Asymptomatic &Burden &Dengue &Diagnosis &Ebola &Elimination &Epidemiology &Health Systems &ITNs &MDA &Mosquitoes &NTDs &Schistosomiasis &Schools &Vector Control &Zoonoses Bill Brieger | 30 Jun 2019
The Weekly Tropical Health News 2019-06-29
Below we highlight some of the news we have shared on our Facebook Tropical Health Group page during the past week.
Polio Persists
If all it took to eradicate a disease was a well proven drug, vaccine or technology, we would not be still reporting on polio, measles and guinea worm, to name a few. In the past week Afghanistan reported 2 wild poliovirus type 1 (WPV1) cases, and Pakistan had 3 WPV1 cases. Circulating vaccine-derived poliovirus type 2 (cVDPV2) was reported in Nigeria (1), DRC (4) and Ethiopia (3) from healthy community contacts.
Continued Ebola Challenges
In the seven days from Saturday to Friday (June 28) there were 71 newly confirmed Ebola Cases and 56 deaths reported by the Democratic Republic of Congo’s Ministry of Health. As Ebola cases continue to pile up in the Democratic Republic of the Congo (DRC), with 12 more confirmed Thursday and 7 more Friday, a USAID official said four major donors have jump-started a new strategic plan for coordinating response efforts. To underscore the heavy toll the outbreak has caused, among its 2,284 cases, as noted on the World Health Organization Ebola dashboard today, are 125 infected healthcare workers, including 2 new ones, DRC officials said.
Pacific Standard explained the differences in Ebola outbreaks between DRC today and the West Africa outbreak of 2014-16. On the positive side are new drugs used in organized trials for the current outbreak. The most important factor is safe, effective vaccine that has been tested in 2014-16, but is now a standard intervention in the DRC. While both Liberia and Sierra Leone had health systems and political weaknesses as post-conflict countries, DRC’s North Kivu and Ituri provinces are currently a war zone, effectively so for the past generation. Ebola treatment centers and response teams are being attacked. There are even cultural complications, a refusal to believe that Ebola exists. So even with widespread availability of improved technologies, teams may not be able to reach those in need.
To further complicate matters in the DRC, Doctors Without Borders (MSF) “highlighted ‘unprecedented’ multiple crises in the outbreak region in northeastern DRC. Ebola is coursing through a region that is also seeing the forced migration of thousands of people fleeing regional violence and is dealing with another epidemic. Moussa Ousman, MSF head of mission in the DRC, said, ‘This time we are seeing not only mass displacement due to violence but also a rapidly spreading measles outbreak and an Ebola epidemic that shows no signs of slowing down, all at the same time.’”
NIPAH and Bats
Like Ebola, NIPAH is zoonotic, and also involves bats, but the viruses differ. CDC explains that, “Nipah virus (NiV) is a member of the family Paramyxoviridae, genus Henipavirus. NiV was initially isolated and identified in 1999 during an outbreak of encephalitis and respiratory illness among pig farmers and people with close contact with pigs in Malaysia and Singapore. Its name originated from Sungai Nipah, a village in the Malaysian Peninsula where pig farmers became ill with encephalitis.
A recent human outbreak in southern India has been followed up with a study of local bats. In a report shared by ProMED, out of 36 Pteropus species bats tested for Nipah, 12 (33%) were found to be positive for anti-Nipah bat IgG antibodies. Unlike Ebola there are currently no experimental drugs or vaccines.
Climate Change and Dengue
Climate change is expected to heighten the threat of many neglected tropical diseases, especially arboviral infections. For example, the New York Times reports that increases in the geographical spread of dengue fever. Annually “there are 100 million cases of dengue infections severe enough to cause symptoms, which may include fever, debilitating joint pain and internal bleeding,” and an estimated 10,000 deaths. Dengue is transmitted by Aedes mosquitoes that also spread Zika and chikungunya. A study, published Monday in the journal Nature Microbiology, found that in a warming world there is a strong likelihood for significant expansion of dengue in the southeastern United States, coastal areas of China and Japan, as well as to inland regions of Australia. “Globally, the study estimated that more than two billion additional people could be at risk for dengue in 2080 compared with 2015 under a warming scenario.”
Schistosomiasis – MDA Is Not Enough, and Neither Are Supplementary Interventions
Schistosomiasis is one of the five neglected tropical diseases (NTDs) that are being controlled and potentially eliminated through mass drug administration (MDA) of preventive chemotherapy (PCT), in this case praziquantel. In The Lancet Knopp et al. reported that biannual MDA substantially reduced Schistosomiasis haematobium prevalence and infection intensity but was insufficient to interrupt transmission in Zanzibar. In addition, neither supplementary snail control or behaviour change activities did not significantly boost the effect of MDA. Most MDA programs focus on school aged children, and so other groups in the community who have regular water contact would not be reached. Water and sanitation activities also have limitations. This raises the question about whether control is acceptable for public health, or if there needs to be a broader intervention to reach elimination?
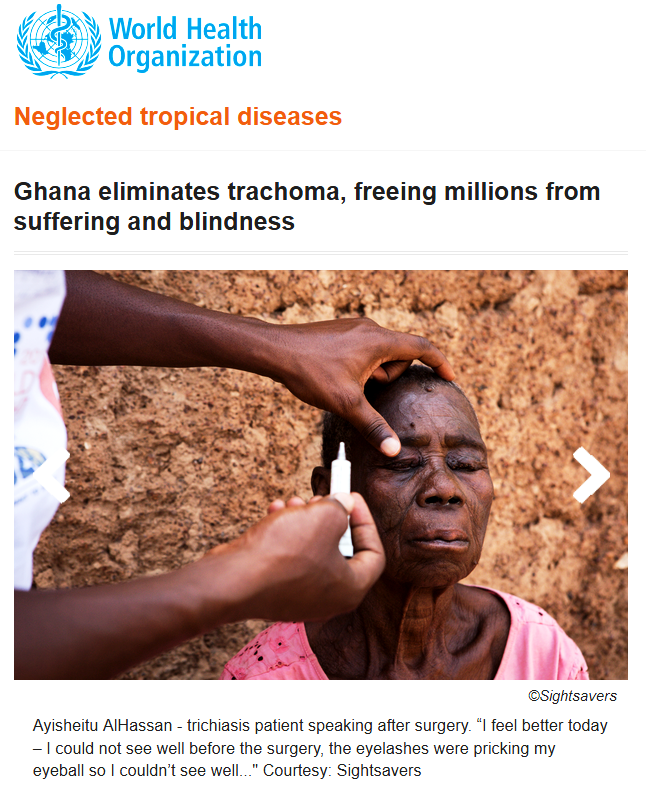
Trachoma on the Way to Elimination
Speaking of elimination, WHO has announced major “sustained progress” on trachoma efforts. “The number of people at risk of trachoma – the world’s leading infectious cause of blindness – has fallen from 1.5 billion in 2002 to just over 142 million in 2019, a reduction of 91%.” Trachoma is another NTD that uses the MDA strategy.
The news about NTDs from Dengue to Schistosomiasis to Trachoma is complicated and demonstrates that putting diseases together in a category does not result in an easy choice of strategies. Do we control or eliminate or simply manage illness? Can our health systems handle the needs for disease elimination? Is the public ready to get on board?
Malaria Updates
And concerning being complicated, malaria this week again shows many facets of challenges ranging from how to recognize and deal with asymptomatic infection to preventing reintroduction of the disease once elimination has been achieved. Several reports this week showed the particular needs for malaria intervention ranging from high burden areas to low transmission verging on elimination to preventing re-introduction in areas declared free from the disease.
In South West, Nigeria Dokunmu et al. studied 535 individuals aged from 6 months were screened during the epidemiological survey evaluating asymptomatic transmission. Parasite prevalence was determined by histidine-rich protein II rapid detection kit (RDT) in healthy individuals. They found that, “malaria parasites were detected by RDT in 204 (38.1%) individuals. Asymptomatic infection was detected in 117 (57.3%) and symptomatic malaria confirmed in 87 individuals (42.6%).
Overall, detectable malaria by RDT was significantly higher in individuals with symptoms (87 of 197/44.2%), than asymptomatic persons (117 of 338/34.6%)., p = 0.02. In a sub-set of 75 isolates, 18(24%) and 14 (18.6%) individuals had Pfmdr1 86Y and 1246Y mutations. Presence of mutations on Pfmdr1 did not differ by group. It would be useful for future study to look at the effect of interventions such as bednet coverage. While Southwest Nigeria is a high burden area, the problem of asymptomatic malaria will become an even bigger challenge as prevalence reduces and elimination is in sight.
Sri Lanka provides a completely different challenge from high burden areas. There has been no local transmission of malaria in Sri Lanka for 6 years following elimination of the disease in 2012. Karunasena et al. report the first case of introduced vivax malaria in the country by diagnosing malaria based on microscopy and rapid diagnostic tests. “The imported vivax malaria case was detected in a foreign migrant followed by a Plasmodium vivax infection in a Sri Lankan national who visited the residence of the former. The link between the two cases was established by tracing the occurrence of events and by demonstrating genetic identity between the parasite isolates. Effective surveillance was conducted, and a prompt response was mounted by the Anti Malaria Campaign. No further transmission occurred as a result.”
Bangladesh has few but focused areas of malaria transmission and hopes to achieve elimination of local transmission by 2030. A particular group for targeting interventions is the population of slash and burn cultivators in the Rangamati District. Respondents in this area had general knowledge about malaria transmission and modes of prevention and treatment was good according to Saha and the other authors. “However, there were some gaps regarding knowledge about specific aspects of malaria transmission and in particular about the increased risk associated with their occupation. Despite a much-reduced incidence of malaria in the study area, the respondents perceived the disease as life-threatening and knew that it needs rapid attention from a health worker. Moreover, the specific services offered by the local community health workers for malaria diagnosis and treatment were highly appreciated. Finally, the use of insecticide-treated mosquito nets (ITN) was considered as important and this intervention was uniformly stated as the main malaria prevention method.”
Kenya offers some lessons about low transmission areas but also areas where transmission may increase due to climate change. A matched case–control study undertaken in the Western Kenya highlands. Essendi et al. recruited clinical malaria cases from health facilities and matched to asymptomatic individuals from the community who served as controls in order to identify epidemiological risk factors for clinical malaria infection in the highlands of Western Kenya.
“A greater percentage of people in the control group without malaria (64.6%) used insecticide-treated bed nets (ITNs) compared to the families of malaria cases (48.3%). Low income was the most important factor associated with higher malaria infections (adj. OR 4.70). Houses with open eaves was an important malaria risk factor (adj OR 1.72).” Other socio-demographic factors were examined. The authors stress the need to use local malaria epidemiology to more effectively targeted use of malaria control measures.
The key lesson arising from the forgoing studies and news is that disease control needs strong global partnerships but also local community investment and adaptation of strategies to community characteristics and culture.
Integration &NTDs Bill Brieger | 18 Jun 2018
Milestones in Eliminating NTDs
WHO lists the milestones towards validation of elimination beginning with stopping the spread of infection through mass drug administration (MDA), implementing MDA in all endemic areas (100% geographical coverage), reducing infection below a threshold at which transmission is not sustainable in all endemic areas and stop MDA, and finally demonstrating sustained reduction of infection below the threshold no earlier than 4 years after stopping MDA. WHO also encourages countries to alleviate suffering by managing morbidity such as lymphedema and preventing disability.
beginning with stopping the spread of infection through mass drug administration (MDA), implementing MDA in all endemic areas (100% geographical coverage), reducing infection below a threshold at which transmission is not sustainable in all endemic areas and stop MDA, and finally demonstrating sustained reduction of infection below the threshold no earlier than 4 years after stopping MDA. WHO also encourages countries to alleviate suffering by managing morbidity such as lymphedema and preventing disability.
By 2015 the partners providing PCT achieved a milestone. As WHO reports, “Preventive chemotherapy is achievable, as proven by the increasing numbers of people being reached each year. In 2015, over 1.5 billion treatments were administered to almost 1 billion individuals for at least one of the targeted infections: lymphatic filariasis, onchocerciasis, schistosomiasis soil-transmitted helminthiases and trachoma.

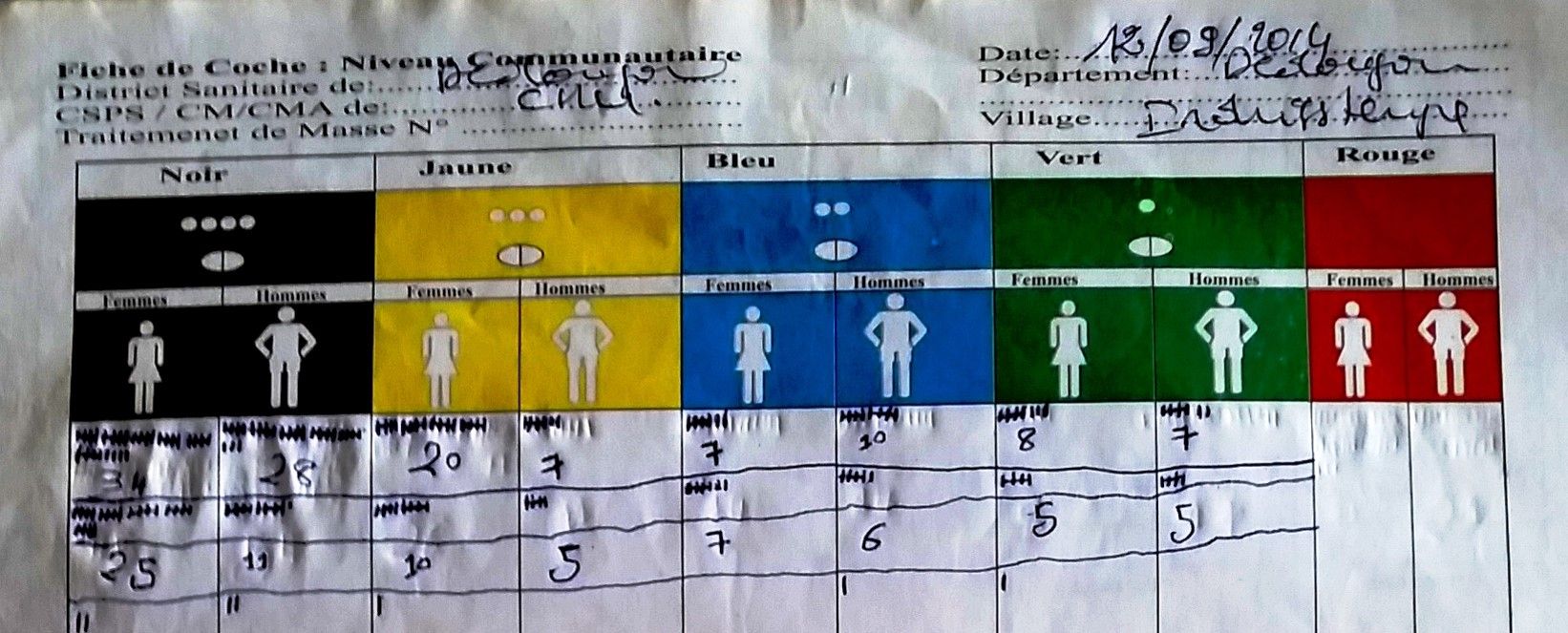
village records of MDA activities
At a low cost – between US$ 0.30 and US$ 0.50 per person treated in most settings – preventive chemotherapy remains the most affordable, cost-effective strategy for controlling and eliminating these diseases.” WHO also explains that to be fully sustainable and to maximize impact, PCT the strategy should be combined and delivered with other interventions, including improving access to safe drinking-water, hygiene, disease management and vector control.
USAID as one of the major NTD partners has spent nearly $700 million since 2006 to build the capacity of 33 endemic countries to plan and implement the MDA strategy for the five PCT diseases. By 2016, “USAID-assisted NTD programs had provided a total of more than 2 billion treatments in the respective countries, representing 935 million persons treated.” Over these years the number of persons living in implementation units (e.g. districts) that no longer require MDA has steadily increased.
 Of the 25 countries USAID has supported for LF MDA, “Three had already stopped MDA treatment in 2015 (Togo, Cambodia, and Vietnam), Four were expected to stop MDA in 2017, and 10 more countries by 2020. There were eight countries where the date for stopping treatment was anticipated beyond 2020.” Likewise, “Most countries are on track to reach WHO 2020 elimination goals for trachoma,” and nearly all countries shown anticipate reaching post-MDA surveillance by 2021.
Of the 25 countries USAID has supported for LF MDA, “Three had already stopped MDA treatment in 2015 (Togo, Cambodia, and Vietnam), Four were expected to stop MDA in 2017, and 10 more countries by 2020. There were eight countries where the date for stopping treatment was anticipated beyond 2020.” Likewise, “Most countries are on track to reach WHO 2020 elimination goals for trachoma,” and nearly all countries shown anticipate reaching post-MDA surveillance by 2021.
In conclusion, Robollo and Bockarie remind us that, “Interventions against neglected tropical diseases (NTD), including lymphatic filariasis (LF), (were) scaled up dramatically after the signing of the London Declaration (LD) in 2012… but some countries are considered not on track to meet the 2020 target using the recommended preventive chemotherapy and morbidity management strategies.” They believe that LF can be eliminated by 2020 “using cross-sectoral and integrated approaches” that incorporate the synergistic effect of the Sustainable Development Goals related to poverty reduction and water and sanitation.
Elimination &Ivermectin &MDA &NTDs &Procurement Supply Management Bill Brieger | 16 Jun 2018
Many Neglected Tropical Diseases: What About Eliminating Them?

Testing to see if transmission of lymphatic filariasis has stopped in Burkina Faso
Two things we need to note about the list of 20 diseases that the World Health Organization and partners classify as Neglected Tropical Diseases (NTDs). First, diseases like Rabies, Snakebite/envenoming, and Leprosy, while certainly more common in the tropics now, have in the past been global in distribution. Secondly some of the diseases have not been neglected. Onchocerciasis or river blindness has been the focus of a global partnership since 1975, and transmission in the America’s and much of the Sahel in Africa has been halted. Elimination of Dracunculiasis or Guinea Worm has also been the subject of many World Health Assembly Resolutions, and concerted effort has brought the number of cases down from 3.5 million in 1986 to 30 in 2017. What is more to the point about these diseases is that they affect neglected people, the poor and vulnerable in remote rural areas or urban slums.
Still when we can compare NTD control programs with the rise of major disease control efforts like the Global Fund to fight AIDS, Tuberculosis and Malaria, the President’s Emergency Program For AIDS Relief, the President’s Malaria Initiative, World Bank Malaria Booster Program, Global A Vaccine Initiative among others, we can see that the global community has been able to focus major financial resources on a few diseases. Now with the Sustainable Development Goals, that focus expanded from infectious to Non-Communicable Diseases. It is natural therefore to fear that tropical health problems that are responsible for major loss of life and economic capacity will not be adequately addressed.

A system of rewards helped identify the last cases in many guinea worm endemic countries
Based on the World Health Organization’s 2020 Roadmap on NTDs, the London Declaration on NTDs recognized a “tremendous opportunity to control or eliminate at least 10 of these devastating diseases by the end of the decade” (i.e. by 2020). These include eradication of Guinea worm disease, and elimination by 2020 of lymphatic filariasis (LF), leprosy, sleeping sickness {human African trypanosomiasis) and blinding trachoma. In addition drug access programmes should help control by 2020 schistosomiasis, soil-transmitted helminthes (STH), Chagas disease, visceral leishmaniasis and river blindness (onchocerciasis).
Five of the diseases are notable in that they can either be controlled or eliminated through Mass Drug Administration (MDA) using Preventive Chemo-Therapy (PCT). This effort is aided by drug donation programs at the global level and community based MDA at the local level. Ten companies were signatories to the London Declaration and contributed to drug donation programs to achieve MDA. According to WHO,
Preventive chemotherapy is aimed at optimizing the largescale use of safe, single-dose medicines and offers the best means of reducing the extensive morbidity associated with four helminthiases (lymphatic filariasis, onchocerciasis, schistosomiasis and soil-transmitted helminthiases) (6). Additionally, the large-scale administration of azithromycin – a key component of the SAFE strategy for trachoma (that is, lid surgery (S), antibiotics to treat the community pool of infection (A), facial cleanliness (C) and environmental improvement (E)) – is amenable to close coordination and, in future, possibly co-administration with interventions targeted at helminthiases.

Community health workers are the cornerstone of many NTD elimination programs
Targets for the 5 PCT diseases vary. The aim is to eliminate LF and Trachoma by 2020. Although the efforts against onchocerciasis have been running the longest, the refocus from control to elimination meant increasing the geographical scope of intervention, and now elimination may not be feasible until 2025. With a focus mainly on the school aged and based populations, programs against schistosomiasis and STH talk of control, not elimination, although some endemic countries hope that elimination may be possible if the focus of these programs expands. So far, Togo is the only Sub-Saharan African country to have eliminated LF, and Ghana to have eliminated Trachoma.
Partnerships, funding and drug donations need to be strengthened if more countries are to join the ranks of Togo and Nepal.
NTDs &Snakebite Bill Brieger | 17 Mar 2018
Modern Day St Patrick Needed to Drive out Snakes and NTDs

https://www.catholic.org/saints/saint.php?saint_id=89
While St. Patrick, the Christian missionary supposedly rid Ireland of snakes during the fifth century A.D., “Nigel Monaghan, who has trawled through vast collections of fossil and other records of Irish animals, has found no evidence of snakes ever existing in Ireland.” The rest of the world, of course, does not rest as easily, and therefore, “On June 9th, 2017 WHO categorized snakebite envenomation into the Category A of the Neglected Tropical Diseases.”
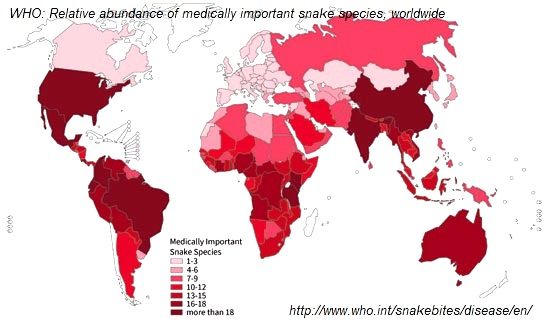
The World Health Organization explains that, “Snakebite envenoming is a potentially life-threatening disease that typically results from the injection of a mixture of different toxins (“venom”) following the bite of a venomous snake. Envenoming can also be caused by having venom sprayed into the eyes by certain species of snakes that have the ability to spit venom as a defense measure.” The organization notes that our of over 3,000 snake species globally, 250 are medically important because of their harmful venom. These can be found in 160 countries.
In preparation for the World Health Assembly, “the 142nd session of the World Health Organization’s Executive Board has recommended a resolution on snakebite envenoming to the 71st World Health Assembly, setting the scene for its possible adoption in May 2018.” The resolution calls on all countries to take definitive steps to stop the death, disability and suffering that snakebite inflicts on many of the poorest and most vulnerable of the world’s people.
A recent WHO report notes that, “As for other neglected tropical diseases, estimation of global morbidity, disability and mortality due to snakebite envenoming is problematic.” Rough estimates of the burden of snakebite include –
- 8 million to 2.7 million cases of snakebite envenoming per year
- 81 000 to 138 000 deaths per year
- 400,000 people a year face permanent disabilities, including blindness, extensive scarring and contractures, restricted mobility and amputation following snakebite envenoming
Mapping is a first important step for countries attempting to tackle this neglected disease. Sri Lanka was able develop snakebite risk maps to identify snakebite hotspots and cold spots in the country. A national survey in India found that, “Snakebite deaths occurred mostly in rural areas (97%), were more common in males (59%) than females (41%), and peaked at ages 15–29 years (25%) and during the monsoon months of June to September.” Costa Rica is using geographical information systems to identify populations in need of improved accessibility to anti-venom treatment for snakebite envenoming.
As Jose Mar?a Gutierrez and colleagues stress, “the need for incorporation of the proposed snakebite initiatives within the general struggle against all the NTDs will result in a significant and more logistically efficient reduction of human suffering.” This can be accomplished by having snakebite become part of the existing unified strategy for several NTDs that, “simplifies drug distribution, reduces duplication, and lessens some of the demands on health systems and staff.”
Thus with a unified approach we can hope to drive out snakes, worms, and other parasites from the homes, communities and countries of those suffering from the neglected diseases of poverty.
Advocacy &Borders &Children &Conflict &Costs &Epidemiology &Funding &Human Resources &Leadership &Monitoring &Mortality &NTDs &Partnership &Surveillance Bill Brieger | 03 Feb 2018
African Leaders Malaria Alliance Recognizes Country Achievements, Adds NTDs to its Scorecard
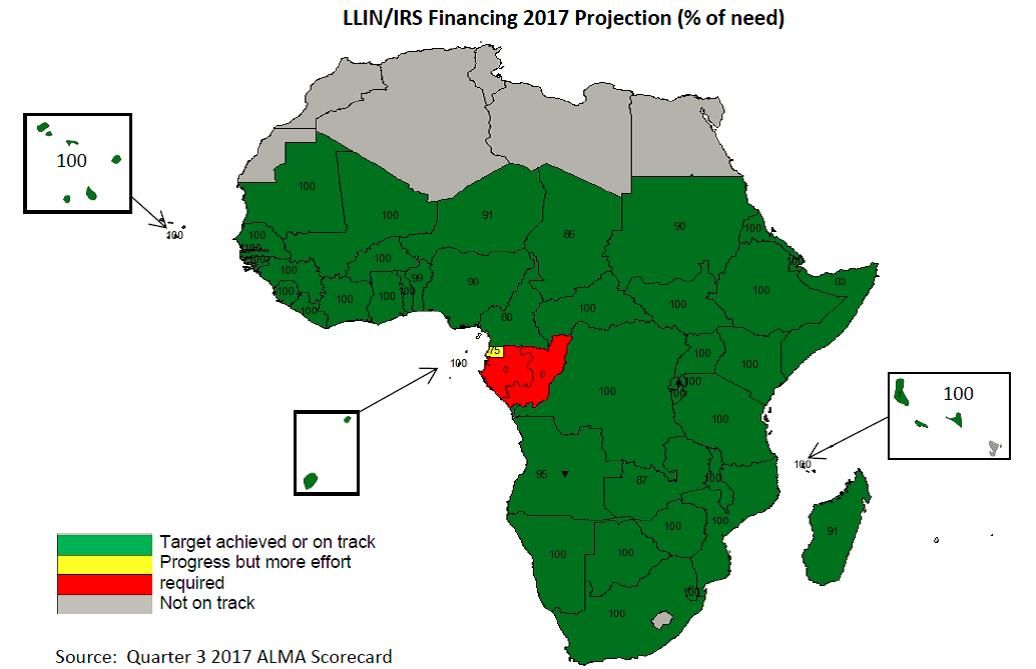
 The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
 For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
The scorecard will now “report progress for the 47 NTD-affected countries in sub-Saharan Africa in their strategies to treat and prevent the five most common NTDs: lymphatic filariasis, onchocerciasis, schistosomiasis, soil-transmitted helminths and trachoma. By adding NTDs to the scorecard, African leaders are making a public commitment to hold themselves accountable for progress on these diseases.”
 In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
The combination is based on the logic that NTDs and malaria are both diseases of poverty. Malaria and several NTDs are also vector-borne. Also community platforms are a foundation for delivering needed drugs and supplies to tackle these diseases. Ultimately the decision shows that Heads of State are holding themselves accountable for progress in eliminating these diseases.
 At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
 The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
H.E . Dr. Barnabas Sibusiso Dlamini, the Prime Minister of the Kingdom of Swaziland, whose King and Head of State is the current chair of ALMA, warned all endemic countries that, “When we take our eyes off malaria, the cost for our countries is huge. Yet if we increase our efforts to control and eventually eliminate malaria, the yield we get from it is tremendous. It is time that we dig deep into our pockets and provide malaria programmes with the needed resources.”
 Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
IRIN concludes that, “For now, the biggest challenge for Zambia will be closing the gap in its malaria elimination strategy, which will cost around $160 million a year and is currently only about 50 percent funded – two thirds from international donors and one third from the Zambian government. Privately, international donors say the government must spend more money on its malaria programme if it is to succeed.” Cross-border transmission adds to the problem.
Internal strife is another challenge to malaria success. “The recent nurses’ strike which lasted for five months may have cost Kenya a continental award in reducing the prevalence of malaria during the 30th African Union Summit in Ethiopia on Sunday.” John Muchangi in the Star also noted that, “However, Kenya lost momentum last year and a major malaria outbreak during the prolonged nurses’ strike killed more than 30 people within two weeks in October.”
 Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Fortunately ALMA is equipped with the monitoring and advocacy tools to ensure that its members recognize and respond to such challenges. The Scorecards will keep the fight against the infectious diseases of poverty on track.
Elimination &Eradication &NTDs Bill Brieger | 26 Jan 2018
The Long and Winding Worm, 1986-2018
Recent reports draw attention that Guinea Worm persisted in small numbers in 2017 in two countries, Chad and Ethiopia. Mali and South Sudan were the only other two countries monitored because of recent cases, but each reported none for 2017.
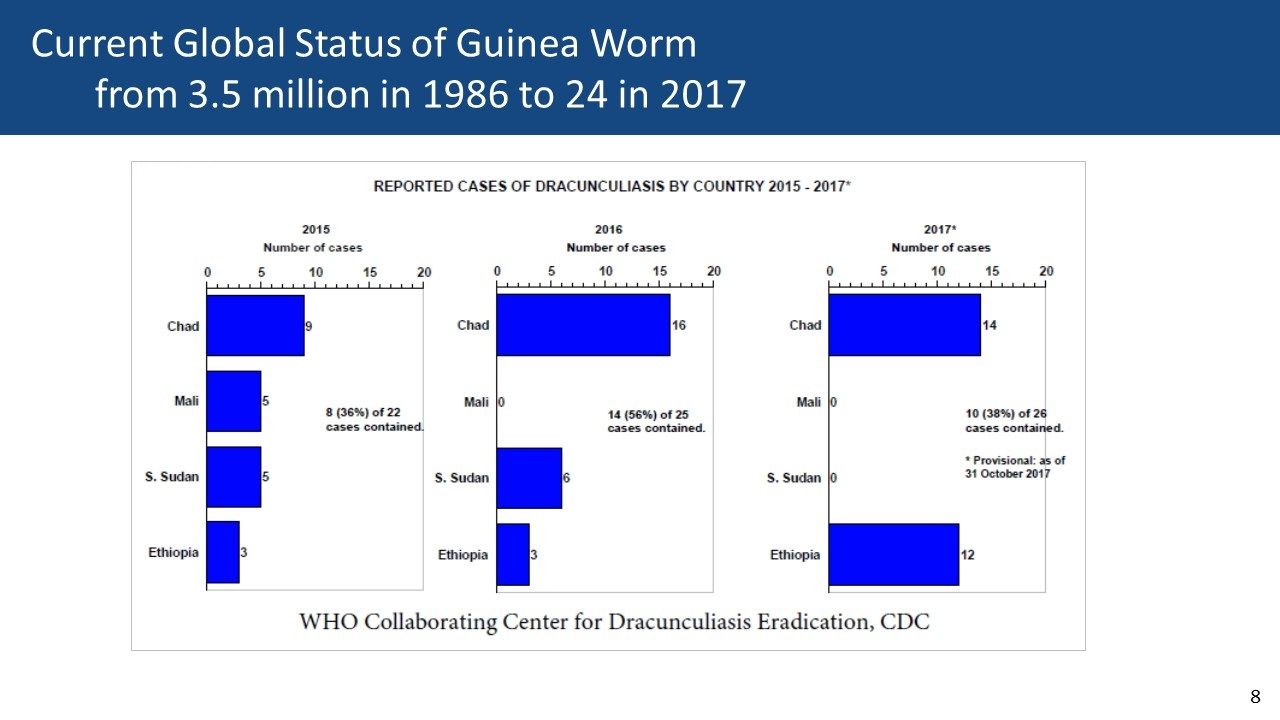
Guinea Worm Wrap-Up #251
We recall that 32 and 23 years have passed since the challenge to eradicate the disease was posed and the hoped for date of eradication was to be achieved. There is no doubt that the 30 cases reported in 2017 is a gigantic drop from the 3.5 million estimated globally when the war on the worm started in 1986.
To date eradication has been achieved for only small pox (though its reemergence from labs as a potential biological war agent is feared). Could it return as global warming melts permafrost (and bodies) in the permafrost of northern latitudes?
Besides Guinea Worm, only polio and malaria have received calls for eradication (malaria for the second time in history). One wonders if even small pox could be eradicated in today’s world of conflicted and failed states – the last case of smallpox was in Somalia. Both Ethiopia and Chad border South Sudan’s civil conflicts.
What had made guinea worm, like smallpox, imminently eradicable was the fact that humans were the main reservoirs of infection (not counting the defenseless crustacean, the cyclops, that served as an intermediate host for work larvae). That has not changed. WHO observed that in Ethiopia both baboons and dogs have been infected with guinea worm in the same communities where humans suffer from the disease. While it was possible to ‘contain’ the infection in dogs, that is preventing them from contaminating water supplies, it was not surprisingly difficult to do the same for baboons. The dog problem has existed in Chad for at least 5 years.
 Another problem in Ethiopia was the infection of seasonal laborers who could potentially take the disease back to other areas of the country. Although a system of rewards had been put in place this did not lead to the timely identification of all cases by either community members or health workers.
Another problem in Ethiopia was the infection of seasonal laborers who could potentially take the disease back to other areas of the country. Although a system of rewards had been put in place this did not lead to the timely identification of all cases by either community members or health workers.
The road to disease eradication is clearly not a straight line from A to B. The twists and turns should be expected as time passes because ideally an eradication should be a short-term effort that is time-limited in order to provide a clear focus and adequate funding on the end goal.
What are the implications for malaria and polio? Conflict led to the hiding of polio cases in Nigeria and longer term efforts allowed vaccine derived poliovirus to emerge. Malaria is now found in Monkeys in Malaysia and Brazil, and parasite resistance to medicines and vector resistance to pesticides threatens effective interventions.
Time is not a commodity that favors eradication. In these days of plateauing financial support for global health, the call for eradicating deadly and economically debilitating infections needs to be louder.
NTDs Bill Brieger | 05 Nov 2017
Online Survey to Elicit Views of Technical Support from Endemic Country Neglected Tropical Disease Managers
 An online survey was part of the process of an evaluation of USAID’s NTD program conducted by the Johns Hopkins Bloomberg School of Public Health. William R. Brieger, Adebamike Oshunbade, Gilbert Burnham, Violetta Yevstigneyeva, Emily Wainwright, and Darin Evans present the process and brief findings from the online survey Monday (20171106) during Poster Session A of the American Society of Tropical Medicine and Hygiene 66th Annual Conference in Baltimore. If you are there, look for Late Breaker Poster #5111. The poster abstract is provided below.
An online survey was part of the process of an evaluation of USAID’s NTD program conducted by the Johns Hopkins Bloomberg School of Public Health. William R. Brieger, Adebamike Oshunbade, Gilbert Burnham, Violetta Yevstigneyeva, Emily Wainwright, and Darin Evans present the process and brief findings from the online survey Monday (20171106) during Poster Session A of the American Society of Tropical Medicine and Hygiene 66th Annual Conference in Baltimore. If you are there, look for Late Breaker Poster #5111. The poster abstract is provided below.
Neglected Tropical Diseases (NTDs) are a diverse group of communicable diseases prevailing in tropical and subtropical conditions in 149 countries and affect more than one billion people, especially those in poverty. Since 2006 The US Agency for International Development has working with global and national NTD partners to control or eliminate 5 NTDs that respond to preventive chemotherapy delivered through mass drug administration at the community level.
 As part of an evaluation of this effort, an online survey was conducted with endemic country NTD staff to learn their views on the successes and challenges of USAID NTD program support. A 22-question 3-part survey of closed and open-ended responses was posted online through Survey Monkey. A list of emails of government, NGO and donor NTD staff from 21 endemic countries was compiled. After 3 contacts, 44 English and 22 French speakers responded.
As part of an evaluation of this effort, an online survey was conducted with endemic country NTD staff to learn their views on the successes and challenges of USAID NTD program support. A 22-question 3-part survey of closed and open-ended responses was posted online through Survey Monkey. A list of emails of government, NGO and donor NTD staff from 21 endemic countries was compiled. After 3 contacts, 44 English and 22 French speakers responded.
Most respondents thought Global NTD goals aligned adequately or fully (88%) with national priorities. Respondents valued regular technical assistance from USAID as 76% rated help in annual planning useful or very useful, and well-coordinated with their own annual planning (71%). Most (71%) said the USAID NTD program had been effective in communicating its goals and accomplishments among country partners.
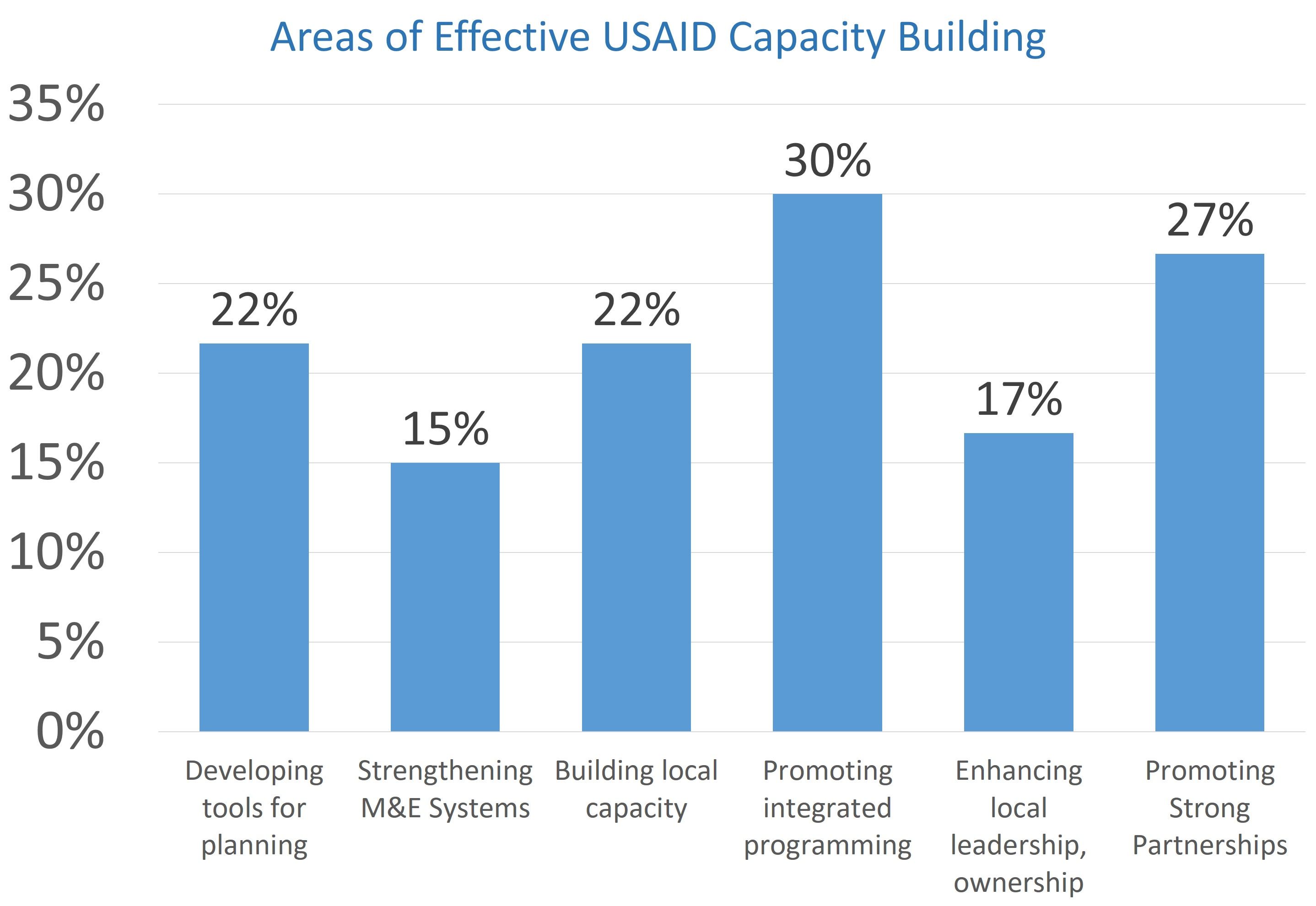 Respondents felt that documentation and dissemination of success stories could be strengthened. Specific USAID contributions were valued: “USAID gives an orientation on the tools to use, shares the guidelines to follow-up and does comments for clarifications.” When asked about integration of NTDs with other programs (WASH, PHC, and MNCH), 81% of respondents felt this was achieved to some degree, but recognized a need for national ministries to take a stronger lead. Concerning strengthening national leadership, 81% felt USAID support helped.
Respondents felt that documentation and dissemination of success stories could be strengthened. Specific USAID contributions were valued: “USAID gives an orientation on the tools to use, shares the guidelines to follow-up and does comments for clarifications.” When asked about integration of NTDs with other programs (WASH, PHC, and MNCH), 81% of respondents felt this was achieved to some degree, but recognized a need for national ministries to take a stronger lead. Concerning strengthening national leadership, 81% felt USAID support helped.
The online survey process was a valuable supplement to time-consuming country visits and ultimately provided useful input from a wider cross-section of persons involved in NTD efforts. The suggestions will guide upcoming technical assistance as countries move toward their control and elimination goals.
Integration &NTDs &Tuberculosis Bill Brieger | 24 Mar 2017
World Tuberculosis Day: United We Can End TB and Tropical Diseases
 The theme of World TB Day is to Unite to end TB: leave no one behind. The communities affected by TB are also ones where tropical diseases like onchocerciasis and malaria are endemic. A successful strategy to control one disease should ideally be “united” with all basic primary health care interventions, thereby truly leaving no one behind.
The theme of World TB Day is to Unite to end TB: leave no one behind. The communities affected by TB are also ones where tropical diseases like onchocerciasis and malaria are endemic. A successful strategy to control one disease should ideally be “united” with all basic primary health care interventions, thereby truly leaving no one behind.
While the causative agents differ between TB and tropical diseases such as malaria, lymphatic filariasis and Dengue, control of these diseases shares a common goal – “an urgent need to develop new vaccines for HIV/AIDS, malaria, and tuberculosis, as well as for respiratory syncytial virus and those chronic and debilitating (mostly parasitic) infections known as neglected tropical diseases (NTDs).” In addition to prevention, there is also need for integrated “treatment pipelines directed at NTDs, Malaria, tuberculosis (TB), and human immunodeficiency virus (HIV)/AIDS,” according to Asada.
There is also a need for integrated primary health care (PHC) programming. In the Journal of Infectious Diseases. Simon reports on linkages showing that, “Recent research suggests that NTDs can affect HIV and AIDS, tuberculosis (TB), and malaria disease progression. A combination of immunological, epidemiological, and clinical factors can contribute to these interactions and add to a worsening prognosis for people affected by HIV/AIDS, TB, and malaria.”
 The possibility of integrating directly observed treatment (DOT) for TB treatment into community health worker (CHW)/PHC programs that addressed malaria treatment and onchocerciasis control was tested by the Tropical Disease Research Program (TDR) some years ago. CHWs in a few of the study sites were able to successfully include DOT for TB in their community duties, but in other sites community and health worker fears about stigma inhibited action.
The possibility of integrating directly observed treatment (DOT) for TB treatment into community health worker (CHW)/PHC programs that addressed malaria treatment and onchocerciasis control was tested by the Tropical Disease Research Program (TDR) some years ago. CHWs in a few of the study sites were able to successfully include DOT for TB in their community duties, but in other sites community and health worker fears about stigma inhibited action.
TB, malaria and NTDs are among the conditions referred to as the infectious diseases of poverty. We will not eliminate poverty by tackling these diseases one-by-one. A “United” and integrated approach from national to community level is needed.
NTDs &Vector Control &water Bill Brieger | 22 Mar 2017
World Water Day: Water and Neglected Tropical Diseases
The United Nations introduces us to the challenges of water. “Water is the essential building block of life. But it is more than just essential to quench thirst or protect health; water is vital for creating jobs and supporting economic, social, and human development.” Unfortunately, “Today, there are over 663 million people living without a safe water supply close to home, spending countless hours queuing or trekking to distant sources, and coping with the health impacts of using contaminated water.”

Haiti: Importance of Water to prevent STH
Many of the infectious health challenges known as Neglected Tropical Diseases (NTDs) have issues of water associated with their transmission. This may relate to scarcity of water and subsequent hygiene problems. It may relate to water quality and contamination. It may also relate to water in the lifecycle of vectors that carry some of the diseases.
Even though water is crucial to the control of many NTDs, it is not often the feature of large scale interventions. The largest current activity against five NTDs is mass drug administration (MDA) on an annual or more frequent basis to break the transmission cycle. Known as diseases that respond to preventive chemotherapy (PCT) through MDA, these include lymphatic filariasis (LF), trachoma, onchocerciasis, schistosomiasis and soil transmitted helminths (STH) has been undertaken for over 10 years.
We have recently passed the Fifth Anniversary of the London Declaration on NTDs, which calls for the control of ten of the many these scourges The Declaration calls for “the elimination “by 2020 lymphatic filariasis, leprosy, sleeping sickness (human African trypanosomiasis) and blinding trachoma.” Another water-borne NTD, guinea worm, should be eradicated soon. Two of the elimination targets are part of MDA efforts, LF and trachoma.

Cameroon: mapping the community to detect NTD transmission sites
Ministries of Health and their donor and NGO partners who deliver MDA against the 5 diseases in endemic countries express interest in coordinating with water and sanitation for health (WASH) programs. People do recognize the value of collaboration between NTD MDA efforts and WASH projects, but these may be located in other ministries and organizations.
The long term implementation of WASH efforts is seen as a way to prevent resurgence of trachoma, for example, and strongly compliment efforts to control STH and schistosomiasis. Hopefully before the 10th Anniversary of the London Declaration the vision of “ensuring access to clean water and basic sanitation,” can also be achieved.
Finally as a reminder our present tools for the control of Zika and Dengue fevers relies almost entirely on safe and protected household and community sources of water to prevent breeding of disease carrying Aedes aegypti mosquitoes. If we neglect water, we will continue to experience neglected tropical diseases. Hopefully the topic of water and NTDs will feature prominently at next months global partners meeting hosted by the World Health Organization.
Diagnosis &NTDs &Schistosomiasis Bill Brieger | 19 Nov 2016
Identifying a More Accurate Test for Schistosomiasis in The Gambia
During the recently concluded 65th Annual Meeting of the American Society of Tropical Meicine and Hygiene colleagues from The Gambian Ministry of Health and Social Welfare, the World Health Organization and the NTD Support Center presented a poster entitled, “Field Performance of a Circulating Cathodic Antigen Rapid Test at Point-Of-Care for Mapping Schistosomiasis-Endemic Districts in Gambia.” The authors included Bakary Sanneh, Kristen Renneker, Joof Ebrima, Sanyang M. Abdoulie, Camara Yaya, Sambou M. Sana, Sey Alhagie Papa, Jagne Sherifo, Baldeh Ignacious, Louis-Albert Tchuem Tchuente, Patrick J Lammie, and Kisito Ogoussan. Their abstract appears below.
 Background: The traditional parasitological Kato Katz smears and urine filtration methods recommended by the World Health Organization (WHO) to implement mapping of schistosomiasis have been found to be less sensitive in the detection of light-intensity schistosomiasis infections. Field surveys in Sub-Sahara Africa have shown that the Circulating Cathodic Antigen (CCA) point-of-care (POC) test is more accurate for detecting Schistosoma mansonia than the microscopic Kato Katz technique.
Background: The traditional parasitological Kato Katz smears and urine filtration methods recommended by the World Health Organization (WHO) to implement mapping of schistosomiasis have been found to be less sensitive in the detection of light-intensity schistosomiasis infections. Field surveys in Sub-Sahara Africa have shown that the Circulating Cathodic Antigen (CCA) point-of-care (POC) test is more accurate for detecting Schistosoma mansonia than the microscopic Kato Katz technique.
Aim: To establish the field sensitivity and specificity of POC CCA as mapping tool to provide the endemicity of schistosomiasis in The Gambia.
Methods: A cross-section study …
- Ten school per region in 4 regions with historical known risk
- Fifty children aged 7 to 14 years: 25 boys and 25 girls (WHO Mapping sampling guide)
- Stool, urine and finger pricks samples were examined for Schistosomiasis
- Parasitological tests: 2 Kato-katz slides to read from each stool sample, and urine filtration technique, urine dip-stick and Circulating Cathodic Antigen (CCA) techniques,
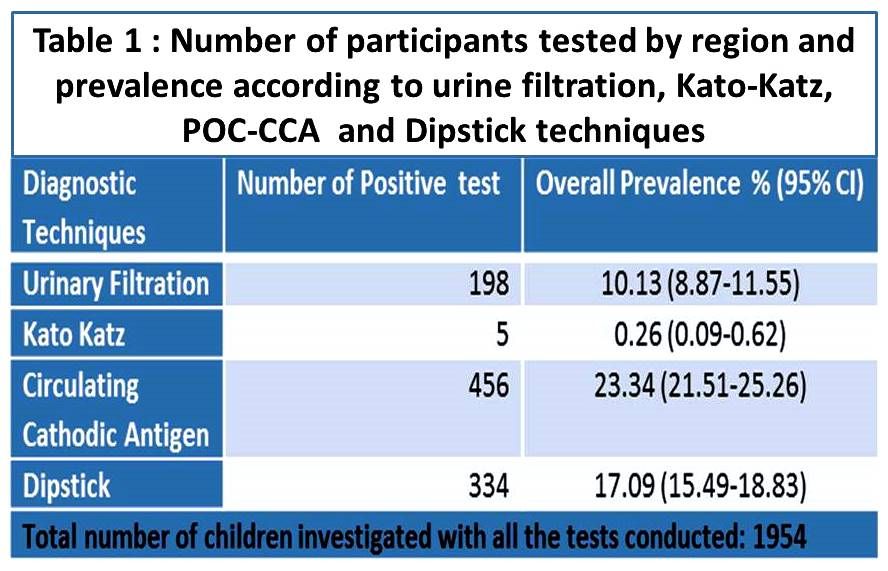 Discussion: The CCA prevalence in this study was 23.34% (95% CI, 21.51-25.26%) two times higher than the prevalence based on egg-detection for S. haematobium and S.mansoni (10.13,95% CI 8.87-11.55; and 0.26%, (95% CI, 0.09-0.62, respectively). Although The Gambia is thought to be endemic for only S. haematobium, yet 5 subjects were found to harbor S. mansoni. Three of the 5 individuals from the high endemic schistosomiasis regions were co-infected with S. haematobium and S. mansoni.
Discussion: The CCA prevalence in this study was 23.34% (95% CI, 21.51-25.26%) two times higher than the prevalence based on egg-detection for S. haematobium and S.mansoni (10.13,95% CI 8.87-11.55; and 0.26%, (95% CI, 0.09-0.62, respectively). Although The Gambia is thought to be endemic for only S. haematobium, yet 5 subjects were found to harbor S. mansoni. Three of the 5 individuals from the high endemic schistosomiasis regions were co-infected with S. haematobium and S. mansoni.
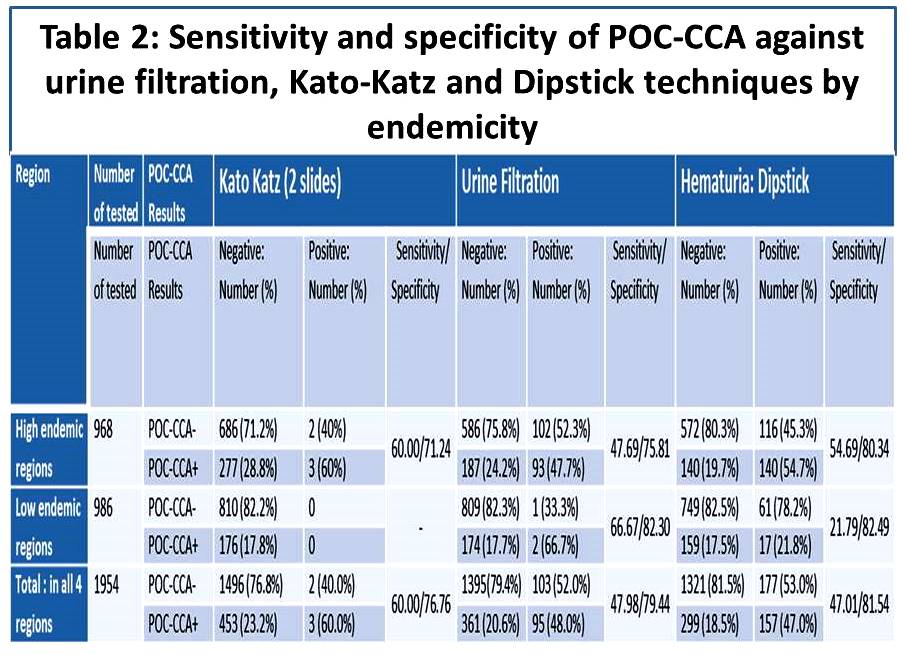 The sensitivity of the POC-CCA proved to be relatively high (60.0%), using double Kato-Katz as a reference for S. mansoni detection, although few infections were found, 5 out 1954 tested. The specificity of the POC CCA was 76.8%, respectively. Using urine filtration as reference standard for the detection of S. haematobium, the sensitivity of POC-CCA was 47.9% and the specificity was 79.4%.
The sensitivity of the POC-CCA proved to be relatively high (60.0%), using double Kato-Katz as a reference for S. mansoni detection, although few infections were found, 5 out 1954 tested. The specificity of the POC CCA was 76.8%, respectively. Using urine filtration as reference standard for the detection of S. haematobium, the sensitivity of POC-CCA was 47.9% and the specificity was 79.4%.
Conclusion: The Gambia is endemic for both urinary and intestinal schistosomiasis although most of the infections are due to S. haematobium in the 4 regions investigated. The results of the study showed a low sensitivity of the POC-CCA test in detecting S. haematobium and therefore we conclude further research is needed to develop an ideal rapid diagnosis tool for urinary schistosomiasis.
 Acknowledgement: Thanks to the Mapping Team, Consultants, MoHSW, WHO, Task Force for Global Health (TFGH) for all their support. For questions please contact: Dr. Kisito Ogoussan, kogoussan@taskforce.org; or Mr. Bakary Sanneh, sheikbakary@yahoo.com
Acknowledgement: Thanks to the Mapping Team, Consultants, MoHSW, WHO, Task Force for Global Health (TFGH) for all their support. For questions please contact: Dr. Kisito Ogoussan, kogoussan@taskforce.org; or Mr. Bakary Sanneh, sheikbakary@yahoo.com