Elimination &Surveillance &Vector Control Bill Brieger | 17 Apr 2020
A look at Botswana from WHO’s E-2020 country brief
 Botswana is one of a handful of countries in Southern Africa that are nearing malaria elimination targets. The information below is extracted from WHO’s Elimination 2020 program site and shared verbatim.
Botswana is one of a handful of countries in Southern Africa that are nearing malaria elimination targets. The information below is extracted from WHO’s Elimination 2020 program site and shared verbatim.
“Botswana has made impressive progress in reducing indigenous malaria transmission, from a reported 71 000 cases in 2000 to 533 in 2018. Despite significant variation from year to year – with a higher number of malaria cases in 2014, 2016 and 2017 – the country has continued to report an overall decline in both cases and deaths since 2000.
“Challenges faced by Botswana’s national malaria control programme include the perception, in some communities, that malaria is a low priority disease, which can lead to people not protecting themselves with insecticide-treated nets and other WHO-recommended prevention measures. Added to this, some residents do not accept vector control activities such as insecticide spraying inside homes. However, the government’s commitment to eliminate malaria remains strong.
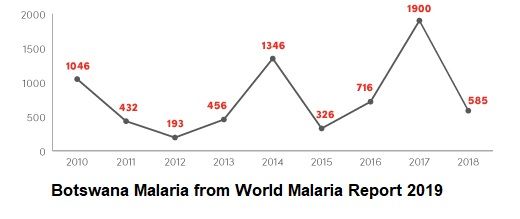 “WHO lists the following Successes in Botswana and the accompanying graph confirms the overall drop, despite some increases:
“WHO lists the following Successes in Botswana and the accompanying graph confirms the overall drop, despite some increases:
- 69% decrease in number of reported malaria cases following outbreaks in 2014, 2016 and 2017;
- all districts using District Health Information Software 2 (DHIS2) for real-time malaria reporting
 mapping of all malaria cases at household level and stratification at village level
mapping of all malaria cases at household level and stratification at village level- adoption of the Community Acting Together to Eliminate Malaria (CATTEM) approach
enhanced community monitoring in malarious districts by malaria surveillance agents”
Hopefully with geographical and epidemiological targeting and attention to early warnings about climate change, Botswana can be among the next group of countries achieving malaria elimination.
Case Management &Elimination &Uncategorized Bill Brieger | 25 Nov 2019
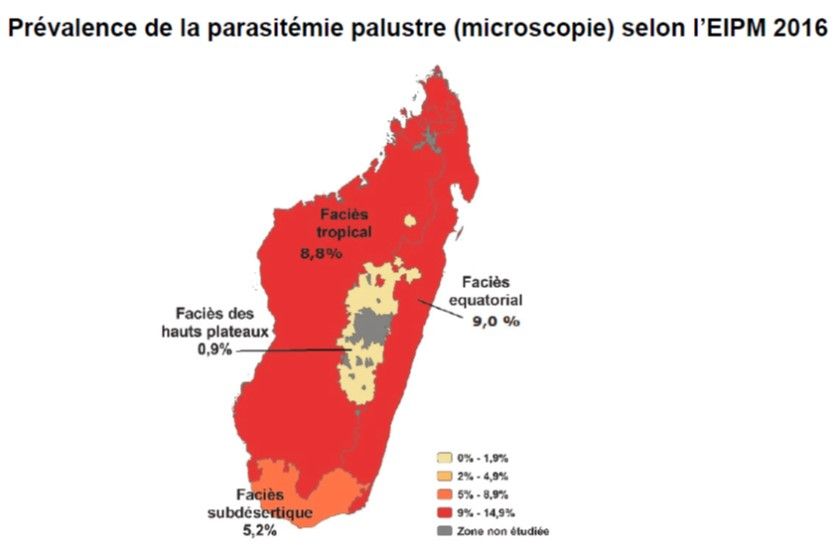
Malaria Case Management Practice and Elimination Readiness in Five Elimination Districts of Madagascar, 2018
Anjoli Anand,* Favero Rachel, Catherine Dentinger, A. Ralaivaomisa, S. Ramamonjisoa, Elaine Razafimandimby, Jocelyn Razafindrakoto, Katherine Wolf, Laura C. Steinhardt, Julie Thwing, Bryan K. Kapella, M. Rabary, Sedera Mioramalala, Jean Pierre Rakotovao presented a poster on “Malaria Case Management Practice and Elimination Readiness in Five Elimination Districts of Madagascar, 2018” at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings are shared below.
 Madagascar’s Malaria National Strategic Plan 2018-2022 calls for progressive malaria elimination beginning in low-incidence districts (< 1 case/1000). Although an elimination plan has not yet been developed, optimizing access to prompt diagnosis and quality treatment will be its foundation, along with improving outbreak detection and response, and developing an elimination plan.
Madagascar’s Malaria National Strategic Plan 2018-2022 calls for progressive malaria elimination beginning in low-incidence districts (< 1 case/1000). Although an elimination plan has not yet been developed, optimizing access to prompt diagnosis and quality treatment will be its foundation, along with improving outbreak detection and response, and developing an elimination plan.
There was need to understand current practices in preparation for elimination such as estimating current implementation readiness, documenting current diagnosis and treatment practices (case management), Assessing the use of data to inform decision-making and determining the availability of commodities, training and supervision. To assess this readiness and inform planning, we surveyed health facilities (HFs) and communities.
 In September 2018, we randomly selected 35 HFs in 5 of the 8 districts identified for elimination, surveyed 41 HWs and 34 community health volunteers (CHVs), and observed 300 clinical encounters between HWs and patients of all ages. Quantitative and qualitative tools were used to collect data. There were a health facility checklist, an interview guide for health facility providers, a clinical observation guide, a community health volunteer CHV) interview guide, and a stakeholder interview guide.
In September 2018, we randomly selected 35 HFs in 5 of the 8 districts identified for elimination, surveyed 41 HWs and 34 community health volunteers (CHVs), and observed 300 clinical encounters between HWs and patients of all ages. Quantitative and qualitative tools were used to collect data. There were a health facility checklist, an interview guide for health facility providers, a clinical observation guide, a community health volunteer CHV) interview guide, and a stakeholder interview guide.
To evaluate elimination readiness, a composite score was assigned to each HF catchment area that incorporates all survey responses based on commodity availability, malaria CM practices, data management, and supervision practices.
In preliminary results, 8 of 34 (24%) CHVs reported that they do not manage children under 5 years (CU5) with fever at the community level. Of 26 CHVs who care for CU5, 18 (69%) identified history of fever as a criterion for suspected malaria, 20 (77%) reported using a malaria rapid diagnostic test (RDT) when evaluating patients reporting fever, and 15 (58%) reported giving antimalarials for a positive RDT. Among treating CHVs, 13 (30%) reported having RDTs, and 11 (42%) reported having antimalarials currently available. A
 Among facility-based HWs, 83% identified history of fever as a criterion for a suspected case. Of 120 patients with reported or recorded fever, 56 (47%) were tested with an RDT. Five RDTs were positive; a first-line antimalarial was prescribed to 4 of those patients. This evaluation is a baseline for CM performance as Madagascar establishes elimination targets. In the evaluated districts, CM could be improved by strategies to increase testing at CHV and HF levels and address availability of commodity stocks in the community.
Among facility-based HWs, 83% identified history of fever as a criterion for a suspected case. Of 120 patients with reported or recorded fever, 56 (47%) were tested with an RDT. Five RDTs were positive; a first-line antimalarial was prescribed to 4 of those patients. This evaluation is a baseline for CM performance as Madagascar establishes elimination targets. In the evaluated districts, CM could be improved by strategies to increase testing at CHV and HF levels and address availability of commodity stocks in the community.
*Affiliations: Epidemic Intelligence Service, Malaria Branch, Division of Parasitic Diseases and Malaria, Center for Global Health, Centers for Disease Control and Prevention, Atlanta, GA, United States; Maternal Child Survival Program, Washington, DC, United States; US President’s Malaria Initiative; US Centers for Disease Control and Prevention, Antananarivo, Madagascar; Maternal Child Survival Program, Madagascar, Antananarivo, Madagascar; Maternal Child Survival Program, Antananarivo, Madagascar; US President’s Malaria Initiative, Antananarivo, Madagascar; Malaria Branch, Division of Parasitic Diseases and Malaria, Center for Global Health, Centers for Disease Control and Prevention, Atlanta, GA, United States; National Malaria Control Program, Antananarivo, Madagascar
Asymptomatic &Elimination &Eradication &Monkeys &Mosquitoes &Resistance &Vaccine Bill Brieger | 23 Aug 2019
Biology and Malaria Eradication: Are there Barriers?
During a press conference prior to the release of the executive summary of 3-year study of trends and future projections for the factors and determinants that underpin malaria by its Strategic Advisory Group on Malaria Eradication (SAGme), WHO outlined some hopeful signs emanating from the SAGme including
- Lack of biological barriers to malaria eradication
- Recognition of the massive social and economic benefits that would provide a return on investment in eradication, and
- Megatrends in the areas of factors such as land use, climate, migration, urbanization that could inhibit malaria transmission
 Concerning the first point, the executive summary notes that, “We did not identify biological or environmental barriers to malaria eradication. In addition, our review of models accounting for a variety of global trends in the human and biophysical environment over the next three decades suggest that the world of the future will have much less malaria to contend with.”
Concerning the first point, the executive summary notes that, “We did not identify biological or environmental barriers to malaria eradication. In addition, our review of models accounting for a variety of global trends in the human and biophysical environment over the next three decades suggest that the world of the future will have much less malaria to contend with.”
The group did agree that, “using current tools, we will still have 11 million cases of malaria in Africa in 2050.” So one wonders whether there are biological barriers or not.
Interestingly the group did identify, “Potential biological threats to malaria eradication include development of insecticide and antimalarial drug resistance, vector population dynamics and altered vector behaviour. For example, Anopheles vectors might adapt to breeding in polluted water, and mosquito vector species newly introduced to Africa, such as Anopheles stephensi, could spread more widely into urban settings.”
This discussion harkens back to an important conceptual article by Bruce Aylward and colleagues that raised the question in the American Journal of Public Health, “When Is a Disease Eradicable?” They outlined three important criteria that had been proposed at two international conferences in 1997 and 1998.
- biological and technical feasibility
- costs and benefits, and
- societal and political considerations
Their further expansion on the biological issues using smallpox as an example is instructive. They noted that not only are humans essential for the life cycle of the organism, but that there was no other reservoir for the causative virus, and the virus could not amplify in the environment. In short, there were no vectors, as in the case of malaria. The relatively recent documentation of transmission of malaria between humans and other primates of different plasmodium species is another biological concern. At this point, Malaysia, for example, is reporting more cases of Plasmodium knowlesi in humans that either P vivax or P falciparum.
Another biological issue identified by Aylward and colleagues was the fact that smallpox had one effective and proven intervention, the vaccine. Application of the vaccine could be targeted using photograph disease recognition cards as the signs were quite specific to the disease. Malaria has several effective interventions, but most strategies emphasize the importance of using a combination of these, and implementation is met with a number of management and logistical challenges. The signs and symptoms of malaria are confused with a number of febrile illnesses.
Finally, two other issues raised concern. Insecticide resistance was recognized in the first malaria eradication effort, and is raising its head again, as pointed out by SAGme. Comparing smallpox and yaws, the challenge of latent or sub-clinical/asymptomatic infection was mentioned. Malaria too, is beleaguered with this problem.
Clearly, we must not lose momentum in the marathon (not a race) to eliminate malaria, but we must, as WHO stressed at the press conference, increase our research and development efforts to strengthen existing tools and develop new once to address the biological and logistical challenges.
Borders &Diagnosis &Ebola &Elimination &Integrated Vector Management &ITNs &Mosquitoes &NTDs &Snakebite &Trachoma &Urban Bill Brieger | 04 Aug 2019
Tropical Health Update 2019-08-04: Ebola, Malaria Vectors, Snakebite and Trachoma
In the past week urban transmission in Goma, a city of at least 2 million inhabitants in eastern Democratic republic of Congo, was documented as a gold miner came home and infected his wife and child. To get a grip on the spread of the disease, DRC is considering another vaccine, not without some controversy. WHO provides detailed guidance on all aspects of response. On the malaria front we have learned more about malaria vectors, natural immunity and reactive case detection.
Ebola Challenges: Vaccines, Urban Transmission
 The current Ebola vaccine being deployed to over 150,000 people in North Kivu and Ituri Provinces was itself an experimental intervention during 2016 when it was first used in the largest ever outbreak located in West Africa. BBC reports that, “World Health Organization (WHO) data show the Merck vaccine has a 97.5% efficacy rate for those who are immunised, compared to those who are not.”
The current Ebola vaccine being deployed to over 150,000 people in North Kivu and Ituri Provinces was itself an experimental intervention during 2016 when it was first used in the largest ever outbreak located in West Africa. BBC reports that, “World Health Organization (WHO) data show the Merck vaccine has a 97.5% efficacy rate for those who are immunised, compared to those who are not.”
The proposed addition of a Johnson and Johnson vaccine would be in that same experimental phase if introduced in DRC now. It has been proven safe as well as effective in other primates. The challenge is that even though the Merck vaccine supplies are near 500,000, this is not enough to cover the potential needs in an area with over 10 million people, although Merck is still producing more. At present, BBC says, “Those pushing for the use of the new Johnson & Johnson vaccine, had proposed using it to create a protective wall, vaccinating people outside the outbreak zone.” In addition, the new national response team is concerned that “Only about 50% of cases of Ebola in the Democratic Republic of Congo are being identified.”
Finally, there is the issue of community mistrust of government workers and challenging logistics. “There are also concerns that the new vaccine – which requires two injections 56 days apart – may be difficult to administer in a region where the population is highly mobile, and insecurity is rife.”
If efforts at vaccination are needed soon in Goma, up to 2 million doses might be needed. Reuters reports that, “Congolese authorities were racing to contain an Ebola epidemic on Thursday, after a gold miner with a large family contaminated several people in the east’s main city of Goma before dying of the hemorrhagic fever.” Readers may recall that the West Africa outbreak of 2014-16 in Guinea, Sierra Leone and Liberia accelerated greatly after infected people went to major cities in search of help.
The miner is the second ‘imported case into Goma, which borders Rwanda, but because his family lives there, he has already infected his wife and one of his 10 children. Contacts are being traced and monitored, but this urban and border threat is one of the factors that led WHO to finally declare the current outbreak a public health emergency.
Malaria
As we move toward malaria elimination Reactive Case Detection (RCD) has been proposed as an integral part of these efforts with the hopes that is can be conceived of as a way of gradually decreasing transmission, according to an article in Malaria Journal. In fact, the value of RCD may be limited as follows:
- RCD alone can eliminate malaria in only a very limited range of settings, where transmission potential is very low
- In other settings, it is likely to reduce disease burden and help maintain the disease-free state in the face of imported infections
Another article looks at “natural exposure to gametocytes that can result in the development of immunity against the gametocyte by the host as well as genetic diversity in the gametocyte.” The researchers learned that there can be variations in immune response depending on season and geography. This information is helpful in planning malaria elimination interventions.
On the vector front a baseline susceptibility testing was conducted in 16 countries in sub-Saharan Africa for neonicotinoids. “The target site of neonicotinoids represents a novel mode of action for vector control, meaning that cross-resistance through existing mechanisms is less likely.” The findings will help in the preparation for rollout of clothianidin formulations as part of national IRS rotation strategies by PMI and other partners.
 Researchers also called on us to learn more about malaria vectors in other parts of the world. In order to eliminate Plasmodium falciparum from the Caribbean and Central America program planners should consider local vector characteristics such as An. albimanus. They found that, “House-screening and repellent IRS are potentially highly effective against An. albimanus if people are indoors during the evening.”
Researchers also called on us to learn more about malaria vectors in other parts of the world. In order to eliminate Plasmodium falciparum from the Caribbean and Central America program planners should consider local vector characteristics such as An. albimanus. They found that, “House-screening and repellent IRS are potentially highly effective against An. albimanus if people are indoors during the evening.”
Vectors are also of concern on the edges of malaria transmission, particularly in South Africa, one of the ‘elimination eight’ countries of the Southern Africa Development Community. Researchers examined the, “potential role of Anopheles parensis and other Anopheles species in residual malaria transmission, using sentinel surveillance sites in the uMkhanyakude District of northern KwaZulu-Natal Province.” They found Anopheles parensis is a potential but minimal vector of malaria in South Africa “owing to its strong zoophilic tendency.” On the other hand, An. arabiensis was found to be the major vector responsible for residual malaria transmission in South Africa. Since these mosquitoes were found in outdoor-placed resting traps, interventions are needed to control outdoor-resting of vector populations.
NTDs of Concern
During the week, the member states of the African Union renewed their commitment to fight and permanently eliminate Neglected Tropical Diseases. Africa.com reported that, “Achievements to date include 1 billion people treated against at least one NTD and 37 countries have completed the removal of at least one NTD.”
Although some reports have discounted the idea of trachoma in Namibia, there may be reason to re-examine the situation. On Twitter Anthony Solomon notes that Namibia needs #trachoma prevalence surveys. A just-completed joint Ministry of Health & Social Services/@WHO mission found active trachoma & trichiasis in Zambezi & Kunene Regions.
 The Times of India draws attention to snakebite. It says that “Under-reported and inadequately treated, fatalities in India are estimated at close to 50,000 a year, the world’s highest.”
The Times of India draws attention to snakebite. It says that “Under-reported and inadequately treated, fatalities in India are estimated at close to 50,000 a year, the world’s highest.”
Overall we can see that the concept of ‘neglect’ has several uses. There is neglect if half of Ebola cases are undetected. There is neglect if we do not understand malaria vectors in low transmission areas. Finally, there is neglect if we do not conduct up-to-date disease surveys to determine whether a disease is present or not. Elimination of tropical diseases is challenging when key processes are neglected.
Borders &Diagnosis &Elimination &Environment &Gender &Health Education &Health Workers &Indoor Residual Spraying &IRS &ITNs &Mosquitoes &Plasmodium/Parasite &Vector Control Bill Brieger | 07 Jul 2019
The Weekly Tropical Health News 2019-07-06: Eliminating Malaria in Low Transmission Settings
This week started with articles that drew attention to the challenges of malaria in low transmission areas and with low density infections. Malaria Journal has provided several insightful articles toward this end.
 Being an island has certainly helped Zanzibar make progress toward malaria elimination as witness the fact that malaria prevalence has remained below 1% for the past decade. Not only does Zanzibar still face threats of infection from the mainland, it may also experience an upsurge locally if residual transmission and the role of human behavior and community actions are not well understood. April Monroe et al. conducted in-depth interviews with community members and local leaders across six sites on Unguja, Zanzibar as well as semi-structured community observations of night-time activities and special events to learn more.
Being an island has certainly helped Zanzibar make progress toward malaria elimination as witness the fact that malaria prevalence has remained below 1% for the past decade. Not only does Zanzibar still face threats of infection from the mainland, it may also experience an upsurge locally if residual transmission and the role of human behavior and community actions are not well understood. April Monroe et al. conducted in-depth interviews with community members and local leaders across six sites on Unguja, Zanzibar as well as semi-structured community observations of night-time activities and special events to learn more.
While there was high reported ITN use, there were also times when people were exposed t mosquitoes while being outdoors during biting times. This could be around the house, or at special night events like such as weddings, funerals, and religious ceremonies. Men spent more time outdoors than women. Clearly appropriate interventions and needed and should be promoted in culturally appropriate ways in order to further reduce and eventually eliminate transmission.
Angela Early and colleagues presented findings on a diagnostic process of deep sequencing for understanding the dynamics and complexity of Plasmodium infections, but stress that knowing the lower limit of detection is challenging. They present “a new amplicon analysis tool, the Parallel Amplicon Sequencing Error Correction (PASEC) pipeline, is used to evaluate the performance of amplicon sequencing on low-density Plasmodium DNA samples.”
The authors learned that, “four state-of-the-art tools resolved known haplotype mixtures with similar sensitivity and precision.” They also cautioned that, “Samples with very low parasitemia and very low read count have higher false positive rates and call for read count thresholds that are higher than current default recommendations.” Better understanding of the genetic mix of plasmodium infections as countries move toward low transmission and elimination is crucial for selecting appropriate interventions and evaluating their outcomes.
 Hannah Edwards and co-researchers examined conditions for malaria transmission along the Thailand-Myanmar border in areas approaching malaria elimination. While prevalence may be less than 1%, residual transmission still occurs. Transmission occurs not only around residences but in the forests where people work. The researchers therefore looked at the behavior of both humans and insects. Overall, they found that, “Community members frequently stayed overnight at subsistence farm huts or in the forest. Entomological collections showed higher biting rates of primary vectors in forested farm hut sites and in a more forested village setting compared to a village with clustered housing and better infrastructure.”
Hannah Edwards and co-researchers examined conditions for malaria transmission along the Thailand-Myanmar border in areas approaching malaria elimination. While prevalence may be less than 1%, residual transmission still occurs. Transmission occurs not only around residences but in the forests where people work. The researchers therefore looked at the behavior of both humans and insects. Overall, they found that, “Community members frequently stayed overnight at subsistence farm huts or in the forest. Entomological collections showed higher biting rates of primary vectors in forested farm hut sites and in a more forested village setting compared to a village with clustered housing and better infrastructure.”
While mosquitoes preferred to bite inside huts, their threat was magnified by those who did not use long lasting insecticide-treated nets (LLINs). While out in the farms and forests, people tended to wake early and increase their likelihood of being bitten. The authors discuss the challenges of dual residences in terms of LLIN ownership and even concerning the potential access to indoor residual spraying. The definition for universal net coverage needs to expand from one net per two people to include adequate nets wherever people are located.
 The Amazonian area of Brazil is another area working toward malaria elimination, in particular, Plasmodium vivax. Felipe Leão Gomes Murta et al. also looked at the human side of the equation and identified misperceptions by both community members and health workers that could inhibit elimination efforts. They found, “many myths regarding malaria transmission and treatment that may hinder the sensitization of the population of this region in relation to the use of current control tools and elimination strategies, such as mass drug administration (MDA),” and LLINs.
The Amazonian area of Brazil is another area working toward malaria elimination, in particular, Plasmodium vivax. Felipe Leão Gomes Murta et al. also looked at the human side of the equation and identified misperceptions by both community members and health workers that could inhibit elimination efforts. They found, “many myths regarding malaria transmission and treatment that may hinder the sensitization of the population of this region in relation to the use of current control tools and elimination strategies, such as mass drug administration (MDA),” and LLINs.
Problematic perceptions included mention by both groups that the use of insecticide-treated nets, may cause skin irritations and allergies. Both community members and health professionals said malaria is “an impossible disease to eliminate because it is intrinsically associated with forest landscapes.” They concluded that such perceptions can be a barrier to control and elimination.
Efforts to eliminate malaria from low transmission settings are an essential to the overall global goals. These four articles tell us that close attention to and better understanding of humans, parasites and mosquitoes is still needed to achieve these goals.
Asymptomatic &Burden &Dengue &Diagnosis &Ebola &Elimination &Epidemiology &Health Systems &ITNs &MDA &Mosquitoes &NTDs &Schistosomiasis &Schools &Vector Control &Zoonoses Bill Brieger | 30 Jun 2019
The Weekly Tropical Health News 2019-06-29
Below we highlight some of the news we have shared on our Facebook Tropical Health Group page during the past week.
Polio Persists
If all it took to eradicate a disease was a well proven drug, vaccine or technology, we would not be still reporting on polio, measles and guinea worm, to name a few. In the past week Afghanistan reported 2 wild poliovirus type 1 (WPV1) cases, and Pakistan had 3 WPV1 cases. Circulating vaccine-derived poliovirus type 2 (cVDPV2) was reported in Nigeria (1), DRC (4) and Ethiopia (3) from healthy community contacts.
Continued Ebola Challenges
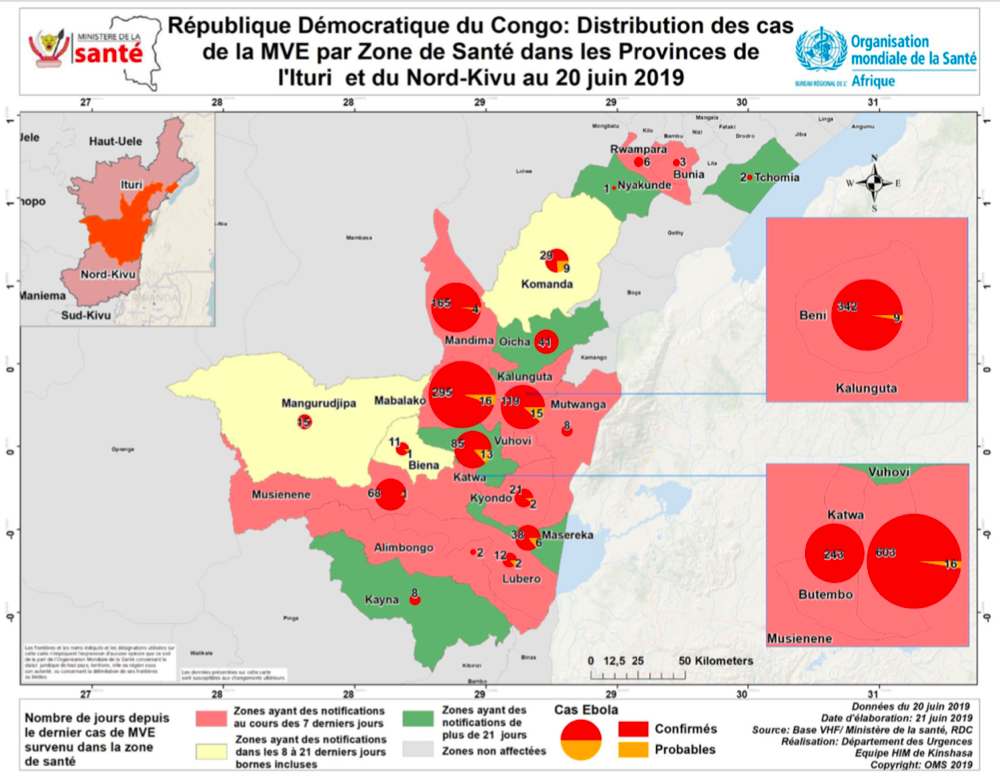
In the seven days from Saturday to Friday (June 28) there were 71 newly confirmed Ebola Cases and 56 deaths reported by the Democratic Republic of Congo’s Ministry of Health. As Ebola cases continue to pile up in the Democratic Republic of the Congo (DRC), with 12 more confirmed Thursday and 7 more Friday, a USAID official said four major donors have jump-started a new strategic plan for coordinating response efforts. To underscore the heavy toll the outbreak has caused, among its 2,284 cases, as noted on the World Health Organization Ebola dashboard today, are 125 infected healthcare workers, including 2 new ones, DRC officials said.
Pacific Standard explained the differences in Ebola outbreaks between DRC today and the West Africa outbreak of 2014-16. On the positive side are new drugs used in organized trials for the current outbreak. The most important factor is safe, effective vaccine that has been tested in 2014-16, but is now a standard intervention in the DRC. While both Liberia and Sierra Leone had health systems and political weaknesses as post-conflict countries, DRC’s North Kivu and Ituri provinces are currently a war zone, effectively so for the past generation. Ebola treatment centers and response teams are being attacked. There are even cultural complications, a refusal to believe that Ebola exists. So even with widespread availability of improved technologies, teams may not be able to reach those in need.
To further complicate matters in the DRC, Doctors Without Borders (MSF) “highlighted ‘unprecedented’ multiple crises in the outbreak region in northeastern DRC. Ebola is coursing through a region that is also seeing the forced migration of thousands of people fleeing regional violence and is dealing with another epidemic. Moussa Ousman, MSF head of mission in the DRC, said, ‘This time we are seeing not only mass displacement due to violence but also a rapidly spreading measles outbreak and an Ebola epidemic that shows no signs of slowing down, all at the same time.’”
NIPAH and Bats
Like Ebola, NIPAH is zoonotic, and also involves bats, but the viruses differ. CDC explains that, “Nipah virus (NiV) is a member of the family Paramyxoviridae, genus Henipavirus. NiV was initially isolated and identified in 1999 during an outbreak of encephalitis and respiratory illness among pig farmers and people with close contact with pigs in Malaysia and Singapore. Its name originated from Sungai Nipah, a village in the Malaysian Peninsula where pig farmers became ill with encephalitis.
A recent human outbreak in southern India has been followed up with a study of local bats. In a report shared by ProMED, out of 36 Pteropus species bats tested for Nipah, 12 (33%) were found to be positive for anti-Nipah bat IgG antibodies. Unlike Ebola there are currently no experimental drugs or vaccines.
Climate Change and Dengue
Climate change is expected to heighten the threat of many neglected tropical diseases, especially arboviral infections. For example, the New York Times reports that increases in the geographical spread of dengue fever. Annually “there are 100 million cases of dengue infections severe enough to cause symptoms, which may include fever, debilitating joint pain and internal bleeding,” and an estimated 10,000 deaths. Dengue is transmitted by Aedes mosquitoes that also spread Zika and chikungunya. A study, published Monday in the journal Nature Microbiology, found that in a warming world there is a strong likelihood for significant expansion of dengue in the southeastern United States, coastal areas of China and Japan, as well as to inland regions of Australia. “Globally, the study estimated that more than two billion additional people could be at risk for dengue in 2080 compared with 2015 under a warming scenario.”
Schistosomiasis – MDA Is Not Enough, and Neither Are Supplementary Interventions
Schistosomiasis is one of the five neglected tropical diseases (NTDs) that are being controlled and potentially eliminated through mass drug administration (MDA) of preventive chemotherapy (PCT), in this case praziquantel. In The Lancet Knopp et al. reported that biannual MDA substantially reduced Schistosomiasis haematobium prevalence and infection intensity but was insufficient to interrupt transmission in Zanzibar. In addition, neither supplementary snail control or behaviour change activities did not significantly boost the effect of MDA. Most MDA programs focus on school aged children, and so other groups in the community who have regular water contact would not be reached. Water and sanitation activities also have limitations. This raises the question about whether control is acceptable for public health, or if there needs to be a broader intervention to reach elimination?
Trachoma on the Way to Elimination
Speaking of elimination, WHO has announced major “sustained progress” on trachoma efforts. “The number of people at risk of trachoma – the world’s leading infectious cause of blindness – has fallen from 1.5 billion in 2002 to just over 142 million in 2019, a reduction of 91%.” Trachoma is another NTD that uses the MDA strategy.
The news about NTDs from Dengue to Schistosomiasis to Trachoma is complicated and demonstrates that putting diseases together in a category does not result in an easy choice of strategies. Do we control or eliminate or simply manage illness? Can our health systems handle the needs for disease elimination? Is the public ready to get on board?
Malaria Updates
And concerning being complicated, malaria this week again shows many facets of challenges ranging from how to recognize and deal with asymptomatic infection to preventing reintroduction of the disease once elimination has been achieved. Several reports this week showed the particular needs for malaria intervention ranging from high burden areas to low transmission verging on elimination to preventing re-introduction in areas declared free from the disease.
In South West, Nigeria Dokunmu et al. studied 535 individuals aged from 6 months were screened during the epidemiological survey evaluating asymptomatic transmission. Parasite prevalence was determined by histidine-rich protein II rapid detection kit (RDT) in healthy individuals. They found that, “malaria parasites were detected by RDT in 204 (38.1%) individuals. Asymptomatic infection was detected in 117 (57.3%) and symptomatic malaria confirmed in 87 individuals (42.6%).
Overall, detectable malaria by RDT was significantly higher in individuals with symptoms (87 of 197/44.2%), than asymptomatic persons (117 of 338/34.6%)., p = 0.02. In a sub-set of 75 isolates, 18(24%) and 14 (18.6%) individuals had Pfmdr1 86Y and 1246Y mutations. Presence of mutations on Pfmdr1 did not differ by group. It would be useful for future study to look at the effect of interventions such as bednet coverage. While Southwest Nigeria is a high burden area, the problem of asymptomatic malaria will become an even bigger challenge as prevalence reduces and elimination is in sight.
Sri Lanka provides a completely different challenge from high burden areas. There has been no local transmission of malaria in Sri Lanka for 6 years following elimination of the disease in 2012. Karunasena et al. report the first case of introduced vivax malaria in the country by diagnosing malaria based on microscopy and rapid diagnostic tests. “The imported vivax malaria case was detected in a foreign migrant followed by a Plasmodium vivax infection in a Sri Lankan national who visited the residence of the former. The link between the two cases was established by tracing the occurrence of events and by demonstrating genetic identity between the parasite isolates. Effective surveillance was conducted, and a prompt response was mounted by the Anti Malaria Campaign. No further transmission occurred as a result.”
Bangladesh has few but focused areas of malaria transmission and hopes to achieve elimination of local transmission by 2030. A particular group for targeting interventions is the population of slash and burn cultivators in the Rangamati District. Respondents in this area had general knowledge about malaria transmission and modes of prevention and treatment was good according to Saha and the other authors. “However, there were some gaps regarding knowledge about specific aspects of malaria transmission and in particular about the increased risk associated with their occupation. Despite a much-reduced incidence of malaria in the study area, the respondents perceived the disease as life-threatening and knew that it needs rapid attention from a health worker. Moreover, the specific services offered by the local community health workers for malaria diagnosis and treatment were highly appreciated. Finally, the use of insecticide-treated mosquito nets (ITN) was considered as important and this intervention was uniformly stated as the main malaria prevention method.”
Kenya offers some lessons about low transmission areas but also areas where transmission may increase due to climate change. A matched case–control study undertaken in the Western Kenya highlands. Essendi et al. recruited clinical malaria cases from health facilities and matched to asymptomatic individuals from the community who served as controls in order to identify epidemiological risk factors for clinical malaria infection in the highlands of Western Kenya.
“A greater percentage of people in the control group without malaria (64.6%) used insecticide-treated bed nets (ITNs) compared to the families of malaria cases (48.3%). Low income was the most important factor associated with higher malaria infections (adj. OR 4.70). Houses with open eaves was an important malaria risk factor (adj OR 1.72).” Other socio-demographic factors were examined. The authors stress the need to use local malaria epidemiology to more effectively targeted use of malaria control measures.
The key lesson arising from the forgoing studies and news is that disease control needs strong global partnerships but also local community investment and adaptation of strategies to community characteristics and culture.
Borders &Diagnosis &Ebola &Elimination &Eradication &Health Systems &Measles &Surveillance &Vaccine &Yaws Bill Brieger | 22 Jun 2019
The Weekly Tropical Health News Update 2019-06-22
For almost 20 years we have been maintaining an email list where current news and articles have been shared with those interested in tropical health and malaria. The listserve host we have been using is changing to a paid model. While there are still some free listserve options, these are cumbersome to produce. Since we are already maintaining this blog, we thought it best to provide a weekly summary of key news events through this medium.
Mapping Plasmodium Vivax
The Malaria Atlas Project has published in The Lancet a global burden of Plasmodium Vivax mapping study. The authors describe the contribution of this study as: “Our study highlights important spatial and temporal patterns in the clinical burden and prevalence of P vivax. Amid substantial progress worldwide, plateauing gains and areas of increased burden signal the potential for challenges that are greater than expected on the road to malaria elimination. These results support global monitoring systems and can inform the optimisation of diagnosis and treatment where P vivax has most impact.”
Ebola Spread from DRC to Uganda
 Since the major ongoing outbreak of Ebola Virus Disease in North Kivu and Ituri Provinces of the Democratic Republic of Congo (DRC) started nearly a year ago, there has been concern that the disease might spread to neighboring countries like Uganda, Rwanda, South Sudan and the Central African Republic. This fear same true recently when a family affected by Ebola crossed from DRC into Uganda to connect with relatives in Kasese District Uganda. Uganda has had many years’ experience dealing with Ebola and was able to contain the situation.
Since the major ongoing outbreak of Ebola Virus Disease in North Kivu and Ituri Provinces of the Democratic Republic of Congo (DRC) started nearly a year ago, there has been concern that the disease might spread to neighboring countries like Uganda, Rwanda, South Sudan and the Central African Republic. This fear same true recently when a family affected by Ebola crossed from DRC into Uganda to connect with relatives in Kasese District Uganda. Uganda has had many years’ experience dealing with Ebola and was able to contain the situation.
A press release this week noted that, “As of today (21 June 2019), Uganda has not registered any new confirmed Ebola Virus Disease (EVD) case in Kasese District or any other part of Uganda since the last registered case one week ago. There are no new suspect cases under admission. Currently, 110 contacts to the confirmed Ebola cases in Kagando and Bwera are being followed up daily. A total of 456 individuals have been vaccinated against EVD using the Ebola-rVSV vaccine in Kasese District, Western Uganda.”
Although many people expected that the meeting of the “International Health Regulations (2005) Emergency Committee} for Ebola virus disease in the Democratic Republic of the Congo would finally declare the current outbreak a Public Health Emergency of International Concern (PHEIC) because it crossed a border, the result was noting that the challenge was still an emergency only for DRC. WHO did note that there were serious funding gaps and support from other countries for the DRC’s predicament. Ironically, such gaps make it more likely that Ebola can spread more widely.
As of 21 June 2019, the DRC reported a total of 2,211 cases since the start of the epidemic last year, of which 2,117 have been confirmed and 94 are probable. There have been 1,489 deaths. To date 139,027 persons have been vaccine with the Merck rVSV-ZEBOV vaccine.
Progress toward Eliminating Malaria – the E-2020 Countries
 The process of eliminating malaria from the world needs to start in a step-by-step fashion. WHO explained that, “Creating a malaria-free world is a bold and important public health and sustainable development goal. It is also the vision of the Global technical strategy for malaria 2016-2030, which calls for the elimination of malaria in at least 10 countries by the year 2020.”
The process of eliminating malaria from the world needs to start in a step-by-step fashion. WHO explained that, “Creating a malaria-free world is a bold and important public health and sustainable development goal. It is also the vision of the Global technical strategy for malaria 2016-2030, which calls for the elimination of malaria in at least 10 countries by the year 2020.”
Actually, WHO identified 21 countries, spanning 5 regions, that could defeat malaria by 2020. The progress report charts the effort. During the recent World Health Assembly two countries received recognition for being certified malaria-free, Argentina and Algeria. This week WHO also announced that 5 more countries have not had malaria cases in the past year. There was also release of a downloadable report on progress toward the 2020 target for selected countries.
Reconsidering Yaws Eradication
In the 1950s and 1960s the world focused on the possibility of eradicating Yaws through screening and treatment interventions. Like the early malaria eradication programs from the same period, the Yaws effort slowed, stopped and experienced a resurgence. The Telegraph reported that, “Between 1952 and 1964, Unicef and the WHO screened some 300 million people for the illness, in a coordinated programme which treated more than 50 million cases. Yaws was on the brink of being wiped out and reports of the disease dropped by 95 per cent.” WHO continues to work on treatment strategies with azithromycin and for resistant cases, benzathine benzylpenicillin injection.
WHO noted that there were 80,472 cases reported in 2018, although this figure is likely to be much higher in actuality. The challenge of case detection exists but may be overcome, according to the Telegraph with a new molecular rapid diagnostic test which detects yaws within 30 minutes, and thus could allow on-the-spot diagnosis in remote regions.
Measles Cases Continue to Increase
The problem of measles in the DRC may not be receiving much attention because of the Ebola epidemic. Ironically, Outbreak News Today reports that, “In a follow-up on the measles outbreak in the Democratic Republic of the Congo (DRC), UN health officials report an additional 7500 suspect cases in the past 2 weeks, bringing the total cases since the beginning of the year to 106,870. The death toll due to the measles outbreak has reached 1815 deaths (case fatality ratio 1.7%).”
Vaccine coverage challenges in the DRC result from health systems weaknesses. Unfortunately, a global study has shown that increasing cases in the Global North are not due to weak systems, but ‘vaccine hesitancy.’ The Guardian reports that a global survey has revealed the scale of the crisis of confidence in vaccines in Europe, “showing that only 59% of people in western Europe and 50% in the east think vaccines are safe, compared with 79% worldwide.” The Guardian observes that, “In spite of good healthcare and education systems, in parts of Europe there is low trust in vaccines. France has the highest levels of distrust, at 33%.”
For more news and daily updates check our other services, a closed/private Facebook Group and a Twitter feed. For those who do not use social media, please check here each weekend to find a summary of some of the stories we have shared during the week.
Asymptomatic &Case Management &Diagnosis &Elimination &Ivermectin &Surveillance &Uncategorized Bill Brieger | 30 Jan 2019
Asymptomatic Malaria – we need to eliminate what we can’t see
After the World’s first attempt at eradicating the complicated disease malaria mainly through a single tool, a period of control set in where the aim was to reduce mortality through prompt and presumptive treatment of fevers with anti-malarials, particularly in young children. During this period in the 1980s and 1990s it was recognized that parasite-based diagnostic capabilities in the form of microscopy were limited, so in malaria endemic areas, it was worth providing inexpensive medicines like chloroquine (CQ) and sulfadoxine-pyrimethamine (SP) to febrile children in order to save lives. When the fevers did not resolve, other illnesses explored.
The difficulty arose in identifying cases that did not offer clinical clues that they might be malaria. Today countries approaching malaria elimination face challenges, such as seen in Zanzibar where, “outdoor transmission, a large asymptomatic parasite reservoir and imported infections, require novel tools and reoriented strategies to prevent a rebound effect and achieve elimination.”[i] Here we examine the challenge of asymptomatic malaria infections.

Background
By 1998 when the Roll Back Malaria partnership formed, there had been enough research done so that the malaria community had a better arsenal of interventions including insecticide-treated bed nets, artemisinin-based combination therapy (ACT) and intermittent preventive treatment with SP during pregnancy. The Abuja Declaration of 2000 set a target of 80% coverage of these interventions by the year 2010.
While ACTs overcame the challenges of parasite resistance that had developed for the single drugs, CQ and SP, it cost several times more than those medicines. The need for easy-to-use, inexpensive, point-of-care diagnostics was recognized so that not only would ACTs be targeted only to parasitologically confirmed malaria cases, but also in the process, overuse and misuse would not contribute to parasite resistance of these new drugs.[ii] Unfortunately, the development and dissemination of antigen-based rapid diagnostic tests (RDTs), lagged behind the availability of ACTs meaning that health workers unfortunately continued their business as usual with presumptive treatment using ACTs.
The benefits of RDTs were generally two-fold. First, they could be used by front-line, auxiliary and community-based health workers. Secondly, they tended to identify more cases than microscopy. The big challenge was convincing health workers to use them and trust the results, because the era of presumptive treatment had given these staff a false sense of confidence in their own clinical diagnostic abilities.

Although reaching the 2010 coverage targets has remained illusive for most endemic countries, there has been enough progress for major reductions in incidence (despite a recent upsurge).[iii] As the proportion of actual malaria cases among febrile illness patients declines, concern has risen that transmission might continue among people with subclinical or asymptomatic malaria. Here we explore the extent of this problem and new directions in parasitological testing needed to ensure continued progress toward elimination in each endemic country.
Understanding the Risk of Asymptomatic Malaria
Risk can relate to geographical, epidemiological, and socio-demographic factors as well as history of malaria interventions. Kenya has stratified the country by higher and lower malaria transmission areas. Even the higher areas are comparatively low compared to its higher transmission neighbors. Studying the prevalence of asymptomatic malaria in some of these higher transmission areas in the west of the country was seen as a way to better identify people at risk and learn about intervention effectiveness. An examination of apparently healthy children (no symptoms) revealed a Plasmodium falciparum malaria prevalence 36.0% (27.5%, 44.5%) by RDT and 22.3% (16.0%, 28.6%) by thick film microscopy.[iv] Living in a household with electricity was protective but the adjusted odds ratio of prevalence comparing households with and without indoor residual spray showed only borderline benefit. Unfortunately, in Zanzibar, asymptomatic malaria infection was not associated “with use of any vector control.”1
A major challenge in detecting cases through routine health care systems is care seeking patterns of care seeking for fever. The 2018 World Malaria Report acknowledges that there are major equity challenges in care seeking wherein families with higher incomes, better education and living in urban areas are more likely to seek help for their febrile children that rural, poor and less educated families who would be more at risk. Care seeking without the signs of fever is more challenging. A dual strategy of enabling better service utilization as well as outreach to detect cases will be necessary to detect asymptomatic cases.3
In Burkina Faso, the prevalence of asymptomatic malaria infection in children under 5 years of age was estimated at 38.2% in 24 of its 70 health districts. Those at most risk for asymptomatic malaria infection included the following:[v]
- older children (48–59 vs < 6 months: OR: 6.79 [5.62, 8.22])
- children from very poor households (Richest vs poorest: OR: 0.85 [0.74–0.96])
- households located more than 5 km from a health facility (< 5 km vs ? 5 km: OR: 1.14 [1.04–1.25])
- localities with inadequate number of nurses (< 3 vs ? 3: 0.72 [0.62, 0.82]
- rural areas (OR: 1.67 [1.39–2.01])
Nine districts reported significantly higher risks (Batié, Boromo, Dano, Diébougou, Gaoua, Ouahigouya, Ouargaye, Sapouy and Toma. The researchers concluded that, “Such national spatial analysis should help to prioritize areas for increased malaria control activities.”
A study in Ghana found that, “children and pregnant women had higher prevalence of submicroscopic gametocytes (39.5% and 29.7%, respectively) compared to adults
(17.4%).”[vi]

An additional concern is emerging in terms of sharing of malaria parasite species between humans and primates, especially as urbanization and deforestation push these two populations into closer contact. For example Mapua and colleagues working in Central Africa Republic, “found the human malaria parasite P. ovale wallikeri in both asymptomatic humans and western lowland gorillas in Dzanga Sangha Protected Areas. Molecular analysis revealed that the genotype of the P. ovale wallikeri DNA found in a gorilla was genetically identical to that of a human isolate within the mt cytb and mt cox 1 genes, indicating potential human–ape transmission.”[vii] They noted similar sharing of parasites in the region between humans and chimpanzees.
Detecting and Responding to Asymptomatic Cases
WHO’s Framework for Malaria Elimination[viii] recognizes the important role of case detection and subsequent treatment as well as broader community level preventive responses around detected cases. In the context of elimination WHO notes that case detection “requires use of a diagnostic test to identify asymptomatic malaria infections.” WHO stresses that a case is a case, regardless of whether it is symptomatic or asymptomatic, as long as the diagnostic process confirms presence of malaria infection.
It is important to monitor Plasmodium parasitemia in areas where malaria transmission has declined and efforts to achieve malaria elimination are underway, such as Zambia, where 3,863 household members were tested.[ix] Only 2.6% were positive by either microscopy, RDT, or PCR. Of these, 48 (47%) had subpatent parasitemia, and 85% of those with subpatent parasitemia were asymptomatic. “Compared with individuals without parasitemia, individuals with subpatent parasitemia were significantly more likely to be aged 5–25 years.” The authors suggested that their findings pointed to the need for active or reactive case detection to identify asymptomatic individuals and thus better target individuals with subpatent parasitemia with appropriate malaria interventions.
WHO explains that active case detection (ACD) takes place in areas of limited or under-utilization of health care services.4 It may start with initial screening for symptoms, followed by appropriate parasitological laboratory confirmation. In low-transmission settings or as part of a focus investigation, “ACD may consist of testing of a defined population group without prior symptom screening (population-wide or mass testing) in order to identify asymptomatic infections.” Elimination cannot be achieved until even asymptomatic infections have stopped. The challenge is the expense of community-wide screening.
Reactive Case Detection (RCD), according to WHO, takes place in settings low transmission intensity where the few “occurring malaria cases are highly aggregated.”4 When a case is identified, usually through identification of an actual infected patient at a local clinic, the community where the patient comes from is visited and a “net is cast around the index case” where household members and neighbors within a selected radius are tested. In this process asymptomatic cases are also identified.

Our existing diagnostic tools may be inadequate. McCreesh and colleagues reported on subpatent malaria in Namibia that, “fever history and standard RDTs are not useful to address this burden. Achievement of malaria elimination may require active case detection using more sensitive point-of-care diagnostics or presumptive treatment and targeted to high-risk groups.” This includes loop-mediated isothermal amplification (LAMP) using dried blood spots, which they tested.[x] Likewise from experience in a Zambian study, Kobayashi and co-researchers suggest, “more sensitive diagnostic tests or focal drug administration may be necessary to target individuals with subpatent parasitemia to achieve malaria elimination.”[xi]
Responses to detecting asymptomatic cases start at the individual level with prompt treatment of those found through RCD to be infected. Then focused preventive interventions such as distribution of insecticide treated bednets can be provided to those in the cluster or village. Follow-up would be needed for such ‘hot spots.’

On a broader basis we have Seasonal Malaria Chemoprevention (SMC) as practiced in Sahelian countries where during the peak transmission (rainy) season intermittent preventive treatment is given to children monthly by community health workers and volunteers. Of course, many of these children would be asymptomatic carriers and SMC could benefit the reduction of parasites in circulation. At present SMC focuses on pre-school aged children, but Thera and co-researchers stress the importance of reaching school aged children who are also often asymptomatic carriers.[xii]
Another intervention being tested for mass drug administration (MDA) use providing the community with ivermectin, a drug that has been highly effective in controlling filarial diseases and also found to kill mosquitoes who take a blood meal from a person who has recently taken it.[xiii] This strategy is still being tested, but again MDA means all community members, especially those with asymptomatic infection, would be reached.
A major question requires further research. To what extent
do asymptomatic, submicroscopic and subpatent parasitemia contribute to
continued malaria transmission? Another question is how can we address malaria
infection in other primates? We know that scientists recommend targeting of
malaria elimination interventions based on mapping of these infections.5
We therefore need to study the actual transmission potential of this
phenomenon.
[i] Björkman A, Shakely D, Ali AS, Morris U, Mkali H, Abbas AK, Al-Mafazy A-W, Haji KA, Mcha J, Omar R, Cook J, Elfving K, Petzold M, Sachs MC, Aydin-Schmidt B, Drakeley V, Msellem M and Mårtensson A. From high to low malaria transmission in Zanzibar—challenges and opportunities to achieve elimination. BMC Medicine (2019) 17:14, https://doi.org/10.1186/s12916-018-1243-z
[ii] Global Malaria Programme. Universal access to malaria diagnostic testing – An operational manual. World Health Organization. November 2011 (rev. February 2013). https://www.who.int/malaria/publications/atoz/9789241502092/en/
[iii] Global Malaria Programme. World malaria report 2018. World Health Organization. 19 November 2018. https://www.who.int/malaria/publications/world-malaria-report-2018/en/
[iv] Peprah S, Tenge C, Genga IO, Mumia M, Were PA, Kuremu RT, Wekes WN, Sumba PO, Kinyera T, Otim T, Legason ID, Biddle J, Reynolds SJ, Talisuna AO, Biggar1 RJ, Bhatia K, Goedert JJ, Pfeiffer RM, Mbulaiteye SM. A Cross-Sectional Population Study of Geographic, Age-Specific, and Household Risk Factors for Asymptomatic Plasmodium falciparum Malaria Infection in Western Kenya. The American Journal of Tropical Medicine and Hygiene, Volume 100, Issue 1, Jan 2019, p.54-65. DOI: https://doi.org/10.4269/ajtmh.18-0481.
[v] Ouédraogo M, Samadoulougou S, Rouamba T, Hien H, Sawadogo JEM Tinto H, Alegana VA, Speybroeck N and Kirakoya?Samadoulougou F. Spatial distribution and determinants of asymptomatic malaria risk among children under 5 years in 24 districts in Burkina Faso. Malaria Journal 2018; 17:460 https://doi.org/10.1186/s12936-018-2606-9
[vi] Lamptey H, Ofori MF, Kusi KA, Adu B, Owusu-Yeboa E, Kyei-Baafour E, Arku AT, Bosomprah S, Alifrangis M, Quakyi IA. The prevalence of submicroscopic Plasmodium falciparum gametocyte carriage and multiplicity of infection in children, pregnant women and adults in a low malaria transmission area in Southern Ghana. Malar J. 2018 Sep 17;17(1):331. doi: 10.1186/s12936-018-2479-y.
[vii] Mapua MI, Hans-Peter Fuehrer HP, Petrželková KJ, Todd A, Noedl H, Qablan MA, and Modrý D. Plasmodium ovale wallikeri in Western Lowland Gorillas and Humans Central African Republic. Emerging Infectious Disease journal. Volume 24, Number 8—August 2018. https://wwwnc.cdc.gov/eid/article/24/8/18-0010_article
[viii] Global Malaria Programme. A framework for malaria elimination. ISBN 978-92-4-151198-8. World Health Organization 2017, http://www.who.int/malaria/publications/atoz/9789241511988/en/
[ix] Kobayashi T, Kanyangarara M, Laban NM, Phiri M, Hamapumbu H, Searle KM, Stevenson JC, Thuma PE, Moss WJ and the Southern Africa International Centers of Excellence for Malaria Research. Characteristics of Subpatent Malaria in a Pre-Elimination Setting in Southern Zambia. The American Journal of Tropical Medicine and Hygiene, 10 December 2018, DOI: https://doi.org/10.4269/ajtmh.18-0399
[x] McCreesh P, Mumbengegwi D, Roberts K, Tambo M, Smith J, Whittemore B, Kelly G, Moe C, Murphy M, Chisenga M, Greenhouse B, Ntuku H, Kleinschmidt I, Sturrock H, Uusiku P, Gosling R, Bennett A, Hsiang MS. Subpatent malaria in a low transmission African setting: a cross-sectional study using rapid diagnostic testing (RDT) and loop-mediated isothermal amplification (LAMP) from Zambezi region, Namibia. Malar J. 2018 Dec 19;17(1):480. doi: 10.1186/s12936-018-2626-5.
[xi] Kobayashi T, Kanyangarara M, Laban NM, Phiri M, Hamapumbu H, Searle KM, Stevenson JC, Thuma PE, Moss WJ, For The Southern Africa International Centers Of Excellence For Malaria Research.Characteristics of Subpatent Malaria in a Pre-Elimination Setting in Southern Zambia. Am J Trop Med Hyg. 2018 Dec 10. doi: 10.4269/ajtmh.18-0399. [Epub ahead of print]
[xii] Thera MA, Konea AK, Tangaraa B, Diarraa E, Niarea A, Dembeleb A, Sissokoa MS, Doumboa OK. School-aged children based seasonal malaria chemoprevention using artesunate-amodiaquine in Mali. Parasite Epidemiology and Control 3 (2018) 96–105. https://doi.org/10.1016/j.parepi.2018.02.001
[xiii] Smit MR, Ochomo EO, Aljayyoussi G, Kwambai TK, Abong’o BO, Chen T, Bousema T, Slater HC, Waterhouse D, Bayoh NM, Gimnig JE, Samuels AM, Desai MR, Phillips-Howard PA, Kariuki SK, Wang D, Ward SA, ter Kuile FO. Safety and mosquitocidal efficacy of high-dose ivermectin when co-administered with dihydroartemisinin-piperaquine. www.thelancet.com/infection Published online March 27, 2018 http://dx.doi.org/10.1016/S1473-3099(18)30163-4
Case Management &Elimination Bill Brieger | 03 Nov 2018
Multiple Approaches for Malaria Case Management in the Struggle to Reach Pre-Elimination of Malaria
![]() Goodluck Tesha, Zahra Mkomwa, Jasmine Chadewa, Lusekelo Njoge, Abdallah Lusasi, Dunstan Bishanga, Chonge Kitojo, Erik Reaves, George Greer of the USAID Boresha Afya Project, the Tanzanian Ministry of Health, and the US President’s Malaria Initiative shared experiences on the role of malaria case management in pre-elimination efforts at the 2018 Annual Meeting of the American Society of Tropical medicine and Hygiene. Their results are seen below.
Goodluck Tesha, Zahra Mkomwa, Jasmine Chadewa, Lusekelo Njoge, Abdallah Lusasi, Dunstan Bishanga, Chonge Kitojo, Erik Reaves, George Greer of the USAID Boresha Afya Project, the Tanzanian Ministry of Health, and the US President’s Malaria Initiative shared experiences on the role of malaria case management in pre-elimination efforts at the 2018 Annual Meeting of the American Society of Tropical medicine and Hygiene. Their results are seen below.
 The 5-year USAID Boresha Afya project works in 1,817 facilities in the seven regions of the Lake/Western Zone, where malaria prevalence is high. Since 2016, Boresha Afya has collaborated with the National Malaria Control Program to support the goal of reducing the malaria case fatality rate to below 1% by 2020 by:
The 5-year USAID Boresha Afya project works in 1,817 facilities in the seven regions of the Lake/Western Zone, where malaria prevalence is high. Since 2016, Boresha Afya has collaborated with the National Malaria Control Program to support the goal of reducing the malaria case fatality rate to below 1% by 2020 by:
- Promoting universal access to early diagnosis and prompt treatment
- Providing preventive therapies to vulnerable groups
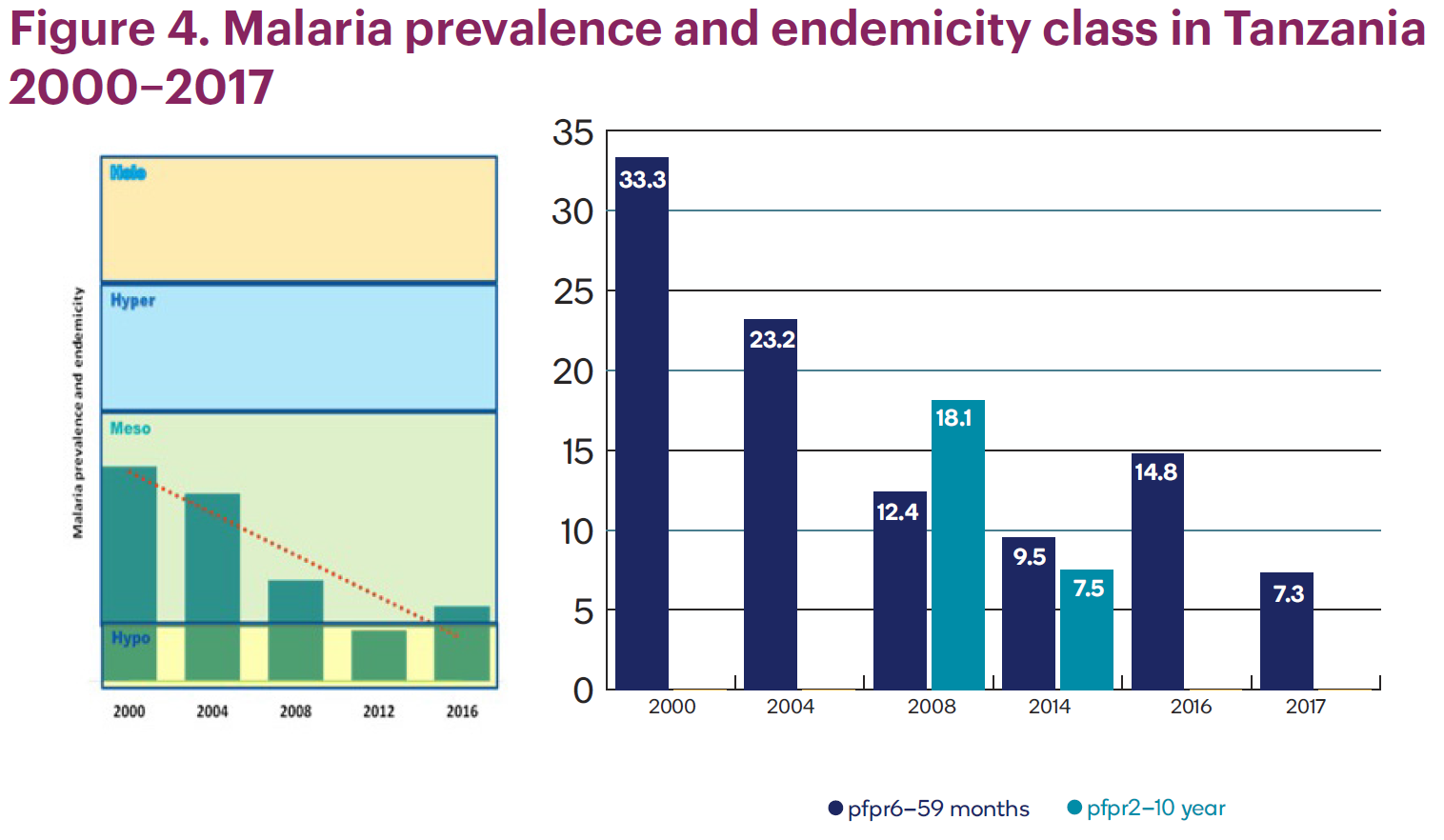
 In the last 15 years, malaria transmission has been cut in half, dropping from about 33% to less than 7.5%. Over the last three malaria indicator surveys, the number of regions with extremely low malaria prevalence (<1%) increased from one (2008) to seven (2016). The percentage of the population living in low-transmission areas (<10% prevalence) increased from 31% in 2000 to 49% in 2015.
In the last 15 years, malaria transmission has been cut in half, dropping from about 33% to less than 7.5%. Over the last three malaria indicator surveys, the number of regions with extremely low malaria prevalence (<1%) increased from one (2008) to seven (2016). The percentage of the population living in low-transmission areas (<10% prevalence) increased from 31% in 2000 to 49% in 2015.
 The intervention trained providers on quality testing using malaria rapid diagnostic tests (mRDTs). Training focused on conducting quality malaria microscopy examinations.
The intervention trained providers on quality testing using malaria rapid diagnostic tests (mRDTs). Training focused on conducting quality malaria microscopy examinations.
In addition, the team stratified malaria burden using GIS mapping and introduced malaria service and data quality improvement through a malaria dashboard. Community outreach programs were formed in remote areas.
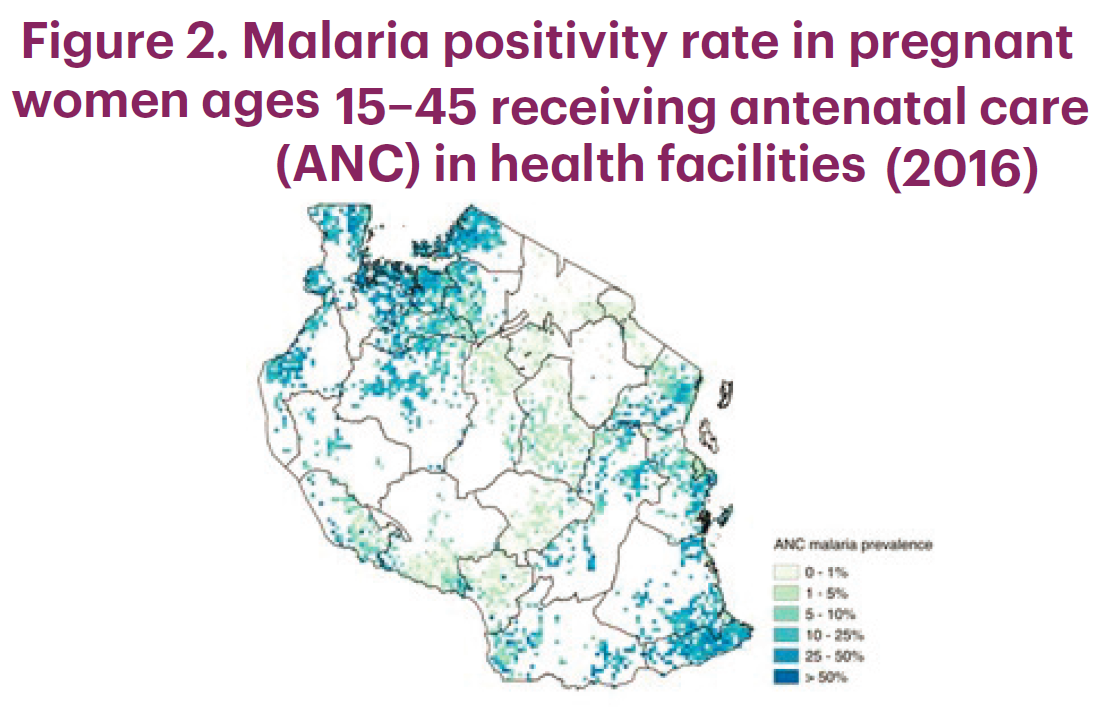
 Due to mRDT availability, more suspected malaria cases are tested before malaria treatment is administered. Per national guidelines, all pregnant women should be tested for malaria on their first visit to the clinic. All project regions have met or exceeded the national 80% testing rate target (see Figure 5).
Due to mRDT availability, more suspected malaria cases are tested before malaria treatment is administered. Per national guidelines, all pregnant women should be tested for malaria on their first visit to the clinic. All project regions have met or exceeded the national 80% testing rate target (see Figure 5).
 In conclusion, to move toward malaria elimination, Boresha Afya will focus on ensuring more suspected cases are tested at facility level. Prompt treatment positive cases will then follow. Performing more community outreach should increase access to malaria case management in remote areas. Using GIS mapping will rapidly target services.
In conclusion, to move toward malaria elimination, Boresha Afya will focus on ensuring more suspected cases are tested at facility level. Prompt treatment positive cases will then follow. Performing more community outreach should increase access to malaria case management in remote areas. Using GIS mapping will rapidly target services.
 This poster is made possible by the support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of Jhpiego and do not necessarily reflect the views of USAID or the United States Government.
This poster is made possible by the support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of Jhpiego and do not necessarily reflect the views of USAID or the United States Government.
Borders &CHW &Climate &Elimination &IPTi &Sahel &Surveillance &Vector Control Bill Brieger | 26 Sep 2018
Hopefully Malaria Elimination will not be the SaME
The Sahel Malaria Elimination Initiative (SaME) has been launched, but builds on a long history of cooperation in the region. Efforts by eight Sahelian countries to share lessons and strategies mirrors the Elimination Eight group on the opposite end of the continent.

The few rainy season months in the Sahel offer optimum malaria transmission, which SaME is tackling
The Roll Back Malaria (RBM) Partnership to End Malaria announced that in Dakar on 31st August 2018, the health “ministers from Burkina Faso, Cabo Verde, Chad, Mali, Mauritania, Niger, Senegal and The Gambia established a new regional platform to combine efforts on scaling up and sustaining universal coverage of anti-malarials and mobilizing financing for elimination.” The group plans a fast-track introduction of “innovative technologies to combat malaria and develop a sub-regional scorecard that will track progress towards the goal of eliminating malaria by 2030.” This will build on the existing country scorecard that has been developed and implemented by AMLA2030 for all countries in the region and tracks roll out of key malaria and health interventions. The Sahel Malaria Elimination Initiative will be hosted by the West African Health Organization, a specialised agency of the Economic Community of West African States (ECOWAS).
RBM explains that while the eight countries will work together, they do not have a homogenous epidemiological picture or experience with malaria programming. The Sahel experiences 20 million annual malaria cases, according to RBM, and “the Sahel region has seen both achievements and setbacks in the fight against the disease in recent years.” These eight have a highly variable malaria experience. Burkina Faso and Niger continue to be among the countries with high malaria burdens. Cabo Verde is on target for malaria free status by 2020. The Gambia, Mauritania and Senegal are reorienting their national malaria program towards malaria elimination. A benefit of this epidemiological and programmatic diversity is that countries can learn important lessons from each other.
The SaME Initiative will use the following main approaches to accelerate the combined efforts towards the attainment of malaria elimination in the sub-region:3
- Regional coordination
- Advocacy to keep malaria elimination high on the development and political agenda
- Sustainable financing mechanisms
- Cross-border collaboration and ensuring accountability
- Fast-track the introduction of innovative and progressive technologies
- Re-enforcing the Regional regulatory mechanism for quality of malaria commodities and introduction of new tools.
- Establish malaria observatory, regional surveillance, and best practice sharing
Collaboration across borders on vector control is an example of needed regional coordination. According to Thomson et al., climate variations have the potential to significantly impact vector-borne disease dynamics at multiple space and time scales. Another challenge to vector control in the region is the issue of how mosquitoes repopulate areas after an extended dry season. Huestis et al. examined the response of Anopheles coluzzii and Anopheles gambiae to environmental cues in season change in the Sahel.

Seasonal Malaria Chemoprevention Round 3 of 2018 in Burkina Faso
In addition to a history of cooperation, Sahelian countries share a unique malaria intervention, Seasonal Malaria Chemoprevention (SMC) that as the name implies, built on the reality of highly seasonal transmission in the region. SMC grew out of over five years of research in several African settings to test the effect of what was originally termed Intermittent Preventive Treatment for Infants (and later children) or IPTi.
Like IPT for pregnant women, SMC would be given monthly for at least 3-4 months, but unlike IPTp, SMC would consist of a combination two medicines, amodiaquine plus sulfadoxine-pyrimethamine (AQ+SP), which required a three daily doses (SP alone as used in IPTp consists on one dose). SMC could not therefore, be delivered effectively as a clinic-based intervention, but “should be integrated into existing programmes, such as Community Case Management and other Community Health Workers schemes.” Access to SMC by pre-school aged children as delivered by CHWs was found to be more equitable than sleeping under an LLIN. SMC has been recommended for school-age children, a neglected group that bears a substantial burden of malaria.
Closely linked to surveillance is modeling the spatial and temporal variability of climate parameters, which is crucial to tackling malaria in the Sahel. This requires reliable observations of malaria outbreaks over a long time period. To date efforts are mainly linked to climate variables such as rainfall and temperature as well as specific landscape characteristics. Other environmental and socio-economic factors that are not included in this mechanistic malaria model.
The Sahel Malaria Elimination initiative offers a unique collaborative opportunity for countries to improve on the quality of proven interventions like SMC and test and take to scale new strategies like school-based malaria programs. Regional coordination can produce better, timelier and longer-term surveillance and better understanding of and actions against malaria vectors. Readers will surely be anticipating the publishing of the regular progress malaria elimination scorecards as promised by SaME leadership.