Advocacy &ITNs &Treatment Bill Brieger | 11 Mar 2015
“Zero Malaria! Count Me In!”: Senegal’s national commitment to the Last Mile to Malaria Elimination
Yacine Djibo, Founder & President of Speak Up Africa is helping focus International Women’s Day (March 8th) on efforts to protect women from malaria in Senegal. She is highlighting the commitments of 8 strong and beautiful women, in Senegal, that are dedicated to eliminating malaria in their country. These commitments are part of an inclusive mass communication campaign that aims to launch a national movement in favor of malaria elimination in Senegal: the “Zero Malaria! Count Me In” campaign
 International Women’s Day, represents an opportunity to celebrate the achievements of women all around the world. This year’s theme is “Empowering Women – Empowering Humanity: Picture it” envisions a world where each woman and girl can exercise her choices, such as participating in politics, getting an education or fighting malaria. Below is the fifth feature on women fighting malaria.
International Women’s Day, represents an opportunity to celebrate the achievements of women all around the world. This year’s theme is “Empowering Women – Empowering Humanity: Picture it” envisions a world where each woman and girl can exercise her choices, such as participating in politics, getting an education or fighting malaria. Below is the fifth feature on women fighting malaria.
Mrs. Oulèye Bèye, Head of the Prevention & Partnership Department at the National Malaria Control Program (NMCP), likes to remind us the national claim stating that “Technicians cure malaria but communities fight it”. It is a simple, yet powerful statement that summarizes the very purpose of all our endeavors. Efforts to reach remote populations and positively change communities’ behaviors are a constant battle for the NMCP.

Mrs. Oulèye Bèye, National Malaria Control Program, Senegal
The scale up of proven interventions recommended by the World Health Organization, have been essential in achieving this drastic decrease in malaria mortality rates over the years. These strategies include ensuring the availability of Artemisinin-based combination therapy (ACT) in health facilities, the mass distribution of free mosquito nets and the introduction of rapid diagnostic tests.
To be effective, all of them require significant and unconditional uptake by beneficiaries. Needless to say that the successes achieved through effective and safe malaria control campaigns, a strong national leadership and a dynamic set of partners are all at risk, if we fail to realize that populations must no longer be considered as plain beneficiaries but as stakeholders of utmost importance.
 By leading the effort around the “Zero Malaria! Count Me In” campaign at the national level, Ouleye strives to create a popular movement and actively engage each and every Senegalese citizen in the fight for a malaria-free Senegal. Sensitization and awareness raising must be the first step of any malaria elimination intervention if we want to achieve positive results in the long run.
By leading the effort around the “Zero Malaria! Count Me In” campaign at the national level, Ouleye strives to create a popular movement and actively engage each and every Senegalese citizen in the fight for a malaria-free Senegal. Sensitization and awareness raising must be the first step of any malaria elimination intervention if we want to achieve positive results in the long run.
*****
Headquartered in Dakar, Senegal, Speak Up Africa is a creative health communications and advocacy organization dedicated to catalyzing African leadership, enabling policy change, securing resources and inspiring individual action for the most pressing issue affecting Africa’s future: child health.
ITNs Bill Brieger | 25 Jan 2015
Insecticide treated nets, a fishy subject
Not long ago I had written a blog posting suggesting that widespread misuse of ITNs/LLINs was probably not a major problem. To date the main official published information on the topic came from a community near Lake Victoria that had received an  abundance of nets through uncoordinated donor activity and the excess was being used to dry fish on the shore.
abundance of nets through uncoordinated donor activity and the excess was being used to dry fish on the shore.
True, newspaper articles over the years have featured Ministry of Health officials in numerous countries berating their citizens not to use nets for fishing, agriculture and other non-disease control needs, but evidence had not been forthcoming in the numerous national demographic, health and malaria surveys over the years. There is also the acknowledged possibility that old nets are being repurposed since there are inadequate disposal mechanisms available.
Such concerns are not idle. We also documented misuse of LLINs in Akwa Ibom State with photographs  of nets used to make football goals, protect seedlings in a nursery, cover small kiosks selling food items and penning animals. This occurred in areas where there was inadequate partnership, planning and follow-up with the community by health officials.
of nets used to make football goals, protect seedlings in a nursery, cover small kiosks selling food items and penning animals. This occurred in areas where there was inadequate partnership, planning and follow-up with the community by health officials.
Now the New York Times has stirred up the controversy again with strong visual evidence of a fishing communities in Zambia and Tanzania using ITNs for not only fishing, but also making chicken pens, ropes, footballs and football goals. People in that community explain their economic needs which are huge in this poor area of the world, and present the hard choice between augmenting their livelihoods and sleeping under an ITN. The environmental impact of the insecticides when nets are misused was also highlighted. The immediate thought is that malaria control efforts must be integrated into health and development efforts in a country.
The US President’s Malaria Initiative has issued a statement of concern. PMI recognizes that misuse of nets can depend on the particular environment (e.g. near water), but also recognizes the need, as mentioned above, of collaborating with the community to get things right in the first place. These problems will persist until national malaria control programs focus less on the total numbers of nets distributed and more on the actual factors that influence net use.
ITNs Bill Brieger | 28 Nov 2014
Is Mosquito Net Mis-Use Exaggerated
Health Officials commonly berate community members for misusing insecticide treated nets (ITNs) given out during malaria prevention campaigns and programs. Villagers are blamed for doing everything from using nets to catch or dry fish, protect crops or poultry, make football goals and cover their market goods.
For example, The Nairobi Star of 12 March 2012 reported that health officials in Nyanza, Kenya were disturbed that people were using their ITNs to protect their gardens from pests and their kitchens from rodents. The officials threatened to prosecute anyone misusing their nets.
Likewise the Lusaka Times published a story on 10 July 2011 that ITNs were being misused to made wedding dresses/veils and for fishing. “North-Western Province Minister Daniel Kalenga has directed District Commissioners in the province to report any misuse of Insecticide Treated mosquito Nets (ITNs) to the police as it is an offense under the public health Act.” A similar story appeared in April 2014.
There is some theoretical logic to net misuse. Keita Honjo and colleagues concluded from a modeling exercise that, “ITN use for malaria protection can be thwarted in settings of extreme poverty, where an increase in labour productivity by an alternative ITN use can offset the perceived benefits of avoiding malaria infection.”
One has often suspected these challenges to net use border on myth at times. Eisele and colleagues leveled the following critique against the media: “There are a number of potentially damaging misconceptions about insecticide-treated mosquito nets (ITNs) in Africa that have been propagated in media
reports, almost all of which are based on anecdotal accounts.”
Therefore, we were quite interested to learn of a newly published study that analyzed ITN use with “Data from 14 sub-national post-campaign surveys conducted in Ghana, Senegal, Nigeria (10 states), and Uganda between 2009 and 2012 (that) were pooled,” to find out what happens to “lost” nets.
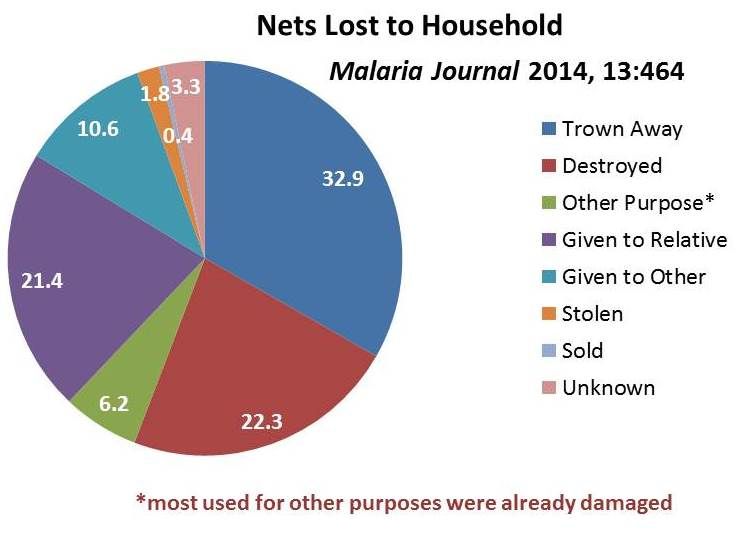 While 16% of 25,447 nets were no longer serving their original purpose, only 6.2% of those were being used for another purpose. Importantly, over 3/4 of those had been damaged prior to re-purposing. The fact that the major reason why nets left the household was because they were given to other users (e.g. relatives) implied that better assessment of community need for nets was required.
While 16% of 25,447 nets were no longer serving their original purpose, only 6.2% of those were being used for another purpose. Importantly, over 3/4 of those had been damaged prior to re-purposing. The fact that the major reason why nets left the household was because they were given to other users (e.g. relatives) implied that better assessment of community need for nets was required.
In fact re-purposing of old nets may be a natural response to failure of health agencies to devise an environmentally safe way of disposing of ITNs that have passed their natural lifetimes. Therefore WHO recommends that National malaria control and elimination programs should work with national environment authorities work together to ensure proper removal of old nets no longer in use to prevent malaria.
This reassuring article certainly takes precedence over newspaper reports of misuse, but we should still be on the look out for net use problems. A classic example appeared in Malaria Journal in 2008 documenting with data and photos the use of ITNs to dry fish along the shores of Lake Victoria. In that case the root cause of the problem was lack of coordination among agencies such that the villages were supplied more nets than they needed. This appears to have been a one-of-a-kind study.
What is more likely to happen, it seems is that households acquire their nets but for various reasons do not always hang them, as was the case with nearly 30% of recipients in a small study in Rivers State, Nigeria. Malaria control programs need to pay more attention to helping people actually hang and use their nets correctly and regularly than simply being satisfied with reporting the numbers distributed.
Communication &ITNs Bill Brieger | 02 Sep 2014
Hearing, Seeing, Changing: Bednet Behavior
An important new article in Malaria Journal by colleagues at the Johns Hopkins University Center for Communications Programs gives confidence to health educators and behavior change practitioners that their interventions do make a difference. Using the 2010 Malaria Indicator Survey (MIS) from Zambia, they were able to comparing women’s reports of exposure to behavior change communication (BCC) messages and their use of insecticide treated nets (ITNs) the previous night.
 Exposure to ITN messages was focused on women who “reported hearing or seeing any malaria messages in the past six months and also cited at least one specific channel: television or radio, in the newspaper, on posters or billboards, or from peer educators and drama groups.” Using two different analytic approaches, the authors found that exposure to messages was responsible for between 12-29% of net use. They concluded that the results “illustrate that BCC programmes can contribute to national programmes seeking to increase the use of ITNs inside the home.”
Exposure to ITN messages was focused on women who “reported hearing or seeing any malaria messages in the past six months and also cited at least one specific channel: television or radio, in the newspaper, on posters or billboards, or from peer educators and drama groups.” Using two different analytic approaches, the authors found that exposure to messages was responsible for between 12-29% of net use. They concluded that the results “illustrate that BCC programmes can contribute to national programmes seeking to increase the use of ITNs inside the home.”
The recent MIS in a variety of endemic countries have taken up the task of measuring not just use of ITNs but also knowledge of the role of ITNs in preventing malaria and exposure to BCC messaging about ITNs. Similar analysis should be performed on these data sets.
 The 2010 Nigeria MIS, for example, reported that 27.9% of women reported exposure to malaria messages in 4 weeks prior to the study. Likewise 57.9% of women had knowledge that Sleeping under mosquito net prevents malaria in pregnancy (MIP). The 2012 MIS from Malawi reported that 25.3 women claimed exposure to malaria messages in past 4 weeks, and of those, 87.3% had knowledge that Sleeping under mosquito net prevents MIP.
The 2010 Nigeria MIS, for example, reported that 27.9% of women reported exposure to malaria messages in 4 weeks prior to the study. Likewise 57.9% of women had knowledge that Sleeping under mosquito net prevents malaria in pregnancy (MIP). The 2012 MIS from Malawi reported that 25.3 women claimed exposure to malaria messages in past 4 weeks, and of those, 87.3% had knowledge that Sleeping under mosquito net prevents MIP.
A 2011 survey in Ghana found that 57.3% of women claimed exposure to malaria messages in past 4 weeks, and of those 83.7% had knowledge that Sleeping under and ITN prevents MIP. A question remains though, what was the actual nature of those media efforts to which women claim exposure?
The surveys do note the broad sources of information, e.g. radio, health workers/clinic, community activities. A review of overall national malaria strategies and specific malaria BCC documents will certainly indicate that national programs and their partners intend to engage in a variety of BCC activities. The issue is whether, where and how those activities took place.
To give more validity to BCC outcomes, we must also encourage national malaria programs and their partners to document better their BCC activities so we can more easily attribute ITN behavior change itself to specific, funded interventions.
Burden &ITNs &Morbidity Bill Brieger | 25 Jul 2014
Attaining and Sustaining – malaria targets
Recent reports on the Global Burden of Disease with a focus on Millennium Development Goal #6 has stressed the improvement in malaria morbidity and mortality indicators since the Abuja Declaration of 2000. In particular, “Global malaria incidence peaked in 2003, with 232 million new cases, subsequently falling by about 29% to 165 million new cases in 2013.”
The improvements are attributed in part to the large increase in funding. The remaining challenge derives in part from the fact that four countries, India, Nigeria, Democratic Republic of the Congo and Mozambique account for nearly two-thirds of the global case load. Global progress in reducing disease has been achieved despite the fact that in these and many other countries, achievement of 2010 targets for malaria intervention coverage (80%) have lagged. In some cases national surveys have shown some declines in coverage (e.g. Nigeria).
 Ghana provides a good example of the challenges. National surveys in 2006, 2008 and 2011 have shown mixed results in the use of insecticide treated nets by children below the age of 5 years. While the proportion rose from 20% to 39% between the first two surveys, it stayed steady in 2011. A new survey in underway, but as of 2012 there were still areas of the country that needed nets, and we know that nets wear out in between distributions and need to be replaced through routine services as seen in the photo.
Ghana provides a good example of the challenges. National surveys in 2006, 2008 and 2011 have shown mixed results in the use of insecticide treated nets by children below the age of 5 years. While the proportion rose from 20% to 39% between the first two surveys, it stayed steady in 2011. A new survey in underway, but as of 2012 there were still areas of the country that needed nets, and we know that nets wear out in between distributions and need to be replaced through routine services as seen in the photo.
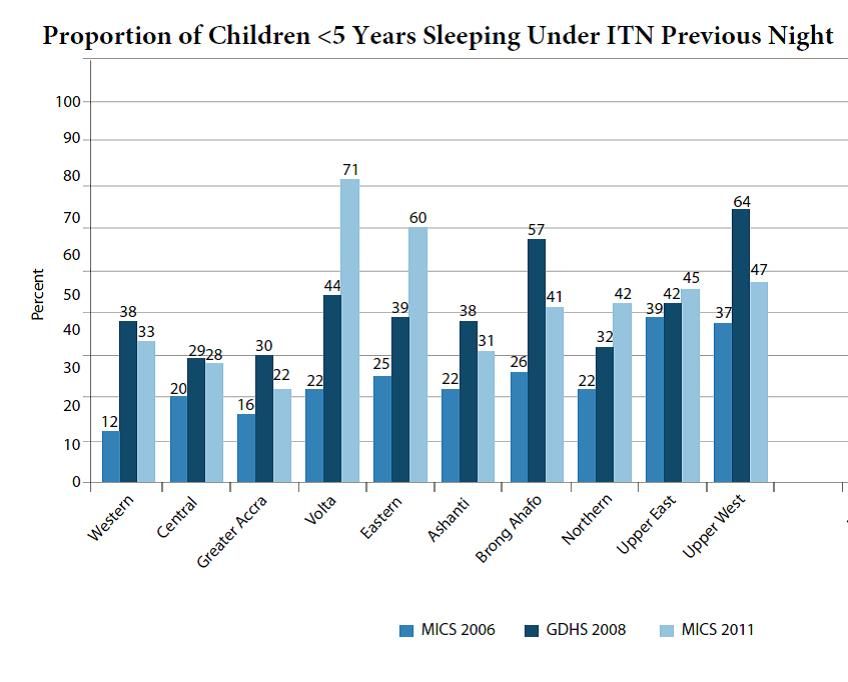 The three surveys so far in Ghana paint a mixed picture as seen in the attached graph. In six of the ten regions, net coverage for young children declined and in four it increased over the period. This on balance led to the lack of overall improvement.
The three surveys so far in Ghana paint a mixed picture as seen in the attached graph. In six of the ten regions, net coverage for young children declined and in four it increased over the period. This on balance led to the lack of overall improvement.
Thinking back to the reduced burden of disease overall, one can surmise that even some level of malaria intervention can impact on incidence of the disease, but the goal was no mortality for 2015, just one year from now. If the trend seen in Ghana (which is reflective of other countries) continues, we will pass 2015 without attaining the 2010 coverage targets and still experience an unacceptable malaria disease burden. Malaria elimination looks farther away each day.
Congenital Malaria &IPTp &ITNs &Malaria in Pregnancy &Mortality Bill Brieger | 12 Jun 2014
Congenital Malaria, an Underappreciated Neonatal Problem
The largest portion of infant deaths occurs in the neonatal period. During those first 28 days, the child is at risk from a variety of problems arising from delivery complications, infections and simply not being kept warm.
 In malaria endemic areas there is the small but important problem of malaria transferred from mother to child, or congenital malaria. The problem occurs with both Plasmodium vivax and falciparum.
In malaria endemic areas there is the small but important problem of malaria transferred from mother to child, or congenital malaria. The problem occurs with both Plasmodium vivax and falciparum.
Congenital malaria in the newborn is often hard to detect. There may be fever, but other signs and symptoms might include anaemia, jaundice, paleness, diarrhoea, vomiting, and general weakness.
Prevalence of congenital malaria in Ghana, for example, ranged from 2% by microscopy to 12% using polymerase chain reaction (PCR). In India microscopy revealed a prevalence of 3% with cases of both vivax and falciparum.
One would hope this problem could be avoided if prevention of malaria in pregnancy was practiced using insecticide treated nets, intermittent preventive treatment (IPTp) and prompt and appropriate case management, but studies still find placental and cord parasiteamia in countries where such interventions are supposed to be integrated into antenatal/prenatal care. In Colombia, “An association was found between congenital malaria and the diagnosis of malaria in the mother during the last trimester of pregnancy or during delivery, and the presence of placental infection.”
Countries are in the process of shifting to the relatively new WHO guidance on IPTp that encourages monthly doses of sulfadoxine-pyrimethamine from the beginning of the second trimester up until delivery. Countries are also trying to ensure universal coverage of ITNs so that women will be using nets prior to even becoming pregnant.
We still have trouble administering to take just two doses of IPTp, but if we want to prevent congenital malaria, we need to ensure that women are protected from malaria in their placentas and are free from parasites right up until they give birth and thereby prevent another cause of neonatal mortality.
ITNs &Malaria in Pregnancy Bill Brieger | 26 May 2014
Women’s Education and Bed Net Use in Nigeria
Concern about women’s and girl’s education in Nigeria and worldwide has peaked with the abduction of around 300 female secondary school school students in northeastern Nigeria. Normally we see many positive benefits of women’s education in various health indicators, but it appears that bednet use does not follow that trend neatly.
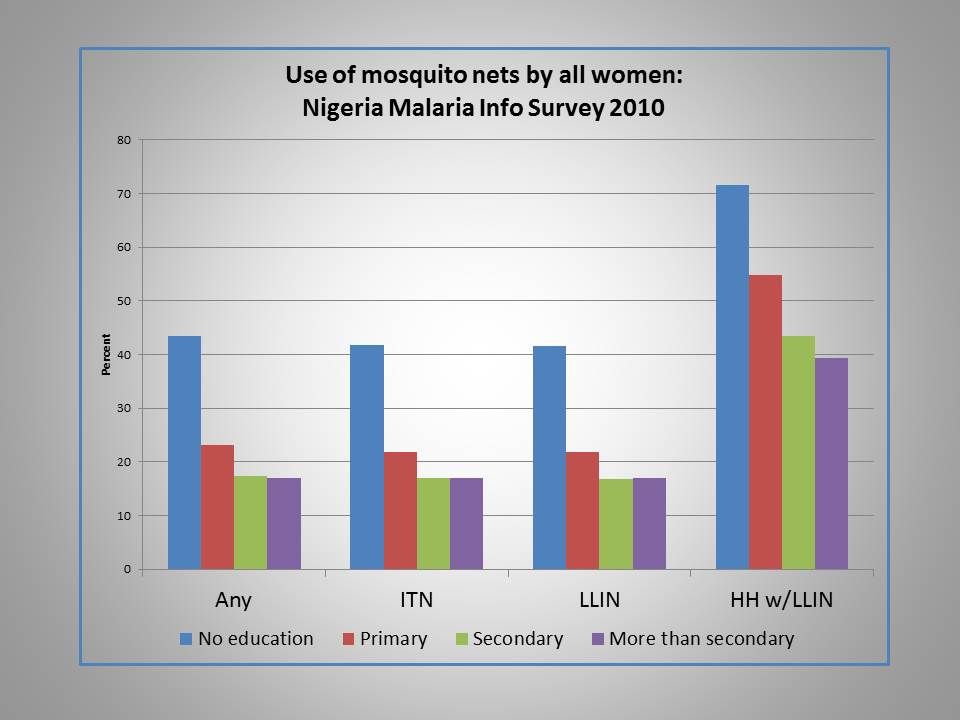 Analysis of bednet use in the Nigeria Malaria Indicator Survey (MIS) of 2010 found that ironically net use of all kinds, including ordinary nets, insecticide treated nets and long lasting insecticide-treated nets actually decreased as educational level of women increased.
Analysis of bednet use in the Nigeria Malaria Indicator Survey (MIS) of 2010 found that ironically net use of all kinds, including ordinary nets, insecticide treated nets and long lasting insecticide-treated nets actually decreased as educational level of women increased.
Interestingly the same picture is painted for levels of wealth with 41% in the lowest quintile using any kind of net the night before the survey versus 16% for the highest quintile. Also of note, 19% of urban women reported using any kind of net versus 34% in the rural areas.
In contrast the 2010 Nigerian MIS found that only 22% of women without education had received any antenatal care (ANC) during a recent pregnancy compared to 89% with greater than secondary education. Getting at least two doses of intermittent preventive treatment (IPTp) during ANC was only 7% for those without formal education, but 24% for those with higher than secondary education. Why does bednet use show a reverse trend here?
One factor may be the delivery mechanism. ANC and IPTp require utilization of a service with all the economic and intra-family dynamics that this implies. Nets have so far been mainly provided during outreach campaigns. Is there an element of equity going on here with an effort to reach the less educated and poorer segment of society with nets?
Also educated people and those with relatively greater wealth may have better housing conditions that are less likely to encourage mosquito entry. Such families may perceive that they have less need for nets if they actually have ceilings and windows with netting.
Just by way of comparison, a similar picture of net use was was seen in the Malawi MIS of 2012. That survey only recorded three levels of education and the contrast between highest and lowest use was only about 10% points compared to 25% difference in Nigeria.
Colleagues have recently documented gaps in net access and use across many countries. We need to ensure not only that nets reach a house, but that adequate numbers of nets are available for universal coverage (UC = at least one for every two residents – though this adequacy calculation depends on cultural sleeping patterns).
Malaria control efforts since 2009 have been aiming at UC, but various surveys have shown this goal to be elusive, let alone sustainable, since nets need to be replaced every 2-3 years. It is encouraging if some element of equity might underlie net distribution, but we still need to learn more about why people get and use nets or alternatives to ensure that all women and other household members are truly protected from malaria.
ITNs &water Bill Brieger | 22 Mar 2014
Water for Malaria
As today is World Water Day it is time to reflect on the relationship between water and malaria. As USAID notes, “The impact of water on all aspects of development is undeniable: A safe drinking water supply, adequate sanitation and hygiene, management of water resources, and improvement of water productivity can help change the lives of millions.”
 The key to the relationship between water and malaria is the word safe. The breeding of the malaria carrying anopheles mosquito species certainly depends on unsafe collections of “clean” but unmoving sources water that could range from a village pond to a cow hoof print. During certain seasons these are ubiquitous.
The key to the relationship between water and malaria is the word safe. The breeding of the malaria carrying anopheles mosquito species certainly depends on unsafe collections of “clean” but unmoving sources water that could range from a village pond to a cow hoof print. During certain seasons these are ubiquitous.
Seid Tiku Mereta and colleagues showed us recently that humans may be their own worst enemies when it comes to producing mosquito larval breeding sites. They found that Anopheline mosquito larvae showed a widespread distribution and especially occurred in small human-made aquatic habitats… In contrast, anopheline mosquito larvae were found to be less prominently present in permanent larval habitats. This could be attributed to the high abundance and diversity of natural predators and competitors suppressing the mosquito population densities.”
The drier parts of northern Benin Republic were studied by Renaud Govoetchan and team. They also found that human activity created water sources in urban areas in the dry season thereby “maintaining the breeding of anopheles larvae and the malaria transmission.” In the rural areas village ponds provided opportunity for dry season mosquito breeding. Although transmission was lower in the dry season and in the urban areas, it still persisted thanks to human water use behaviors and persistence of unsafe rural water sources.
 From the above we can see that safe water alone would not prevent malaria. Water use behaviors must also be targeted. That said, it is interesting how water may also be related to other malaria interventions such as insecticide treated nets and case management with local herbs.
From the above we can see that safe water alone would not prevent malaria. Water use behaviors must also be targeted. That said, it is interesting how water may also be related to other malaria interventions such as insecticide treated nets and case management with local herbs.
A major factor that influences the durability of the so-called long lasting insecticide treated nets (LLINs) is how often people wash them. Frequent washing of curtains, bed sheets and of course personal clothing is so routine that villagers may not even consider this hygenic behavior to be harmful. In fact it reduces the potency of the insecticide-treated nets.
Virgile Gnanguenon and co-researchers found that LLINs that might be expected to last 3 years if they were only occasionally washed were in fact only likely to be functional for two years or less. Water issues were prominent among the five factors that predicted net integrity and survival: “washing frequency, proximity to water for washing, location of kitchen, type of cooking fuel, and low net maintenance.”
Finally because primary health care does not reach all, community members still use their indigenous herbs to treat malaria. A recent study by Sabine Montcho and colleagues found an unexpected risk from the herbs. In Benin the plant Senna rotundifolia Linn. is commonly used for malaria treatment. Unfortunately the researchers learned that it was contaminated with lead and cadmium. “In terms of risk assessment through the consumption of Senna, the values recorded for lead were nine times higher with children and six times higher with adults than the daily permissive intake.” Polluted water does not have to be drunk directly to harm people.
Our relationships with water and malaria and the connection between the two are complex. World Water Day should provide us an opportunity to consider how our interventions ranging from appropriate use and care of LLINs, to provision of appropriate malaria treatment to larvae control and environmental management need to take into consideration the importance of water to human survival and disease prevention.
Elimination &IPTp &ITNs &Treatment Bill Brieger | 06 Dec 2013
Draft Nigeria 2013 DHS Shows Slow Progress for Malaria
The Nigeria Demographic and Health Survey (DHS) 2013 Draft Preliminary Report from the National Population Commission, Abuja, Nigeria and MEASURE DHS, ICF International, Calverton, Maryland, USA was released in-country in September 2013. These are the same organizations that conducted the 2010 Malaria Information Survey (MIS).
From the malaria perspective this has been a long anticipated event since the country has distributed over 60 million long lasting insecticide-treated nets since 2009. The 2010 MIS showed some progress over the 2008 DHS, but since it took place near the beginning of the massive net distribution effort, there was hope that a subsequent survey would highlight an improvement. If that were the expectation, people will be quite disappointed.
Lets start with nets. Our attached table shows only a slight improvement in the proportion of households owning at least one net. The idea behind the massive net campaigns from 2009-12 were achievement of universal coverage where there would be at least one net for every two people in a household. Where did these nets go? Were they damaged beyond use in the relatively short time that elapsed?
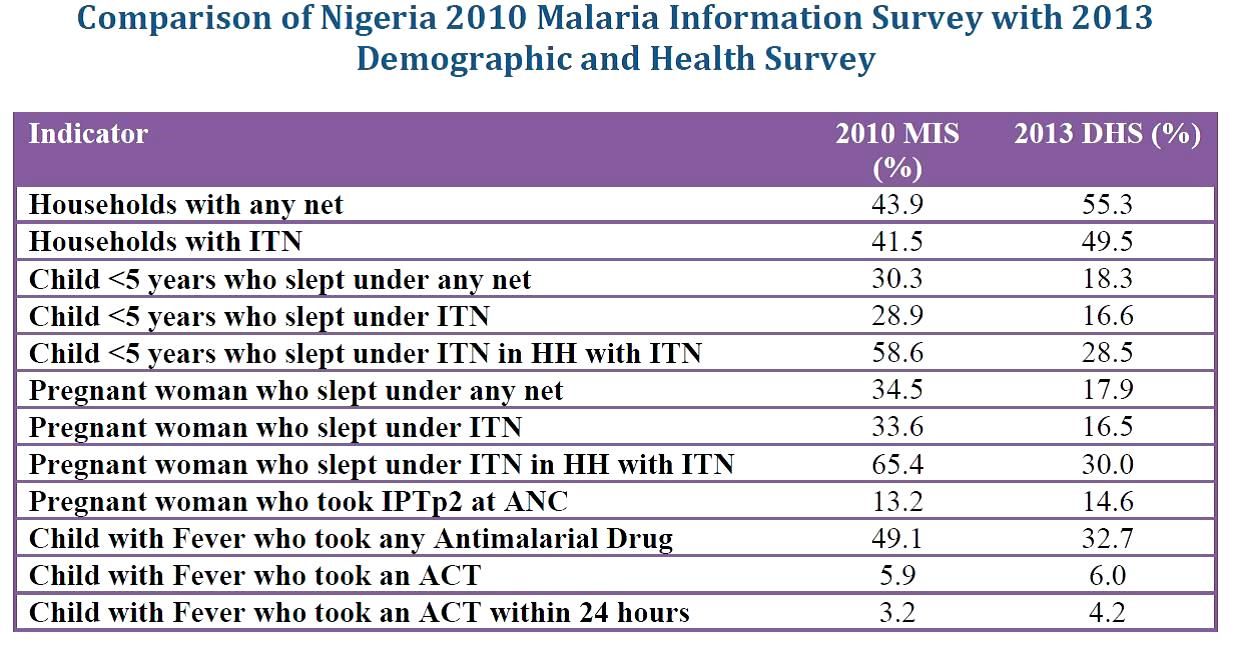 What is more disappointing is that th proportion of young children and pregnant women sleeping under an insecticide treated net (ITN) reduced to just slightly over half of the 2010 figure. This reduction also happened even in households that actually owned ITNs. This is mysterious to say the least.
What is more disappointing is that th proportion of young children and pregnant women sleeping under an insecticide treated net (ITN) reduced to just slightly over half of the 2010 figure. This reduction also happened even in households that actually owned ITNs. This is mysterious to say the least.
Prevention of malaria in pregnancy has been a neglected part of malaria control in many countries, but since the drug used for intermittent preventive treatment (IPT), sulphadoxine-pyrimethamine (SP) is so cheap, it was assumed that most health systems could afford to guarantee every woman attending antenatal care the required dosed. Unfortunately the status of IPT showed almost no improvement between 2010 and 2013 and remained far, far below the 2010 Roll Back Malaria target of 80% coverage. SP is produced in Nigeria; why can it not reach pregnant women?
Finally appropriate malaria treatment of young children is also in the doldrums. The actual number of children who received any anti-malarial drug declined, while those receiving the appropriate artemisinin-based combination therapy (ACT) remained essentially level at around 6%. Where have all the ACTs brought in through Global Fund, the US President’s Malaria Initiative and other donors gone? How can we expect infant and child mortality to decrease in the absence of appropriate treatment for one of the most common child killer diseases?
At the recently concluded 6th Pan African Malaria Conference in Durban, South Africa, participants were told that the only way to truly eliminate malaria is to tackle the high burden countries like Nigeria head on. If these data indicate how we are waging the malaria battle in Nigeria, our hopes for elimination in the near future will be dashed.
Community &ITNs Bill Brieger | 06 Nov 2013
Building Community Capacity in Malaria Control: the Malaria Communities Program
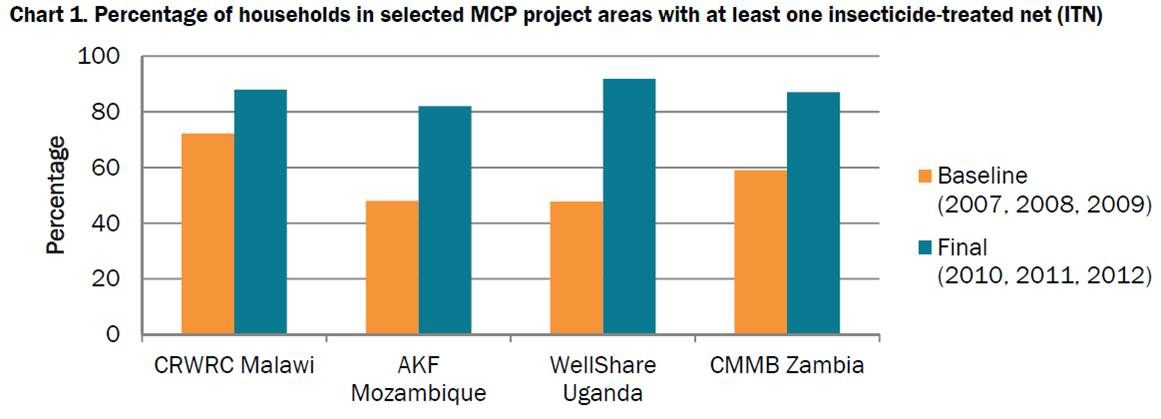
The Malaria Communities Program (MCP) was launched on December 14, 2006. Through 20 awards to 18 partners in 12 countries, the President’s Malaria Initiative (PMI) has supported efforts of communities and nongovernmental organizations (NGOs) to combat malaria at the local level. Excerpts from one of the MCP case studies are found below.
This case study examines different models of community outreach and engagement implemented by five MCP partners: the Christian Reformed World Relief Committee (CRWRC) Malawi, HealthPartners Uganda, Catholic Medical Mission Board (CMMB) Zambia, Aga Khan Foundation (AKF) Mozambique in partnership with Progresso, and Lutheran World Relief (LWR) Mali. MCHIP collected multiple forms of data from these five partners using qualitative methods, including individual interviews with key project personnel and review of key documents.
MCHIP then compared data across projects to better understand the overall contributions made by MCP. Some partners conducted surveys, and this report includes relevant quantitative data. Data are limited by a lack of standardized reporting on this topic. Future studies about the relationship between community capacity and malaria control could utilize frameworks described in relevant literature for planning and reporting results.
 The major sub-theme emerging from the data was effective utilization of community volunteers as a way to build community capacity and sustain project results. Each partner’s strategy to engage and retain volunteers included these key attributes: selection of volunteers, motivation/retention of volunteers, ensuring sustainability of the volunteer program, and addressing challenges. Building community capacity can be described as the means by which communities and individuals enhance their skills, abilities, resources, and commitments to identify challenges and solutions in their communities, and nurture their unique talents and leadership. In this process, individuals and groups increase their abilities to impact the health and vitality of their communities.
The major sub-theme emerging from the data was effective utilization of community volunteers as a way to build community capacity and sustain project results. Each partner’s strategy to engage and retain volunteers included these key attributes: selection of volunteers, motivation/retention of volunteers, ensuring sustainability of the volunteer program, and addressing challenges. Building community capacity can be described as the means by which communities and individuals enhance their skills, abilities, resources, and commitments to identify challenges and solutions in their communities, and nurture their unique talents and leadership. In this process, individuals and groups increase their abilities to impact the health and vitality of their communities.
MCP partners trained, empowered, and equipped volunteers with skills and tools to promote key messages about malaria prevention and treatment. MCP partnerships with National Malaria Control Programs (NMCPs) and community members have strengthened local ownership by facilitating community-driven processes for volunteer selection and supervision.
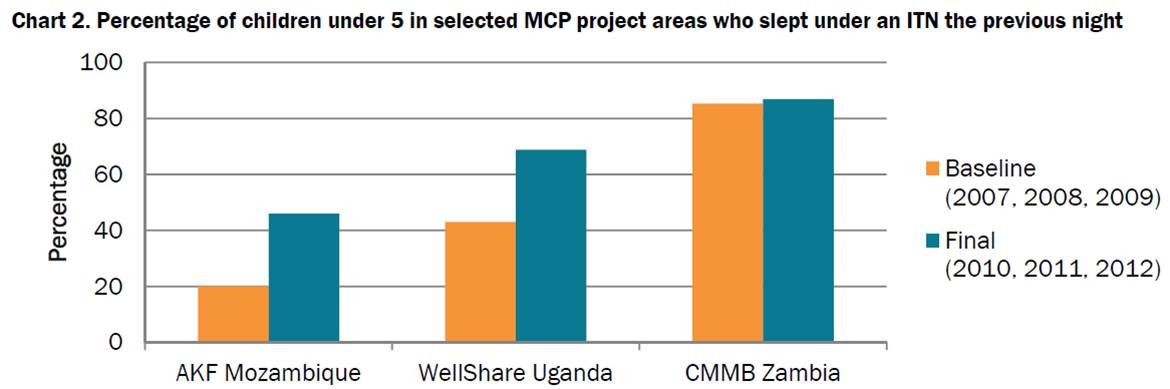 Trained volunteers have helped increase community demand for nets and fostered trust between health workers and community volunteers, creating a foundation for communities to control malaria. Charts 1 and 2 show positive trends in selected MCP project areas in net ownership and use, which may result from strengthened community capacity, as seen in the Zambia study.
Trained volunteers have helped increase community demand for nets and fostered trust between health workers and community volunteers, creating a foundation for communities to control malaria. Charts 1 and 2 show positive trends in selected MCP project areas in net ownership and use, which may result from strengthened community capacity, as seen in the Zambia study.
Download and read the full case study at: http://www.mchip.net/node/2069
See also: Underwood C et al. 2013 Community capacity as means to improved health practices and an end in itself: Evidence from a multi-stage study. Intl Quarterly of Community Health Education 33(2): 105–127.