Ebola &Infection Prevention Bill Brieger | 30 Oct 2018
Institutionalizing Infection Prevention and Control: Post-Ebola Experience in Liberian Health Facilities
 Allyson R. Nelson, Anne Fiedler,Topian Zikeh, Nancy Moses, Chandrakant Ruparelia, Lolade Oseni, Mantue Reeves, and Birhanu Getahun presented the work of the Maternal and Child Survival Project in preventing infection among health workers during Ebola and other infectious disease outbreaks. Their efforts are shared below.
Allyson R. Nelson, Anne Fiedler,Topian Zikeh, Nancy Moses, Chandrakant Ruparelia, Lolade Oseni, Mantue Reeves, and Birhanu Getahun presented the work of the Maternal and Child Survival Project in preventing infection among health workers during Ebola and other infectious disease outbreaks. Their efforts are shared below.
 Ebola virus disease (EVD) outbreak in 2014–2015 affected an estimated 4% of the Liberian health workforce. 372 health workers contracted EVD, and 184 died. EVD outbreak and transmission between health care workers and clients highlighted critical gaps in health facilities, especially infection prevention (IPC) practices including waste, water, and triage infrastructure.
Ebola virus disease (EVD) outbreak in 2014–2015 affected an estimated 4% of the Liberian health workforce. 372 health workers contracted EVD, and 184 died. EVD outbreak and transmission between health care workers and clients highlighted critical gaps in health facilities, especially infection prevention (IPC) practices including waste, water, and triage infrastructure.
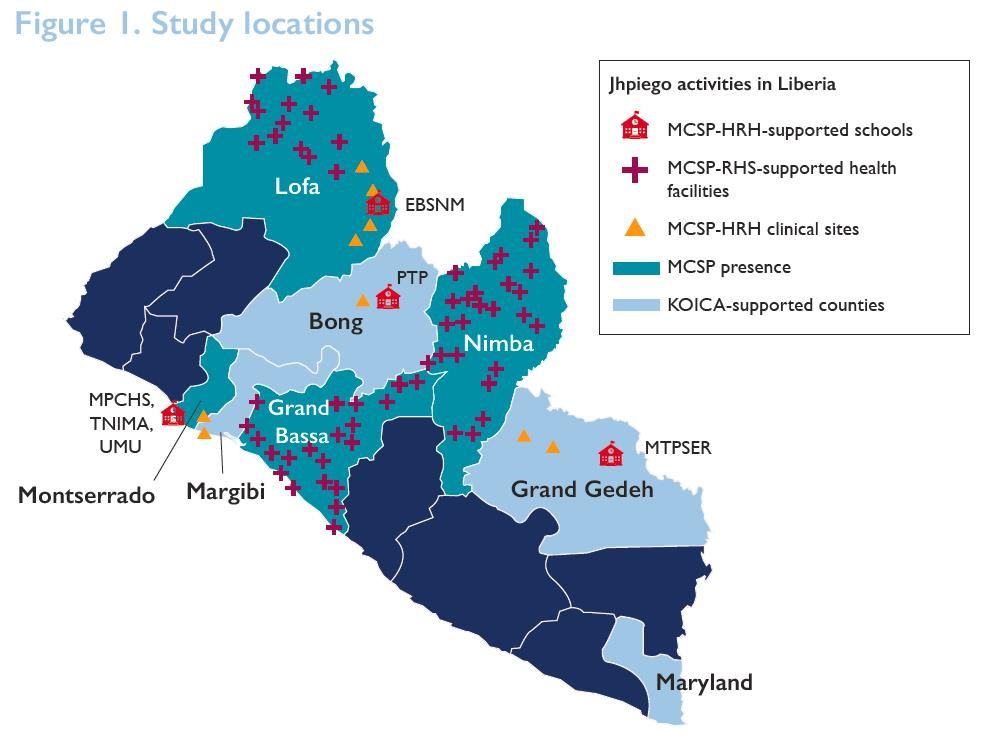
 Liberia’s ministry of health (MOH), with support from Jhpiego and other partners, developed and introduced IPC standards in 2015. Through funding from the Office of U.S. Foreign Disaster Assistance (OFDA), Korea International Cooperation Agency (KOICA), and the United States Agency for International Development’s Maternal and Child Survival Program (MCSP), Jhpiego worked with the MOH to achieve and maintain adherence to IPC standards in over 200 health facilities from 2015 to 2017.
Liberia’s ministry of health (MOH), with support from Jhpiego and other partners, developed and introduced IPC standards in 2015. Through funding from the Office of U.S. Foreign Disaster Assistance (OFDA), Korea International Cooperation Agency (KOICA), and the United States Agency for International Development’s Maternal and Child Survival Program (MCSP), Jhpiego worked with the MOH to achieve and maintain adherence to IPC standards in over 200 health facilities from 2015 to 2017.
 Capacity-building was central to addressing the problem. The team identified critical gaps in skills, infrastructure, supplies hindering adherence to IPC standards. They developed and rolled out standard operating procedures for clinical and nonclinical settings.
Capacity-building was central to addressing the problem. The team identified critical gaps in skills, infrastructure, supplies hindering adherence to IPC standards. They developed and rolled out standard operating procedures for clinical and nonclinical settings.
Partners provided IPC supplies including personal protective equipment (PPE), 90 hand hygiene buckets, Soap, Gloves, 50 waste containers, Rain boots, and Sharps containers.
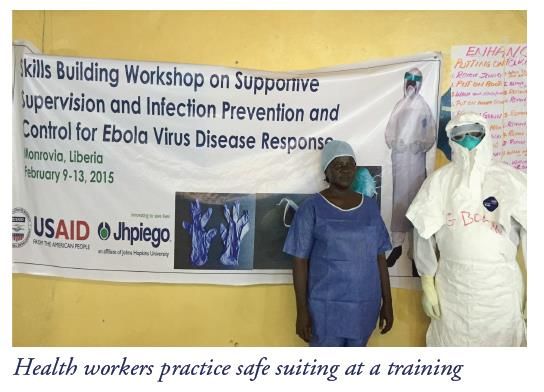 Capacity building included Training (clinical and support personnel). 278 existing health facility staff members as IPC focus points for daily monitoring (OFDA) were trained. Additionally 1,065 health facility staff were trained in Keep Safe Keep Serving IPC and emergency response training (OFDA). Onsite IPC management teams were established in 210 facilities (KOICA and MCSP). Also health workers were offered onsite refresher trainings.
Capacity building included Training (clinical and support personnel). 278 existing health facility staff members as IPC focus points for daily monitoring (OFDA) were trained. Additionally 1,065 health facility staff were trained in Keep Safe Keep Serving IPC and emergency response training (OFDA). Onsite IPC management teams were established in 210 facilities (KOICA and MCSP). Also health workers were offered onsite refresher trainings.
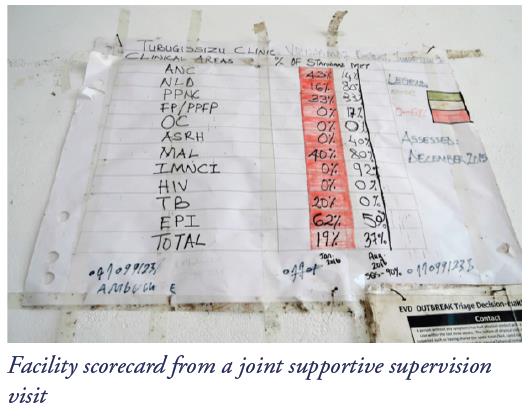 Supportive supervision, mentoring, and coaching were capacity building interventions. 50 district health officers and supervisors were trained in eight counties in supportive supervision, mentoring, and coaching (OFDA). They co-conducted, with district and county health staff, 7,980 weekly and 2,280 monthly supportive supervision visits (OFDA). IPC practices were monitored against the MOH’s IPC minimum standards tool monthly, with scoring, feedback to clinicians and supervisors, and development of action plans for improvement of gaps. Onsite mentoring and coaching was provided on adherence using IPC minimum standards tool at least four times yearly (KOICA and MCSP).
Supportive supervision, mentoring, and coaching were capacity building interventions. 50 district health officers and supervisors were trained in eight counties in supportive supervision, mentoring, and coaching (OFDA). They co-conducted, with district and county health staff, 7,980 weekly and 2,280 monthly supportive supervision visits (OFDA). IPC practices were monitored against the MOH’s IPC minimum standards tool monthly, with scoring, feedback to clinicians and supervisors, and development of action plans for improvement of gaps. Onsite mentoring and coaching was provided on adherence using IPC minimum standards tool at least four times yearly (KOICA and MCSP).
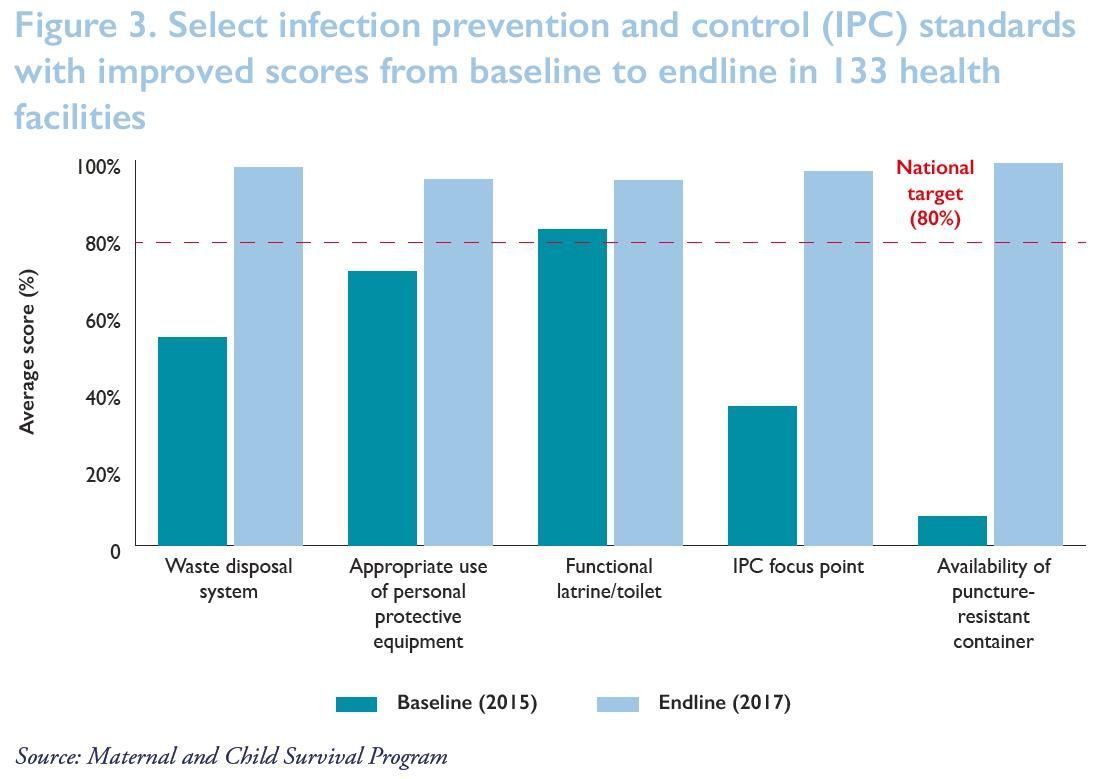
 As a result of the intervention Clinicians and support personnel at program-supported health care facilities adopted, adhered to, and maintained proper IPC practices. This enabled them to provide safe services and evidenced by IPC scores from the Safe, Quality Health Services IPC standards tool. Out of 131 health facilities at endline 99% improved their waste disposal, particularly the availability and use of puncture-resistant sharps containers for the safety of cleaning staff. All (100%) had in place and were using a clear protocol for management and disposal of waste. 98% were segregating waste for safe disposal and management to avoid contamination and spread of infectious disease. 94% had a functional latrine/toilet. All (100%) had operational IPC focus points ensuring adherence to IPC practices. In 95%, staff were regularly using risk-appropriate personal protective equipment during routine care.
As a result of the intervention Clinicians and support personnel at program-supported health care facilities adopted, adhered to, and maintained proper IPC practices. This enabled them to provide safe services and evidenced by IPC scores from the Safe, Quality Health Services IPC standards tool. Out of 131 health facilities at endline 99% improved their waste disposal, particularly the availability and use of puncture-resistant sharps containers for the safety of cleaning staff. All (100%) had in place and were using a clear protocol for management and disposal of waste. 98% were segregating waste for safe disposal and management to avoid contamination and spread of infectious disease. 94% had a functional latrine/toilet. All (100%) had operational IPC focus points ensuring adherence to IPC practices. In 95%, staff were regularly using risk-appropriate personal protective equipment during routine care.
Lessons learned from the intervention showed the importance of the following efforts:
- Comprehensive support is needed to improve adherence to infection prevention and control (IPC) standard practices:
- Capacity-building among health facility staff
- Infrastructure upgrades
- Provision/availability of IPC supplies
- To maintain that adherence after the immediate threat has passed and thus mitigate potential future outbreaks, health facilities need:
- Continuous hands-on mentoring
- Upgraded IPC infrastructure for reproductive, maternal, newborn, child, and adolescent health services
- Changes in behavior and attitudes of health facility staff
- Regular and rigorous data collection and feedback
 This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Abbreviations: EBSNM, Esther Bacon School of Nursing and Midwifery; HRH, Human Resources for Health; KOICA, Korea International Cooperation Agency; MCSP, Maternal and Child Survival Program; MPCHS, Mother Patern College of Health Sciences; MTPSER, Midwifery Training Program-Southeastern Region; PTP, Phebe Paramedical Training Program; RHS, Restoration of Health Services; TNIMA, Tubman National Institute of Medical Arts; UMU, United Methodist University