Diagnosis &Elimination &Funding &IPTp &ITNs &Journalists/Media &Malaria in Pregnancy &Migration &Zero Malaria Bill Brieger | 26 Sep 2020
Malaria News Today 2020-09-26: supporting and strengthening malaria programs
Today’s selection of abstracts and news looks at the role of the media in supporting malaria programs, mass treatment to prevent Imported malaria, problems managing malaria in pregnancy services, malaria research in Mali and health systems strengthening to support malaria control in Guinea. Follow links to read mor details.
GHS calls for media support to eradicate malaria

The media has a role in supporting malaria programs
The Ghana Health Service (GHS) has called on journalists to support the Service to deliver integrated health package through accurate messages towards malaria eradication in the country.“Also, we need your support to set malaria as a national development agenda. This will drive advocacy for political will, increase partnership, availability and accessibility of effective tool for prevention, diagnoses and treatment of malaria in all the vulnerable populations.”
Dr Anthony Adofo Ofosu, the Deputy Director General, GHS, said this at the launch of “Zero malaria starts with me” campaign in Accra. The launch coincided with a sensitisation programme by the African Media and Malaria Research Network (AMMRN), the National Malaria Control Programme and the Speak Up African Organisation. The Deputy Director General said “It is the belief of the GHS that with effective engagement…we will be able to eradicate malaria from the country in the near future.”
Mass radical treatment of a group of foreign workers to mitigate the risk of re-establishment of malaria in Sri Lanka
Following malaria elimination, Sri Lanka was free from indigenous transmission for six consecutive years, until the first introduced case was reported in December 2018. The source of transmission (index case) was a member of a group of 32 migrant workers from India and the location of transmission was their residence reporting a high prevalence of the primary vector for malaria. Despite extensive vector control the situation was highly susceptible to onward transmission if another of the group developed malaria. Therefore, Mass Radical Treatment (MRT) of the group of workers for Plasmodium vivax malaria was undertaken to mitigate this risk.
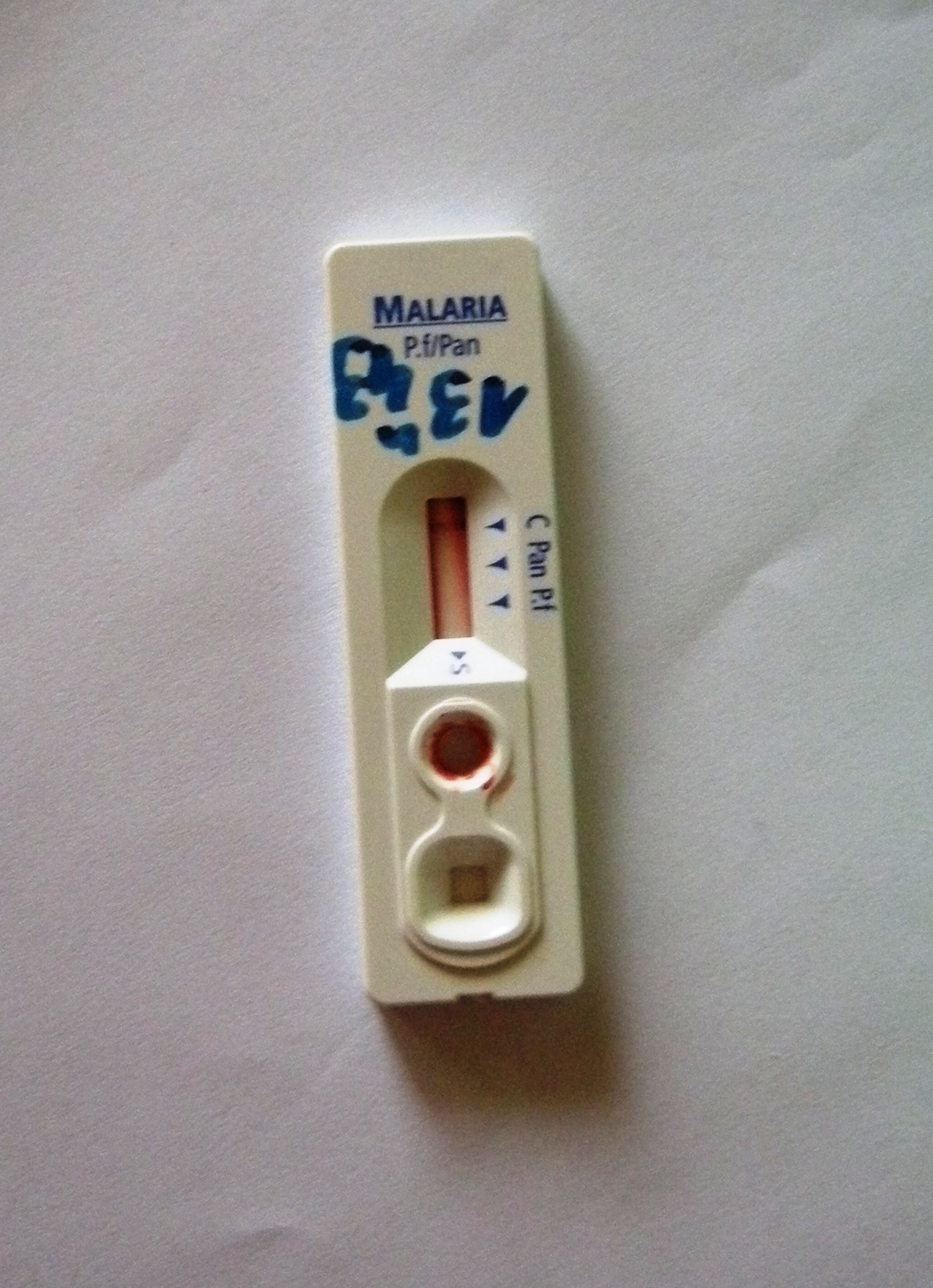
The workers were screened for malaria by microscopy and RDT, their haemoglobin level assessed, and tested for Glucose 6 phosphate dehydrogenase deficiency (G6PD) using the Care Start RDT and Brewers test prior to treatment with chloroquine (CQ) 25 mg/kg body weight (over three days) and primaquine (PQ, based on G6PD test results) (0.25 mg/kg/day bodyweight for 14 days) following informed consent. All were monitored for adverse events. None of the foreign workers were parasitaemic at baseline screening.
Mass treatment may be an option in prevention of reintroduction settings for groups of migrants who are likely to be carrying latent malaria infections, and resident in areas of high receptivity. However, in the case of Plasmodium vivax and Plasmodium ovale, a more reliable and affordable point-of-care test for G6PD activity would be required. Most countries which are eliminating malaria now are in the tropical zone and face considerable and similar risks of malaria re-introduction due to massive labour migration between them and neighbouring countries. Regional elimination of malaria should be the focus of global strategy if malaria elimination from countries is to be worthwhile and sustainable.
Managing intermittent preventive treatment of malaria in pregnancy challenges: an ethnographic study of two Ghanaian administrative regions
Malaria in pregnancy (MiP) is an important public health problem across sub-Saharan Africa. The package of measures for its control in Ghana in the last 20 years include regular use of long-lasting insecticide-treated bed nets (LLINs), directly-observed administration (DOT) of intermittent preventive treatment with sulfadoxine-pyrimethamine (IPTp-SP) and prompt and effective case management of MiP. Unfortunately, Ghana like other sub-Saharan African countries did not achieve the reset Abuja targets of 100% of pregnant women having access to IPTp and 100% using LLINs by 2015.
This ethnographic study explored how healthcare managers dealt with existing MiP policy implementation challenges and the consequences on IPTp-SP uptake and access to maternal healthcare. Healthcare managers addressed frequent stock-outs of malaria programme drugs and supplies from the National Malaria Control Programme and delayed reimbursement from the NHIS, by instituting co-payment, rationing and prescribing drugs for women to buy from private pharmacies.
 Some clients did not receive the recommended 5?+?doses of SP, others did not obtain LLINs early and some did not obtain treatment for MiP. Healthcare providers felt frustrated whenever they could not provide comprehensive care to women who could not afford comprehensive maternal and MiP care. For Ghana to achieve her goal of controlling MiP, the Ministry of Health and other supporting institutions need to ensure prompt reimbursement of funds, regular supply of programme drugs and medical supplies to public, faith-based and private health facilities.
Some clients did not receive the recommended 5?+?doses of SP, others did not obtain LLINs early and some did not obtain treatment for MiP. Healthcare providers felt frustrated whenever they could not provide comprehensive care to women who could not afford comprehensive maternal and MiP care. For Ghana to achieve her goal of controlling MiP, the Ministry of Health and other supporting institutions need to ensure prompt reimbursement of funds, regular supply of programme drugs and medical supplies to public, faith-based and private health facilities.
Malaria prevention program continuation in Guinea
CRS Guinea is the Principal Recipient (PR) in Malaria prevention program continuation grant by the Global Fund for the new cycle of funding (NFM) (January 2021-December 2023). Community health is a top priority of the Ministry of Health as a primary strategy to increase accessibility and coverage to basic health services. Under the new Global Fund grant, the community health component will be expanded to six districts, in addition to two pilot districts, Kindia and Telimele. CRS will also support coordination with other donors, including World Bank, UNICEF, Gavi, European Union and the Guinea Ministry of Health to implement the national community health strategy in 12 health districts supported by Global Fund malaria project.
The United States and Mali Celebrate 60 Years of Friendship and Partnership
Thirty years ago, our National Institutes of Health created a Malaria Research and Training Center, which is now a component of the International Center for Excellence in Research in Mali. Until today, it serves as a reference center with over 700 Malian scientists and support staff who work on malaria and other infectious diseases. Together, we have dropped malaria prevalence rates in Mali by an astounding 60 percent since 2012.
Artesunate &Children &Diagnosis &Elimination &Plasmodium/Parasite &Private Sector &Resistance &Surveillance Bill Brieger | 25 Sep 2020
Malaria News Today 2020-09-25: Testing, Surveillance, Elimination
Differentiating malaria parasite species is something science can do today, but in the 1800s the debate was over what actually caused the disease. This ability to test and diagnose gives us an important surveillance tool, the 3Ts. News from Ghana is that malaria deaths are reducing, and Guatemala is focusing on elimination. Read more at the links in each section.
Wyss Researchers Develop Malaria Diagnostic Procedure Capable of Differentiating Malaria Species
Researchers at Harvard’s Wyss Institute have developed a new malaria diagnostic test that efficiently detects and can distinguish between species of malaria parasites,
the new procedure significantly improves upon current diagnostic methods, which fail to differentiate between types of malaria. Procedures that only identify Plasmodium falciparum can lead to severe consequences for patients, since other types of malaria are resilient to therapies designed to treat Plasmodium falciparum because they enter a dormant stage in the human liver.
These genes help explain how malaria parasites survive treatment with common drug.
The essential malaria drug artemisinin acts like a “ticking time bomb” in parasite cells—but in the half a century since the drug was introduced, malaria-causing parasites have slowly grown less and less susceptible to the treatment, threatening attempts at global control over the disease.
In a paper published September 23 in Nature Communications, Whitehead Institute Member Sebastian Lourido and colleagues use genome screening techniques in the related parasite Toxoplasma gondii (T. gondii) to identify genes that affect the parasites’ susceptibility to artemisinin. Two genes stood out in the screen: one that makes the drug more lethal, and another that helps the parasite survive the treatment…
Test, Treat, and Track: Strengthening Malaria Response Capabilities in Sierra Leone
A public-private partnership in Sierra Leone aimed to build capacity for testing, treating, and tracking malaria. The post notes the “public-private partnership in Sierra Leone was a collaboration between USAID’s Human Resources for Health in 2030 (HRH2030) program; the U.S. President’s Malaria Initiative (PMI), the Global Fund to Fight AIDS, Tuberculosis and Malaria; the Pharmacy Consultancy of Sierra Leone; and the Sierra Leone National Malaria Control Program”.
NMCP partnered with pharmacies to strengthen their malaria case management capabilities. Anitta and her colleague Brenda Stafford, a trained pharmacist and Procurement and Supply Management officer, led the initiative, going pharmacy-to-pharmacy to train staff on the NMCP’s “Three T” approach: Test, Treat, and Track.
To address the first T, private pharmacies were given free malaria rapid diagnostic tests. According to 2016 data, only half of children under-five with fever received appropriate malaria testing. For the second T, the pharmacists were trained on malaria prevention, treating patients with uncomplicated malaria, and referring patients with severe malaria to health facilities. As for the last T, tracking malaria test results is key in forecasting the spread of disease. NMCP provided pharmacies with two forms that track results: a registry form to track patient information and a summary form which aggregates that into monthly data reports
Miasma War over cause of malaria was heated
Nicole Layton of the Chowan Herald reported that in the 1850s, two North Carolina doctors had a heated and protracted battle over the cause of malaria in the state. This Miasma War is so famous. So what the heck is Miasma? Those fans of Charles Dickens can tell you that at one point miasmas were thought to be the main vector for disease transmission.
During Dickens’ time in London the air was very foul and rather visible because of wood and coal and it smelled bad due to the lack of indoor plumbing. It was thought that this foul air was the cause of disease. Because our part of North Carolina had a lot of rotting vegetation and swamps there was certainly foul air about and very noticeable illness. So the general thought was that malaria was a result of this bad air.
Escuintla, Guatemala: Clinton Health Access Initiative (CHAI)
CHAI’s Guatemala Malaria Team is supporting the Ministry of Health’s National Malaria Program by providing technical assistance and supporting programmatic planning, execution, monitoring and evaluation of effective interventions in the department of Escuintla in southern Guatemala. Over the past five years, CHAI has engaged in the country and helped them make meaningful steps towards orienting their national strategic plans and systems towards the historical goal of malaria elimination.
CHAI’s Guatemala team works in close coordination with the Ministry of Health and other international partners to design, plan, execute and evaluate the impact of the country´s elimination-focused interventions in Escuintla.
Ghana: Malaria deaths in children under five reduce
Ghana has recorded a reduction in malaria deaths in children under five by 83 per cent over the last eight years, the National Malaria Control Programme (NMCP) has said. The rate of malaria-related deaths reduced from 0.6 per cent in 2012 to 0.1 per cent in 2019, showing significant inroads in malaria-related deaths among children. Malaria-related deaths of all ages also reduced by 2,799 in 2012 to 333 by end of 2019, representing an 88 per cent reduction.
Agriculture &Counterfeit Drugs &Dengue &Diagnosis &Elimination &Environment &Floods &Irrigation &Mosquitoes &Severe Malaria &Surveillance &water Bill Brieger | 24 Sep 2020
Malaria News Today 2020-09-23/24
 Today the issue of water is important for malaria mosquito propagation, both in irrigation and flooding. Artificial skin enables testing of mosquito biting. Fake medicines for malaria and other conditions threaten Africa’s health. Archived RDTs can aid surveillance. Finally there is concern for co-infection with both malaria and dengue leading to severe disease. Follow links below to read details.
Today the issue of water is important for malaria mosquito propagation, both in irrigation and flooding. Artificial skin enables testing of mosquito biting. Fake medicines for malaria and other conditions threaten Africa’s health. Archived RDTs can aid surveillance. Finally there is concern for co-infection with both malaria and dengue leading to severe disease. Follow links below to read details.
Impact of sugarcane irrigation on malaria vector Anopheles mosquito fauna, abundance and seasonality in Arjo-Didessa, Ethiopia
Despite extensive irrigation development in Ethiopia, limited studies assessed the impact of irrigation on malaria vector mosquito composition, abundance and seasonality. This study aimed to evaluate the impact of sugarcane irrigation on species composition, abundance and seasonality of malaria vectors. Adult Anopheles mosquitoes were collected using CDC light traps from three irrigated and three non-irrigated clusters in and around Arjo-Didessa sugarcane irrigation scheme in southwestern Ethiopia.
Overall, 2108 female Anopheles mosquitoes comprising of six species were collected. The ongoing sugarcane irrigation activities in Arjo-Didessa created conditions suitable for malaria transmitting Anopheles species diversity and abundance. This could drive malaria transmission in Arjo-Didessa and its environs in both dry and wet seasons. Currently practiced malaria vector interventions need to be strengthened by including larval source management to reduce vector abundance in the irrigated areas.
Prevalence of and risk factors for severe malaria caused by Plasmodium and dengue virus co-infection
A systematic review and meta-analysis examined co-infection with both Plasmodium and dengue virus (DENV) infectious species could have serious and fatal outcomes if left undiagnosed and without timely treatment. The present study aimed to determine the pooled prevalence estimate of severe malaria among patients with co-infection, the risk of severe diseases due to co-infection, and to describe the complications of severe malaria and severe dengue among patients with co-infection. Relevant studies published between databases between 12 September 1970 and 22 May 2020 were identified and retrieved.
The present study found that there was a high prevalence of severe malaria among patients with Plasmodium and DENV co-infection. Physicians in endemic areas where these two diseases overlap should recognize that patients with this co-infection can develop either severe malaria or severe dengue with bleeding complications, but a greater risk of developing severe dengue than severe malaria was noted in patients with this co-infection.
South Sudan: Flooding deepens a humanitarian crisis in Pibor area
Today, however, the Pibor River has swelled to make parts of the town inaccessible and is threatening the clinic. Many neighborhoods cannot be reached by foot, and a local ferry is too expensive for many who live in the area. A mobile MSF team is providing medical care in hard-to-reach areas. “Our focus is now on malaria, measles and flooding,” said Josh Rosenstein, MSF deputy head of mission. “Today we are reaching out to the community through our daily mobile clinics, treating the most severe illnesses. We’re also implementing our flood contingency plan, which includes building additional flood defenses around the clinic to ensure we can continue to provide medical services, as the water level is rising at an alarming speed.”
Stratifying malaria receptivity in Bangladesh using archived rapid diagnostic tests
Surveillance of low-density infections and of exposure to vectors is crucial to understand where malaria elimination might be feasible, and where the risk of outbreaks is high. Archived rapid diagnostic tests (RDTs), used by national malaria control and elimination programs for clinical diagnosis, present a valuable, yet rarely used resource for in-depth studies on malaria epidemiology. 1022 RDTs from two sub-Districts in Bangladesh (Alikadam and Kamalganj) were screened by qPCR for low-density Plasmodium falciparum and Plasmodium vivax infections, and by ELISA for Anopheles salivary gland antibodies as a marker for exposure to vectors.
 Concordance between RDT and qPCR was moderate. qPCR detected 31/1022 infections compared to 36/1022 diagnosed by RDT. Exposure to Anopheles was significantly higher in Kamalganj despite low transmission, which could be explained by low bed net use. Archived RDTs present a valuable source of antibodies for serological studies on exposure to vectors. In contrast, the benefit of screening archived RDTs to obtain a better estimate of clinical case numbers is moderate. Kamalganj could be prone to outbreaks.
Concordance between RDT and qPCR was moderate. qPCR detected 31/1022 infections compared to 36/1022 diagnosed by RDT. Exposure to Anopheles was significantly higher in Kamalganj despite low transmission, which could be explained by low bed net use. Archived RDTs present a valuable source of antibodies for serological studies on exposure to vectors. In contrast, the benefit of screening archived RDTs to obtain a better estimate of clinical case numbers is moderate. Kamalganj could be prone to outbreaks.
New tool mimics human skin to allow detailed study of mosquito biting
eLife: Researchers develop a human skin mimic to study mosquito biting in high resolution without using humans as ‘bait.’ The tool, which uses an artificial blood meal and a surface that mimics human skin, will provide detailed understanding of blood feeding without using human subjects as bait. It can also fit conveniently into a backpack, allowing the study of mosquitoes in laboratory and natural environments.
Blood feeding is essential for mosquitoes to reproduce, but it is during blood feeds on human hosts that they pass on pathogens such as malaria. It consists of a bite ‘substrate’ – a transparent, temperature-controlled surface that mimics body temperature to attract mosquitoes. An artificial meal is applied on top of this and covered with a commonly used membrane that mosquitoes can pierce. The meal resembles blood, allowing mosquitoes to engorge and increase their weight by two to threefold. This bite substrate is then placed in a transparent cage, and an external camera records the mosquitoes’ behaviour. The team tested biteOscope with four medically important species of mosquito.
Counterfeiting of Fake Drugs in Africa: current situation, causes and countermeasures
The more desirable a product is the higher the tendency to replicate it and meet that parcel of consumers that want to join the trend but cannot pay the price. Profit is one of the many reasons that make counterfeit an attractive business for many. Africa, unfortunately but not surprisingly, is one of the most affected continents, comprehensible since its markets have become a huge target for second generation goods, with a major focus on pharmaceutical drugs.
The World Health Organization (hereinafter, WHO) stated that 42% of all fake medicine reported to them between the years of 2013 and 2017 was linked to the African continent and we expect that these numbers fall short of reality. Africa is seriously affected by it and one clear example is the anti-malarial medication. Anti-malarials and antibiotics are amongst the most commonly reported as fake or substandard medical products.
COVID-19 &Drug Development &Elimination &Funding &Plasmodium/Parasite &Resistance &Vaccine Bill Brieger | 17 Sep 2020
Malaria News Today 2020-09-17
 Leading off our news update are findings from eastern Kenya about a genetic blood grouping that may help prevent malaria. While government leaders in the Asia-Pacific region committed to eliminating malaria, a report from the Gates Foundation explains how COVID-19 has set progress back and without new tools it may take more than 25 years to rid the world of the disease. In that light, Novartis is staking its finances on being able to make medicines that will be accessible and fight malaria. More details and the Gates video can be seen by clicking the links below.
Leading off our news update are findings from eastern Kenya about a genetic blood grouping that may help prevent malaria. While government leaders in the Asia-Pacific region committed to eliminating malaria, a report from the Gates Foundation explains how COVID-19 has set progress back and without new tools it may take more than 25 years to rid the world of the disease. In that light, Novartis is staking its finances on being able to make medicines that will be accessible and fight malaria. More details and the Gates video can be seen by clicking the links below.
How Dantu Blood Group protects against malaria
The secret of how the Dantu genetic blood variant helps to protect against malaria has been revealed for the first time by scientists at the Wellcome Sanger Institute, the University of Cambridge and the KEMRI-Wellcome Trust Research Programme, Kenya. The team found that red blood cells in people with the rare Dantu blood variant have a higher surface tension that prevents them from being invaded by the world’s deadliest malaria parasite, Plasmodium falciparum. The findings were published in Nature and could be significant in the wider battle against malaria.
In 2017, researchers discovered that the rare Dantu blood variant, which is found regularly only in parts of East Africa, provides some degree of protection against severe malaria. The intention behind this new study was to explain why. Red blood cell samples were collected from 42 healthy children in Kilifi, Kenya, who had either one, two or zero copies of the Dantu gene. The Dantu variant created cells with a higher surface tension—like a drum with a tighter skin. At a certain tension, malaria parasites were no longer able to enter the cell.
Novartis ties bond sale to malaria treatment access in sustainability push
Novartis raised 1.85 billion euros on Wednesday from the sale of a bond on which interest payments will rise if the drugmaker fails to expand access to medicines and programmes to combat malaria and leprosy in a number of developing countries.
Investors are increasingly pushing companies to improve their track record on environmental, social and governance (ESG) issues while sustainable investing grows in popularity, spurring an increase in sustainable debt issuance year after year. Novartis’ bond is only the third issue to date to link payments to creditors to company-wide sustainable development targets. By Yoruk Bahceli
Commitment to make Asia Pacific a malaria free region
Government officials from across Asia Pacific have come together during virtual Malaria Week 2020, to reaffirm their commitment to eliminating malaria and strengthening health systems to keep the region safe from health threats. Embracing the theme of “Inclusion. Integration. Innovation.”, officials called for increased collaboration and action to accelerate towards the goal of ending malaria in the region by 2030, at a time when major gains and regional progress are under threat due to disruptions caused by Covid-19.
It could take up to 25 years to eradicate malaria from Africa – Bill Gates
Bill Gates said: “Moving to malaria which is a very awful disease not just to the kids it kills but many kids whose brains are permanently damaged, the economic effects you have with malaria. If we don’t have new tools like vaccines or new ways of killing mosquitoes, it would probably take more than 25 years to get rid of malaria. If we get the new tools and they work, we think it can be done in under 20 years. So the malaria field is both trying to keep the number of deaths down, and we have to deal with the resistance that comes up, that the mosquitoes develop.”
Gates Foundation Report notes that, “We’ve been set back about 25 years in about 25 weeks.” Extreme poverty increased 7% because of COVID-19. In a video included in the Foundation’s report, Bill Gates explains how COVID-19 disrupts the fight against malaria.
Agriculture &Artesunate &Case Management &Children &Drug Development &Elimination &Funding &NTDs &Resistance Bill Brieger | 16 Sep 2020
Malaria News Today 2020-09-15
Malaria Journal released three articles ranging from the relation between malaria and agricultural irrigation, artemisinin resistance on the Myanmar-China border, and efforts at costing malaria elimination interventions. PLoS Medicine examined the quality of malaria clinical management in children. Finally, Frontiers in Cellular and Infection Microbiology reported on a new drug against malaria and toxoplasmosis. Click on links to read more details.
Minimal tillage and intermittent flooding farming systems show a potential reduction in the proliferation of Anopheles mosquito larvae in a rice field in Malanville, Northern Benin
Irrigation systems have been identified as one of the factors promoting malaria disease around agricultural farms in sub-Saharan Africa. However, if improved water management strategy is adopted during rice cultivation, it may help to reduce malaria cases among human population living around rice fields.
A clear reduction of larva density was observed with both intermittent flooding systems applied to minimal tillage (MT?+?IF?+?NL) and intermittent flooding applied to deep tillage (DT?+?IF?+?AL), showing that intermittent flooding could reduce the abundance of malaria vector in rice fields. Recommending intermittent flooding technology for rice cultivation may not only be useful for water management but could also be an intentional strategy to control mosquitoes vector-borne diseases around rice farms.
No evidence of amplified Plasmodium falciparum plasmepsin II gene copy number in an area with artemisinin-resistant malaria along the China–Myanmar border
The emergence and spread of artemisinin resistance in Plasmodium falciparum poses a threat to malaria eradication, including China’s plan to eliminate malaria by 2020. Piperaquine (PPQ) resistance has emerged in Cambodia, compromising an important partner drug that is widely used in China in the form of dihydroartemisinin (DHA)-PPQ. Several mutations in a P. falciparum gene encoding a kelch protein on chromosome 13 (k13) are associated with artemisinin resistance and have arisen spread in the Great Mekong subregion, including the China–Myanmar border. Multiple copies of the plasmepsin II/III (pm2/3) genes, located on chromosome 14, have been shown to be associated with PPQ resistance.
DHA-PPQ for uncomplicated P. falciparum infection still showed efficacy in an area with artemisinin-resistant malaria along the China–Myanmar border. There was no evidence to show PPQ resistance by clinical study and molecular markers survey. Continued monitoring of the parasite population using molecular markers will be important to track emergence and spread of resistance in this region.
Costing malaria interventions from pilots to elimination programmes
Malaria programmes in countries with low transmission levels require evidence to optimize deployment of current and new tools to reach elimination with limited resources. Recent pilots of elimination strategies in Ethiopia, Senegal, and Zambia produced evidence of their epidemiological impacts and costs. There is a need to generalize these findings to different epidemiological and health systems contexts. Drawing on experience of implementing partners, operational documents and costing studies from these pilots, reference scenarios were defined for rapid reporting (RR), reactive case detection (RACD), mass drug administration (MDA), and in-door residual spraying (IRS). These generalized interventions from their trial implementation to one typical of programmatic delivery. In doing so, resource use due to interventions was isolated from research activities and was related to the pilot setting. Costing models developed around this reference implementation, standardized the scope of resources costed, the valuation of resource use, and the setting in which interventions were evaluated. Sensitivity analyses were used to inform generalizability of the estimates and model assumptions.
Populated with local prices and resource use from the pilots, the models yielded an average annual economic cost per capita of $0.18 for RR, $0.75 for RACD, $4.28 for MDA (two rounds), and $1.79 for IRS (one round, 50% households). Intervention design and resource use at service delivery were key drivers of variation in costs of RR, MDA, and RACD. Scale was the most important parameter for IRS. Overall price level was a minor contributor, except for MDA where drugs accounted for 70% of the cost. The analyses showed that at implementation scales comparable to health facility catchment area, systematic correlations between model inputs characterizing implementation and setting produce large gradients in costs. Prospective costing models are powerful tools to explore resource and cost implications of policy alternatives. By formalizing translation of operational data into an estimate of intervention cost, these models provide the methodological infrastructure to strengthen capacity gap for economic evaluation in endemic countries. The value of this approach for decision-making is enhanced when primary cost data collection is designed to enable analysis of the efficiency of operational inputs in relation to features of the trial or the setting, thus facilitating transferability.
Quality of clinical management of children diagnosed with malaria: A cross-sectional assessment in 9 sub-Saharan African countries between 2007–2018
Appropriate clinical management of malaria in children is critical for preventing progression to severe disease and for reducing the continued high burden of malaria mortality. This study aimed to assess the quality of care provided to children under 5 diagnosed with malaria across 9 sub-Saharan African countries. We used data from the Service Provision Assessment (SPA) survey. SPAs are nationally representative facility surveys capturing quality of sick-child care, facility readiness, and provider and patient characteristics across 9 countries, including Uganda (2007), Rwanda (2007), Namibia (2009), Kenya (2010), Malawi (2013), Senegal (2013–2017), Ethiopia (2014), Tanzania (2015), and Democratic Republic of the Congo (2018).
In this study, we found that a majority of children diagnosed with malaria across the 9 surveyed sub-Saharan African countries did not receive recommended care. Clinical management is positively correlated with the stocking of essential commodities and is somewhat improved in more recent years, but important quality gaps remain in the countries studied. Continued reductions in malaria mortality will require a bigger push toward quality improvements in clinical care. Despite increases in the distribution of malaria tests and effective antimalarial medications, significant gaps in the quality of care for pediatric malaria are present in these 9 countries. Further improvements in quality of malaria care may require a better understanding of remaining barriers and facilitators to appropriate management.
Novel drug could be a powerful weapon in the fight against malaria and toxoplasmosis
Princeton researchers are making key contributions toward developing a promising new treatment for the widespread and devastating diseases toxoplasmosis and malaria.
The Princeton scientists specialize in preparing the drug compound into a medicine that is both safe and effective for humans and able to reach its intended sites of action in the body in sufficient doses. An international team of scientists found the new drug—designated JAG21—to be highly effective against parasites in cell-based studies in the lab. After the discovery, team representatives contacted Princeton’s Robert Prud’homme for help in translating the JAG21 compound into a deliverable medication. Prud’homme is a co-author of a study, published in June 2020 in Frontiers in Cellular and Infection Microbiology, that describes the compound and its excellent preliminary results in mice.
Diagnosis &Elimination &Environment &Health Information &Health Systems &History &Invest in Malaria Control &Microscopy &Surveillance &Trachoma Bill Brieger | 10 Sep 2020
Malaria News Today 2020-09-10
These malaria and related news and abstracts stress the importance of sentinel surveillance systems, strong political and systems commitment to disease elimination, malachite green loop-mediated isothermal amplification for better malaria detection, and the threat of neglected fungal infections. An article from The Lancet shows that it is not just money that is needed to eliminate malaria, but better management and systems. Finally a bit of history from 18th Century North Carolina is shared. Click the links in each section to learn more about each topic.
Implementation of a malaria sentinel surveillance system in Togo: a pilot study
Since July 2017, 16 health facilities called sentinel sites, 4 hospitals and 12 peripheral care units located in 2 epidemiologically different health regions of Togo, have provided weekly data on malaria morbidity and mortality for the following 3 target groups:?<?5-years-old children,???5-years-old children and adults, and pregnant women. Data from week 29 in 2017 to week 13 in 2019 were analysed.
Each sentinel site provided complete data and the median time to data entry was 4 days. The number of confirmed malaria cases increased during the rainy seasons both in children under 5 years old and in children over 5 years old and adults. Malaria-related deaths occurred mainly in children under 5 years old and increased during the rainy seasons. The mean percentage of tested cases for malaria among suspected malaria cases was 99.0%. The mean percentage of uncomplicated malaria cases handled in accordance with national guidelines was 99.4%. The mean percentage of severe malaria cases detected in peripheral care units that were referred to a hospital was 100.0%. Rapid diagnostic tests and artemisinin-based combination therapies were out of stock several times, mainly at the beginning and end of the year. No hospital was out of stock of injectable artesunate or injectable artemether.
These indicators showed good management of malaria cases in the sentinel sites. Real-time availability of data requires a good follow-up of data entry on the online platform. The management of input stocks and the promptness of data need to be improved to meet the objectives of this malaria sentinel surveillance system.
Evaluation of the colorimetric malachite green loop-mediated isothermal amplification (MG-LAMP) assay …
… for the detection of malaria species at two different health facilities in a malaria endemic area of western Kenya. Prompt diagnosis and effective malaria treatment is a key strategy in malaria control. However, the recommended diagnostic methods, microscopy and rapid diagnostic tests (RDTs), are not supported by robust quality assurance systems in endemic areas. This study compared the performance of routine RDTs and smear microscopy with a simple molecular-based colorimetric loop-mediated isothermal amplification (LAMP) at two different levels of the health care system in a malaria-endemic area of western Kenya.
Patients presenting with clinical symptoms of malaria at Rota Dispensary (level 2) and Siaya County Referral Hospital (level 4) were enrolled into the study after obtaining written informed consent. Capillary blood was collected to test for malaria by RDT and microscopy at the dispensary and county hospital, and for preparation of blood smears and dried blood spots (DBS) for expert microscopy and real-time polymerase chain reaction (RT-PCR).
Results of the routine diagnostic tests were compared with those of malachite green loop-mediated isothermal amplification (MG-LAMP) performed at the two facilities.
A total of 264 participants were enrolled into the study. At the dispensary level, the positivity rate by RDT, expert microscopy, MG-LAMP and RT-PCR was 37%, 30%, 44% and 42%, respectively, and 42%, 43%, 57% and 43% at the county hospital. Using RT-PCR as the reference test, the sensitivity of RDT and MG-LAMP was 78.1% (CI 67.5–86.4) and 82.9% (CI 73.0–90.3) at Rota dispensary.
At Siaya hospital the sensitivity of routine microscopy and MG-LAMP was 83.3% (CI 65.3–94.4) and 93.3% (CI 77.9–99.2), respectively. Compared to MG-LAMP, there were 14 false positives and 29 false negatives by RDT at Rota dispensary and 3 false positives and 13 false negatives by routine microscopy at Siaya Hospital. MG-LAMP is more sensitive than RDTs and microscopy in the detection of malaria parasites at public health facilities and might be a useful quality control tool in resource-limited settings.
Terminating Trachoma. How Myanmar eliminated blinding trachoma.
 Download the book from WHO New Delhi: World Health Organization, Regional Office for South-East Asia; 2020. Licence: CC BY-NC-SA 3.0 IGO. Myanmar’s three-phase approach to eliminating trachoma has been a great success, which will certainly continue. The country’s visionary National Eye Health Plan 2017-2021, which is closely aligned with international policies for prevention of blindness, gives confidence that Myanmar will maintain its elimination status. This book chronicles how a combination of good leadership, effective partnerships, health-care facilities and hardworking health-care personnel helped Myanmar eliminate trachoma as a public health problem.
Download the book from WHO New Delhi: World Health Organization, Regional Office for South-East Asia; 2020. Licence: CC BY-NC-SA 3.0 IGO. Myanmar’s three-phase approach to eliminating trachoma has been a great success, which will certainly continue. The country’s visionary National Eye Health Plan 2017-2021, which is closely aligned with international policies for prevention of blindness, gives confidence that Myanmar will maintain its elimination status. This book chronicles how a combination of good leadership, effective partnerships, health-care facilities and hardworking health-care personnel helped Myanmar eliminate trachoma as a public health problem.
Health sector spending and spending on HIV/AIDS, tuberculosis, and malaria, and development assistance for health, SDG Progress
Although the progress towards Sustainable Development Goal (SDG) 3, which aims to “ensure healthy lives and promote well-being for all at all ages”, has been assessed in various works, there is less research focusing on tracking spending towards this goal. In this study, spending estimates were used to determine progress in financing the priority areas of SDG3, examine the correlation between outcomes and financing, and identify where resource gains are most required to attain the SDG3 indicators for which data are available.
 From 1995 to 2017, domestic health spending was determined, disaggregated by source (government, out-of-pocket, and prepaid private) for 195 countries and territories. Outcomes suggest a global rise in total health spending since the state of the SDGs in 2015, reaching $7·9 trillion (7·8–8·0) in 2017, and is estimated to rise to $11·0 trillion (10·7–11·2) by 2030, although with substantial disparity across countries. Per estimates, low-income and middle-income countries, in 2017, had an estimated spending of $20·2 billion on HIV/AIDS, $10·9 billion on tuberculosis, and $5·1 billion on malaria in endemic countries.
From 1995 to 2017, domestic health spending was determined, disaggregated by source (government, out-of-pocket, and prepaid private) for 195 countries and territories. Outcomes suggest a global rise in total health spending since the state of the SDGs in 2015, reaching $7·9 trillion (7·8–8·0) in 2017, and is estimated to rise to $11·0 trillion (10·7–11·2) by 2030, although with substantial disparity across countries. Per estimates, low-income and middle-income countries, in 2017, had an estimated spending of $20·2 billion on HIV/AIDS, $10·9 billion on tuberculosis, and $5·1 billion on malaria in endemic countries.
Although there is an increase in both domestic government and DAH spending, across these three diseases, variation in the accompanied changes in outcomes was observed. Malaria was noted to have the most consistent reductions in outcomes across countries as spending has raised. Findings thereby suggest mixed progress towards meeting the SDG3 targets; the progress varied by country and by target. The evidence on the scale-up of spending and improvements in health outcomes suggest a nuanced relationship, such that outcomes do not always improve with increases in spending.
Although more resources may be required by the countries to achieve SDG3, there will also be a necessity for addressing other constraints in the broader health system such as inefficient allocation of resources across interventions and populations, weak governance systems, human resource shortages, and drug shortages.
Ignored fungal infections kill more people annually than HIV and malaria combined
Carolina Pohl-Albertyn says that, “You may also know that there are other infections causing great concern, such as HIV (690 000 deaths/year), tuberculosis (1.5-million deaths/year), and malaria (405,000 deaths/year). But what would be your reaction if you knew that fungal infections (ranging from skin and mucosal infections (e.g. vaginal or oral thrush) to deadly systemic and organ infections (e.g. candidiasis, cryptococcal meningitis, and bronchopulmonary aspergillosis]) affect more than one-billion people each year, of which more than 150-million cases are severe and life-threatening and cause 1.7 million deaths per year?”
Malaria was once scourge in Chowan County, North Carolina
Nicole Bowman-Layton (Editor) provides some history of malaria. It’s fascinating to think that less than 100 years ago this disease was still a major scourge in Chowan County. I’ve wanted to write about this topic for a long time since the coronavirus popped up but was a bit concerned about writing about a somewhat depressing topic.
According to NCPedia malaria came to North Carolina in the 1500s from some of the first European explorers who were bitten by our friendly Anopheles mosquitoes and then transmitted to the native population. And as we well know, we live in a very damp environment surrounded by sitting water which certainly increases the harvest of mosquitos. Some of the most prominent Revolutionary Edentonians suffered from the “Ague” during their lives. Declaration signer Joseph Hewes suffered from “intermittent fever and ague” throughout his life which were certainly symptoms of malaria.
The German traveler Dr. Johan Schoepf wrote in his book Travels in the Confederation, 1783-1784, of “…the sickliness of the inhabitants, especially prevalent in the low, overflowed, and swampy parts of this country, and giving the people a pale, decayed, and prematurely old look. This is the case not only about Edenton, but along the entire low-lying coast, which this fall, from Virginia to South Carolina, was visited with numerous fevers.
Anemia &Dracunculiasis Guinea Worm &Elimination &Leishmaniasis &MDA &Schistosomiasis Bill Brieger | 09 Sep 2020
NTD News Today 2020-09-09 from ASTMH
![]() The current table of contents from the American Journal of Tropical Medicine and Hygiene features several important articles on neglected tropical diseases and malaria. Below are abstracts of several with links to the journal.
The current table of contents from the American Journal of Tropical Medicine and Hygiene features several important articles on neglected tropical diseases and malaria. Below are abstracts of several with links to the journal.
Agent-Based Simulation for Seasonal Guinea Worm Disease in Chad Dogs
The campaign to eradicate dracunculiasis (Guinea worm [GW] disease) and its causative pathogen Dracunculus medinensis (GW) in Chad is challenged by infections in domestic dogs, which far outnumber the dwindling number of human infections. We present an agent-based simulation that models transmission of GW between a shared water source and a large population of dogs. The simulation incorporates various potential factors driving the infections including external factors and two currently used interventions, namely, tethering and larvicide water treatments.
By defining and estimating infectivity parameters and seasonality factors, we test the simulation model on scenarios where seasonal patterns of dog infections could be driven by the parasite’s life cycle alone or with environmental factors (e.g., temperature and rainfall) that could also affect human or dog behaviors (e.g., fishing versus farming seasons).
We show that the best-fitting model includes external factors in addition to the pathogen’s life cycle. From the simulation, we estimate that the basic reproductive number, R 0, is approximately 2.0; our results also show that an infected dog can transmit the infection to 3.6 other dogs, on average, during the month of peak infectivity (April). The simulation results shed light on the transmission dynamics of GWs to dogs and lay the groundwork for reducing the number of infections and eventually interrupting transmission of GW.
Village Response to Mass Drug Administration for Schistosomiasis in Mwanza Region, Northwestern Tanzania
Are We Missing Socioeconomic, Cultural, and Political Dimensions?
Praziquantel (PZQ)-based mass drug administration (MDA) is the main approach for controlling schistosomiasis in endemic areas. Interventions such as provision and use of clean and safe water, minimizing contacts with infested water, disposal of human waste in latrines, and snail control provide additional key interventions to break the transmission cycle and could complement and perhaps sustain the benefits of MDA. However, all interventions deployed need to be accepted by the targeted communities. A qualitative study was conducted to examine factors that might differentiate villages which did not show a substantial decrease in Schistosoma mansoni prevalence despite repeated, high treatment coverage referred to as “persistent hotspot villages” from villages which showed a substantial decrease in prevalence referred to as “responding (RES) villages.” A convenient sample of adults was drawn from eight villages. Thirty-nine key informants were interviewed and 16 focus groups were held with a total of 123 participants. Data were analyzed manually using a thematic content approach. In both hotspot and RES villages, schistosomiasis was not considered to be a priority health problem because of its chronic nature, lack of knowledge and awareness, and poverty among study communities.
Hotspot villages exhibited poor leadership style, lack of or insufficient social engagement, little or lack of genuine community participation, little motivation, and commitment to schistosomiasis control compared with RES villages where there were commitment and motivation to fight schistosomiasis. We support the view of scholars who advocate for the adoption of a biosocial approach for effective and sustainable PZQ-based MDA for schistosomiasis control.
Assessment of Incubation Period of Cutaneous Leishmaniasis due to Leishmania major in Tunisia
The period between the infective sandfly bites and appearance of cutaneous leishmaniasis (CL) lesions is still hypothetical and little studied. This work aimed at assessing the incubation time of zoonotic CL (ZCL) due to Leishmania major using a standardized methodology. The retrospective analysis used the epidemiological, clinical, and biological information available in the database recording all the CL cases diagnosed at the Parasitology Department of the Pasteur Institute of Tunis during 2015–2019. It allowed for the selection of 92 privileged observations 1) of confirmed CL cases with presentation suggestive of ZCL form 2) living in northern regions free of ZCL 3) with a single infective trip of less than a week to ZCL foci during transmission season and 4) with accurate dates of travel and onset of lesions. Incubation length computed in this population ranged from 1 to 21 weeks, with a median of 5 weeks (interquartile range: 3–8.5 weeks).
Schistosoma mansoni Vector Snails in Antigua and Montserrat
Snail-Related Considerations Pertinent to a Declaration of Elimination of Human Schistosomiasis.
Investigations leading to a WHO-validated declaration of elimination of schistosomiasis transmission are contemplated for several countries, including Caribbean island nations. With assistance from the Pan American Health Organization, we undertook freshwater snail surveys in two such nations, Antigua and Barbuda, and Montserrat in September and October 2017. Historically, the transmission of Schistosoma mansoni supported by the Neotropical vector snail Biomphalaria glabrata occurred in both countries. Transmission on the islands is thought to have been interrupted by the treatment of infected people, improved sanitation, introduction of competitor snails, and on Montserrat with the eruption of the Soufrière volcano which decimated known B. glabrata habitats. Guided by the available literature and local expertise, we found Biomphalaria snails in seven of 15 and one of 14 localities on Antigua and Montserrat, respectively, most of which were identified anatomically and molecularly as Biomphalaria kuhniana.
Two localities on Antigua harbored B. glabrata, but no schistosome infections in snails were found. For snail-related aspects of validation of elimination, there are needs to undertake basic local training in medical malacology, be guided by historical literature and recent human schistosomiasis surveys, improve and validate sampling protocols for aquatic habitats, enlist local expertise to efficiently find potential transmission sites, use both anatomical and molecular identifications of schistosomes or putative vector snail species found, if possible determine the susceptibility of recovered Biomphalaria spp. to S. mansoni, publish survey results, and provide museum vouchers of collected snails and parasites as part of the historical record.
Decreased Mortality of falciparum Malaria in Anemic Prisoners of War?
Modern clinical trials have suggested that anemia protects against malaria mortality. Military records of the Second World War in Asia were examined to see if there was support for this hypothesis. When relatively well-nourished Imperial Japanese Navy sailors captured on Nauru (n = 799) were imprisoned on the Fauro Islands, 26% died from falciparum malaria. Similarly treated but very malnourished colocated Imperial Army soldiers experienced low stable malaria mortality. One-fifth of previously healthy Australian Army soldiers (n = 252) retreating from New Britain died largely because of malaria in April 1942. Malnourished prisoners of war, who were as a group very anemic, both Australian Army soldiers in Thailand and Japanese Army soldiers in Papua New Guinea, had high malaria rates but very low (< 3%) mortality rates. Malaria immunity does not adequately explain this dichotomy, suggesting that severe nutritional deprivation may be protective against malaria mortality possibly because of iron-deficiency anemia.
Artesunate &Dengue &Elimination &Malaria in Pregnancy &Mosquitoes &Nigeria &Resistance &Vector Control &Zika Bill Brieger | 03 Sep 2020
Malaria News Today 2020-09-03
Various updates were found in newsletters and journal abstracts online today. These looked at mosquitoes – what attracts them to people, how ookinetes move in the midgut, and how perlite from volcanic rock may be a barrier repellent. Nigeria reports that there is no ACT resistance – so far. And malaria partners join to coordinate actions in Uganda. Click on links to read details.
Nigeria yet to detect resistance of malaria parasite to ACTs, says ministe
Contrary to reports that Africa has for the first time identified resistance strain of the malaria parasite to the drug of choice, Artemisinin Combination Therapy (ACT), the Minister of Health, Dr. Osagie Emmanuel Ehanire, on Monday said a study conducted in three states of the country showed there is no such phenomenon in Nigeria. “However, we are still monitoring the situation. We insist that people should conduct a malaria test before using the drug of choice. This we hope will help prevent any kind of resistance of the malaria parasite to ACTs.”
Ministry of Health launches the Malaria Free Uganda Fund
Health Minister Dr Jane Ruth Aceng told journalists in Kampala today that the idea of having this new board was reached after realizing that different entities have been conducting the same malaria control related work. She said that the ministry resolved that mainstreaming responsibility will remove financial and operational bottlenecks that deter them from achieving set targets for elimination of the disease. The fund with a board of 11 members is chaired by Kenneth Wycliffe Mugisha of the Rotarian Malaria Partners-Uganda.
Volcanic Rock Yields a New Kind of Insecticide for Mosquitoes
Insecticide resistance to pesticides has become widespread in mosquito populations, making insecticides less effective over time. Therefore, there is an urgent need for insecticides with alternative modes of action. tested a material derived from volcanic rock, perlite, as a potential non-chemical insecticide against Anopheles gambiae, one of the primary mosquitoes that spreads malaria in Africa. In their new report published in August in the Journal of Medical Entomology, they show that perlite has encouraging potential as a mechanical insecticide. Perlite is believed to act by causing dehydration in the mosquitoes. read more…
Mosquitoes love pregnant, beer-drinking exercisers with Type O blood
Mosquitoes spread Zika, West Nile, Chikungunya, Dengue, and Malaria, resulting in 700 million illnesses a year and a million deaths. Even if you don’t get sick from a mosquito bite, the blood thinner they pump into your flesh before draining your blood causes swelling and itching. This article in Smithsonian Magazine lists the factors that make some people more tempting targets than others to mosquito bites. They include:
- Blood type: “One study found that in a controlled setting, mosquitoes landed on people with Type O blood nearly twice as often as those with Type A.”
- Carbon Dioxide: “people who simply exhale more of the gas over time—generally, larger people—have been shown to attract more mosquitoes than others.”
- Exercise: “mosquitoes find victims at closer range by smelling the lactic acid, uric acid, ammonia and other substances expelled via their sweat”
- Skin bacteria: “scientists found that having large amounts of a few types of bacteria made skin more appealing to mosquitoes”
- Beer: “Just a single 12-ounce bottle of beer can make you more attractive to the insects”
- Pregnancy: “pregnant people exhale about 21 percent more carbon dioxide and are on average about 1.26 degrees Fahrenheit warmer than others”
- Clothing color: “wearing colors that stand out (black, dark blue or red) may make you easier to find”
- Genetics: “underlying genetic factors are estimated to account for 85 percent of the variability between people in their attractiveness to mosquitoes”
Live In Vivo Imaging of Plasmodium Invasion of the Mosquito Midgut
Malaria is one of the most devastating parasitic diseases in humans and is transmitted by anopheline mosquitoes. The mosquito midgut is a critical barrier that Plasmodium parasites must overcome to complete their developmental cycle and be transmitted to a new host. Here, we developed a new strategy to visualize Plasmodium ookinetes as they traverse the mosquito midgut and to follow the response of damaged epithelial cells by imaging live mosquitoes. Understanding the spatial and temporal aspects of these interactions is critical when developing novel strategies to disrupt disease transmission.
Community &COVID-19 &Dracunculiasis Guinea Worm &Elimination &Integration &NTDs &Snakebite &Surveillance Bill Brieger | 19 May 2020
Tropical Diseases and the World Health Assembly 73rd Meeting
If it were not difficult enough to guide global health during a pandemic, some world leaders are trying to deflect attention from the real dangers at hand to score on their petty political concerns. In the meantime, we need to focus on what tropical health and disease issues may actually be coming under consideration at the virtual WHA 73.
 Agenda item 3 (A73/CONF./1 Rev.1) or “COVID-19 response Draft resolution” directly addresses the concerns of many that other major deadly diseases and essential services should not be further neglected. The large group of resolution proponents urge countries and organizations to,
Agenda item 3 (A73/CONF./1 Rev.1) or “COVID-19 response Draft resolution” directly addresses the concerns of many that other major deadly diseases and essential services should not be further neglected. The large group of resolution proponents urge countries and organizations to,
“Maintain the continued functioning of the health system in all relevant aspects, in accordance with national context and priorities, necessary for an effective public health response to the COVID-19 pandemic and other ongoing epidemics, and the uninterrupted and safe provision of population and individual level services, for, among others, communicable diseases, including by undisrupted vaccination programmes, neglected tropical diseases, noncommunicable diseases, mental health, mother and child health and sexual and reproductive health and promote improved nutrition for women and children, recognizing in this regard the importance of increased domestic financing and development assistance where needed in the context of achieving UHC.”
In Provisional agenda item 23 (A73/32) “Progress reports by the Director-General” we find updates on guinea worm eradication and the burden of snakebite envenoming. The report notes the situation in 2019, which is a far cry from the millions of cases in the 1980d when the dracunculiasis eradication effort was launched. “In 2019, three countries reported a total of 53 human indigenous cases of dracunculiasis (guinea-worm disease), namely, Angola (one case), Chad (48 cases) and South Sudan (four cases), from a total of 28 villages. Cameroon reported one human case, probably imported from Chad.”
It is important to note that, “The global dracunculiasis eradication campaign is based on both community and country-focused interventions,” where community members play an important role in surveillance and notification. This includes at-risk and border areas, as is being done in Cameroon. The challenge of human Dracunculus medinensis infection in dogs continues and points to the importance of One Health in the control and elimination of NTDs. Surveillance is not cheap, and the report stresses that funds are still needed so that international partners can continue to ensure that the last case of guinea worm is detected and contained.
Moving from the smaller serpent to the larger variety, the report recalls the May 2018 World Health Assembly resolution WHA71.5 on addressing the burden of snakebite envenoming. A global strategy, “Snakebite envenoming: a strategy for prevention and control” was launched in in May 2019. The WHO Secretariat has “fostered international efforts to improve the availability, accessibility and affordability of safe and effective antivenoms for all, through assessments of antivenom manufacturing, training programs and stockpile procedures.
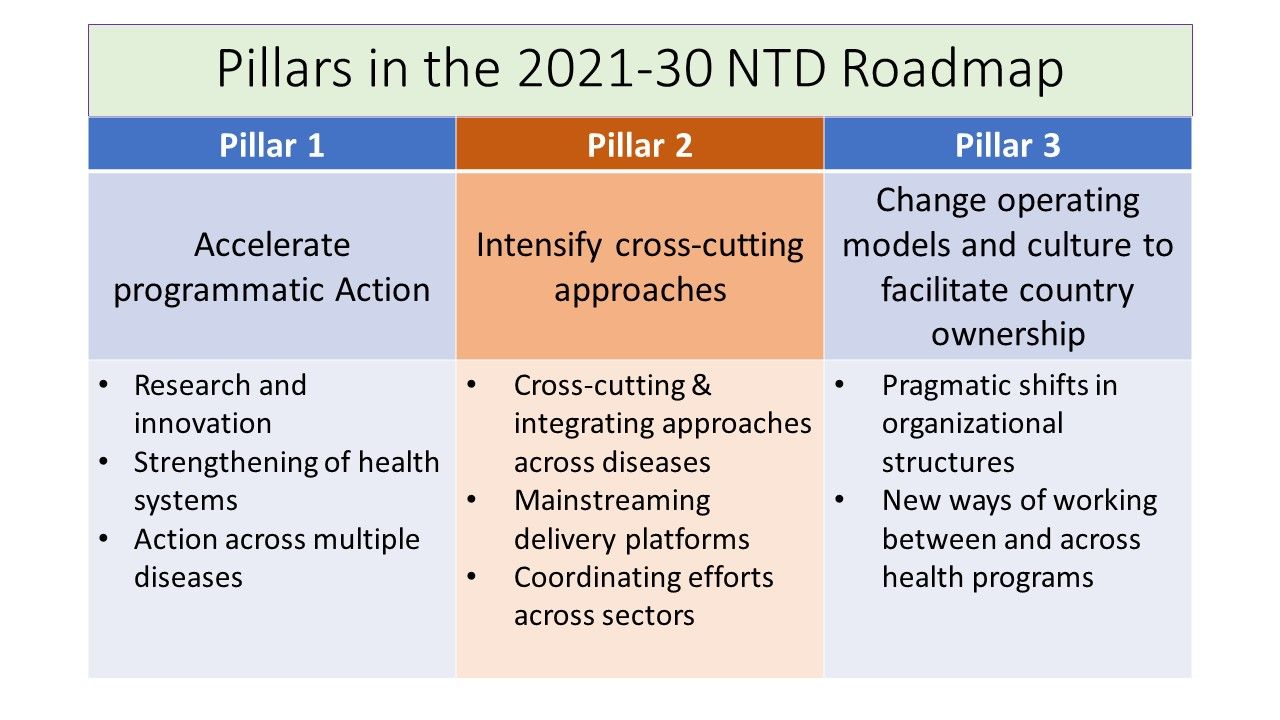 Finally, provisional agenda item 11.8 (A73/8) addresses a “Draft road map for neglected tropical diseases 2021–2030.” This builds on resolution WHA66.12 (2013) on WHO’s earlier road map for accelerating work to overcome the global impact of neglected tropical diseases (2012–2020). The proposed interventions build on important principles including:
Finally, provisional agenda item 11.8 (A73/8) addresses a “Draft road map for neglected tropical diseases 2021–2030.” This builds on resolution WHA66.12 (2013) on WHO’s earlier road map for accelerating work to overcome the global impact of neglected tropical diseases (2012–2020). The proposed interventions build on important principles including:
- Tackling neglected tropical diseases through support of the vision of universal health coverage
- Adopting grassroots approaches that enable access to some of the world’s poorest, hard-to reach communities and people affected by complex emergencies
- Monitoring progress against neglected tropical diseases as a litmus test of progress towards the achievement of universal health coverage
The report notes that “40 countries, territories and areas have eliminated at least one neglected tropical disease,” most notably dracunculiasis (as mentioned above, lymphatic filariasis and trachoma. Although “substantive progress has been made since 2012, it is evident that not all of the 2020 targets will be met.” Hence, a new draft road map for neglected tropical diseases for 2021–2030 is required. The three pillars supporting the new roadmap are outlined in the attached figure.
It is good to know that the 73rd World Health Assembly will not be completely overshadowed by COVID-19 and politics. Efforts to sustain and improve NTD control and elimination must not be jeopardized.
coronavirus &COVID-19 &Ebola &Elimination &iCCM &IPTi &IPTp &IRS &ITNs &Research Bill Brieger | 25 Apr 2020
Zero Malaria Starts after Lockdown?
 The novel 2019 coronavirus, also known as COVID-19 and SARS-COV2, is casting a heavy shadow over the 2020 World Malaria Day. People are trying to remain upbeat declaring the tagline “zero malaria starts with me,” but nothing can hide the fear that the current pandemic will both disrupt the current delivery of essential malaria preventive and treatment services, but will have longer term impacts on malaria funding and our capacity to learn new ways to reach malaria elimination goals. As we can see in the graphic to the right, accessible, lifesaving, community-based services may be especially hard hit.
The novel 2019 coronavirus, also known as COVID-19 and SARS-COV2, is casting a heavy shadow over the 2020 World Malaria Day. People are trying to remain upbeat declaring the tagline “zero malaria starts with me,” but nothing can hide the fear that the current pandemic will both disrupt the current delivery of essential malaria preventive and treatment services, but will have longer term impacts on malaria funding and our capacity to learn new ways to reach malaria elimination goals. As we can see in the graphic to the right, accessible, lifesaving, community-based services may be especially hard hit.
 Another ironic image is the indoor residual spray (IRS) team member with a face mask needed for protection from the insecticides being sprayed. When will such teams be able to go back into homes? When can household members actually pack out their belongings so that spraying can commence? When will such masks not be needed for intensive care COVID-19 case management instead?
Another ironic image is the indoor residual spray (IRS) team member with a face mask needed for protection from the insecticides being sprayed. When will such teams be able to go back into homes? When can household members actually pack out their belongings so that spraying can commence? When will such masks not be needed for intensive care COVID-19 case management instead?
WHO is urging “countries to move quickly to save lives from malaria in sub-Saharan Africa” because “New analysis supports the WHO call to minimize disruptions to malaria prevention and treatment services during the COVID-19 pandemic.” This will be difficult in high burden countries like Nigeria that are already on lockdown with over 1,000 coronavirus cases detected already. Modeling by WHO and partners has projected, “Severe disruptions to insecticide-treated net campaigns and in access to antimalarial medicines could lead to a doubling in the number of malaria deaths in sub-Saharan Africa this year compared to 2018.”
 The Global Malaria Program offers guidance for tailoring malaria interventions to the present circumstances. Great concern is drawn from previous epidemic situations when observing that, “it is essential that other killer diseases, such as malaria, are not ignored. We know from the recent Ebola outbreak in west Africa that a sudden increased demand on fragile health services can lead to substantial increases in morbidity and mortality from other diseases, including malaria. The COVID-19 pandemic could be devastating on its own – but this devastation will be substantially amplified if the response undermines the provision of life-saving services for other diseases.”
The Global Malaria Program offers guidance for tailoring malaria interventions to the present circumstances. Great concern is drawn from previous epidemic situations when observing that, “it is essential that other killer diseases, such as malaria, are not ignored. We know from the recent Ebola outbreak in west Africa that a sudden increased demand on fragile health services can lead to substantial increases in morbidity and mortality from other diseases, including malaria. The COVID-19 pandemic could be devastating on its own – but this devastation will be substantially amplified if the response undermines the provision of life-saving services for other diseases.”
Specifically, GMP recommends that national malaria programs should ensure the following:
- a focal point for malaria is a member of the National COVID-19 Incident Management Team.
- continued engagement with all relevant national COVID-19 stakeholders and partners.
- continued access to and use of recommended insecticide-treated mosquito nets (ITNs)
- continuation of planned targeted indoor residual spraying (IRS)
- early care-seeking for fever and suspected malaria by the general population to prevent a spike in severe malaria
- access to case management services in health facilities and communities with diagnostic confirmation through rapid diagnostic tests [RDTs]
- treatment of confirmed malaria cases with approved protocols
- continued delivery of planned preventive services normally provided to specific target populations (SMC, IPTi, IPTp)
- the safety of all malaria personnel and their clients in the process of carrying out the above interventions
 In editorial in the American Journal of Tropical Medicine and Hygiene by Yanow and Good address the damaging longer term impact of the present shutdown. “The impacts of research shutdowns will be felt long after the pandemic. Many scientists study diseases that do not share the same obvious urgency as COVID-19 and yet take a shocking toll on human life. For example, malaria infects more than 200 million people and takes the lives of nearly half a million people, mostly young children, each year.1 During laboratory closures and without clinical studies, there will be no progress toward treating and preventing malaria: no progress toward new drugs, vaccines, or diagnostics.”
In editorial in the American Journal of Tropical Medicine and Hygiene by Yanow and Good address the damaging longer term impact of the present shutdown. “The impacts of research shutdowns will be felt long after the pandemic. Many scientists study diseases that do not share the same obvious urgency as COVID-19 and yet take a shocking toll on human life. For example, malaria infects more than 200 million people and takes the lives of nearly half a million people, mostly young children, each year.1 During laboratory closures and without clinical studies, there will be no progress toward treating and preventing malaria: no progress toward new drugs, vaccines, or diagnostics.”
The case for continuing malaria services to save hundreds of thousands of lives is not difficult to make. The actual implementation during lockdowns and quarantines is a management challenge. The importance of malaria testing to provide patients with appropriate care for the right disease is crucial. The question is whether in resource strapped endemic countries these decisions and management arrangements can be made in a timely fashion and for the long term whether the next generation of research can proceed with much needed new medicines and technologies.