and Wells give the example of “GSK’s research site in Tres Cantos, Spain. The lab operates with the support and advice of a broad range of actors, including GSK, the Wellcome Trust, the European Union, and MMV (Medicines for Malaria Venture), as well as various other product-development partnerships and academic centers.” Such efforts may be jeopardized when permits for malaria scientists to work in other countries are more difficult to obtain.
There may be other aid mechanisms too, the Commonwealth Secretariat being one. During World Malaria Day in 2012 the Commonwealth Secretariat pledged to assist in sustaining the gains made in tackling malaria. We hope that Brexit will not become an exit for malaria commitments and saving lives.
Advocacy &Economics &Funding Bill Brieger | 22 Mar 2015
Investing in Malaria at the Country Level: removing the financial burden on the poor
 World Malaria Day 2015 is continuing a 3-year theme of promoting continued financial resource commitment to control and eliminate the disease. Investing in malaria can take many forms, the most obvious of which is the large donor agency grants from the Global Fund (GFATM), the US President’s Malaria Initiative (PMI), DfID, and the World Bank Malaria Booster Program, a name a few. International and local businesses and corporations also provide a share usually through their corporate social responsibility and employee health projects.
World Malaria Day 2015 is continuing a 3-year theme of promoting continued financial resource commitment to control and eliminate the disease. Investing in malaria can take many forms, the most obvious of which is the large donor agency grants from the Global Fund (GFATM), the US President’s Malaria Initiative (PMI), DfID, and the World Bank Malaria Booster Program, a name a few. International and local businesses and corporations also provide a share usually through their corporate social responsibility and employee health projects.
Cost recovery systems are not uncommon
The global financial crisis that began in 2008 lingers in many corners of the world, and has caused thoughtful concern since then about how global disease control efforts can be sustained. In relation to malaria, this concern must take account of the fact that when interventions (ITNs, ACTs, RDTs, IPT) are scaled up and sustained, incidence will drop and the nature of programming and financial commitments will change. A greater emphasis on surveillance, identification of hotspots, response to epidemics, and import of cases from neighboring countries will take the foreground. All this will still require financial support, but where will it come from?
Many of the frontline malaria elimination countries in Africa do not receive external financial support but rely on their own national treasury. As incidence in other endemic countries drops, will the same be expected of them? It is important therefore to look at the current pattern on national commitment to funding malaria control and eventual elimination, including whether countries are devoting 15% of their annual budgets to health. Unfortunately in many countries household out-of-pocket expenditures for malaria services form the bulk of national funding for the disease, a major burden in terms of health equity.

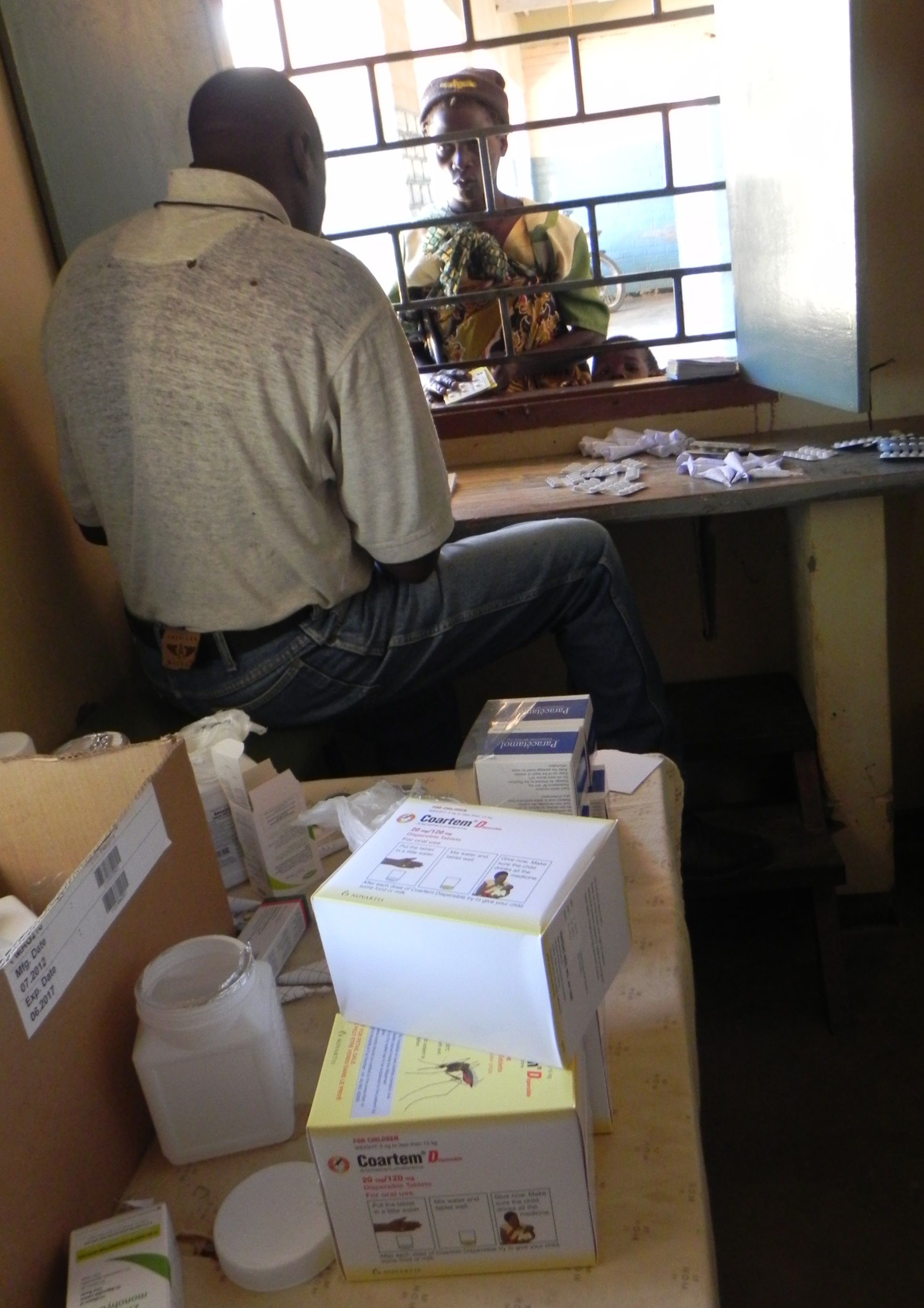
medicine shops are a common place for out-of-pocket malaria expenditures
Cost recovery schemes have been tried in Burkina Faso. Rwanda has instituted community insurance programs. Yet these efforts still put a major financial burden on the poor. Ironically, while the poor pay more, the rich, both individuals, and corporations (national and multi-national) in malaria endemic countries conduct illicit financial transfers out of the country or evade local taxes.
Ultimately the challenges of political accountability for results and financial management within countries to citizens, domestic civil society and other non-state actors must be resolved if governments are going to take on a growing role for eliminating the malaria burden within their borders. Monetary investments alone cannot eliminate malaria. Political will must also be invested to close financial gaps, mobilize resources from various sectors and create a true partnership to end malaria.
(A longer version of this article will appear in the March 2015 issue of Africa Health.)
Advocacy &Costs &Equity &Funding &Treatment &Universal Coverage Bill Brieger | 13 Dec 2014
Malaria Care: Can We Achieve Universal Coverage?
![]() In New York on 12 December 2014, a new global coalition of more than 500 leading health and development organizations worldwide was launched to advocate for universal coverage (UC) and urged “governments to accelerate reforms that ensure everyone, everywhere, can access quality health services without being forced into poverty.” This marked Universal Health Coverage Day which fell on the “two-year anniversary of a United Nations resolution … which endorsed universal health coverage as a pillar of sustainable development and global security.”
In New York on 12 December 2014, a new global coalition of more than 500 leading health and development organizations worldwide was launched to advocate for universal coverage (UC) and urged “governments to accelerate reforms that ensure everyone, everywhere, can access quality health services without being forced into poverty.” This marked Universal Health Coverage Day which fell on the “two-year anniversary of a United Nations resolution … which endorsed universal health coverage as a pillar of sustainable development and global security.”
According to WHO delivery of UC involves four components:
- A strong, efficient, well-run health system
- Affordable care
- Accessible care
- A health workforce with sufficient capacity to meet patient needs
To this list we might add a functioning and timely procurement and supply management system, and not trust people to read between the lines on component #1 to consider this need.
 While much attention in malaria control is appropriately on prevention through various vector control measures, we cannot forget the importance of prompt and appropriate case management, especially as cases decline (according to the new 2014 World Malaria Report) and case detection assumes greater importance.
While much attention in malaria control is appropriately on prevention through various vector control measures, we cannot forget the importance of prompt and appropriate case management, especially as cases decline (according to the new 2014 World Malaria Report) and case detection assumes greater importance.
In 2000 Roll Back Malaria sponsored the Abuja Summit where targets were set for malaria intervention coverage. The goals were established at 80% for insecticide-treated nets (ITNs), intermittent preventive treatment and prompt and appropriate malaria treatment. In 2009, the United Nations declared a goal of universal coverage for ITNs. The potential for UC in malaria case management remained vague, but the new international push for US can certainly include malaria. It would not be coming too late because as we can see from the chart, many endemic countries are far from adequate malaria treatment coverage, let alone UC.
 Frequent surveys help us track progress toward RBM goals and UC – Demographic and Health Survey, Malaria Information Survey, Multi Indicator Cluster Survey. Their helpfulness depends on the questions asked. The 2013 MIS from Rwanda gets closest to finding out what is really happening (Chart 2). We might infer a sequence of events that while not everyone seeks care for their febrile child, those who do are screened by the health worker (including volunteer community health workers); those suspected of malaria are tested (microscopy in clinics, RDTs in communities); and only those found positive are given ACTs.
Frequent surveys help us track progress toward RBM goals and UC – Demographic and Health Survey, Malaria Information Survey, Multi Indicator Cluster Survey. Their helpfulness depends on the questions asked. The 2013 MIS from Rwanda gets closest to finding out what is really happening (Chart 2). We might infer a sequence of events that while not everyone seeks care for their febrile child, those who do are screened by the health worker (including volunteer community health workers); those suspected of malaria are tested (microscopy in clinics, RDTs in communities); and only those found positive are given ACTs.
 Equity is a major concern for advocates of UC. Health insurance is one method to address this. In Ghana around 60% of people have taken part in the National Health Insurance Scheme, but only around 5% in Nigeria where 60% of health expenditure comes from out-of-pocket purchases. Rwanda has a system of mutuelles – community insurance schemes. Insurance does not meet the full need for malaria case management, and thus efforts to expand outlets for affordable quality malaria medicines through the Affordable Medicines Facility malaria (AMFm) was piloted in several countries.
Equity is a major concern for advocates of UC. Health insurance is one method to address this. In Ghana around 60% of people have taken part in the National Health Insurance Scheme, but only around 5% in Nigeria where 60% of health expenditure comes from out-of-pocket purchases. Rwanda has a system of mutuelles – community insurance schemes. Insurance does not meet the full need for malaria case management, and thus efforts to expand outlets for affordable quality malaria medicines through the Affordable Medicines Facility malaria (AMFm) was piloted in several countries.
A combination of approaches is needed to achieve UC in malaria case management. Public and private sources are requires. Low cost, subsidized and free care must to be part of the mix. Over half a million people, mostly children, are still dying from malaria annually. Solving the UC challenge for malaria is crucial.