Community &IPTp &Malaria in Pregnancy Bill Brieger | 08 Nov 2017
Baseline for Coverage of Intermittent Preventive Treatment of Malaria in Pregnancy for Planning Community Interventions in Burkina Faso

Under supervision from health center Community Health Worker provides SP for IPTp to Pregnant Woman
Now that the World Health Organization recommends that pregnant women in high and stable malaria transmission areas receive three or more doses of Intermittent Preventive Treatment (IPTp) with Sulfadoxine-pyrimethamine, it is necessary to learn ways to reach more women with this intervention. William R. Brieger, Mathurin Dodo, Danielle Burke, Ousmane Badolo, Justin Tiendrebeogo, Kristen Vibbert, Susan J Youll, and Julie R Gutman conducted a baseline household survey of recently pregnant women in Burkina Faso to learn about the extent of current IPTp coverage and where improvements are needed. With support from the US President’s Malaria Initiative and the USAID Maternal and Child Survival Program Their findings were made available at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
The World Health Organization recommends intermittent preventive treatment (IPTp) to prevent the adverse effects of malaria in pregnancy in high burden settings; IPTp coverage has lagged behind international targets. In Burkina Faso, the 2014 Malaria Indicator Survey found that 22% of women received 3 or more doses of IPTp (IPTp3). In 2014, Burkina Faso’s IPTp policy was updated from recommending 2 doses to providing at least 3 doses of IPTp. Prior studies have suggested that use of community health workers to deliver IPTp can increase coverage.
 To improve IPTp coverage, we will pilot community delivery of IPTp within 3 southern districts: Po, Ouargaye, and Batie. Here we report results from a baseline assessment in the selected districts. Health Management Information System (HMIS) data for 2015 were collected in each district, and IPTp3 coverage was 37%. Four health facilities per district were randomly selected to participate in the pilot. In 2017, a baseline household survey was conducted among recently pregnant women in the catchment areas of these health facilities.
To improve IPTp coverage, we will pilot community delivery of IPTp within 3 southern districts: Po, Ouargaye, and Batie. Here we report results from a baseline assessment in the selected districts. Health Management Information System (HMIS) data for 2015 were collected in each district, and IPTp3 coverage was 37%. Four health facilities per district were randomly selected to participate in the pilot. In 2017, a baseline household survey was conducted among recently pregnant women in the catchment areas of these health facilities.
 Women were asked to recall the number of antenatal care (ANC) visits and IPTp doses they had received during their most recent pregnancy. The same information was extracted from their ANC cards. A total of 374 women were interviewed during the baseline survey.
Women were asked to recall the number of antenatal care (ANC) visits and IPTp doses they had received during their most recent pregnancy. The same information was extracted from their ANC cards. A total of 374 women were interviewed during the baseline survey.
ANC attendance was reported to be 98% for any visit, and 84% for four visits; these rates were 90% and 62% as documented on the ANC cards. Over 95% of women recalled receiving the first dose of IPTp, while over 80% of cards verified that the first dose was given.
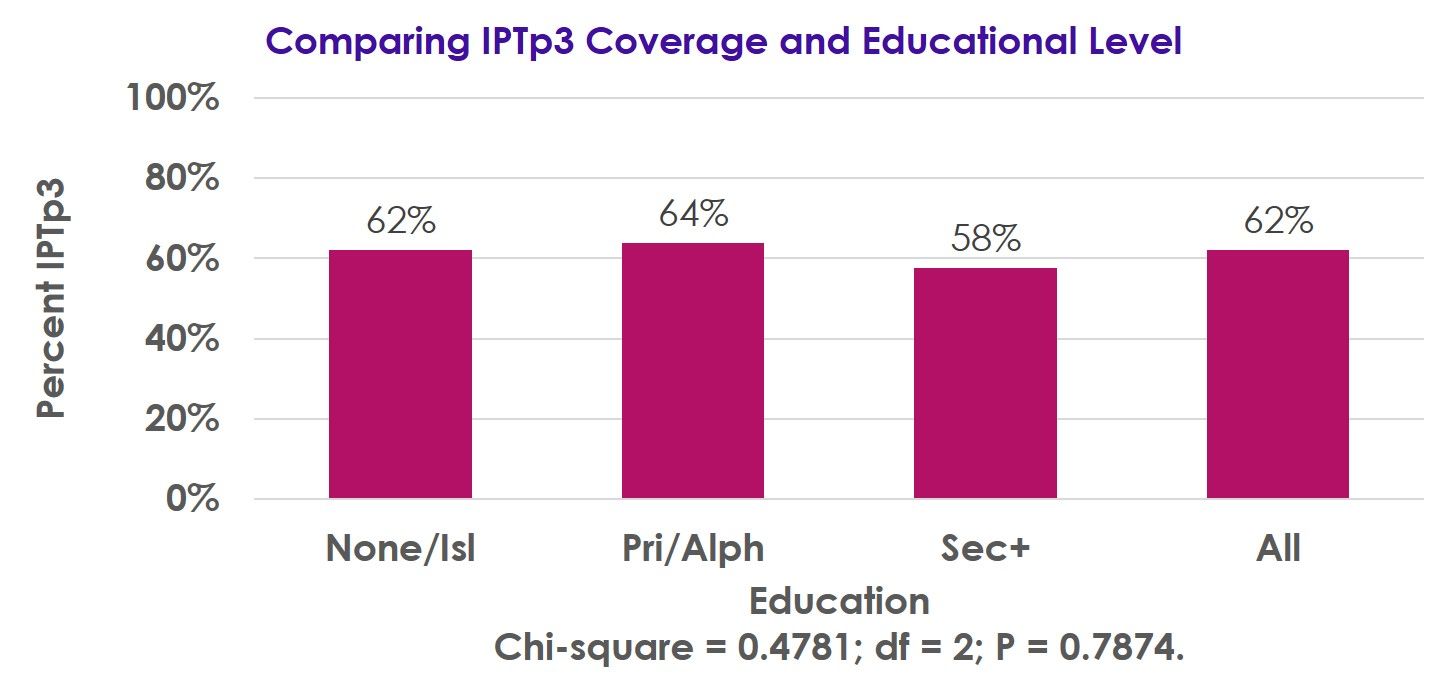 Receipt of the third IPTp dose was 62% by recall and 52% as recorded on the ANC cards, while receipt of 4 doses was 32% by recall and 19% per the ANC cards. IPTp3 coverage was not associated with parity or educational level.
Receipt of the third IPTp dose was 62% by recall and 52% as recorded on the ANC cards, while receipt of 4 doses was 32% by recall and 19% per the ANC cards. IPTp3 coverage was not associated with parity or educational level.
Following implementation of the revised IPTp policy, there has been a substantial improvement in IPTp coverage, though more work is needed to achieve the national 85% coverage target.
Our pilot will examine the impact that delivery of IPTp by community workers has on IPTp coverage, with endline surveys planned for 2018.
Health Systems &Quality of Services Bill Brieger | 08 Nov 2017
Enhancing Core Competencies & Improving Midwifery Quality of Care in Lake Zone, Tanzania
 With support from USAID’s Maternal and Child Survival Project in Tanzania Annamagreth Mukwenda, John George George, Mary Rose Giatas, Agrey Mbilinyi, Gustav Moyo, and Justine Ngenda have been addressing the quality of case and services provided by midwives. Their poster at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene is summarized below.
With support from USAID’s Maternal and Child Survival Project in Tanzania Annamagreth Mukwenda, John George George, Mary Rose Giatas, Agrey Mbilinyi, Gustav Moyo, and Justine Ngenda have been addressing the quality of case and services provided by midwives. Their poster at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene is summarized below.
 In sub-Saharan Africa, maternal mortality is unacceptably high accounting for 56% of all maternal deaths. Tanzania is not different. It is estimated that five in every 100 children die before their first birthdays and that four women out of 1000 live births die due to pregnancy related causes.
In sub-Saharan Africa, maternal mortality is unacceptably high accounting for 56% of all maternal deaths. Tanzania is not different. It is estimated that five in every 100 children die before their first birthdays and that four women out of 1000 live births die due to pregnancy related causes.
With prompt recognition and timely intervention most maternal and neonatal deaths can be avoided. Access to skilled care at these critical times save lives.
 A new initiative is working to improve midwifery care by building capacity of training institutions to prepare highly skilled nurse-midwives to enhance on job live saving skills.
A new initiative is working to improve midwifery care by building capacity of training institutions to prepare highly skilled nurse-midwives to enhance on job live saving skills.
In 2014 A collaboration between the Tanzania Ministry of Health, Jhpiego through Maternal child survival program (MCSP), conducted a baseline assessment to assess the quality of midwifery pre-service education to adequately prepare students with the clinical skills to provide competent nursing and midwifery care.
Four nursing and midwifery schools from two regions of Lake Zone were assessed to identify issues affecting the schools’ ability to produce clinically competent graduates in nursing and midwifery. Among things, the assessment focused on tutors and recent graduates, with findings showing critical deficit on content/skill competencies.
 To address these challenges, midwifery tutors from 9 schools (100%) were updated in high impact midwifery interventions through trainings and supportive supervision including coaching and mentorship. Skills labs were also equipped with all mannequins necessary for midwifery training.
To address these challenges, midwifery tutors from 9 schools (100%) were updated in high impact midwifery interventions through trainings and supportive supervision including coaching and mentorship. Skills labs were also equipped with all mannequins necessary for midwifery training.
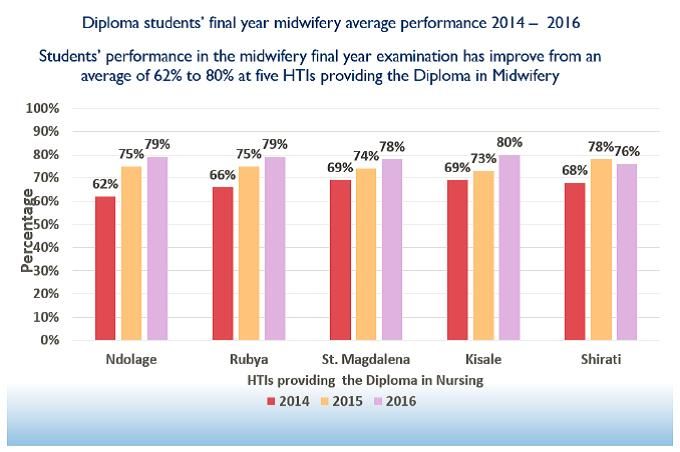
The program is in the third year of implementation with tremendous improvement in midwifery training as evidenced by students final examination results as well as tutors’ and students’ testimonies.
Experience of MCSP approach to strengthen competencies of graduates has contributed to improve midwifery quality of care to reduce maternal deaths in Tanzania.
Case Management &Health Workers &Training Bill Brieger | 08 Nov 2017
Health provider orientation to national malaria case management guidelines in regional hospitals in Burkina Faso
 Good clinical practice in managing malaria requires awareness and understanding of national case management guidelines. Moumouni Bonkoungou, Ousmane Badolo, and Thierry Ouedraogo of Jhpiego in Collaboration with the National Malaria Control Program and sponsorship from the “Improving Malaria Care” project of USAID/PMI explain how health workers in Burkina Faso were oriented to the national guidelines at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. They have found that short orientations are less expensive and reach more health workers that traditional training sessions.
Good clinical practice in managing malaria requires awareness and understanding of national case management guidelines. Moumouni Bonkoungou, Ousmane Badolo, and Thierry Ouedraogo of Jhpiego in Collaboration with the National Malaria Control Program and sponsorship from the “Improving Malaria Care” project of USAID/PMI explain how health workers in Burkina Faso were oriented to the national guidelines at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. They have found that short orientations are less expensive and reach more health workers that traditional training sessions.
Malaria remains the leading cause of consultations, hospitalization and death in health facilities in Burkina Faso. In 2015, 23,634 cases of severe malaria were recorded in hospitals with 1,634 deaths, a mortality rate of 7% at this level compared to 1% nationally. Since April 2014, 1,819 providers from 49 districts have been trained in malaria case management, specifically at the first level (health center – CSPS). Conversely, at referral centers – medical centers with surgical units (CMA), regional hospitals (CHR) and university hospitals (CHU) – providers are not well educated on the new WHO guidelines for malaria prevention and case management.

Health worker orientation session
This situation led the United States Agency for International Development-supported Improving Malaria Care (IMC) project and the National Malaria Control Program (NMCP) to organize orientation sessions for providers in 8 CHR in September 2016. The sessions were conducted by trainers at the national level, supported by clinicians from hospitals including pediatricians and gynecologists.
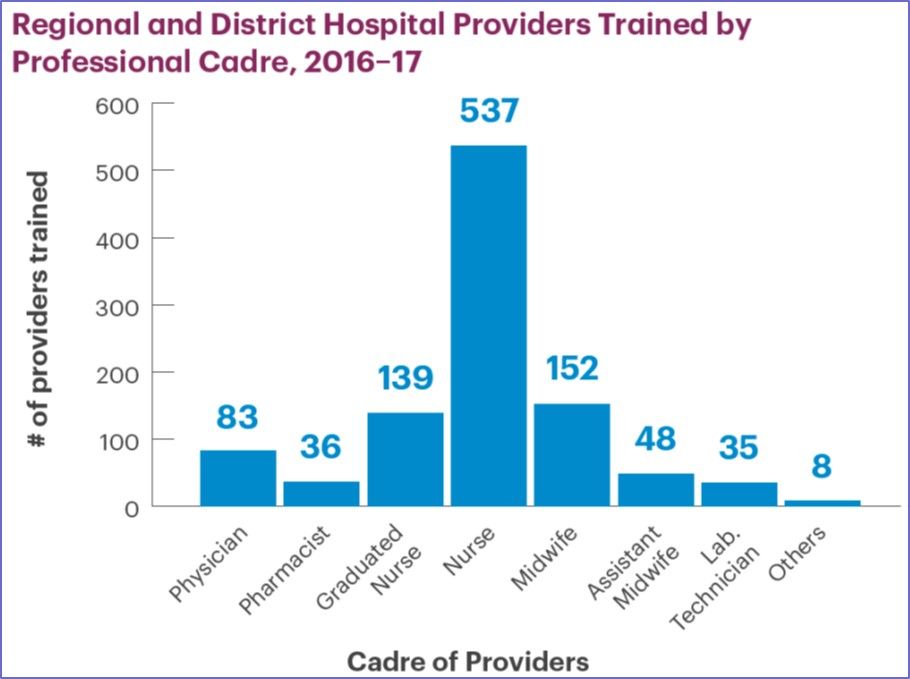
A total of 298 health workers were oriented, including 24 physicians, 157 nurses, 56 midwives, as well as pharmacists and laboratory technicians. 39% of participants were female and 43% have less than 5 years of service in these hospitals. The sessions have provided participants with an opportunity to familiarize themselves with the new guidelines for malaria prevention and case management.
 The orientations have also made it possible to identify the difficulties encountered by referral structures in malaria case management, which include: insufficient staff, inadequate capacity building, no blood bank in some hospitals, reagent stock-outs, inadequacies in the referral system, and insufficient equipment.
The orientations have also made it possible to identify the difficulties encountered by referral structures in malaria case management, which include: insufficient staff, inadequate capacity building, no blood bank in some hospitals, reagent stock-outs, inadequacies in the referral system, and insufficient equipment.
To address these difficulties, staff redeployment, internal supervision, development of tools to monitor reagents stocks have been proposed. To move forward, response plans for the period of high malaria transmission is expected to be developed for these referral facilities.
Health Information &Malaria in Pregnancy Bill Brieger | 07 Nov 2017
Improving Quality of Data to Advance Malaria in Pregnancy Indicator Coverage in Ebonyi State, Nigeria
Progress in preventing malaria in pregnancy depends on good data. Bright Orji, Gladys Olisaekee, Onyinye Udenze, Enobong Umoekeyo, Chika Nwankwo, Boniface Onwe, Chibugo Okoli, and Emmanuel Otolorin of Jhpiego discussed ways to improve data quality in Nigeria at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene with support from the USAID Maternal and Child Health Program. A summary of their points follows:

Reviewing Health Facility Data
Quality data are crucial for informed decision-making to address health challenges and improve malaria service delivery among countries on the pathway to malaria elimination. This emphasis on better data quality was reflected in the World Malaria Day theme of “Counting Malaria Out” in 2009 and 2010.
In Nigeria, improving malaria data quality has been difficult due to critical health system challenges including poor coordination across different departments, institutional complexities, and a shortage of medical record officers and service providers sufficiently trained in data visualization and use of data for decision-making. In response, the Maternal and Child Health Survival Program (MCSP) in Nigeria embarked on the implementation of key activities to improve quality of malaria data in Ebonyi State.
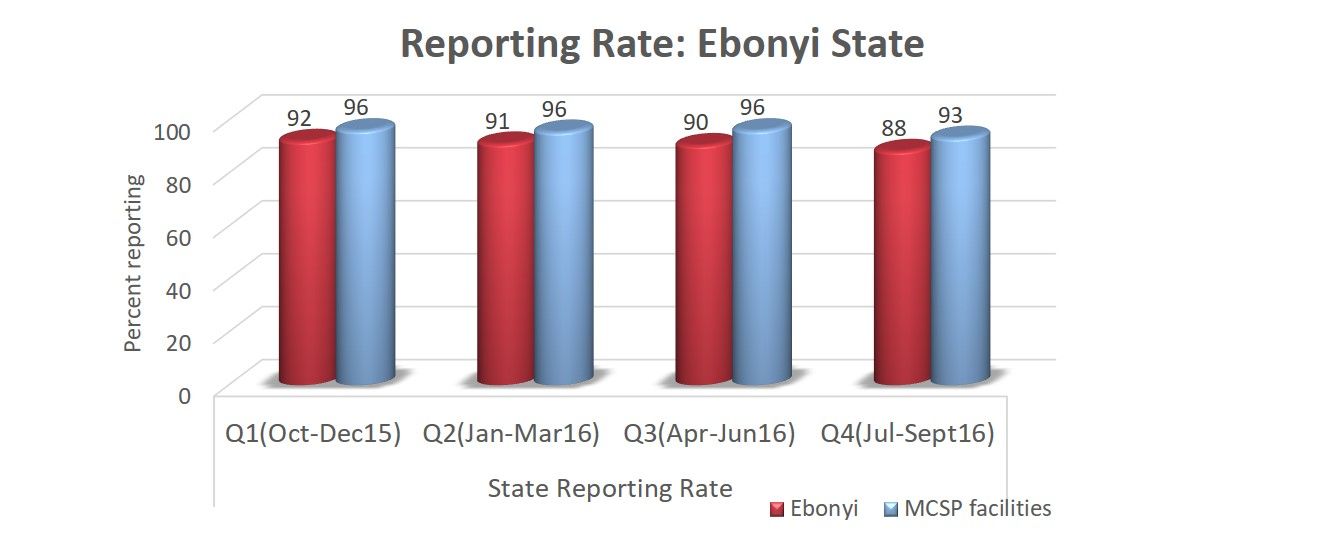 These activities included training on record keeping and use of data for decision-making; post training follow-up; dash boards at the frontline for better data visualization; monthly data collation meetings; improved synergy among service departments; and quarterly data quality assurance visits. As a result, more than 75% of facilities graphed malaria indicators thereby increasing data visualization and use of data for decision-making.
These activities included training on record keeping and use of data for decision-making; post training follow-up; dash boards at the frontline for better data visualization; monthly data collation meetings; improved synergy among service departments; and quarterly data quality assurance visits. As a result, more than 75% of facilities graphed malaria indicators thereby increasing data visualization and use of data for decision-making.
An example of data improvements leading to service increases was Intermittent Preventive Treatment for malaria in pregnancy (IPTp). IPTp1 service statistics in MCSP-supported facilities improved from 54.1% in Oct-Dec 2015 to 81.3% by Jul-Sept 2016 compared to 54.7% to 67.8% in the same periods for non-MCSP facilities.
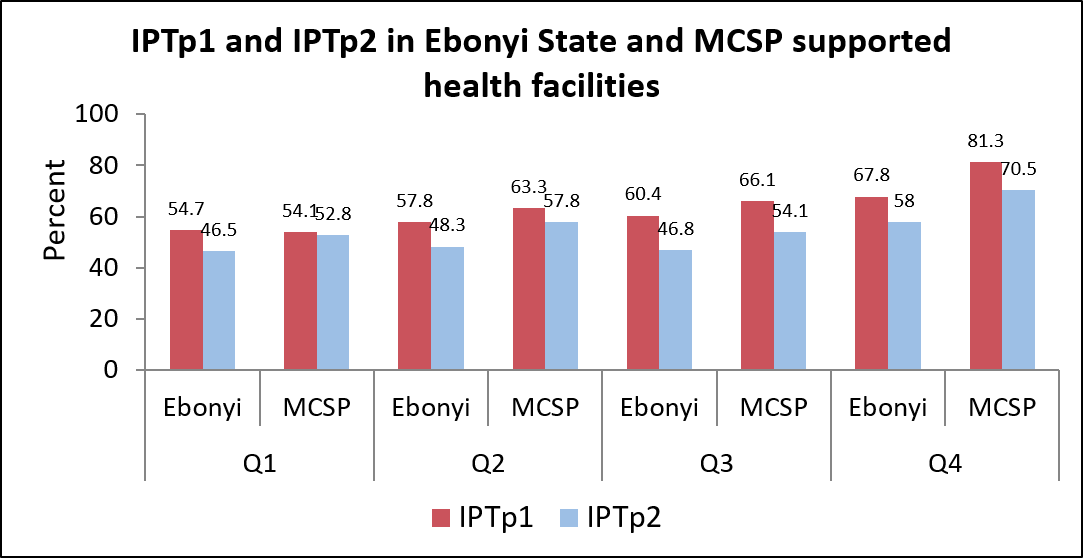 Similarly, IPTp2 service statistics in MCSP-supported facilities improved from 52.8% to 70.5%compared to 46.5% to 58.0% in the same period for non-MCSP facilities.
Similarly, IPTp2 service statistics in MCSP-supported facilities improved from 52.8% to 70.5%compared to 46.5% to 58.0% in the same period for non-MCSP facilities.
Data quality improvement interventions such as monthly data collation and validation meetings prior uploading data to DHIS can contribute to improved quality of malaria performance indicators, better coordination between antenatal care, outpatient and pharmacy departments and increased IPTp coverage.
CHW &Community &IPTp &Malaria in Pregnancy Bill Brieger | 07 Nov 2017
Potential Contribution of Community-Based Health Workers to Improving Prevention of Malaria in Pregnancy
 Justin Tiendrebeogo, Ousmane Badolo, Mathurin Dodo, Danielle Burke, and Bill Brieger of Jhpiego have designed and are implementing a study to determine the effect of delivering Intermittent Preventive Treatment for Malaria in Pregnancy through community health workers in Burkina Faso with the support of the US President’s Malaria Initiative and the USAID Maternal and Child Survival Project. They have shared the design and start-up activities for the study at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. A summary follows:
Justin Tiendrebeogo, Ousmane Badolo, Mathurin Dodo, Danielle Burke, and Bill Brieger of Jhpiego have designed and are implementing a study to determine the effect of delivering Intermittent Preventive Treatment for Malaria in Pregnancy through community health workers in Burkina Faso with the support of the US President’s Malaria Initiative and the USAID Maternal and Child Survival Project. They have shared the design and start-up activities for the study at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. A summary follows:
CHW Flipchart Page
The Ministry of Health of Burkina Faso with the support of its partners initiated a study on the feasibility of increasing provision of Intermittent Preventive Malaria Treatment in pregnant women (IPTp) with sulfadoxine-pyrimethamine (SP) by involving existing community-based health workers (CBHWs). As Burkina Faso adopted the WHO recommendations for more doses of IPTp during pregnancy, it was proposed that the challenge of achieving coverage of third, fourth and additional doses could be met using CBHWs.
The approved protocol calls for CBHWs to refer pregnant women to antenatal care (ANC) to receive their first IPTp dose. Subsequent doses at one-month intervals would be provided by trained CBHWs, who would report back to supervising midwives at the ANC clinics. Several steps were taken to gain approval and set up the intervention.
CHW Using Flipchart
First, IPTp data from the health information system was gathered. IPTp coverage based on ANC registration in the 6 intervention clinics was 69% IPTp1, 68% IPTp2, 56% IPTP3, and 1% IPTp4. Similar information was obtained from the 6 control clinic catchment areas. Situation analysis found that while CBHW curriculum stresses the importance of ANC, it does not address IPTp at community level.
In response updated training materials have been developed. The study team also collected information on village size and availability of CBHWs, especially females. Among the villages in the catchment of the 6 intervention ANC clinics, 33 were found to lack female CBHWs.

Supervisory Meeting
As a result, the team needed to recruit additional female CBHWs, as revised national recruitment guidance stressed attainment of primary school certificate over gender, meaning mainly men had been hired previously. Two institutional review boards were involved and suggested the need to address the potential rare side effects of SP and concerns that community IPTp would not detract from ANC clinic attendance.
Since district and clinic level health staff will be involved in implementing the program using the national CBHW program, lessons learned from this effort to expand the work of CBHWs in preventing malaria in pregnancy should be applicable and adaptable to the whole country.
Uncategorized Bill Brieger | 07 Nov 2017
Data use for malaria decision-making through data monitoring posters in Kribi Cameroon
Kodjo Morgah, Eric M. Tchinda, and Naibei Mbaïbardoum of Jhpiego based in Chad and Cameroon have been building the capacity of health workers to use malaria data to improve services. A summary of their experiences as seen below is being presented at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Cameroon Malaria is the leading cause of morbidity and mortality in Cameroon, where an estimated 500,000 cases occur every year and led to 55% of hospitalizations and 241 deaths among pregnant women in 2010.
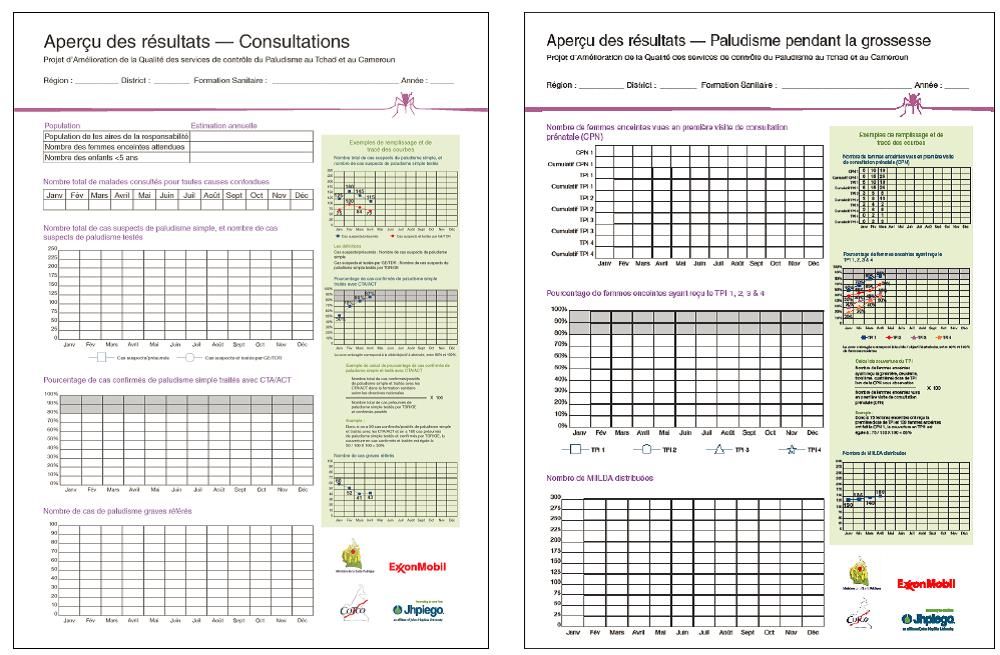 In order to measure the long-term impact of malaria prevention and treatment interventions at the facility level through outcome indicators, Jhpiego developed a data analysis process using an affiche de monitorage or data monitoring poster, which includes indicators on case management, suspected cases tested, intermittent preventive treatment for pregnant women (IPTp) and use of long-lasting insecticide-treated net (LLINs).
In order to measure the long-term impact of malaria prevention and treatment interventions at the facility level through outcome indicators, Jhpiego developed a data analysis process using an affiche de monitorage or data monitoring poster, which includes indicators on case management, suspected cases tested, intermittent preventive treatment for pregnant women (IPTp) and use of long-lasting insecticide-treated net (LLINs).
Jhpiego and the National Malaria Control Program (NMCP) with support from the ExxonMobil Foundation identified inadequate and irregular data collection and data use as a systemic problem throughout Kribi district. In response, Jhpiego developed and implemented training sessions on the data posters that focused on:
- the context and rationale for this type of data visualization
- techniques for data collection, analysis, and interpretation for decision-making, and
- practical sessions enabling health providers to practice mapping data onto the posters
 In September 2015, Jhpiego introduced the posters in 26 health facilities in Kribi that were already trained in malaria prevention and case management interventions. Jhpiego then provided blank copies of the data posters and supported sites via biannual supervision visits during which they reviewed data posters for accuracy against facility registers.
In September 2015, Jhpiego introduced the posters in 26 health facilities in Kribi that were already trained in malaria prevention and case management interventions. Jhpiego then provided blank copies of the data posters and supported sites via biannual supervision visits during which they reviewed data posters for accuracy against facility registers.
Furthermore, supervisors assessed facility’s progress on their objectives, identified gaps and their causes, and discussed corrective actions. As a result of Jhpiego’s efforts by June 2017, 61% of the trained facilities use the data poster for decision-making. With the introduction of the posters, the percentage of health facilities that did not experience stock shortages increased by 17 percentage points, from 21% in October 2016 to 38% in March 2017.
Additionally, the Ministry of Health requested Jhpiego to lead a training of 181 health administrators and providers aimed at scaling-up the use of the data posters across all 9 districts of the South Region of Cameroon.
Health Workers &Human Resources &IPTp &Training &Treatment Bill Brieger | 07 Nov 2017
Using rapid task analysis to strengthen Pre-Service Education (PSE) learning and performance of critical malaria interventions in Liberia
 Understanding the tasks that health workers perform in real life can improve their basic Training. Marion Subah of MCSP and Jhpiego shares experiences in using Task Analysis to improve pre-service training of midwives and lab technicians in Liberia. Her findings summarized below, are presented at the American Society of Tropical Medicine’s 66th Annual Meeting.
Understanding the tasks that health workers perform in real life can improve their basic Training. Marion Subah of MCSP and Jhpiego shares experiences in using Task Analysis to improve pre-service training of midwives and lab technicians in Liberia. Her findings summarized below, are presented at the American Society of Tropical Medicine’s 66th Annual Meeting.
Health worker task analysis helps human resource planners and managers update pre-service education (PSE) curricula and plan needed in- service training. In Liberia, a task analysis was conducted focusing on Liberia’s midwives’ and Medical Laboratory Technicians’ (MLT) work practices.
service training. In Liberia, a task analysis was conducted focusing on Liberia’s midwives’ and Medical Laboratory Technicians’ (MLT) work practices.
Task lists were developed using curricula, job descriptions and professional scope of practice, and validated by key stakeholders for each cadre. Responses from 25 MLTs and 26 midwives were examined that addressed the following questions:
- How often do you do the task (frequency)?
- Where did you learn to do the task (location)?
- How well do you think you are able to perform the task (performance)?
- How critical is the task in terms of patient and/or public health outcomes (criticality).
 Eligibility criteria included those currently practicing between 6 months and 5.5 years following graduation. Midwives were assessed for five tasks relating to malaria service provision, including provision of preventive treatment for malaria in pregnancy, management of vector borne diseases, diagnosis and management uncomplicated malaria in adults and children (respectively), and provision of malaria preventive services.
Eligibility criteria included those currently practicing between 6 months and 5.5 years following graduation. Midwives were assessed for five tasks relating to malaria service provision, including provision of preventive treatment for malaria in pregnancy, management of vector borne diseases, diagnosis and management uncomplicated malaria in adults and children (respectively), and provision of malaria preventive services.
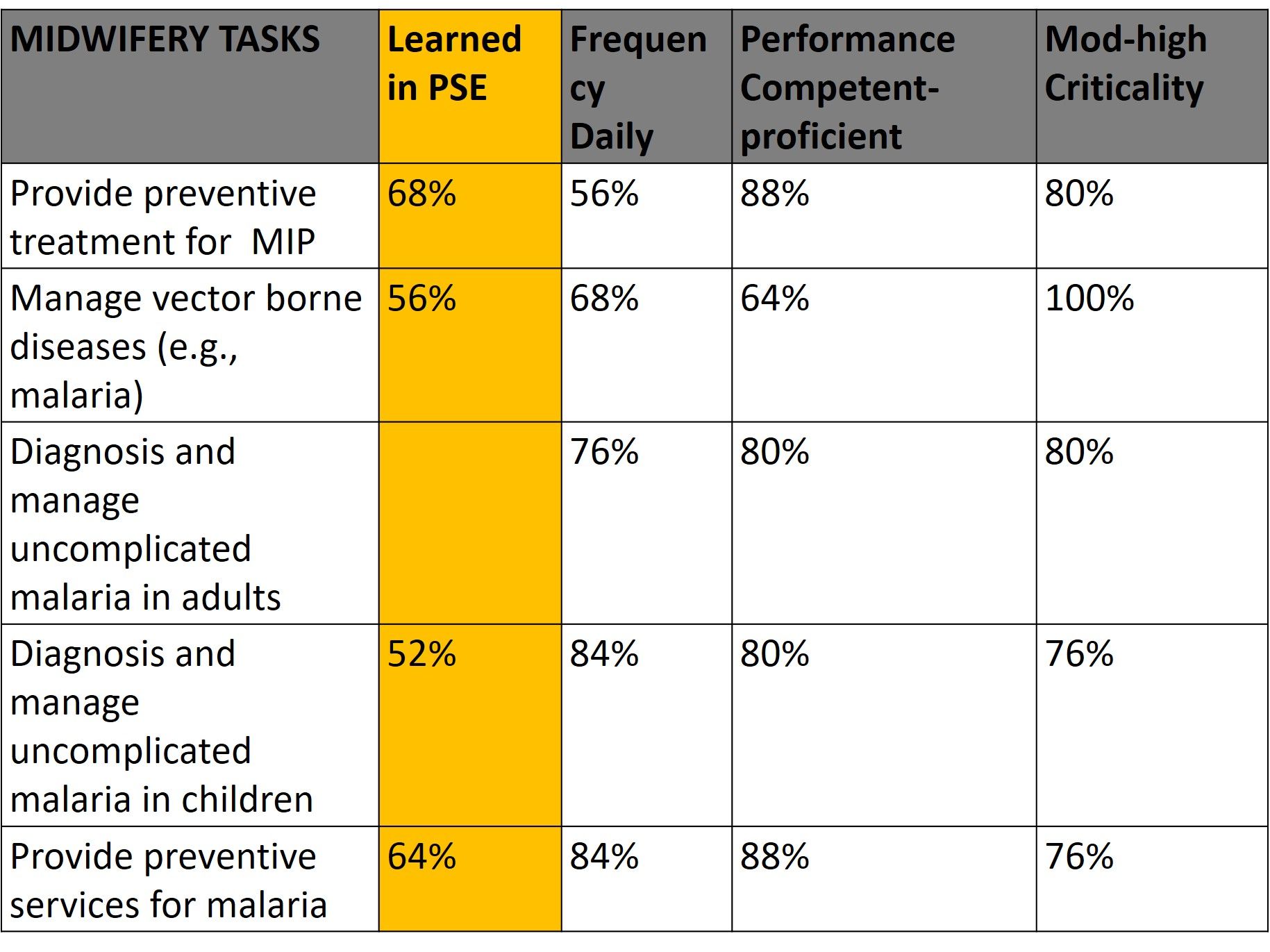 Lab technicians were assessed for one malaria task, performance of parasitological tests. On average 61% of midwives learned these malaria tasks in PSE, 74% said they performed these tasks daily, 80% felt proficient in performing the tasks, and 82% rated the tasks moderate to high in criticality. For MLTs, 88% learned malaria testing in pre-service education, 100 % performed this task daily, 77% felt they were proficient and 93% said the task was of moderate to high criticality.
Lab technicians were assessed for one malaria task, performance of parasitological tests. On average 61% of midwives learned these malaria tasks in PSE, 74% said they performed these tasks daily, 80% felt proficient in performing the tasks, and 82% rated the tasks moderate to high in criticality. For MLTs, 88% learned malaria testing in pre-service education, 100 % performed this task daily, 77% felt they were proficient and 93% said the task was of moderate to high criticality.
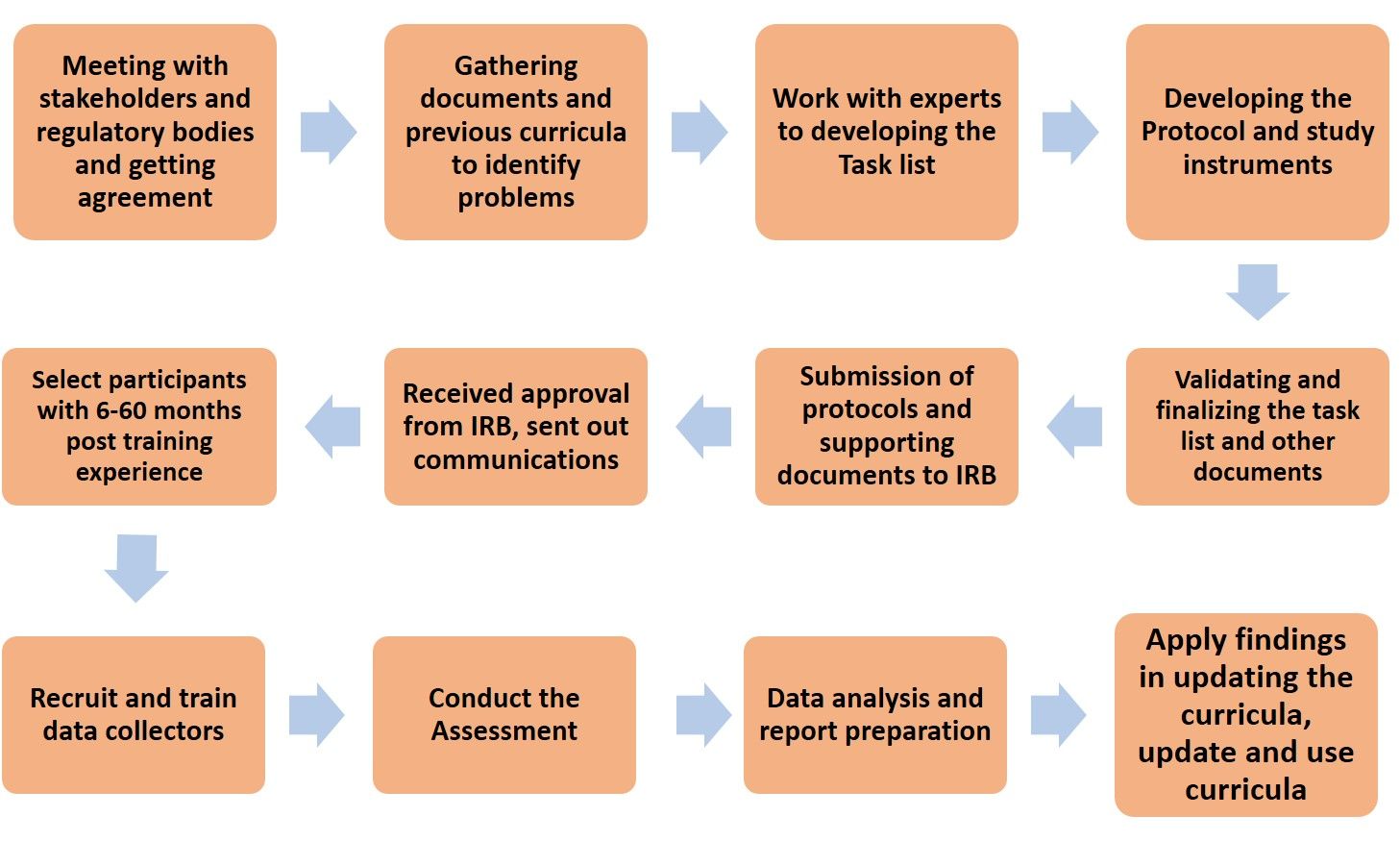
Task Analysis Flow Chart
The results from this rapid task analysis are being applied to the current curricula review. Courses that could be updated or strengthened have been identified. Malaria Case Management Technical Update and Effective Teaching Skills Training are being organized for tutors at the training schools. Finally, integrated supportive supervision tools are being strengthened to improve performance of these malaria tasks by midwives and lab technicians.
Case Management &IPTp &Quality of Services Bill Brieger | 06 Nov 2017
Implementation of a Quality Improvement Approach for Malaria Service Delivery in Zambezia Province, Mozambique
 Baltazar Candrinho, Armindo Tiago, Custodio Cruz, Mercino Ombe, Katherine Wolf, Maria da Luz Vaz, Connie Lee and Rosalia Mutemba are sharing their work during a scientific session on enhancing quality of care for malaria services in Mozambique at the 66th Annual Meeting of the American Society of Tropical Medicine 66th Annual Meeting on 6 November 2017. A summary of their talk follows:
Baltazar Candrinho, Armindo Tiago, Custodio Cruz, Mercino Ombe, Katherine Wolf, Maria da Luz Vaz, Connie Lee and Rosalia Mutemba are sharing their work during a scientific session on enhancing quality of care for malaria services in Mozambique at the 66th Annual Meeting of the American Society of Tropical Medicine 66th Annual Meeting on 6 November 2017. A summary of their talk follows:
 In Mozambique, malaria in pregnancy (MIP) is one of the leading causes of maternal and newborn morbidity and mortality. Malaria also accounts for over 40% of deaths in children less than five years old. With provincial and facility-level commitment, a simple and comprehensive quality improvement (QI) system has been established in 10 of 16 districts in Zambezia Province.
In Mozambique, malaria in pregnancy (MIP) is one of the leading causes of maternal and newborn morbidity and mortality. Malaria also accounts for over 40% of deaths in children less than five years old. With provincial and facility-level commitment, a simple and comprehensive quality improvement (QI) system has been established in 10 of 16 districts in Zambezia Province.
Since 2016, the Mozambique Ministry of Health (MOH) and Zambezia Provincial Health Directorate, in collaboration with partners, have implemented a malaria QI effort based on the Standards-Based Management and Recognition (SBM-R) approach. A standards-based approach to improving quality of malaria care engages both management and service providers to work together to assess the current performance, address gaps to ensure that all patients receive a minimum (standardized / evidence-based) package of care, and ultimately improve patient outcomes and facility performance.
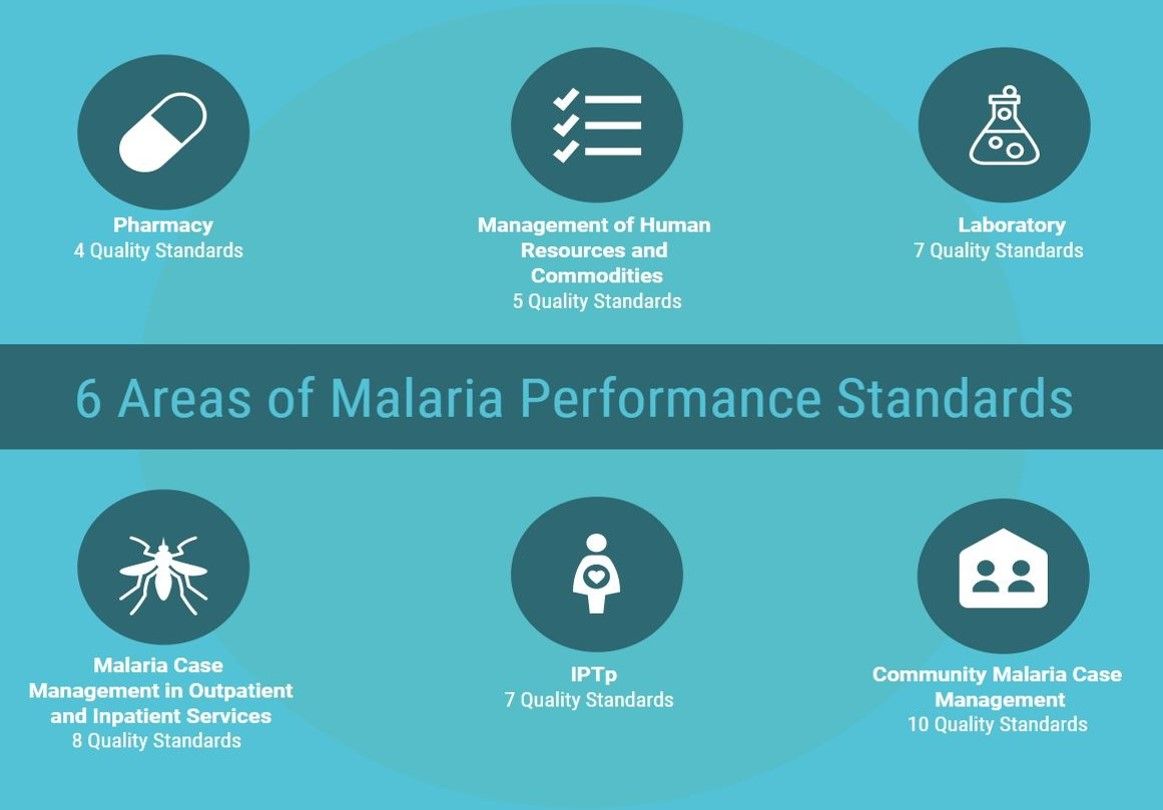 Thirty-one performance standards in five content areas (MIP, Case Management, Laboratory, Pharmacy, and Management of Human Resources and Malaria Commodities) were developed and adopted by the MOH in 2016. With support from partners, 40 health workers, including managers, clinicians and lab technicians, received training on SBM-R, and facility QI teams were established.
Thirty-one performance standards in five content areas (MIP, Case Management, Laboratory, Pharmacy, and Management of Human Resources and Malaria Commodities) were developed and adopted by the MOH in 2016. With support from partners, 40 health workers, including managers, clinicians and lab technicians, received training on SBM-R, and facility QI teams were established.
These teams use checklists based on standards to conduct quarterly assessments that identify performance gaps, and then develop action plans to address areas of improvement. The MOH antenatal care and child health registers also contain information o n coverage of key malaria interventions, including IPTp, and malaria diagnosis and treatment during pregnancy and for children under five with fever.
n coverage of key malaria interventions, including IPTp, and malaria diagnosis and treatment during pregnancy and for children under five with fever.
Average attainment of standards at baseline in 20 health facilities was 30%, and is expected to improve as implementation progresses with quarterly application of the checklist (data will be available before November). Improvements in key malaria indicators for pregnant women and children under five years old are expected as the percentage of standards attained increases.
Health Systems Bill Brieger | 06 Nov 2017
Malaria Programs Implementation in Ebonyi State, Nigeria: Where Are We?
 Jhpiego has developed a tool to help malaria programs understand implementation successes and challenges. Bright Orji, Daniel Umezurike, Lawrence Nwankwo, Boniface Onwe, Gladys Olisaekee, Enobong Ndekhedehe, and Emmanuel Otolorin outline the application of this tool for the malaria program in Ebonyi State, Nigeria at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene in the Poster Session of 6th November 2017. Their abstract follows:
Jhpiego has developed a tool to help malaria programs understand implementation successes and challenges. Bright Orji, Daniel Umezurike, Lawrence Nwankwo, Boniface Onwe, Gladys Olisaekee, Enobong Ndekhedehe, and Emmanuel Otolorin outline the application of this tool for the malaria program in Ebonyi State, Nigeria at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene in the Poster Session of 6th November 2017. Their abstract follows:
Despite important strides in recent years, Nigeria has yet to achieve global targets of universal coverage for malaria case management nor 80% coverage for malaria in pregnancy. While available malaria interventions are effective, critical health system challenges undermine implementation. Jhpiego has developed a health systems framework and planning tool to assist malaria control programs identify and respond to these challenges.
 The tool was recently used with the Ebonyi State Malaria Control Program (MCP) with Jhpiego’s guidance. An initial situational analysis used the 2015 Malaria Information Survey to highlight that 89% of state households had long lasting insecticide treated bed-nets but only 50% of children under five used them.
The tool was recently used with the Ebonyi State Malaria Control Program (MCP) with Jhpiego’s guidance. An initial situational analysis used the 2015 Malaria Information Survey to highlight that 89% of state households had long lasting insecticide treated bed-nets but only 50% of children under five used them.
Likewise, intermittent preventive treatment during pregnancy (IPTp) was only 44% for two IPTp doses and 41% for three. Use of parasitological diagnosis for malaria was low and unacceptable. A subsequent meeting among MCP and Jhpiego staff was held to review nine health systems areas to determine reasons for the low performance on malaria indicators. The group reviewed strategies and annual workplans and then ranked each health system area on a scale from 1 (low) to 4 (high) to reflect level of progress, and then the average score computed.
 The highest scoring components were human resource capacity (3) and integration and coordination (3), based on findings such as integrated supportive supervision and the holding of monthly coordination and review meetings among partners at the state and local level. Community Involvement (1.9) and finance (1.8) scored lowest, based on lack of community outreach and engagement, in control efforts, and late/ sporadic release of funds for program implementation, respectively.
The highest scoring components were human resource capacity (3) and integration and coordination (3), based on findings such as integrated supportive supervision and the holding of monthly coordination and review meetings among partners at the state and local level. Community Involvement (1.9) and finance (1.8) scored lowest, based on lack of community outreach and engagement, in control efforts, and late/ sporadic release of funds for program implementation, respectively.
In response, the group drew up action plans to address identified weaknesses and used monthly partners meetings for advocacy and learning. In conclusion Nigerian health workers can use health systems analysis and planning tools to identify best practices, address challenges, and create an action plan to help advance their state (and country) along the pathway to malaria elimination.
Diagnosis &Health Workers &Learning/Training Bill Brieger | 05 Nov 2017
Performance assessment of laboratory technicians on Malaria Microscopy in 5 high endemic districts of Rwanda
 Parasitological diagnosis plays an increasing role in malaria control and elimination. Noella Umulisa, Angelique Mugirente, Tharcisse Munyaneza, Aniceth Rucogoza, Aline Uwimana, Beata Mukarugwiro, Stephen Mutwiwa, Aimable and Mbituyumuremyi of the
Parasitological diagnosis plays an increasing role in malaria control and elimination. Noella Umulisa, Angelique Mugirente, Tharcisse Munyaneza, Aniceth Rucogoza, Aline Uwimana, Beata Mukarugwiro, Stephen Mutwiwa, Aimable and Mbituyumuremyi of the
Maternal and Child Survival Program, Jhpiego, the National Reference Laboratory, Rwanda Biomedical Centre (RBC), and the Malaria and Other Parasitic Diseases Division (Mal & OPDD) in Rwanda will present their experiences building the capacity of lab technicians during Session 47 at the American Society of Tropical Medicine and Hygiene Annual Meeting on 6 November 2017. Their abstract is found below.
Accurate malaria diagnostics help to establish the true prevalence of each Plasmodium species and can ensure appropriate treatment. Light microscopy is the gold standard for malaria diagnosis and sufficient training of laboratory staff is paramount for the correct microscopy diagnosis of malaria. In Rwanda each of about 400 health centers has a laboratory able to perform malaria microscopy, at least 2 trained lab technicians and 1 to 2 functioning microscopes.
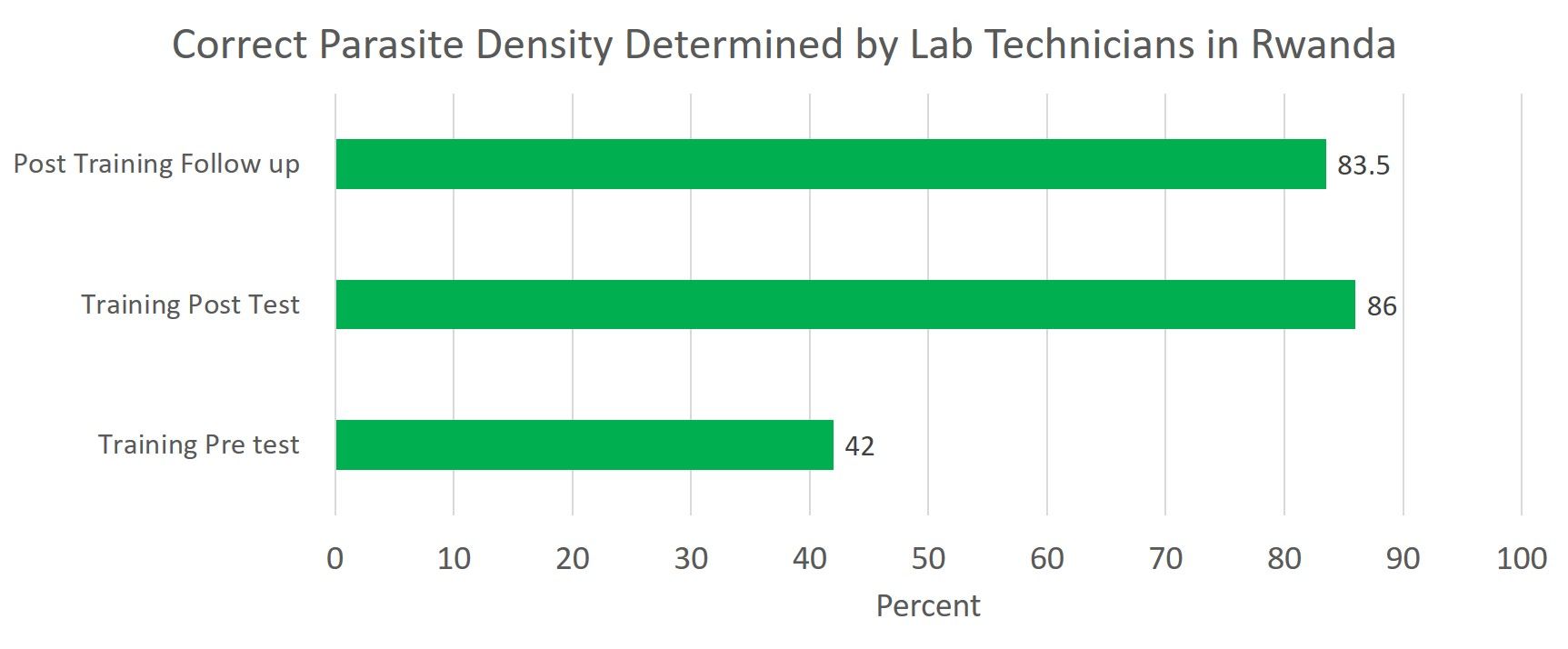
The objective of the study is to evaluate the performance of laboratory technicians in detecting and quantifying malaria parasites in 81 health centers from 5 highly endemic districts (Huye, Nyanza, Ngoma, Kirehe, Kayonza, Gatsibo). In October 2015 the Rwanda Biomedical Center and partners trained 1 lab technician per health center from these districts in malaria microscopy.
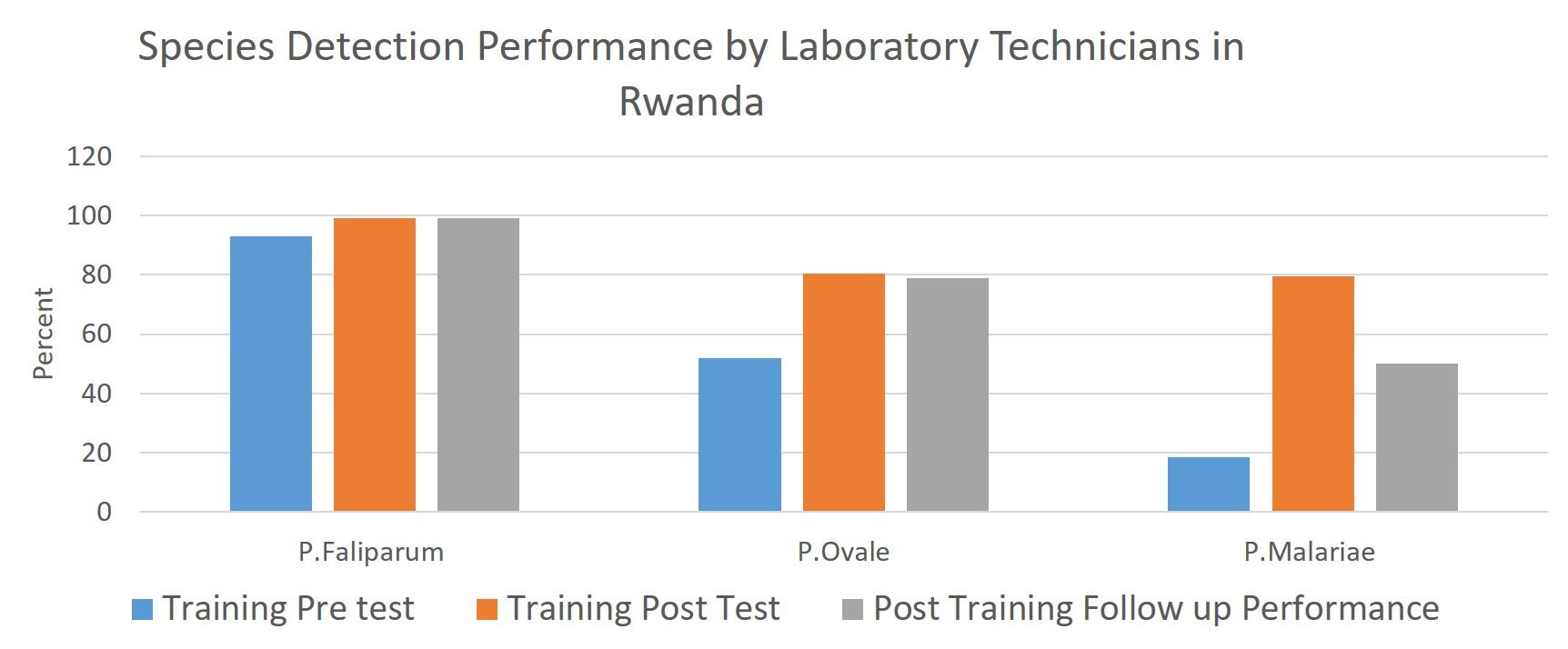 The training emphasized determining parasite density and detection of malaria species. From August to September 2016 a follow-up assessment was conducted. Of the 81 technicians trained, 30 were randomly chosen and assessed at their health facilities.
The training emphasized determining parasite density and detection of malaria species. From August to September 2016 a follow-up assessment was conducted. Of the 81 technicians trained, 30 were randomly chosen and assessed at their health facilities.
A standardized pre-validated slide panel of 5 slides was distributed, a comprehensive checklist used to collect information and conduct visual inspection and maneuvers used in routine malaria diagnosis. During the training a significant increase was found between pre and post tests with median scores improving from 47% to 85%.
 As part of the assessment 150 lab tech-prepared slides were analyzed to evaluate the quality of thick and thin blood smears. There was a significant increase in quality of both blood smear types. The sensitivity and specificity of participants in detection of malaria parasites were 100% and 86% respectively, while species identification and parasite quantification accuracy were 79% and 75% respectively.
As part of the assessment 150 lab tech-prepared slides were analyzed to evaluate the quality of thick and thin blood smears. There was a significant increase in quality of both blood smear types. The sensitivity and specificity of participants in detection of malaria parasites were 100% and 86% respectively, while species identification and parasite quantification accuracy were 79% and 75% respectively.
The findings of this assessment support the need for continuous capacity building for laboratory staff to ensure accurate malaria diagnosis for appropriate treatment and suggest that District hospitals may benefit from conducting regular malaria microscopy diagnosis quality control/assurance activities at health center laboratories.