Integration &IPTp &Malaria in Pregnancy Bill Brieger | 15 Nov 2016
Joint efforts, a key to success for the Malaria in Pregnancy Program in Luanda, Angola
A poster entitled “Joint efforts, a key to success for the Malaria in Pregnancy Program in Luanda, Angola” was presented by Jhony Juarez, Adolfo Sampaio, William R. Brieger, and Domingos F. Gueve from Jhpiego’s Angola Team at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
 Angola, in response to WHO’s 2012 updated guidance on Intermittent Preventive Treatment in pregnancy (IPTp), revised its national malaria protocol to better address the fact that 25% of maternal mortality is caused by the disease. The new protocol was a collaborative effort of a national technical working group assisting the National Malaria Control Program (NMCP) including the National Reproductive Health Program, the national AIDS Institute, WHO, UNICEF, UNFPA and implementing partners of the U.S. Presidents Malaria Initiative (PMI).
Angola, in response to WHO’s 2012 updated guidance on Intermittent Preventive Treatment in pregnancy (IPTp), revised its national malaria protocol to better address the fact that 25% of maternal mortality is caused by the disease. The new protocol was a collaborative effort of a national technical working group assisting the National Malaria Control Program (NMCP) including the National Reproductive Health Program, the national AIDS Institute, WHO, UNICEF, UNFPA and implementing partners of the U.S. Presidents Malaria Initiative (PMI).
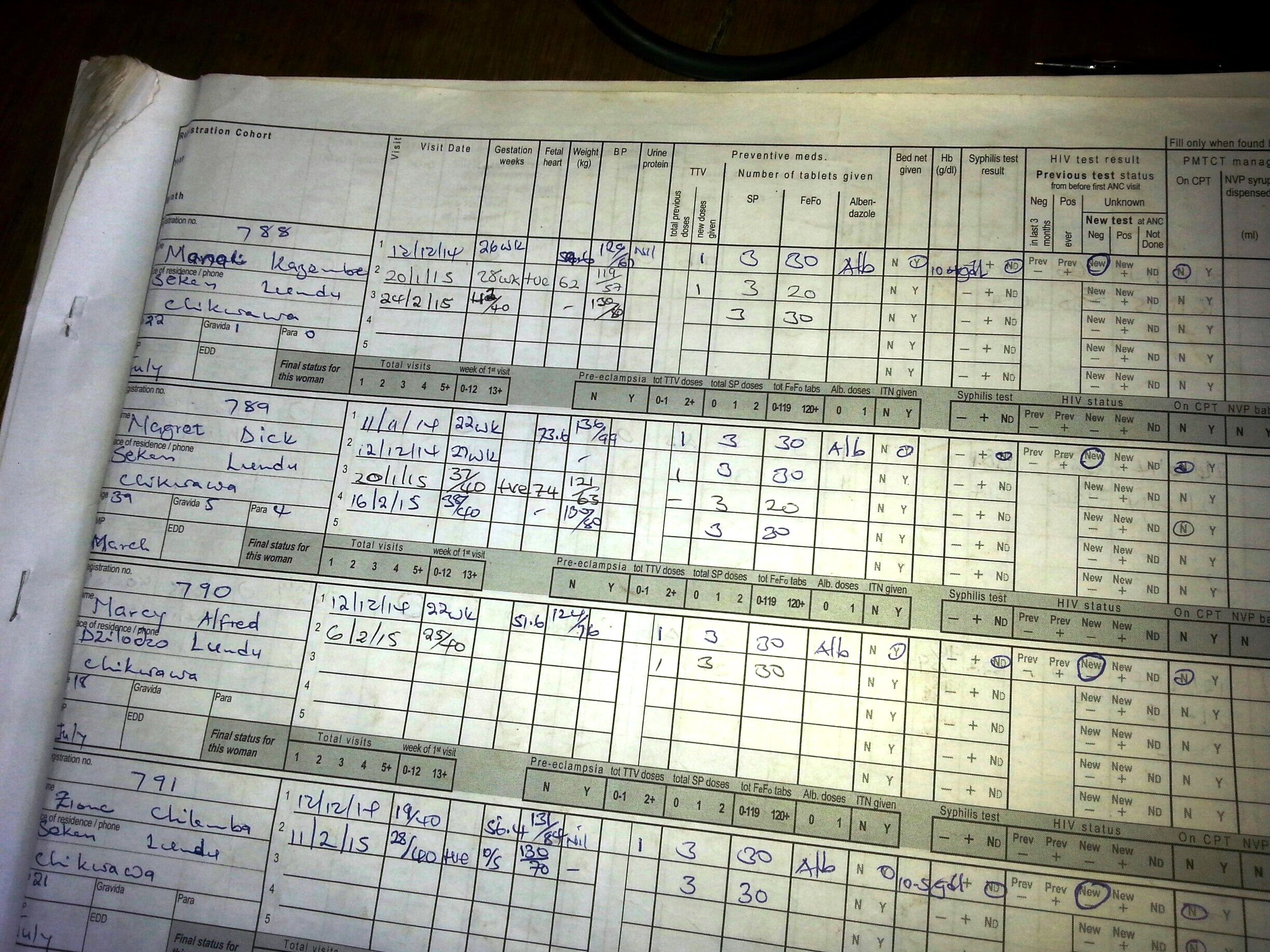
The updated Prevention and Treatment Manual for Malaria in Pregnancy, based on the revised protocol, was approved in 2014, and efforts continued with reviewing and updating training modules, job aids and monitoring tools that would reflect the additional doses of IPTp. The Ministry of Health, with support from partners, then disseminated these materials in the provinces and municipalities where they worked. USAID’s ForçaSaúde program, with support from PMI, worked with the Provincial Health Directorate of Luanda to build capacity of 297 health professionals to implement the new guidance in 78 health facilities of four municipalities, Belas, Cazenga, Cacuaco and Viana, with a combined population of 4.3 million.
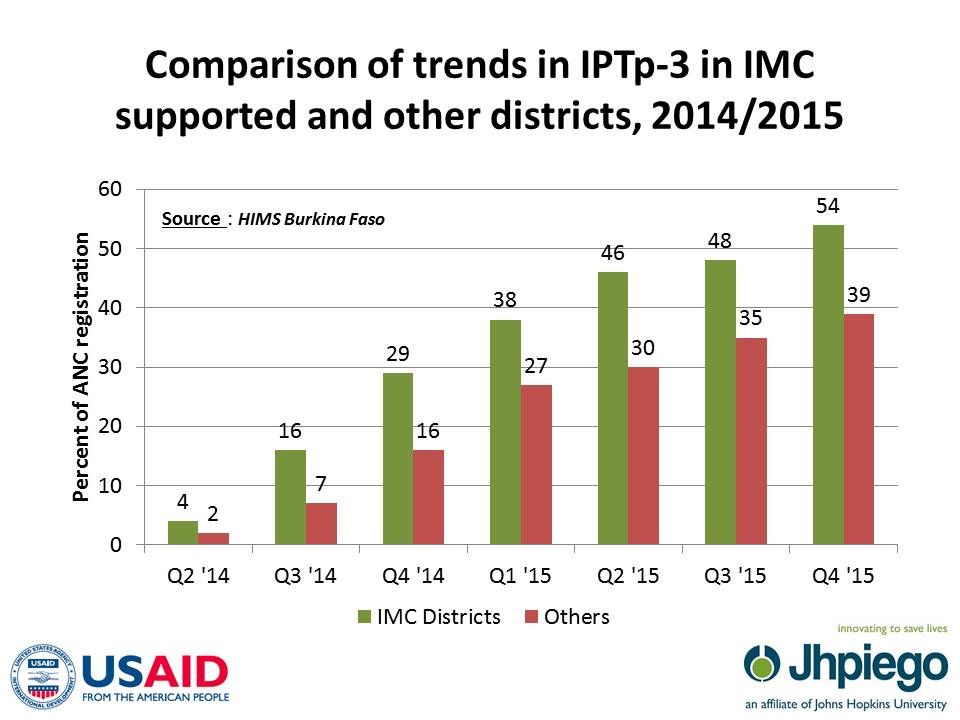
 Comparing the IPTp data from the four municipalities between 2014 and 2015, one can see that the new guidance has started to take effect. In both years approximately 70,000 pregnant women received the first dose or around 60% of women registering for antenatal care (ANC). For the new third dose there was an increase of 85% (from 12,490 women to 23,046), and receipt of the fourth dose rose by 164% (3,345 to 8,839).
Comparing the IPTp data from the four municipalities between 2014 and 2015, one can see that the new guidance has started to take effect. In both years approximately 70,000 pregnant women received the first dose or around 60% of women registering for antenatal care (ANC). For the new third dose there was an increase of 85% (from 12,490 women to 23,046), and receipt of the fourth dose rose by 164% (3,345 to 8,839).
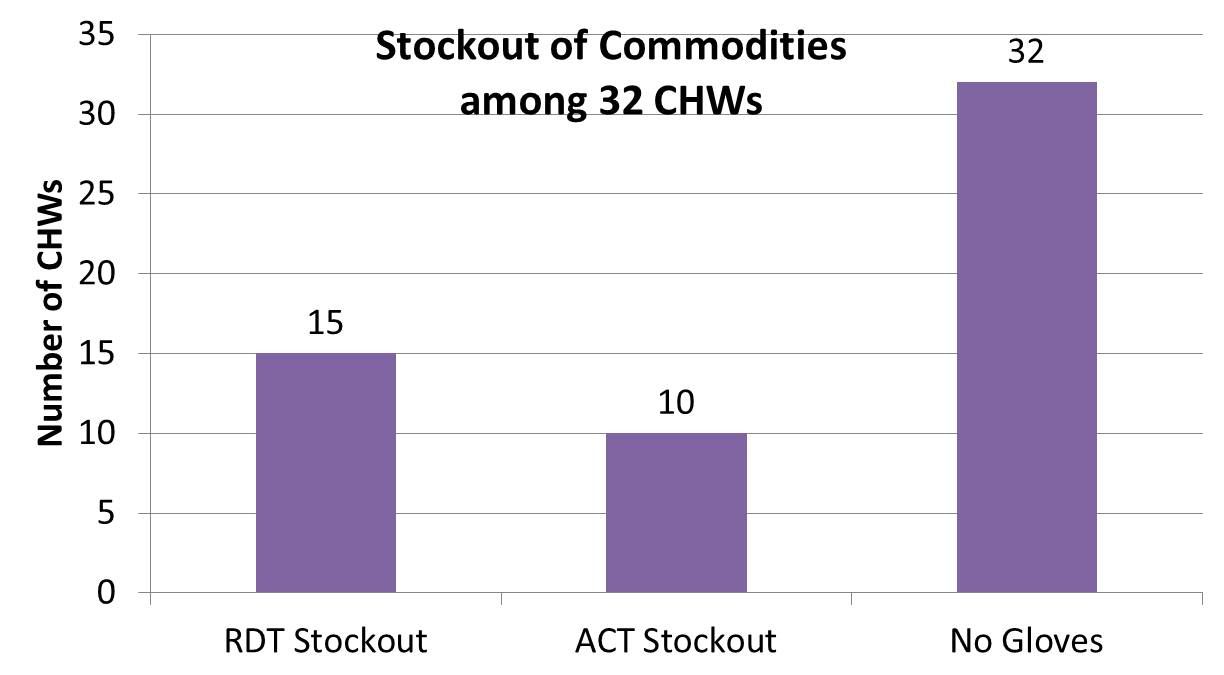
Two major challenges remain: increasing ANC registration and addressing missed opportunities to provide ANC doses for those who do attend including ensuring regular supplies of sulfadoxine-pyrimethamine for IPTp. Future progress requires continued inter-departmental collaboration among NMCP, Reproductive Health and the AIDs Institute, on-the-job training, enhanced statistical capacity, and supervision.