Asymptomatic &Burden &Dengue &Diagnosis &Ebola &Elimination &Epidemiology &Health Systems &ITNs &MDA &Mosquitoes &NTDs &Schistosomiasis &Schools &Vector Control &Zoonoses Bill Brieger | 30 Jun 2019
The Weekly Tropical Health News 2019-06-29
Below we highlight some of the news we have shared on our Facebook Tropical Health Group page during the past week.
Polio Persists
If all it took to eradicate a disease was a well proven drug, vaccine or technology, we would not be still reporting on polio, measles and guinea worm, to name a few. In the past week Afghanistan reported 2 wild poliovirus type 1 (WPV1) cases, and Pakistan had 3 WPV1 cases. Circulating vaccine-derived poliovirus type 2 (cVDPV2) was reported in Nigeria (1), DRC (4) and Ethiopia (3) from healthy community contacts.
Continued Ebola Challenges
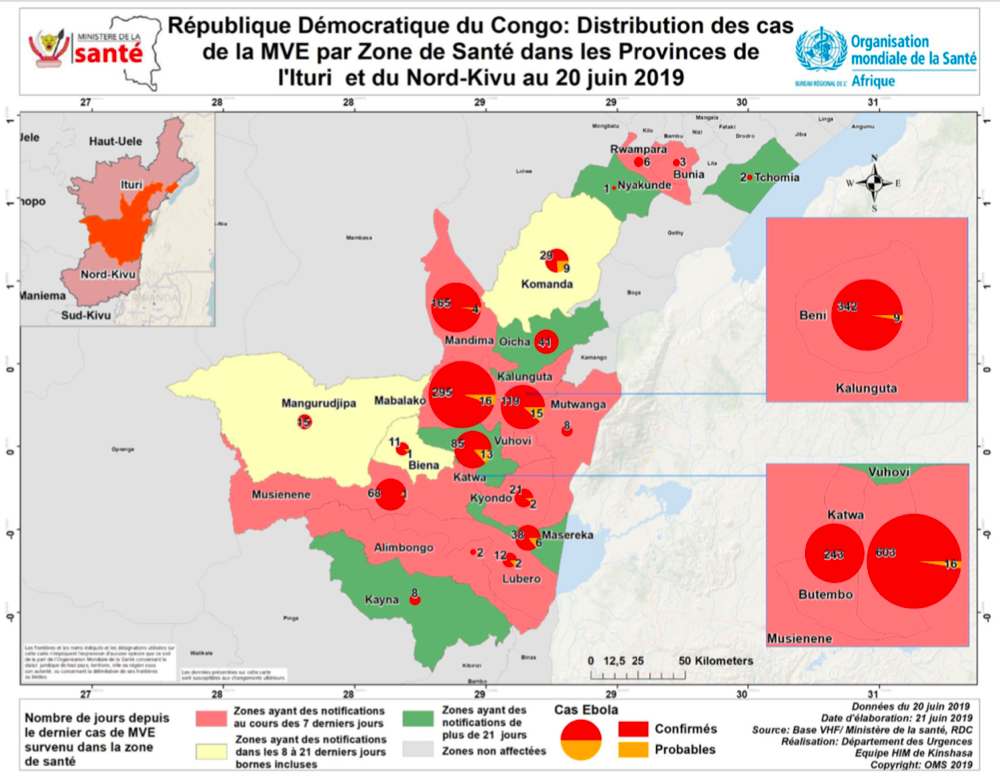
In the seven days from Saturday to Friday (June 28) there were 71 newly confirmed Ebola Cases and 56 deaths reported by the Democratic Republic of Congo’s Ministry of Health. As Ebola cases continue to pile up in the Democratic Republic of the Congo (DRC), with 12 more confirmed Thursday and 7 more Friday, a USAID official said four major donors have jump-started a new strategic plan for coordinating response efforts. To underscore the heavy toll the outbreak has caused, among its 2,284 cases, as noted on the World Health Organization Ebola dashboard today, are 125 infected healthcare workers, including 2 new ones, DRC officials said.
Pacific Standard explained the differences in Ebola outbreaks between DRC today and the West Africa outbreak of 2014-16. On the positive side are new drugs used in organized trials for the current outbreak. The most important factor is safe, effective vaccine that has been tested in 2014-16, but is now a standard intervention in the DRC. While both Liberia and Sierra Leone had health systems and political weaknesses as post-conflict countries, DRC’s North Kivu and Ituri provinces are currently a war zone, effectively so for the past generation. Ebola treatment centers and response teams are being attacked. There are even cultural complications, a refusal to believe that Ebola exists. So even with widespread availability of improved technologies, teams may not be able to reach those in need.
To further complicate matters in the DRC, Doctors Without Borders (MSF) “highlighted ‘unprecedented’ multiple crises in the outbreak region in northeastern DRC. Ebola is coursing through a region that is also seeing the forced migration of thousands of people fleeing regional violence and is dealing with another epidemic. Moussa Ousman, MSF head of mission in the DRC, said, ‘This time we are seeing not only mass displacement due to violence but also a rapidly spreading measles outbreak and an Ebola epidemic that shows no signs of slowing down, all at the same time.’”
NIPAH and Bats
Like Ebola, NIPAH is zoonotic, and also involves bats, but the viruses differ. CDC explains that, “Nipah virus (NiV) is a member of the family Paramyxoviridae, genus Henipavirus. NiV was initially isolated and identified in 1999 during an outbreak of encephalitis and respiratory illness among pig farmers and people with close contact with pigs in Malaysia and Singapore. Its name originated from Sungai Nipah, a village in the Malaysian Peninsula where pig farmers became ill with encephalitis.
A recent human outbreak in southern India has been followed up with a study of local bats. In a report shared by ProMED, out of 36 Pteropus species bats tested for Nipah, 12 (33%) were found to be positive for anti-Nipah bat IgG antibodies. Unlike Ebola there are currently no experimental drugs or vaccines.
Climate Change and Dengue
Climate change is expected to heighten the threat of many neglected tropical diseases, especially arboviral infections. For example, the New York Times reports that increases in the geographical spread of dengue fever. Annually “there are 100 million cases of dengue infections severe enough to cause symptoms, which may include fever, debilitating joint pain and internal bleeding,” and an estimated 10,000 deaths. Dengue is transmitted by Aedes mosquitoes that also spread Zika and chikungunya. A study, published Monday in the journal Nature Microbiology, found that in a warming world there is a strong likelihood for significant expansion of dengue in the southeastern United States, coastal areas of China and Japan, as well as to inland regions of Australia. “Globally, the study estimated that more than two billion additional people could be at risk for dengue in 2080 compared with 2015 under a warming scenario.”
Schistosomiasis – MDA Is Not Enough, and Neither Are Supplementary Interventions
Schistosomiasis is one of the five neglected tropical diseases (NTDs) that are being controlled and potentially eliminated through mass drug administration (MDA) of preventive chemotherapy (PCT), in this case praziquantel. In The Lancet Knopp et al. reported that biannual MDA substantially reduced Schistosomiasis haematobium prevalence and infection intensity but was insufficient to interrupt transmission in Zanzibar. In addition, neither supplementary snail control or behaviour change activities did not significantly boost the effect of MDA. Most MDA programs focus on school aged children, and so other groups in the community who have regular water contact would not be reached. Water and sanitation activities also have limitations. This raises the question about whether control is acceptable for public health, or if there needs to be a broader intervention to reach elimination?
Trachoma on the Way to Elimination
Speaking of elimination, WHO has announced major “sustained progress” on trachoma efforts. “The number of people at risk of trachoma – the world’s leading infectious cause of blindness – has fallen from 1.5 billion in 2002 to just over 142 million in 2019, a reduction of 91%.” Trachoma is another NTD that uses the MDA strategy.
The news about NTDs from Dengue to Schistosomiasis to Trachoma is complicated and demonstrates that putting diseases together in a category does not result in an easy choice of strategies. Do we control or eliminate or simply manage illness? Can our health systems handle the needs for disease elimination? Is the public ready to get on board?
Malaria Updates
And concerning being complicated, malaria this week again shows many facets of challenges ranging from how to recognize and deal with asymptomatic infection to preventing reintroduction of the disease once elimination has been achieved. Several reports this week showed the particular needs for malaria intervention ranging from high burden areas to low transmission verging on elimination to preventing re-introduction in areas declared free from the disease.
In South West, Nigeria Dokunmu et al. studied 535 individuals aged from 6 months were screened during the epidemiological survey evaluating asymptomatic transmission. Parasite prevalence was determined by histidine-rich protein II rapid detection kit (RDT) in healthy individuals. They found that, “malaria parasites were detected by RDT in 204 (38.1%) individuals. Asymptomatic infection was detected in 117 (57.3%) and symptomatic malaria confirmed in 87 individuals (42.6%).
Overall, detectable malaria by RDT was significantly higher in individuals with symptoms (87 of 197/44.2%), than asymptomatic persons (117 of 338/34.6%)., p = 0.02. In a sub-set of 75 isolates, 18(24%) and 14 (18.6%) individuals had Pfmdr1 86Y and 1246Y mutations. Presence of mutations on Pfmdr1 did not differ by group. It would be useful for future study to look at the effect of interventions such as bednet coverage. While Southwest Nigeria is a high burden area, the problem of asymptomatic malaria will become an even bigger challenge as prevalence reduces and elimination is in sight.
Sri Lanka provides a completely different challenge from high burden areas. There has been no local transmission of malaria in Sri Lanka for 6 years following elimination of the disease in 2012. Karunasena et al. report the first case of introduced vivax malaria in the country by diagnosing malaria based on microscopy and rapid diagnostic tests. “The imported vivax malaria case was detected in a foreign migrant followed by a Plasmodium vivax infection in a Sri Lankan national who visited the residence of the former. The link between the two cases was established by tracing the occurrence of events and by demonstrating genetic identity between the parasite isolates. Effective surveillance was conducted, and a prompt response was mounted by the Anti Malaria Campaign. No further transmission occurred as a result.”
Bangladesh has few but focused areas of malaria transmission and hopes to achieve elimination of local transmission by 2030. A particular group for targeting interventions is the population of slash and burn cultivators in the Rangamati District. Respondents in this area had general knowledge about malaria transmission and modes of prevention and treatment was good according to Saha and the other authors. “However, there were some gaps regarding knowledge about specific aspects of malaria transmission and in particular about the increased risk associated with their occupation. Despite a much-reduced incidence of malaria in the study area, the respondents perceived the disease as life-threatening and knew that it needs rapid attention from a health worker. Moreover, the specific services offered by the local community health workers for malaria diagnosis and treatment were highly appreciated. Finally, the use of insecticide-treated mosquito nets (ITN) was considered as important and this intervention was uniformly stated as the main malaria prevention method.”
Kenya offers some lessons about low transmission areas but also areas where transmission may increase due to climate change. A matched case–control study undertaken in the Western Kenya highlands. Essendi et al. recruited clinical malaria cases from health facilities and matched to asymptomatic individuals from the community who served as controls in order to identify epidemiological risk factors for clinical malaria infection in the highlands of Western Kenya.
“A greater percentage of people in the control group without malaria (64.6%) used insecticide-treated bed nets (ITNs) compared to the families of malaria cases (48.3%). Low income was the most important factor associated with higher malaria infections (adj. OR 4.70). Houses with open eaves was an important malaria risk factor (adj OR 1.72).” Other socio-demographic factors were examined. The authors stress the need to use local malaria epidemiology to more effectively targeted use of malaria control measures.
The key lesson arising from the forgoing studies and news is that disease control needs strong global partnerships but also local community investment and adaptation of strategies to community characteristics and culture.
Borders &Diagnosis &Ebola &Elimination &Eradication &Health Systems &Measles &Surveillance &Vaccine &Yaws Bill Brieger | 22 Jun 2019
The Weekly Tropical Health News Update 2019-06-22
For almost 20 years we have been maintaining an email list where current news and articles have been shared with those interested in tropical health and malaria. The listserve host we have been using is changing to a paid model. While there are still some free listserve options, these are cumbersome to produce. Since we are already maintaining this blog, we thought it best to provide a weekly summary of key news events through this medium.
Mapping Plasmodium Vivax
The Malaria Atlas Project has published in The Lancet a global burden of Plasmodium Vivax mapping study. The authors describe the contribution of this study as: “Our study highlights important spatial and temporal patterns in the clinical burden and prevalence of P vivax. Amid substantial progress worldwide, plateauing gains and areas of increased burden signal the potential for challenges that are greater than expected on the road to malaria elimination. These results support global monitoring systems and can inform the optimisation of diagnosis and treatment where P vivax has most impact.”
Ebola Spread from DRC to Uganda
 Since the major ongoing outbreak of Ebola Virus Disease in North Kivu and Ituri Provinces of the Democratic Republic of Congo (DRC) started nearly a year ago, there has been concern that the disease might spread to neighboring countries like Uganda, Rwanda, South Sudan and the Central African Republic. This fear same true recently when a family affected by Ebola crossed from DRC into Uganda to connect with relatives in Kasese District Uganda. Uganda has had many years’ experience dealing with Ebola and was able to contain the situation.
Since the major ongoing outbreak of Ebola Virus Disease in North Kivu and Ituri Provinces of the Democratic Republic of Congo (DRC) started nearly a year ago, there has been concern that the disease might spread to neighboring countries like Uganda, Rwanda, South Sudan and the Central African Republic. This fear same true recently when a family affected by Ebola crossed from DRC into Uganda to connect with relatives in Kasese District Uganda. Uganda has had many years’ experience dealing with Ebola and was able to contain the situation.
A press release this week noted that, “As of today (21 June 2019), Uganda has not registered any new confirmed Ebola Virus Disease (EVD) case in Kasese District or any other part of Uganda since the last registered case one week ago. There are no new suspect cases under admission. Currently, 110 contacts to the confirmed Ebola cases in Kagando and Bwera are being followed up daily. A total of 456 individuals have been vaccinated against EVD using the Ebola-rVSV vaccine in Kasese District, Western Uganda.”
Although many people expected that the meeting of the “International Health Regulations (2005) Emergency Committee} for Ebola virus disease in the Democratic Republic of the Congo would finally declare the current outbreak a Public Health Emergency of International Concern (PHEIC) because it crossed a border, the result was noting that the challenge was still an emergency only for DRC. WHO did note that there were serious funding gaps and support from other countries for the DRC’s predicament. Ironically, such gaps make it more likely that Ebola can spread more widely.
As of 21 June 2019, the DRC reported a total of 2,211 cases since the start of the epidemic last year, of which 2,117 have been confirmed and 94 are probable. There have been 1,489 deaths. To date 139,027 persons have been vaccine with the Merck rVSV-ZEBOV vaccine.
Progress toward Eliminating Malaria – the E-2020 Countries
 The process of eliminating malaria from the world needs to start in a step-by-step fashion. WHO explained that, “Creating a malaria-free world is a bold and important public health and sustainable development goal. It is also the vision of the Global technical strategy for malaria 2016-2030, which calls for the elimination of malaria in at least 10 countries by the year 2020.”
The process of eliminating malaria from the world needs to start in a step-by-step fashion. WHO explained that, “Creating a malaria-free world is a bold and important public health and sustainable development goal. It is also the vision of the Global technical strategy for malaria 2016-2030, which calls for the elimination of malaria in at least 10 countries by the year 2020.”
Actually, WHO identified 21 countries, spanning 5 regions, that could defeat malaria by 2020. The progress report charts the effort. During the recent World Health Assembly two countries received recognition for being certified malaria-free, Argentina and Algeria. This week WHO also announced that 5 more countries have not had malaria cases in the past year. There was also release of a downloadable report on progress toward the 2020 target for selected countries.
Reconsidering Yaws Eradication
In the 1950s and 1960s the world focused on the possibility of eradicating Yaws through screening and treatment interventions. Like the early malaria eradication programs from the same period, the Yaws effort slowed, stopped and experienced a resurgence. The Telegraph reported that, “Between 1952 and 1964, Unicef and the WHO screened some 300 million people for the illness, in a coordinated programme which treated more than 50 million cases. Yaws was on the brink of being wiped out and reports of the disease dropped by 95 per cent.” WHO continues to work on treatment strategies with azithromycin and for resistant cases, benzathine benzylpenicillin injection.
WHO noted that there were 80,472 cases reported in 2018, although this figure is likely to be much higher in actuality. The challenge of case detection exists but may be overcome, according to the Telegraph with a new molecular rapid diagnostic test which detects yaws within 30 minutes, and thus could allow on-the-spot diagnosis in remote regions.
Measles Cases Continue to Increase
The problem of measles in the DRC may not be receiving much attention because of the Ebola epidemic. Ironically, Outbreak News Today reports that, “In a follow-up on the measles outbreak in the Democratic Republic of the Congo (DRC), UN health officials report an additional 7500 suspect cases in the past 2 weeks, bringing the total cases since the beginning of the year to 106,870. The death toll due to the measles outbreak has reached 1815 deaths (case fatality ratio 1.7%).”
Vaccine coverage challenges in the DRC result from health systems weaknesses. Unfortunately, a global study has shown that increasing cases in the Global North are not due to weak systems, but ‘vaccine hesitancy.’ The Guardian reports that a global survey has revealed the scale of the crisis of confidence in vaccines in Europe, “showing that only 59% of people in western Europe and 50% in the east think vaccines are safe, compared with 79% worldwide.” The Guardian observes that, “In spite of good healthcare and education systems, in parts of Europe there is low trust in vaccines. France has the highest levels of distrust, at 33%.”
For more news and daily updates check our other services, a closed/private Facebook Group and a Twitter feed. For those who do not use social media, please check here each weekend to find a summary of some of the stories we have shared during the week.
Capacity Building &Case Management &Funding &Health Systems &IPTp &ITNs &Leadership Bill Brieger | 09 Feb 2019
Guinea: The Challenge of Malaria Control in a Post-Ebola Context
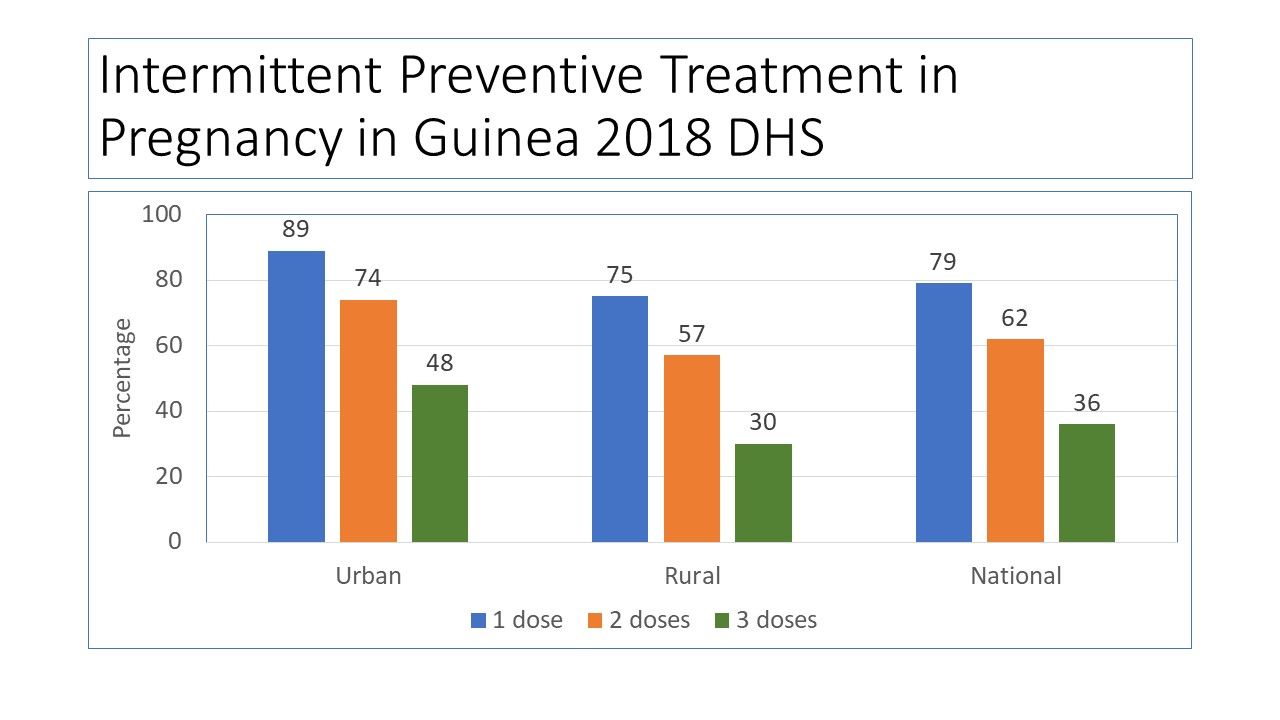
The preliminary 2018 Demographic and Health Survey (DHS) data have been released for Guinea (Conakry). Since the last DHS in 2012, Guinea and its neighbors experienced the largest Ebola outbreak in history, an event that damaged already weak health systems.
 The previous DHS showed very weak malaria indicators. Only 47% of households had at least one ITN, which averages to 0.8 ITNs per person (compared to the universal coverage of 2.0). Among vulnerable groups only 26% of children below the age of 5 years slept under an ITN, as did 28% of pregnant women. Very few, 18%, pregnant women got two doses of IPTp, and only 5% of febrile children received ACTs (testing was not reported then).
The previous DHS showed very weak malaria indicators. Only 47% of households had at least one ITN, which averages to 0.8 ITNs per person (compared to the universal coverage of 2.0). Among vulnerable groups only 26% of children below the age of 5 years slept under an ITN, as did 28% of pregnant women. Very few, 18%, pregnant women got two doses of IPTp, and only 5% of febrile children received ACTs (testing was not reported then).
 Not much has changed concerning ITN coverage as reported in 2018. Slight improvements are seen in IPTp (which now requires 3 or more doses) and malaria testing and treatment for children. Ironically none of the indicators has passed the original 2006 Roll Back Malaria target of 60%, let alone 80% for 2010 and not of course the drive for universal coverage.
Not much has changed concerning ITN coverage as reported in 2018. Slight improvements are seen in IPTp (which now requires 3 or more doses) and malaria testing and treatment for children. Ironically none of the indicators has passed the original 2006 Roll Back Malaria target of 60%, let alone 80% for 2010 and not of course the drive for universal coverage.
 DHS has released a preliminary report for 2018 and the malaria component is summarized in the charts posted here. The national coverage for ITNs is 44%, slightly lower than 2012, but the average per household member is slightly higher at 1.1. Again, these numbers do not mark significant progress. Looking at wealth and ITN ownership there is a slight benefit in terms of equity in net possession among those with lower income, but this must be seen in the overall context of very low basic coverage.
DHS has released a preliminary report for 2018 and the malaria component is summarized in the charts posted here. The national coverage for ITNs is 44%, slightly lower than 2012, but the average per household member is slightly higher at 1.1. Again, these numbers do not mark significant progress. Looking at wealth and ITN ownership there is a slight benefit in terms of equity in net possession among those with lower income, but this must be seen in the overall context of very low basic coverage.
 Having a net in the household and using it are different challenges as seen in the reports of sleeping under the net on the night prior to the survey among children under 5 years of age and pregnant women. The sad finding is that even in households that own a net, the coverage of these two groups remains very low. This is reflected in the low net per person ratio nationally (1.1).
Having a net in the household and using it are different challenges as seen in the reports of sleeping under the net on the night prior to the survey among children under 5 years of age and pregnant women. The sad finding is that even in households that own a net, the coverage of these two groups remains very low. This is reflected in the low net per person ratio nationally (1.1).
 One would almost wonder if malaria is a neglected disease in Guinea. The reality is that since 2003, Guinea has received around $172 million US dollars in malaria project funding from the Global Fund. Its most recent annual funding from the US President’s Malaria Initiative (PMI) is around $14 million. Of that PMI funding 24% was designated for nets and related activities, while 52% was to be spent on medicines, diagnostics and pharmaceutical management. These investments include systems strengthening and capacity building in addition to commodities.
One would almost wonder if malaria is a neglected disease in Guinea. The reality is that since 2003, Guinea has received around $172 million US dollars in malaria project funding from the Global Fund. Its most recent annual funding from the US President’s Malaria Initiative (PMI) is around $14 million. Of that PMI funding 24% was designated for nets and related activities, while 52% was to be spent on medicines, diagnostics and pharmaceutical management. These investments include systems strengthening and capacity building in addition to commodities.
PMI provides the needed context: “Since the country was declared Ebola-free in in June of 2016, Guinea continues to make positive advances towards building a strong health system in line with the health recovery plan. The government continues to mobilize internal and external resources for rolling out the health system recovery plan, but much remains to be done if this plan is to yield the intended results.” Areas in particular need of strengthening within the National Malaria Control Program include coordination, health information systems, leadership, supervision and logistics.
Three years have passed since the last Ebola case in Guinea. Hopefully the country can stave off another outbreak and at the same time strengthen its health system. Guinea may not yet be targeted for malaria elimination, but until systems are strengthened, the resources going into malaria control will not be able to push malaria indicators toward saving more lives.
Burden &Funding &Health Education &Health Systems &Invest in Malaria Control &ITNs &Management Bill Brieger | 19 Nov 2018
Malaria funding may never be enough, but better program management should be possible
 The World Malaria Report shows that malaria cases are up, and even though there are fewer reported cases in 2017 than 2010, the number is greater than 2016. So once again high burden countries are being targeted. Today this focus is on “High Burden to High Impact”, but in 2012-13 it was the “Malaria Situation Room” that also focused on 10 high burden countries.
The World Malaria Report shows that malaria cases are up, and even though there are fewer reported cases in 2017 than 2010, the number is greater than 2016. So once again high burden countries are being targeted. Today this focus is on “High Burden to High Impact”, but in 2012-13 it was the “Malaria Situation Room” that also focused on 10 high burden countries.
Progress was being made up to around 2015-16, it then started to reverse. The challenge was not just funding. As the WHO Director General noted in the foreword to the 2018 World Malaria Report (WMR), “Importantly, ‘High burden to high impact’ calls for increased funding, with an emphasis on domestic funding for malaria, and better targeting of resources. The latter is especially pertinent because many people who could have benefited from malaria interventions missed out because of health system inefficiencies.”
 Over the years there have never been enough pledged funds to fully achieve targets, but as funding has never reached desired levels, attention is now being drawn more and more to the source of that funding (more emphasis on domestic/endemic countries) and especially how the health system functions to use the funds that are made available. In 1998 during one of the early meetings establishing the Roll Back Malaria Partnership, a speaker stressed that malaria control could not succeed without concomitant health systems strengthening and reform. That 20-year-old thought was prescient for today’s dilemma.
Over the years there have never been enough pledged funds to fully achieve targets, but as funding has never reached desired levels, attention is now being drawn more and more to the source of that funding (more emphasis on domestic/endemic countries) and especially how the health system functions to use the funds that are made available. In 1998 during one of the early meetings establishing the Roll Back Malaria Partnership, a speaker stressed that malaria control could not succeed without concomitant health systems strengthening and reform. That 20-year-old thought was prescient for today’s dilemma.
First, what is the funding situation? As outlined in the World Malaria Report …
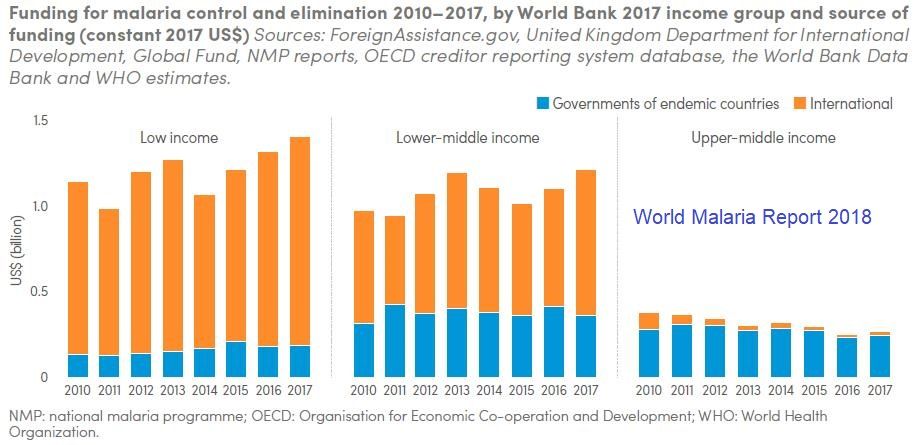
- In 2017, an estimated US$ 3.1 billion was invested in malaria control and elimination efforts globally by governments of malaria endemic countries and international partners – an amount slighter higher than the figure reported for 2016.
- Governments of endemic countries contributed 28% of total funding (US$ 900 million) in 2017, a figure unchanged from 2016.
- Funding for malaria has remained relatively stable since 2010
- To reach the Global Technical Strategy 2030 targets, it is estimated that annual malaria funding will need to increase to at least US$ 6.6 billion per year by 2020
 The question remains – does investment lead to results. The WMR shows, for example, that “Between 2015 and 2017, a total of 624 million insecticide-treated mosquito nets (ITNs/LLINs), were reported by manufacturers as having been delivered globally. This represents a substantial increase over the previous period 2012–2014, when 465 million ITNs were delivered globally”.
The question remains – does investment lead to results. The WMR shows, for example, that “Between 2015 and 2017, a total of 624 million insecticide-treated mosquito nets (ITNs/LLINs), were reported by manufacturers as having been delivered globally. This represents a substantial increase over the previous period 2012–2014, when 465 million ITNs were delivered globally”.
At the same time the report states that, “Households with at least one ITN for every two people doubled to 40% between 2010 and 2017. However, this figure represents only a modest increase over the past 3 years, and remains far from the target of universal coverage.” Is it simply a matter of funding to reach the other 60% of households, or are there serious management problems on the ground?
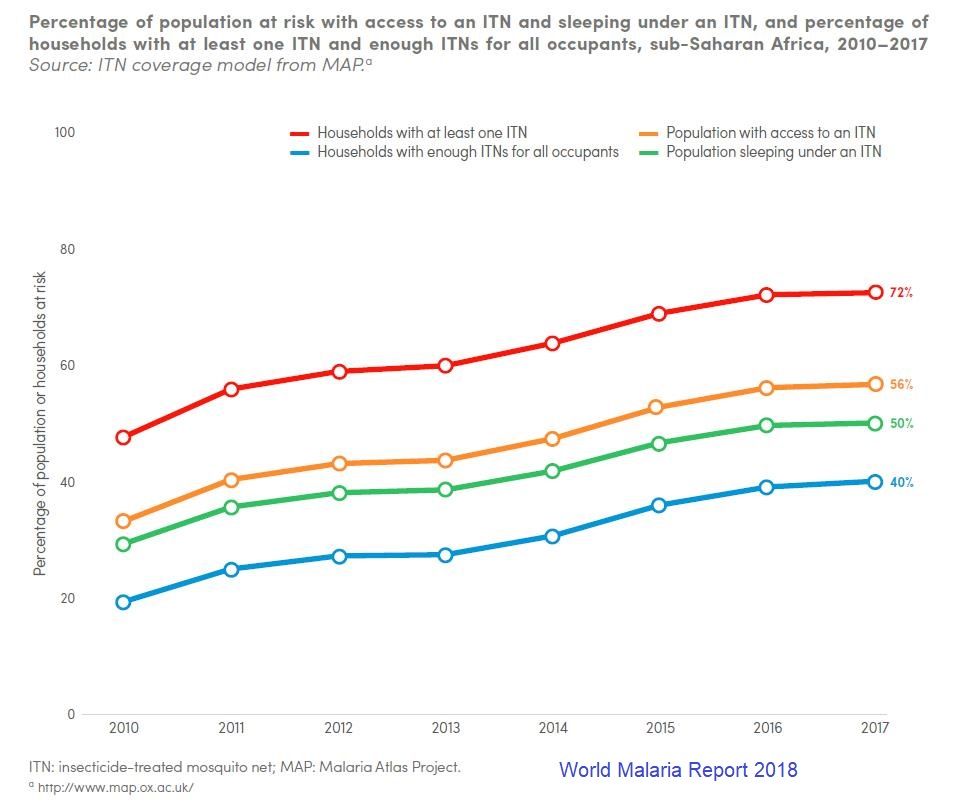 Then there is the issue of using nets. The WMR traces new ownership and use from 2010 to 2017, and we can see that overall the proportion of the population at risk who slept under a net increased from around 30% to 50%, but only 56% of those with access to a net were sleeping under them. This can be attributed in part but not completely to the adequacy of nets in a household.
Then there is the issue of using nets. The WMR traces new ownership and use from 2010 to 2017, and we can see that overall the proportion of the population at risk who slept under a net increased from around 30% to 50%, but only 56% of those with access to a net were sleeping under them. This can be attributed in part but not completely to the adequacy of nets in a household.
We should ask are enough nets getting to the right places, and also are efforts in place to promote their use. Behavior change efforts should be a major component of malaria program management. Even the so called biological challenges to malaria control have a human element. Monkey malaria transmission to people results from deforestation. Malaria parasite resistance to medicines comes from poor drug management on individual and systems levels.
The target year 2030 will be here before we know it. Will malaria still be here, or will countries and donors get serious about malaria financing AND program management?
Health Information &Health Systems &Health Workers &Leadership Bill Brieger | 30 Oct 2018
Assessing Organizational Capacity to Deliver Malaria Services in Rural Liberia
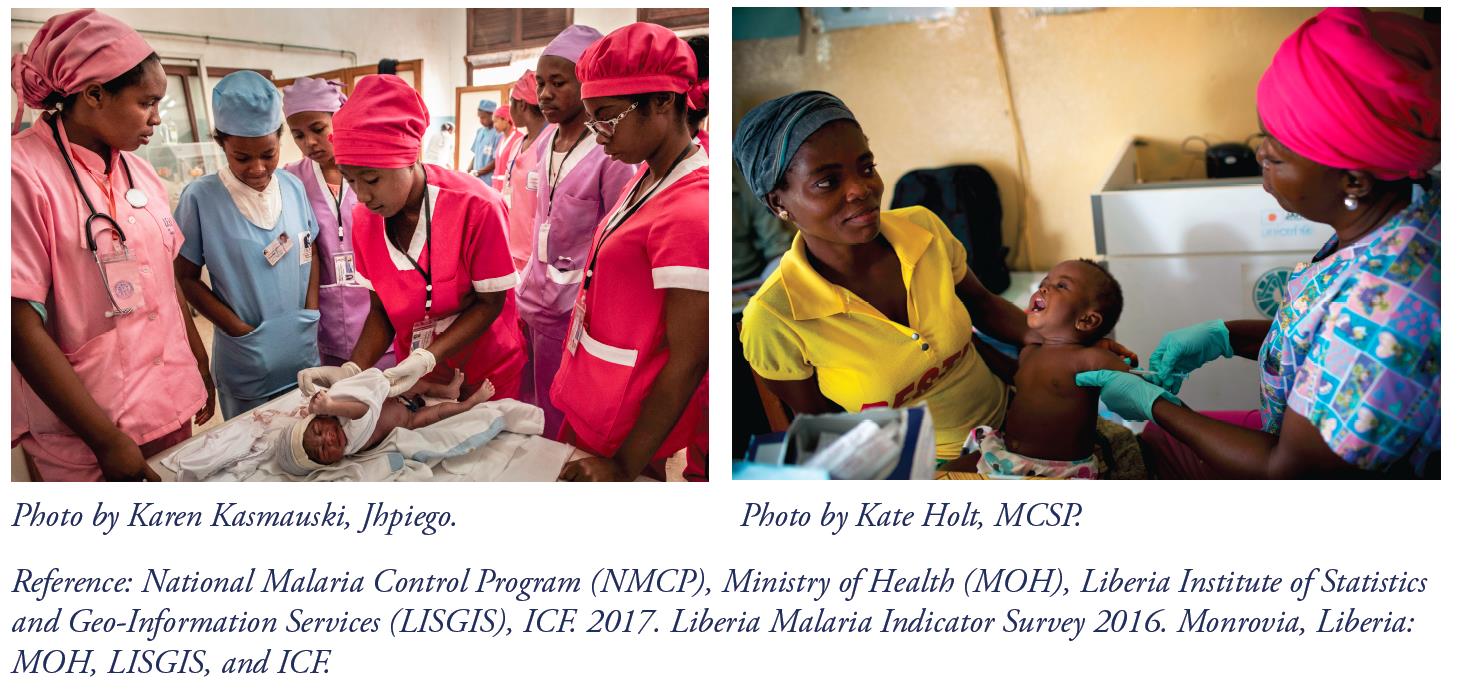
 Swaliho F. Kamara, Wede Tate, Allyson R. Nelson, Lauretta N. Se, Lolade Oseni, Gladys Tetteh of MCSP/Jhpiego are presenting a poster at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene on Malaria Service delivery in rural Liberia. Their findings are shared below:
Swaliho F. Kamara, Wede Tate, Allyson R. Nelson, Lauretta N. Se, Lolade Oseni, Gladys Tetteh of MCSP/Jhpiego are presenting a poster at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene on Malaria Service delivery in rural Liberia. Their findings are shared below:
 In Liberia Malaria prevalence in children under 5 is 45% nationally and higher in rural counties (NMCP et al. 2017). The National Malaria Control Program (NMCP) leads the rollout of malaria prevention and control activities to county health teams (CHTs), per the National Malaria Strategic Plan (2016–2020). A key donor supporting malaria prevention and control, the President’s Malaria Initiative (PMI), has been committed to the Ministry of Health and Social Welfare (MOHSW) strategy since 2008, when it began working in three out of 15 malaria-affected counties. PMI supports CHTs in their management of local health systems and service delivery oversight. As part of an expansion program to five additional rural, neglected, high-burden counties in 2017, the United States Agency for International Development (USAID)/ PMI-funded Maternal and Child Survival Program (MCSP) assessed CHTs’ organizational capacity to identify ways to improve the quality of malaria health services.
In Liberia Malaria prevalence in children under 5 is 45% nationally and higher in rural counties (NMCP et al. 2017). The National Malaria Control Program (NMCP) leads the rollout of malaria prevention and control activities to county health teams (CHTs), per the National Malaria Strategic Plan (2016–2020). A key donor supporting malaria prevention and control, the President’s Malaria Initiative (PMI), has been committed to the Ministry of Health and Social Welfare (MOHSW) strategy since 2008, when it began working in three out of 15 malaria-affected counties. PMI supports CHTs in their management of local health systems and service delivery oversight. As part of an expansion program to five additional rural, neglected, high-burden counties in 2017, the United States Agency for International Development (USAID)/ PMI-funded Maternal and Child Survival Program (MCSP) assessed CHTs’ organizational capacity to identify ways to improve the quality of malaria health services.
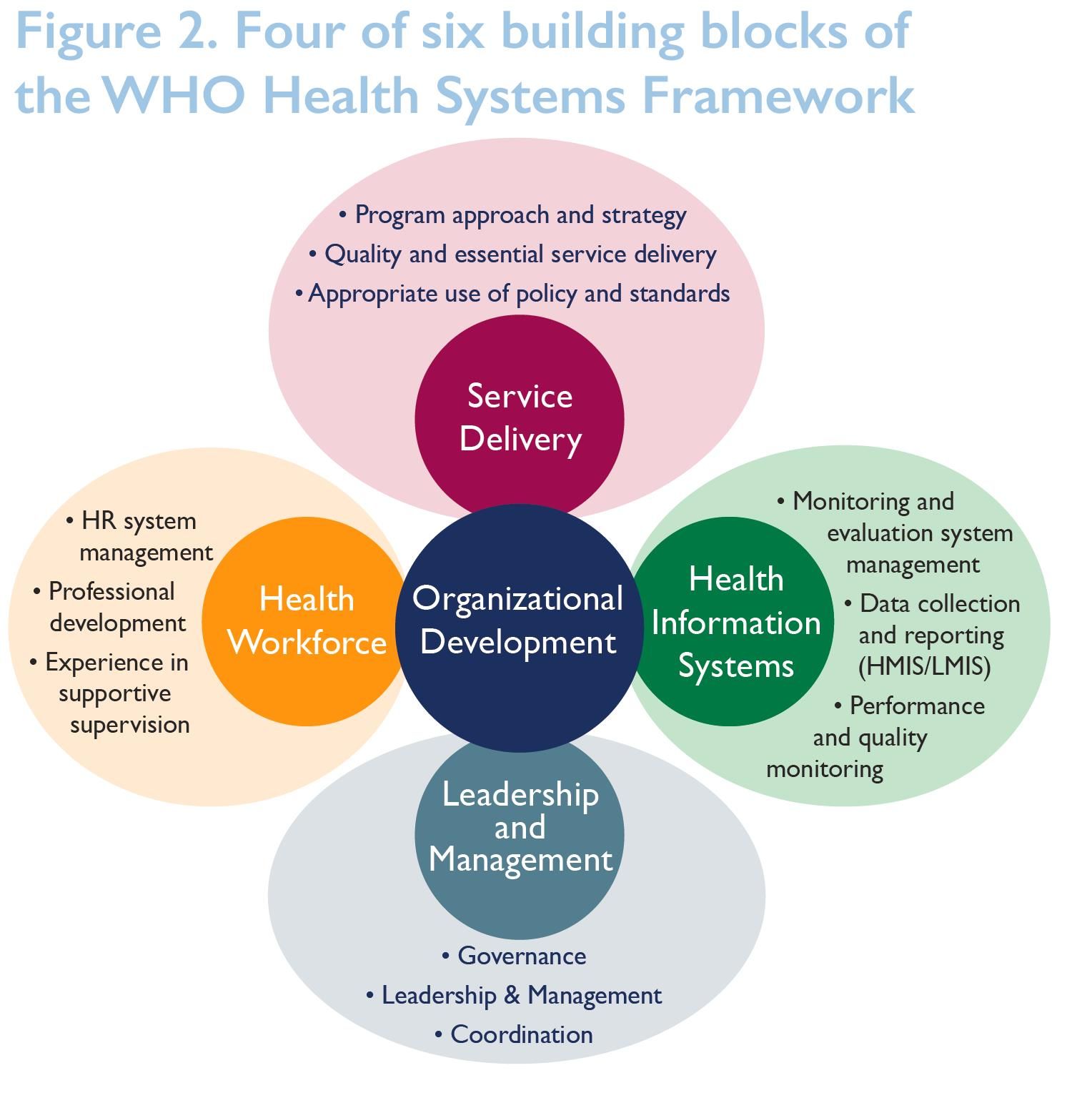 We assessed CHTs’ capacity using a modified organizational capacity assessment (OCA) tool that was used by the USAID’s Rebuilding Basic Health Services (RBHS) project to assess the capacity of the MOHSW, CHTs, and district health teams (DHTs), capturing four of the six World Health Organization (WHO) building blocks of the Health Systems Framework. We also assessed all 30 districts in five counties. Performed desk review, review of self- evaluations, and face- to-face validation interviews. The assessment focused on processes, not physical systems, so the capacity and knowledge of the respondents may have influenced results in some of counties.
We assessed CHTs’ capacity using a modified organizational capacity assessment (OCA) tool that was used by the USAID’s Rebuilding Basic Health Services (RBHS) project to assess the capacity of the MOHSW, CHTs, and district health teams (DHTs), capturing four of the six World Health Organization (WHO) building blocks of the Health Systems Framework. We also assessed all 30 districts in five counties. Performed desk review, review of self- evaluations, and face- to-face validation interviews. The assessment focused on processes, not physical systems, so the capacity and knowledge of the respondents may have influenced results in some of counties.
 Scoring Structure of the OCA Tool: Following each assessment, MCSP used a detailed summary sheet (Figure 3) to display the aggregate scores for each subarea under all key domains, then generated an overall score for each domain. The total score was then expressed as a percentage for each key domain. The majority of the assessment involved asking specific questions about performing malaria interventions per the project scope.
Scoring Structure of the OCA Tool: Following each assessment, MCSP used a detailed summary sheet (Figure 3) to display the aggregate scores for each subarea under all key domains, then generated an overall score for each domain. The total score was then expressed as a percentage for each key domain. The majority of the assessment involved asking specific questions about performing malaria interventions per the project scope.
Effective Interventions were determined:
- Health Workforce Interventions …
- Trained health care workers.
- Trained supervisors on revised supervision tool.
- Performed quarterly supervision and mentoring.
- Leadership and Governance
- Identified a malaria focal point.
- Activated functional health-sector coordination committees.
- Held quarterly review meetings.
- Health Information System
- Provided health management information systems (HMIS) forms to health facilities.
- Facilitated in-service training on onsite data verification.
 Results showed that CHTs’ overall average score was 87% in service delivery, 65% in health information systems, 78% in health workforce, and 70% in leadership/management. Interventions addressing gaps identified in health workforce, leadership and governance, and health information systems resulted in improved service delivery (see Figure 4).
Results showed that CHTs’ overall average score was 87% in service delivery, 65% in health information systems, 78% in health workforce, and 70% in leadership/management. Interventions addressing gaps identified in health workforce, leadership and governance, and health information systems resulted in improved service delivery (see Figure 4).
 In conclusion, The OCA tool helps to identify common challenges, assist with systemwide improvements across CHTs or DHTs, evaluate progress, and meet specific needs. Future efforts are needed to improve the tool’s specificity, the weighting attached to different sections and issues, and its relevance to different types of organizations. Training is an important component to capacity-building, but it is just one part of the picture. Need to improve the way organizations and CHTs/DHTs coordinate with partners to improve all health interventions. Need to focus on application and results of capacity-building, not on capacity as an end in itself.
In conclusion, The OCA tool helps to identify common challenges, assist with systemwide improvements across CHTs or DHTs, evaluate progress, and meet specific needs. Future efforts are needed to improve the tool’s specificity, the weighting attached to different sections and issues, and its relevance to different types of organizations. Training is an important component to capacity-building, but it is just one part of the picture. Need to improve the way organizations and CHTs/DHTs coordinate with partners to improve all health interventions. Need to focus on application and results of capacity-building, not on capacity as an end in itself.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
CHW &Civil Society &Community &Health Systems &Partnership &Primary Health Care Bill Brieger | 28 Oct 2018
Achieving UHC through PHC Requires an Implementation Plan
 The new Astana Declaration says that, “We are convinced that strengthening primary health care (PHC) is the most inclusive, effective and efficient approach to enhance people’s physical and mental health, as well as social well-being, and that PHC is a cornerstone of a sustainable health system for universal health coverage (UHC) and health-related Sustainable Development Goals.” The Declaration outlined a vision, a mission, and a commitment. An opportunity to discuss how to implement this existed at the two-day conference in Astana Kazakhstan celebrating the 40th anniversary of the seminal Alma Ata Declaration.
The new Astana Declaration says that, “We are convinced that strengthening primary health care (PHC) is the most inclusive, effective and efficient approach to enhance people’s physical and mental health, as well as social well-being, and that PHC is a cornerstone of a sustainable health system for universal health coverage (UHC) and health-related Sustainable Development Goals.” The Declaration outlined a vision, a mission, and a commitment. An opportunity to discuss how to implement this existed at the two-day conference in Astana Kazakhstan celebrating the 40th anniversary of the seminal Alma Ata Declaration.
Ironically the opportunity was not fully grasped. There were many sessions that shared country experiences ranging from finance to information technology. Youth who will carry PHC forward for the next 40 years gave their opinions and thoughts. Lip-service as well as actual case examples of community involvement were featured. What we did not hear much of was the specifics of how countries, moving forward, will actually implement the commitments spelled out in the document.
 One colleague who has worked with the sponsoring agencies was of the view that since much advanced input and work from many partners and countries had gone into the new Declaration, which was already nicely printed, they were reluctant to provide the slightest chance that debate would be reopened.
One colleague who has worked with the sponsoring agencies was of the view that since much advanced input and work from many partners and countries had gone into the new Declaration, which was already nicely printed, they were reluctant to provide the slightest chance that debate would be reopened.
As they say, fair enough (maybe), but even if one takes the Declaration as a done deal, the matter if implementation needs to be addressed. There was ample criticism that the Alma Ata Declaration was not properly implemented. This was in part because academics and development agencies jumped the gun and pushed, with focused financial backing, what would be called selective primary health care that was more agency driven, not community directed as envisioned at Alma Ata (now Almaty) in 1978.
In order not to repeat those mistakes and give full voice to the community and key constituents, at minimum the implementation strategies of the pre-agreed Declaration should have been discussed in specific terms. Sure many ideas and examples were aired, but there was no attempt to focus these into workable strategies.
 But was the community even there in Astana to take part in strategizing? One community health worker from Liberia received much attention because she was the odd one out. Sure, there were plenty of NGOs, but not the real grassroots of civil society, although the youth involvement aspect of the conference approached that. Some of these NGOs and agencies had themselves been part of the selective PHC agenda.
But was the community even there in Astana to take part in strategizing? One community health worker from Liberia received much attention because she was the odd one out. Sure, there were plenty of NGOs, but not the real grassroots of civil society, although the youth involvement aspect of the conference approached that. Some of these NGOs and agencies had themselves been part of the selective PHC agenda.
There was plenty of talk about us involving them, especially when it came to community health workers (CHWs). CHWs should first be integrated into community systems to ensure they are accountable to communities. Then there should be an equal partnership between community systems and health systems. Otherwise CHWs get lost as just front line laborers.
Of course it is never too late. Regional gatherings may be a better forum that can discuss implementation in a more socially, economically and culturally appropriate way. Let’s hope we don’t look back in another 40 years and with the Astana Declaration had been better and more faithfully implemented.
Health Systems &IPTp &Malaria in Pregnancy &Neonatal &Procurement Supply Management Bill Brieger | 03 Jul 2018
Progress on Malaria in Pregnancy in 12 PMI Focus Countries
The challenges of implementing programs to control malaria in pregnancy based on experiences with US President’s Malaria Initiative Countries was presented at the Malaria World Congress in Melbourne this week. The team included Katherine Wolf, MCSP/Jhpiego, Marianne Henry, PMI/USAID, Lia Florey, PMI/USAID, Gabrielle Conecker, MCSP/Jhpiego, Betsy Hendrickson, MCSP/Jhpiego, Katherine Lilly, MCSP/Jhpiego, Nicholas
Furtado, GFATM, Maria Petro, GFATM, Susan Youll, PMI/USAID, and Julie Gutman, PMI/CDC, and their findings are shared below.
 What is the danger of malaria in pregnancy (MiP)? Each year MIP is responsible for 20% of stillbirths in Sub-Saharan Africa, 100,000 Newborn deaths globally, 11% of newborn deaths in Africa and 10,000 maternal deaths globally. Four interventions are aimed at MIP, Intermittent Preventive Treatment in Pregnancy (IPTp), consistent use of insecticide treated nets, effective diagnosis and treatment and low-dose folic acid during antenatal care. IPTp with sulfadoxine-pyrimethamine reduces low birth weight by 29%, severe maternal anemia by 38% and neonatal mortality by 31%. What can be done?
What is the danger of malaria in pregnancy (MiP)? Each year MIP is responsible for 20% of stillbirths in Sub-Saharan Africa, 100,000 Newborn deaths globally, 11% of newborn deaths in Africa and 10,000 maternal deaths globally. Four interventions are aimed at MIP, Intermittent Preventive Treatment in Pregnancy (IPTp), consistent use of insecticide treated nets, effective diagnosis and treatment and low-dose folic acid during antenatal care. IPTp with sulfadoxine-pyrimethamine reduces low birth weight by 29%, severe maternal anemia by 38% and neonatal mortality by 31%. What can be done?
- Scale-up and full coverage of the WHO lifesaving interventions
- Promote early and regular ANC
- Preserve SP efficacy by avoiding its use for treating clinical cases of malaria
- Reserve SP stocks for IPTp at ANC clinics
 Methodology for MiP country review: Initial survey took place in 23 PMI countries. PMI resident advisors were surveyed, Qualitative and quantitative responses were collected and Input from NMCP/partners was obtained. Country selection resulted in 12 that were Tiptop-implementing countries, represented Geographic diversity, had varied IPTp coverage, and made clear progress or best practices to share.
Methodology for MiP country review: Initial survey took place in 23 PMI countries. PMI resident advisors were surveyed, Qualitative and quantitative responses were collected and Input from NMCP/partners was obtained. Country selection resulted in 12 that were Tiptop-implementing countries, represented Geographic diversity, had varied IPTp coverage, and made clear progress or best practices to share.
Desk review including HMIS and house hold survey data, current studies and recent assessments, Selected interviews with PMI resident advisors, Jhpiego field staff and current/former NMCP staff. Analysis was a Review and clarification of qualitative and qualitative data.
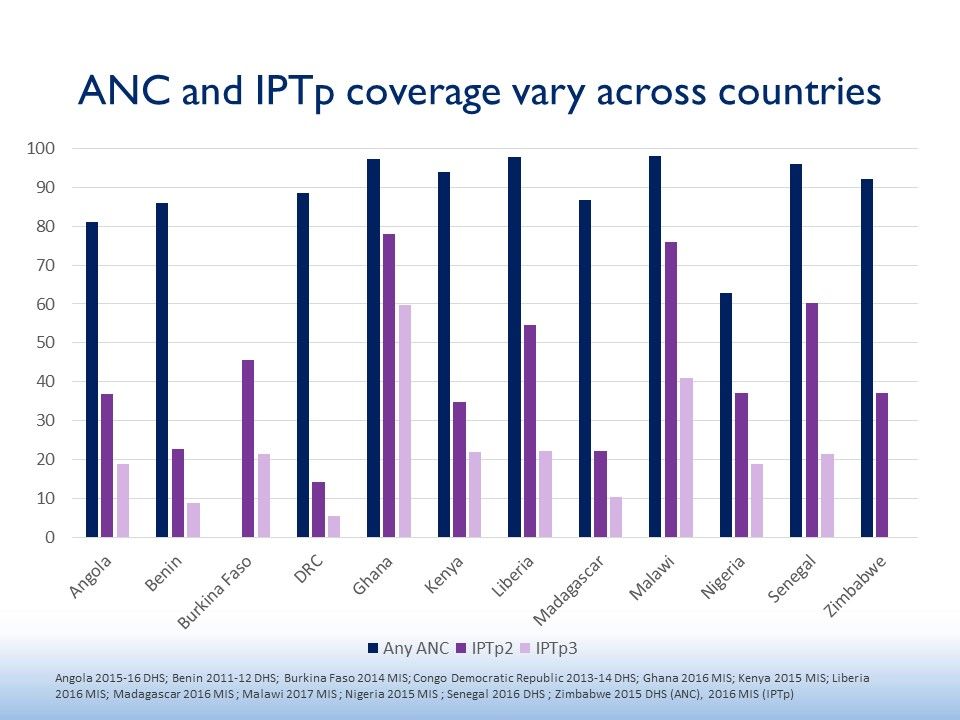
 The 12 countries included Angola, Benin, Burkina Faso, DRC, Ghana, Kenya, Liberia, Madagascar, Malawi, Nigeria, Senegal, and Zimbabwe (see map). The figure shows that none of these attained 80% of 2 doses of IPTp. The current recommendations are for monthly dosages from the 13th week of pregnancy. Often less that half of those receiving IPTp2 also got IPTp3.
The 12 countries included Angola, Benin, Burkina Faso, DRC, Ghana, Kenya, Liberia, Madagascar, Malawi, Nigeria, Senegal, and Zimbabwe (see map). The figure shows that none of these attained 80% of 2 doses of IPTp. The current recommendations are for monthly dosages from the 13th week of pregnancy. Often less that half of those receiving IPTp2 also got IPTp3.
Several health systems findings helped explain the IPT results. For Policy & Implementation, Countries reporting strong, coordinated leadership delivered
high IPTp coverage. With Community Engagement, countries reported a diversity of approaches to community health promotion and service delivery.
Concerning Service Delivery, Many countries struggle to implement MiP policies consistently and with quality in the private sector. Commodities were a challenge. Some countries continue to struggle with SP stockouts at facility level, whether ongoing or episodic. Monitoring and Evaluation processes need to catch up. Countries’ routine information systems are transitioning from tracking IPTp2 to IPTp3.
The team offered several Recommendations.
- Strengthen consistency of IPTp policies across malaria and reproductive health programs
- Scale up of evidence-based country appropriate
community engagement strategies - Alleviation of supply chain bottlenecks at peripheral level
- Inclusion and harmonization of key MIP indicators in routine information systems
For more information please visit www.mcsprogram.org, facebook.com/MCSPglobal and twitter.com/MCSPglobal
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative AgreementAID-OAA-A-14-00028. The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government.
Diagnosis &Health Systems &IPTp &ITNs &Universal Coverage Bill Brieger | 31 Mar 2018
Universal Health Coverage – Where is Malaria?
 Universal Health Coverage (UHC) is the theme of the 2018 World Health Day on April 7th. The concept was applied to malaria in 2009 regarding the provision of long lasting insecticide-treated nets (LLINs aka ITNs) with the definition of universal meaning one net for every two persons in a household. Up until that time coverage targets for malaria interventions set at the 2000 Abuja Declaration had focused on achieving by the year 2010, 80% of people (particularly pregnant women and children below the age of 5 years) sleeping under ITNs, 80% of children receiving appropriate malaria treatment with artemisinin-based combination therapy (ACTs) within 24 hours of onset of illness and 80% of pregnant women receiving two doses of Intermittent Preventive Treatment (IPTp) for malaria as part of antenatal care (ANC).
Universal Health Coverage (UHC) is the theme of the 2018 World Health Day on April 7th. The concept was applied to malaria in 2009 regarding the provision of long lasting insecticide-treated nets (LLINs aka ITNs) with the definition of universal meaning one net for every two persons in a household. Up until that time coverage targets for malaria interventions set at the 2000 Abuja Declaration had focused on achieving by the year 2010, 80% of people (particularly pregnant women and children below the age of 5 years) sleeping under ITNs, 80% of children receiving appropriate malaria treatment with artemisinin-based combination therapy (ACTs) within 24 hours of onset of illness and 80% of pregnant women receiving two doses of Intermittent Preventive Treatment (IPTp) for malaria as part of antenatal care (ANC).
 Definitions have evolved since the Abuja Declaration. The target for ITNs was extended to all household members (thus universal). The ACT target was modified to require treatment based on parasitological testing (microscopy or rapid diagnostic tests). IPTp targets were extended to achieving monthly dosing from the 13th week of pregnancy, which depending on the point in pregnancy when a women entered the ANC system could be 3, 4 or more doses. In addition to these changes, the US President’s malaria Initiative upped the Abuja targets from 80% to 85% in the countries where it supported national malaria programs.
Definitions have evolved since the Abuja Declaration. The target for ITNs was extended to all household members (thus universal). The ACT target was modified to require treatment based on parasitological testing (microscopy or rapid diagnostic tests). IPTp targets were extended to achieving monthly dosing from the 13th week of pregnancy, which depending on the point in pregnancy when a women entered the ANC system could be 3, 4 or more doses. In addition to these changes, the US President’s malaria Initiative upped the Abuja targets from 80% to 85% in the countries where it supported national malaria programs.
We are eight years past 2010. It had been assumed that if scale up to 80% had been achieved by then and sustained for five or more years, malaria deaths would come close to zero and elimination of the disease would be in sight. National surveys have shown that reaching these targets has not been simple.
 The example of ITNs is a good place to start, as is Nigeria with the highest burden of malaria. The attached chart shows findings from the Demographic and Health or Malaria Information Surveys in 2010, 2013 and 2015. Whether one measures universal coverage by the house possessing at least one net per two residents or by the proportion who actually use/sleep under the nets, we can see that UHC for this intervention is difficult to achieve. Even when households possess nets, not everyone sleeps under them either because of adequacy of nets, preferred sleeping arrangements, internal household power structure or other factors.
The example of ITNs is a good place to start, as is Nigeria with the highest burden of malaria. The attached chart shows findings from the Demographic and Health or Malaria Information Surveys in 2010, 2013 and 2015. Whether one measures universal coverage by the house possessing at least one net per two residents or by the proportion who actually use/sleep under the nets, we can see that UHC for this intervention is difficult to achieve. Even when households possess nets, not everyone sleeps under them either because of adequacy of nets, preferred sleeping arrangements, internal household power structure or other factors.
In 2015 the majority of nets that existed in households were obtained through campaigns (77%), 14% were acquired from the health services, and 7% were purchased. These systems are not keeping up with the need.
 Four endemic countries reported a malaria Information Survey in 2016, Liberia, Ghana, Madagascar, and Sierra Leone. The chart shows that they too have had difficulty in achieving universal coverage of malaria interventions. Of note the chart only includes whether appropriate malaria parasitological diagnosis was done on children who had fever in the preceding two weeks. Data on provision of ACTs is based on fever, not test results, so there is no way to know whether it was appropriate. Generally 20-30% more febrile children received ACTs than were tested.
Four endemic countries reported a malaria Information Survey in 2016, Liberia, Ghana, Madagascar, and Sierra Leone. The chart shows that they too have had difficulty in achieving universal coverage of malaria interventions. Of note the chart only includes whether appropriate malaria parasitological diagnosis was done on children who had fever in the preceding two weeks. Data on provision of ACTs is based on fever, not test results, so there is no way to know whether it was appropriate. Generally 20-30% more febrile children received ACTs than were tested.
 All three malaria interventions, ACTs, Diagnostics and ITNs, require contact with the health system (including community health workers). If malaria services are indicative of other health interventions, then universal coverage including seeking interventions, getting them and ultimately using them is still a distant goal. To achieve universal coverage there also needs to be universal commitment by countries, donors and technical partners.
All three malaria interventions, ACTs, Diagnostics and ITNs, require contact with the health system (including community health workers). If malaria services are indicative of other health interventions, then universal coverage including seeking interventions, getting them and ultimately using them is still a distant goal. To achieve universal coverage there also needs to be universal commitment by countries, donors and technical partners.
Education &Health Systems &Primary Health Care &Social/Cultural &Training Bill Brieger | 15 Mar 2018
New Fully Online Global Health Learning Programs at JHU
Continuing professional development has often been a challenge for people in the field.  They may not be able to get study leave, but they do need advanced training in order to progress. The Johns Hopkins Bloomberg School of Public Health as started a new Online Programs for Applied Learning (OPAL) that offers completely online Masters and Certificate degrees.
They may not be able to get study leave, but they do need advanced training in order to progress. The Johns Hopkins Bloomberg School of Public Health as started a new Online Programs for Applied Learning (OPAL) that offers completely online Masters and Certificate degrees.
The Department of International Health is Offering three Master of Applied Learning (MAS) and one Certificate covering global health. The Certificate can be completed in one year minimum and the MAS in two years minimum. More information on these programs can be obtained at the links below.
- Request information for fully online Master of Applied Science in Community-based Primary Health Care Programs in Global Health
 Also get information for fully online Master of Applied Science in Master of Applied Science in Global Health Planning and Management
Also get information for fully online Master of Applied Science in Master of Applied Science in Global Health Planning and Management- Learn more about fully online Certificate in Global Health Practice, a stand alone or first year for our 2 Global Health Masters of Applied Science
- Master of Applied Science in Humanitarian Health

Health Systems &Quality of Services Bill Brieger | 08 Nov 2017
Enhancing Core Competencies & Improving Midwifery Quality of Care in Lake Zone, Tanzania
 With support from USAID’s Maternal and Child Survival Project in Tanzania Annamagreth Mukwenda, John George George, Mary Rose Giatas, Agrey Mbilinyi, Gustav Moyo, and Justine Ngenda have been addressing the quality of case and services provided by midwives. Their poster at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene is summarized below.
With support from USAID’s Maternal and Child Survival Project in Tanzania Annamagreth Mukwenda, John George George, Mary Rose Giatas, Agrey Mbilinyi, Gustav Moyo, and Justine Ngenda have been addressing the quality of case and services provided by midwives. Their poster at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene is summarized below.
 In sub-Saharan Africa, maternal mortality is unacceptably high accounting for 56% of all maternal deaths. Tanzania is not different. It is estimated that five in every 100 children die before their first birthdays and that four women out of 1000 live births die due to pregnancy related causes.
In sub-Saharan Africa, maternal mortality is unacceptably high accounting for 56% of all maternal deaths. Tanzania is not different. It is estimated that five in every 100 children die before their first birthdays and that four women out of 1000 live births die due to pregnancy related causes.
With prompt recognition and timely intervention most maternal and neonatal deaths can be avoided. Access to skilled care at these critical times save lives.
 A new initiative is working to improve midwifery care by building capacity of training institutions to prepare highly skilled nurse-midwives to enhance on job live saving skills.
A new initiative is working to improve midwifery care by building capacity of training institutions to prepare highly skilled nurse-midwives to enhance on job live saving skills.
In 2014 A collaboration between the Tanzania Ministry of Health, Jhpiego through Maternal child survival program (MCSP), conducted a baseline assessment to assess the quality of midwifery pre-service education to adequately prepare students with the clinical skills to provide competent nursing and midwifery care.
Four nursing and midwifery schools from two regions of Lake Zone were assessed to identify issues affecting the schools’ ability to produce clinically competent graduates in nursing and midwifery. Among things, the assessment focused on tutors and recent graduates, with findings showing critical deficit on content/skill competencies.
 To address these challenges, midwifery tutors from 9 schools (100%) were updated in high impact midwifery interventions through trainings and supportive supervision including coaching and mentorship. Skills labs were also equipped with all mannequins necessary for midwifery training.
To address these challenges, midwifery tutors from 9 schools (100%) were updated in high impact midwifery interventions through trainings and supportive supervision including coaching and mentorship. Skills labs were also equipped with all mannequins necessary for midwifery training.
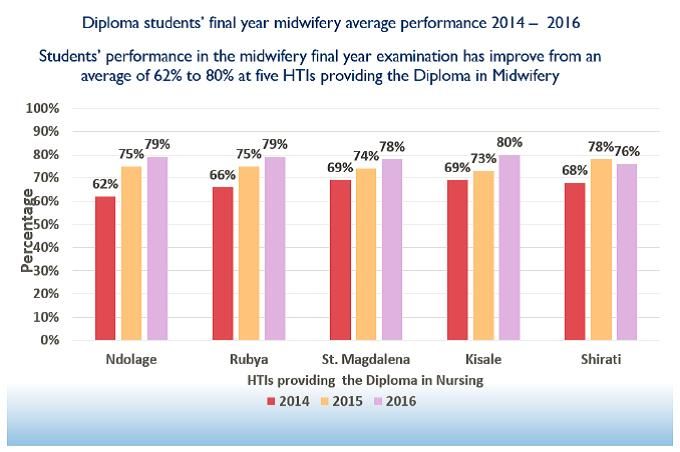
The program is in the third year of implementation with tremendous improvement in midwifery training as evidenced by students final examination results as well as tutors’ and students’ testimonies.
Experience of MCSP approach to strengthen competencies of graduates has contributed to improve midwifery quality of care to reduce maternal deaths in Tanzania.