Community Bill Brieger | 12 May 2014 10:48 am
Community case management – in the community or of the community?
In response to sharing of the following article: “Community case management of malaria: exploring support, capacity and motivation of community medicine distributors in Uganda” by Banek et al., a colleague responded that it, “confirms what is known from ever: communities do not sustain their CHWs. When the INGO (international NGO) withdraws, CHWs drop their tools, this is history.”
 The article itself, a qualitative assessment of community medicine distributors (CMDs) from a program of home/community based management (HBM) of malaria in Uganda that was started around 2002, did paint a bleak picture of volunteer motivation, support and supervision. Unfortunately the article focused either on the motivation of the individual CMDs or on the health system and its employees. We do not come away from reading this article with an understanding of the role of the community and why the CMDs felt disappointed at the level of community support they received.
The article itself, a qualitative assessment of community medicine distributors (CMDs) from a program of home/community based management (HBM) of malaria in Uganda that was started around 2002, did paint a bleak picture of volunteer motivation, support and supervision. Unfortunately the article focused either on the motivation of the individual CMDs or on the health system and its employees. We do not come away from reading this article with an understanding of the role of the community and why the CMDs felt disappointed at the level of community support they received.
In fact community volunteers do not always drop out or if they do, communities can actually replace them if the program is organized well. The African Program for Onchocerciasis Control (APOC) has maintained community distribution of ivermectin since 1997-98 in now over 120,000 villages. The key to the success of community directed distributors (CDDs) of ivermectin was the approach that focused on getting community commitment, not on individual volunteers.
In fact this approach, now know as community directed intervention (CDI) has been found appropriate to delivering a package of simple interventions, including community case management of malaria. What makes the difference in CDI is first the determination of what constitutes a community and secondly that the community itself manages the interventions, not individual volunteers, though CDDs who are selected by the community certainly play a major role.
 First, what is the ‘community?’ Experience with APOC has shown that one needs to consult with local people on the ground to determine what is a community. When program planners, for example, in eastern Nigeria thought lets encourage ‘the community’ to select a couple volunteers, they did not realize that an ‘autonomous community’ or town, while having its own chief and council, was actually made up of 4-6 ‘villages’ of from 1,000 to 5,000 people having their own leaders. If the community/town selected a couple volunteers two problems occurred – 1) the workload was high and CDDs became discouraged and 2) not all villages were represented so villages without CDDs felt neglected and did not participate well.
First, what is the ‘community?’ Experience with APOC has shown that one needs to consult with local people on the ground to determine what is a community. When program planners, for example, in eastern Nigeria thought lets encourage ‘the community’ to select a couple volunteers, they did not realize that an ‘autonomous community’ or town, while having its own chief and council, was actually made up of 4-6 ‘villages’ of from 1,000 to 5,000 people having their own leaders. If the community/town selected a couple volunteers two problems occurred – 1) the workload was high and CDDs became discouraged and 2) not all villages were represented so villages without CDDs felt neglected and did not participate well.
A closer look by sociologists involved in the program learned what was the smallest natural unit of commnuity. They saw that in fact even the villages were made up of kin groups of 100-200 people. Ultimately it was found that selection of CDDs by their kin group worked best. They could be held accountable by close relatives and friends and they would have a manageable volunteer workload.
The supplies needed did not vary much as the population estimates still accounted for the whole town. The design of the training was simplified enough and held in local schools or other public buildings so that costs were minimal. Peer support and meetings at the nearest health facility played an important and low cost function in supervision.
Similar lessons were learned in western Nigeria which had a different settlement pattern based on towns and satellite farm hamlets. As long as family compounds in town (kin groups) and outlying hamlets were directly involved in selecting and supervising their own volunteers, the services were delivered. Communities could chose as many volunteers as they needed, and when additional service components were added, communities could decide to increase the number of CDDs so that no one volunteer was burdened with the whole package.
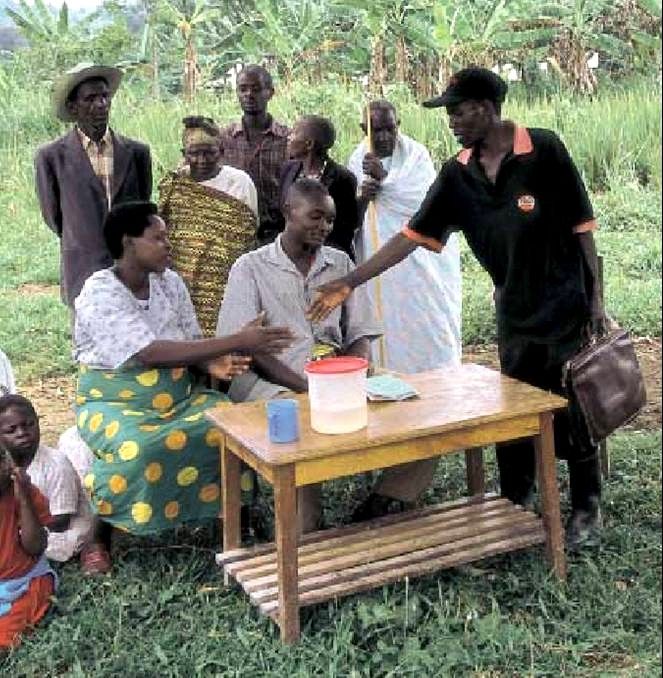
 A number of articles have arisen from the Uganda home based management of malaria project and work continues with the support of other NGOs and government agencies. What is of interest is the fact that over the history of the work, little has been said about the community. One WHO publication that discussed the early stages mentioned “Selection of distributors in Uganda took place during village council meetings,” but there was also reference to having “at least two distributors in each parish and more in larger communities.”
A number of articles have arisen from the Uganda home based management of malaria project and work continues with the support of other NGOs and government agencies. What is of interest is the fact that over the history of the work, little has been said about the community. One WHO publication that discussed the early stages mentioned “Selection of distributors in Uganda took place during village council meetings,” but there was also reference to having “at least two distributors in each parish and more in larger communities.”
The districts of Uganda are divided into counties which themselves are divided into sub-counties, and are further divided into parishes and villages. It appears that parishes may have several villages, so again it is not clear whether the Uganda HBM project was based on the smallest natural units of community or not.
Banek and colleagues conclude that, “social factors that impact on the implementation of community-based programmes, such as community perceptions and acceptability and community health worker motivation, remain understudied.” The reality is that people in the malaria world have not communicated well with people working on onchocerciasis and NTDs. Had they done so, they would realize that there has been much study on how to set up sustainable volunteer programs in thousands and thousands of villages that put the community in charge. It is not enough to work in the community, the community must be in charge