Advocacy &Elimination &Women Bill Brieger | 07 Mar 2015
Association of Women Doctors of Senegal joins the “Zero Malaria! Count Me In!” campaign to eliminate malaria in Senegal
Yacine Djibo, Founder & President of Speak Up Africa is helping focus International Women’s Day (March 8th) on efforts to protect women from malaria in Senegal. She is highlighting the commitments of 8 strong and beautiful women, in Senegal, that are dedicated to eliminating malaria in their country. These commitments are part of an inclusive mass communication campaign that aims to launch a national movement in favor of malaria elimination in Senegal: the “Zero Malaria! Count Me In” campaign
International Women’s Day, represents an opportunity to celebrate the achievements of women all around the world. This year’s theme is “Empowering Women – Empowering Humanity: Picture it” envisions a world where each woman and girl can exercise her choices, such as participating in politics, getting an education or fighting malaria. Below is the first feature on women fighting malaria.

Amy Niambo Ndao Fall, President of the Association of Women Doctors
Dr. Amy Ndao Fall is the President of the Association of Women Doctors of Senegal (AFEMS). This Association, composed of 400 members across the country, aims to undertake sustainable activities for the health of the Senegalese populations.
On the eve of Women International Day, in partnership with the Ministry of health and UN women, AFEMS organized in Dakar on March 7, a conference on the theme “women’s health for an emergent Senegal”.
This conference attracted approximately 150 women from all over the country and was chaired by Professor Awa Marie Coll Seck, Minister of Health and Social Action of Senegal.
The conference started with Dr. Ndao signing a pledge, on behalf of AFEMS to support the “Zero Malaria, Count me In” campaign and the National Malaria Control Program in their elimination efforts.
Dr. Ndao stated the association’s commitment to support all efforts toward malaria elimination in Senegal and abroad and concluded with the following words:
 “It is a pleasure and an honour for me, to sign this engagement on behalf of AFEMS, to mobilize all our efforts to eliminate malaria in Senegal. We need to keep in mind that women are particularly vulnerable to this disease and that they can be change agents in their families for more efficient vector control in particular by promoting the systematic use of long lasting insecticide-treated mosquito nets for all their family members.”
“It is a pleasure and an honour for me, to sign this engagement on behalf of AFEMS, to mobilize all our efforts to eliminate malaria in Senegal. We need to keep in mind that women are particularly vulnerable to this disease and that they can be change agents in their families for more efficient vector control in particular by promoting the systematic use of long lasting insecticide-treated mosquito nets for all their family members.”
On this International Women Day, we celebrate and thank Dr. Ndao and all the women Doctors of Senegal for their leadership and commitment to eliminate malaria and are proud to see such amazing partners joining efforts to make Zero Malaria a reality in Senegal.
*****
Headquartered in Dakar, Senegal, Speak Up Africa is a creative health communications and advocacy organization dedicated to catalyzing African leadership, enabling policy change, securing resources and inspiring individual action for the most pressing issue affecting Africa’s future: child health.
Elimination Bill Brieger | 07 Mar 2015
A new working group to support malaria elimination in the Amazon region
DR Antonio Quispe

In February 2014, the Malaria Elimination Working Group (MEWoG), in partnership with the Peruvian Ministry of Health (MoH), hosted its first international conference on malaria elimination in Iquitos, Peru. The two-day meeting gathered 85 malaria experts, including 18 international panelists, 23 stakeholders from different malaria endemic regions of Peru, and 11 MoH authorities.
Several key conclusions and points of consensus arose from this meeting. The most important one is that malaria elimination in the Peruvian Amazon is an achievable and nationally and internationally important goal. It will be important to develop a Comprehensive Regional Strategic Plan, which must satisfy several key characteristics.
It was strongly recommended to first, pilot such strategy in suitable sites in the region to establish efficacy and acceptability.
As such strategy is implemented, it will be important to monitor and evaluate progress through a variety of metrics and to set intermediate goals on the path to regional elimination. Targeted parasite elimination strategies that are appropriate to the region must be used, stressing active case detection using sufficiently sensitive and effective RDTs and species-specific treatment of the asymptomatic reservoir.
This is particularly important in the case P. falciparum malaria, which must be treated with ACT and primaquine to interrupt transmission. The strategy must include and facilitate communication between key stakeholders from the region and political support at all levels of government, and the program should be incorporated into established health systems to improve acceptability and sustainability.
The progression of such strategy should be flexible to allow new knowledge of the social determinants of malaria, the cultural acceptability of key interventions, and novel tests and treatments to be incorporated throughout the effort. With this conference, an agreement on the relevance of pursuing malaria elimination as goal has been reached, and the necessary components characteristics of this effort described.
Moving forward, further detail should be elaborated as commitments from numerous key stakeholders are obtained.
(see more on malaria elimination in the Americas – PAHO)
Asia &Elimination Bill Brieger | 03 Sep 2014
Press Release: Bangladesh joins APMEN as new Country Partner
Bangladesh joins the Asia Pacific Malaria Elimination Network (APMEN) as Country Partner
 The Asia Pacific Malaria Elimination Network (APMEN) is pleased to announce Bangladesh as the 16th Country Partner to join the Network.
The Asia Pacific Malaria Elimination Network (APMEN) is pleased to announce Bangladesh as the 16th Country Partner to join the Network.
APMEN brings together countries in the Asia Pacific region that have adopted a national or sub-national goal for malaria elimination, and connects them with a broad range of regional and global malaria partners to develop best practices for eliminating the disease. By strengthening linkages in eliminating countries, APMEN addresses important regional challenges such as Plasmodium vivax, and provides a forum for the discussion of important issues such as the spread of anti-malarial drug resistance.
Malaria remains endemic in 13 of the 64 districts in Bangladesh, and more than 13 million1 people are still at risk of the disease. Malaria control and elimination activities fall under the National Malaria Control Program (NMCP) of the Ministry of Health and Family Welfare. The NMCP is currently aiming for malaria pre-elimination in four districts, with the goal of Bangladesh becoming malaria-free by 2020.
Director of Disease Control in Bangladesh and Public Health and Infectious Disease Specialist, Professor Be-Nazir Ahmed, expressed his gratitude towards APMEN at the formalization of this important partnership, saying that it is another step forward for Bangladesh and the region to eliminate the disease.

The spatial distribution of Plasmodium falciparum malaria endemicity map in 2010 in Bangladesh – http://www.map.ox.ac.uk/browse-resources/endemicity/Pf_mean/BGD/
“Bangladesh is moving very quickly towards elimination after concerted national efforts to focus on malaria control,” Professor Be-Nazir said.
“By joining APMEN, Bangladesh now has many windows of opportunities to learn from other eliminating countries in our region as we face similar challenges.”
According to the World Health Organization, Bangladesh has reduced the number of confirmed malaria cases from nearly 440,000 in 2000 to less than 30,000 in 2012; a 93% overall decline2. The success is a result of intensive control interventions such as high coverage and increased use of insecticide-treated nets, increased use of rapid diagnostic tests and effective antimalarial treatment, as well as the deployment of a high number of community health workers in collaboration with NGOs and augmenting services at the health facilities. The combination of technical and human resource capacity serves as a strong example of how national and international efforts can lead to reduced malaria transmission3.
Bangladesh, like many other APMEN Country Partners, face many challenges en route to its national elimination goal of 2020, namely ensuring services reach mobile populations in highly endemic districts such as the Jhum cultivators4, and sustaining commitment by the government, communities and development partners to malaria control and elimination.
Malaria was nearly eliminated from Bangladesh pre-1970, but never disappeared in the eastern border regions which are associated with tea gardens and forests. These districts have international boundaries with the eastern states of India and partly with Myanmar. In the 1990s, malaria re-emerged as a major public health concern.
A key Bangladesh public health organization, the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b), joined APMEN as a Partner Institution in August 2013.
APMEN Joint Secretariat (UQ) Office, School of Population Health | Room 117 | Public Health Building, Herston Road | Herston Qld 4006| Australia, Email: apmen@sph.uq.edu.au | Website: www.apmen.org | Phone (within Australia): 07 3365 5446 | Phone (from outside Australia): 61 7 3365 5446
Elimination &Eradication Bill Brieger | 16 Jun 2014
Guinea Worm, Inching Toward Eradication
Twenty-eight years ago efforts to eradicate guinea worm began in earnest. It was the UN Water Decade, and there was optimism that guinea worm could be the test case for success of the global effort to guarantee adequate and safe water for all.
 As can be seen in the CDC infographic, we have gone from 3.5 million cases to 148 during this time. As we reach toward the tail end of the worm, we find some challenges remain.
As can be seen in the CDC infographic, we have gone from 3.5 million cases to 148 during this time. As we reach toward the tail end of the worm, we find some challenges remain.
On the list of currently endemic countries one finds Chad. Chad was supposed to be in the pre-certification phase, but new cases appeared a few years ago.
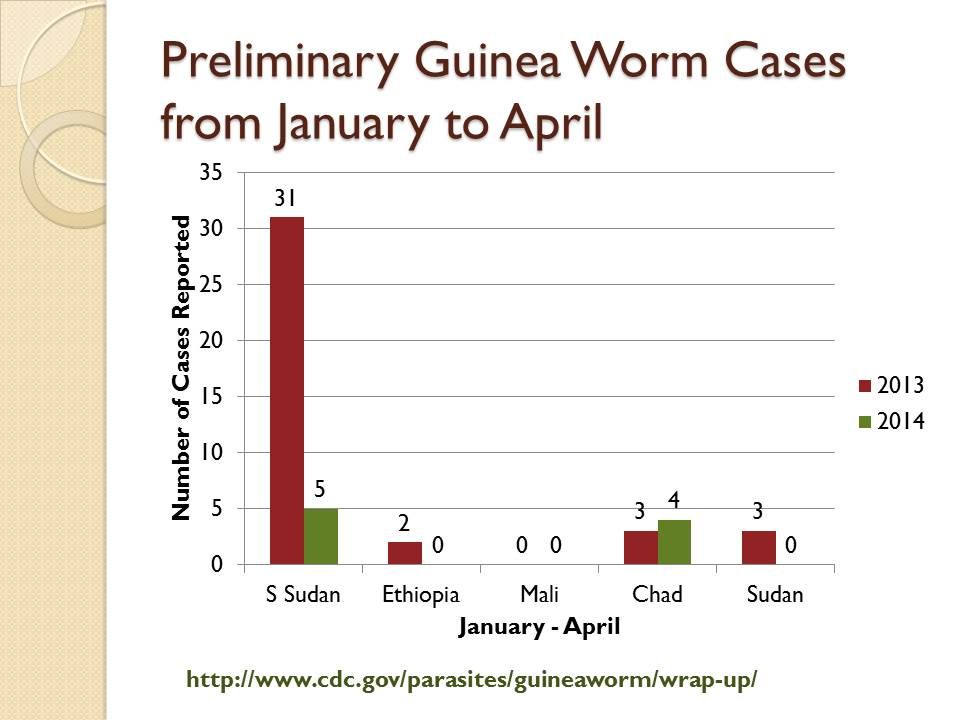
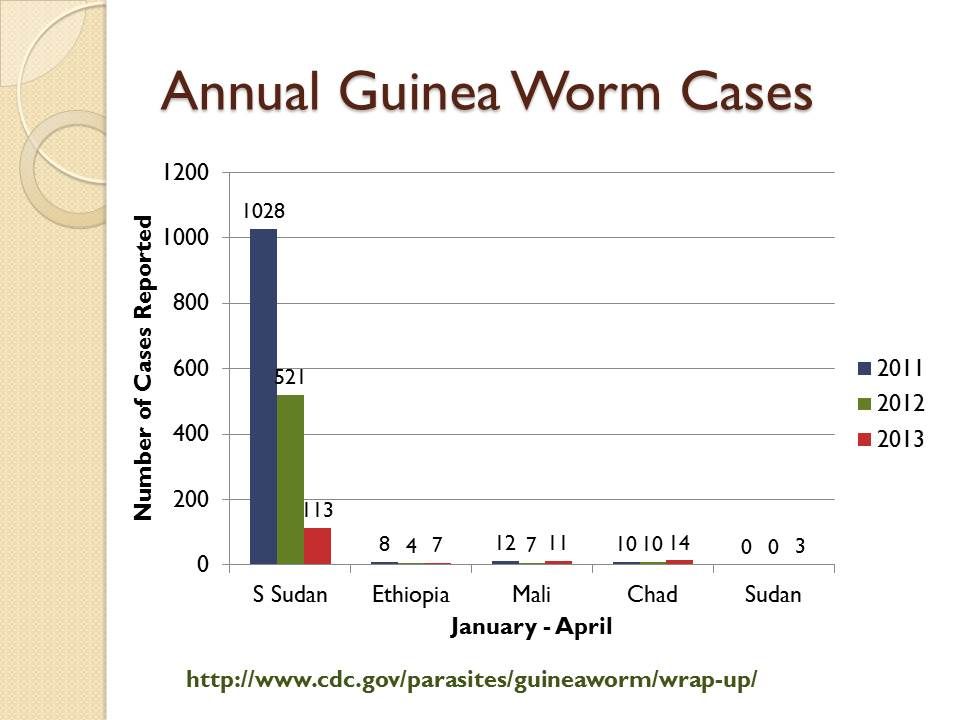 Sudan was the most highly endemic country until South Sudan gained independence and took the guinea worm cases with it. Recently a few cases have also appeared again in the Sudan itself seen in charts derived from CDC’s newsletter, Guinea Worm Wrap-Up.
Sudan was the most highly endemic country until South Sudan gained independence and took the guinea worm cases with it. Recently a few cases have also appeared again in the Sudan itself seen in charts derived from CDC’s newsletter, Guinea Worm Wrap-Up.
Looking at the most recent data from early 2014, one can see that Mali is back to reporting no cases as have Ethiopia and Sudan for 2014. Caution is needed since transmission is more likely in the upcoming rainy season months than in the current dry period.
 What is common in these areas is either being in a state of conflict or bordering a conflict zone. This makes efforts to detect cases and put interventions in place in a timely manner to prevent the next season’s transmission very difficult.
What is common in these areas is either being in a state of conflict or bordering a conflict zone. This makes efforts to detect cases and put interventions in place in a timely manner to prevent the next season’s transmission very difficult.
Unlike some other diseases, guinea worm has some relatively simple, epidemiologically appropriate and less expensive interventions like cloth water filters, abate/temephos for water source treatment and case containment. Of course investments in improved water supplies will also solve the problem. But without easy access to the communities where transmission is occurring, the disease will persist at this incredibly low level.
Other disease elimination programs are equally affected by the problems of access and conflict, polio being a good example. We know that malaria is also exacerbated in conflict situations, but in the locations where pre-elimination is near, like Swaziland, Botswana, South Africa and Namibia, the main concern is ensuring a strong health system to handle the additional surveillance tasks. Still we should not be complacent, because malaria is also endemic in these very sites where guinea worm stubbornly lingers.
Elimination &Research Bill Brieger | 30 May 2014
New operational research projects in malaria elimination
 Kate Whitfield is sharing with us the following information about MESA‘s operational research …
Kate Whitfield is sharing with us the following information about MESA‘s operational research …
New operational research projects in malaria elimination started in April 2014, after being selected for funding through MESA (the Malaria Eradication Scientific Alliance).
 The MESA operational research portfolio includes: proof-of-concept of novel vector control and diagnostic tools, use of mapping technologies for surveillance and tailored response, and mobile phone applications for hard to reach populations. Urban, rural and forest settings are addressed. The projects are summarised below …
The MESA operational research portfolio includes: proof-of-concept of novel vector control and diagnostic tools, use of mapping technologies for surveillance and tailored response, and mobile phone applications for hard to reach populations. Urban, rural and forest settings are addressed. The projects are summarised below …
- Mopping up and getting to zero: mapping residual malaria transmission for targeted response in urban Lusaka, Zambia.
- Using voice]based technology to improve access to malaria care and treatment among high risk mobile population of forest goers in Cambodia.
- Applying novel nucleic acid surveillance to malaria elimination in South Cotabato Province, Mindanao, The Philippines.
- Efficacy and safety of high]dose ivermectin in reducing malaria transmission.
 inety-one proposals were submitted to the call and after a thorough review process with an independent Peer Review Panel, 4 were selected for funding. The Peer Review Panel was composed of 12 experts from all over the globe. You can find a schematic of the review process through this link.
inety-one proposals were submitted to the call and after a thorough review process with an independent Peer Review Panel, 4 were selected for funding. The Peer Review Panel was composed of 12 experts from all over the globe. You can find a schematic of the review process through this link.
MESA (the Malaria Eradication Scientific Alliance) follows-up on the mal ERA agenda and provides a dedicated platform for the community in order to accelerate the translation of the science of malaria eradication for impact.
Elimination &IPTp &ITNs &Treatment Bill Brieger | 06 Dec 2013
Draft Nigeria 2013 DHS Shows Slow Progress for Malaria
The Nigeria Demographic and Health Survey (DHS) 2013 Draft Preliminary Report from the National Population Commission, Abuja, Nigeria and MEASURE DHS, ICF International, Calverton, Maryland, USA was released in-country in September 2013. These are the same organizations that conducted the 2010 Malaria Information Survey (MIS).
From the malaria perspective this has been a long anticipated event since the country has distributed over 60 million long lasting insecticide-treated nets since 2009. The 2010 MIS showed some progress over the 2008 DHS, but since it took place near the beginning of the massive net distribution effort, there was hope that a subsequent survey would highlight an improvement. If that were the expectation, people will be quite disappointed.
Lets start with nets. Our attached table shows only a slight improvement in the proportion of households owning at least one net. The idea behind the massive net campaigns from 2009-12 were achievement of universal coverage where there would be at least one net for every two people in a household. Where did these nets go? Were they damaged beyond use in the relatively short time that elapsed?
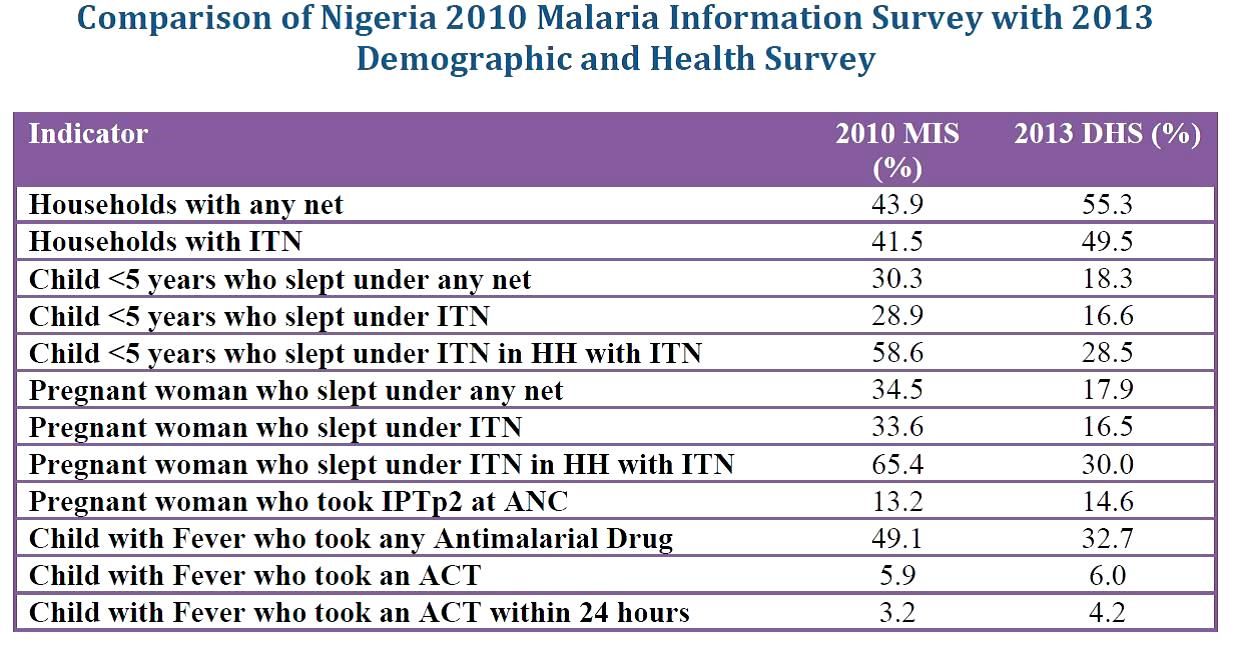 What is more disappointing is that th proportion of young children and pregnant women sleeping under an insecticide treated net (ITN) reduced to just slightly over half of the 2010 figure. This reduction also happened even in households that actually owned ITNs. This is mysterious to say the least.
What is more disappointing is that th proportion of young children and pregnant women sleeping under an insecticide treated net (ITN) reduced to just slightly over half of the 2010 figure. This reduction also happened even in households that actually owned ITNs. This is mysterious to say the least.
Prevention of malaria in pregnancy has been a neglected part of malaria control in many countries, but since the drug used for intermittent preventive treatment (IPT), sulphadoxine-pyrimethamine (SP) is so cheap, it was assumed that most health systems could afford to guarantee every woman attending antenatal care the required dosed. Unfortunately the status of IPT showed almost no improvement between 2010 and 2013 and remained far, far below the 2010 Roll Back Malaria target of 80% coverage. SP is produced in Nigeria; why can it not reach pregnant women?
Finally appropriate malaria treatment of young children is also in the doldrums. The actual number of children who received any anti-malarial drug declined, while those receiving the appropriate artemisinin-based combination therapy (ACT) remained essentially level at around 6%. Where have all the ACTs brought in through Global Fund, the US President’s Malaria Initiative and other donors gone? How can we expect infant and child mortality to decrease in the absence of appropriate treatment for one of the most common child killer diseases?
At the recently concluded 6th Pan African Malaria Conference in Durban, South Africa, participants were told that the only way to truly eliminate malaria is to tackle the high burden countries like Nigeria head on. If these data indicate how we are waging the malaria battle in Nigeria, our hopes for elimination in the near future will be dashed.
Elimination &Epidemiology Bill Brieger | 21 Nov 2013
Man’s Best Friend May Harbor Guinea Worm
 Chad had been free of debilitating guinea worm disease for a decade when ten new cases were uncovered in 2010. Logistical factors have prevented containment and the disease persists into the current transmission season. The Ministry of Health in Chad is currently examining 9 cases of human guinea worm but also 50 cases in dogs and one in a cat.
Chad had been free of debilitating guinea worm disease for a decade when ten new cases were uncovered in 2010. Logistical factors have prevented containment and the disease persists into the current transmission season. The Ministry of Health in Chad is currently examining 9 cases of human guinea worm but also 50 cases in dogs and one in a cat.
Donald Hopkins and colleagues recently explained that “Guinea worms in dogs have been reported for almost a century in some areas of Asia, Africa, and North America, including in some recently endemic countries that have interrupted transmission, but disease caused by D. medinensis has never been reported again after human transmission was interrupted.” In this situation where the cases in dogs far outnumber those in humans, one wonders hat the future holds for breaking transmission.
 Two key lessons from this experience are to be learned by the malaria community. First is the fact that once eliminated, an infectious disease can return. The context though probably relates to the neighborhood. Post-conflict South Sudan is one of the few remaining countries with continued guinea worm transmission and refugee movement may have contributed to the problem.
Two key lessons from this experience are to be learned by the malaria community. First is the fact that once eliminated, an infectious disease can return. The context though probably relates to the neighborhood. Post-conflict South Sudan is one of the few remaining countries with continued guinea worm transmission and refugee movement may have contributed to the problem.
The second lesson is the potential for inter-species transmission. Plasmodium knowlesi, a disease of primates, appears about to become entrenched in the human population of Southeast Asia. Cases of monkeys having P. vivax have been documented in South America and Africa. Elimination of human transmission of malaria may be hampered by non-human reservoirs.
We may not be able to say that elimination has occurred until there is no local transmission of any species of Plasmodium that affect humans in any other life form. We have a hard enough time tracking malaria in humans when it falls below levels detectable by microscopes and rapid tests. What of the challenges of tracking it in monkeys? Maybe these complications explain why to date smallpox remains the exception to the eradication rule.
Elimination &Eradication Bill Brieger | 10 Oct 2013
After Dramatic Decline in Malaria Deaths in Africa, Scientists Plan for Final Eradication
 PRESS RELEASE: Thursday, 10 October 2013 at 12:00pm SAST (GMT+2)
PRESS RELEASE: Thursday, 10 October 2013 at 12:00pm SAST (GMT+2)
After Dramatic Decline in Malaria Deaths in Africa, Scientists Plan for Final Eradication: How to win the Endgame Against an Ancient Foe?
At world’s largest meeting of malaria experts, evidence of elimination work underway at edge of disease distribution; focus now turns to malaria heartlands
DURBAN, SOUTH AFRICA (10 OCTOBER 2013)—With widespread use of insecticide-treated nets, indoor spraying and potent malaria medications credited with dramatically reducing malaria deaths in Africa, experts at a major malaria conference discussed the potential to use this progress as a springboard for achieving eradication of a disease that still kills some 660,000 people each year—most of them young African children.
“For the first time we have achieved very large-scale vector control coverage in Africa, and these interventions have prevented a large number of deaths and greatly reduced the burden of transmission,” said Jo Lines, a malaria expert with the London School of Hygiene & Tropical Medicine who previously led the Vector Control Unit of the World Health Organization’s Global Malaria Program. “So while there is a lot of attention still rightly focused on how we can win the battles of today or next week or next year, we can start turning our attention to the longer-term and think about what is needed to win the war.”
Lines was one of several malaria experts discussing the road to malaria eradication in Africa at the Sixth Multilateral Initiative on Malaria (MIM) Pan-African Malaria Conference—the world’s largest gathering of malaria experts—taking place in Durban, South Africa, 6-11 October 2013. Presentations at MIM, including the symposium Lines chaired on “planning for the endgame in Africa,” highlighted how scientists are transitioning from eradication as a lofty aspiration to one that involves an operational plan on the ground.
For example, researchers from South Africa discussed efforts to develop a web site dense with data on local malaria infections, part of the country’s effort to fight practically case by case to achieve its goal of eliminating malaria from the country by 2018. And researchers from Namibia presented the results from a joint effort to police malaria with neighboring Angola, an example, they said, of the cross-border initiatives that will be needed across Africa to eliminate malaria from the continent. Other researchers offered new approaches to malaria control they believe may be more “sustainable.”
According to an abstract by Chistopher Plowe with the Howard Hughes Medical Institute, vaccines are likely to be essential to malaria elimination, given that vaccines have been part of “nearly all successful” infectious disease eradication efforts and “absent from all unsuccessful campaigns.”
THE ELIMINATION CONUNDRUM: MAKING MALARIA GET OUT AND STAY OUT
Lines said that eliminating malaria in Africa requires confronting a range of confounding questions. For example, he noted that increasing access to things like insecticide treated nets and artemisinin combination therapies (ACTs), while crucial to saving lives and reducing disease transmission, comes at a cost: the more they are used, the faster mosquitoes and parasites are likely develop resistance. Also, he said that while malaria transmission patterns are “changing radically” across Africa, it’s not always clear why.
For example, he said his research has documented that there was a significant decrease in malaria transmission in parts of Tanzania before these areas saw widespread use of insecticide treated nets. Meanwhile, in parts of Uganda and Malawi, he said transmission has remained intense despite aggressive use of bed nets and better access to effective medications.
“We don’t know why these interventions are not working equally well in all places in Africa or why in some areas, like Tanzania, the fight against malaria appears to be aided by some other process,” he said. “We do know that when we look back at areas that have eliminated malaria, like the Southern US and Europe, we see that things like land use change, housing and human behavior played a part—potentially a very large part—in conquering the disease.”
Lines said eliminating malaria in Africa requires a better understanding of the different factors affecting transmission and also more attention to disease surveillance. Such work is crucial, he said, to ensuring that once malaria is eliminated from a particular region, it doesn’t simply re-establish itself when an infected individual migrates from areas where malaria is still common.
“The lesson you want to learn from areas that have eliminated malaria is not just how did you drive it out but how did you keep it out,” he said. He said elimination might ultimately need to involve some way of reducing the capacity of mosquitoes or humans to transmit the parasite.
For example, there is work underway today to develop a vaccine that would interrupt the life-cycle of the malaria parasite by preventing it from passing from humans back to mosquitoes. Other efforts have focused on the potential of genetically modified mosquitoes that are rendered incapable of passing along the parasite.
EYES ON THE PRIZE: ELIMINATION VIA DISEASE SURVEILLANCE
In South Africa, which hopes to eliminate malaria by 2018, tracking the total number of infections, recording where they are occurring and following-up to confirm details such as travel history and symptoms is a cornerstone of the country’s elimination strategy. South Africa’s intensive malaria surveillance program includes a website that is constantly updated and features an outbreak alert system and an automated mapping program that can depict malaria cases down to the local level.
A study by Bridget M. Shandukani with South Africa’s National Department of Health found that this type of meticulous surveillance, while costly and labor-intensive, is essential to finishing off malaria in countries like South Africa that have reduced malaria transmission to relatively low levels. She and her colleagues reported that during the 2012-2013 season, all nine of the districts in South Africa at risk for malaria entered into elimination mode, “reporting local case incidences of less than one case per one thousand population at risk.”
Meanwhile, researchers from Namibia presented a study that highlights the importance of cross-border initiatives for countries targeting elimination. They noted that most of the malaria cases in northern Namibia are “imported from southern Angola.” The study examined the effectiveness of a program—the Trans Kunene Malaria Initiative—that implemented a host of interventions in a 20-square kilometer region on both sides of the Namibia-Angola border.
The interventions included long-lasting insecticide treated bed nets, rapid diagnostic tests, community education and case management. Also, both governments agreed to remove customs duties from malaria “commodities,” including bed nets and chemicals used for indoor spraying programs.
The study, presented at MIM and led by Constance Njovu with the JC Flowers Foundation’s Isdell:Flowers Cross Border Malaria Initiative, noted that both areas targeted achieved a significant reduction in malaria. “These results show that cross-border work is both critical to elimination of malaria and possible despite (involving) different national governments with language and cultural differences,” the scientists reported.
Meanwhile, researchers from the University of Pretoria focused on developing “sustainable” tools for malaria control, which they view as crucial to creating more durable reduction in illness and death and thus a more stable platform from which to pursue malaria eradication.
A study by Leo Braack with the University’s Center for Sustainable Malaria Control (CSMC) investigated night-time mosquito biting behavior outdoors, which, given the effectiveness of bed nets, are where an increasing proportion of malaria infections occur. The study found that most bites happen at or near ground level. Braack and his colleagues concluded that simply wearing mosquito-repellent anklets “holds the potential to lower malaria incidence.”
The CSMC’s Taneshka Kruger along with colleagues at the University’s Institute of Applied Materials sought to address limits to bed nets and indoor spraying as control measures: one has to be sleeping under a bed net to enjoy its protection, they noted, while indoor spraying is costly and raises fears of exposure to toxic chemicals. They found that lining interior doors with a mesh fabric treated with a slow-releasing insecticide was a safe, effective and potentially inexpensive form of long-lasting malaria control.
The Multilateral Initiative on Malaria (MIM) (http://www.mimalaria.org/eng/), launched in Dakar, Senegal in 1997, is an international alliance of organizations and individuals seeking to maximize the impact of scientific research against malaria in Africa to ensure that research findings yield practical health benefits. The MIM conference in Durban follows successful conferences held in Yaoundé, Cameroon, in November 2005, and in Nairobi in October 2009. The MIM Secretariat is currently hosted by the Biotechnology Centre of the University of Yaoundé I/Amsterdam Medical Centre.
Media Contacts:
South Africa
Louis Da Gama: +44-7990810642, ldagama@gmail.com
Jessica Rockwood: +27-793517881, jessicarockwood@verizon.net
Geoffrey So: +27-728367853, gso@rbmny.org
Jennifer Jackson: +27.835987778, jennifer.jackson@mrc.ac.za
Keletso Ratsela: +27.828048883, keletso.ratsela@mrc.ac.za
Senegal: Fara Ndiaye: +221.773328863, fara.ndiaye@speakupafrica.org
France: Michel Aublanc: +33-608719795, michel.aublanc@orange.fr
Switzerland: Pru Smith: +41-227914586, smithp@who.int
United Kingdom: Alex Fullem: +44-7787404884, afullem@path.org
USA: Geoffrey So: +1-3479320820, gso@rbmny.org
Trey Watkins: +1-6466266054, kwatkins@rbmny.org
Follow the conversation on social media! #MIM2013 @MIMConf2013
Elimination &Health Systems Bill Brieger | 30 Sep 2013
Will we eliminate malaria programs before we eliminate malaria?
 As malaria cases dwindle and we approach elimination, will malaria programs be integrated into broader disease control efforts? Integration is all the rage, but what does it mean for disease eradication efforts?
As malaria cases dwindle and we approach elimination, will malaria programs be integrated into broader disease control efforts? Integration is all the rage, but what does it mean for disease eradication efforts?
The arguments for and against vertical versus horizontal, siloed versus integrated programming sometimes misses the point when it comes to disease eradication. Eradication is by nature a time-bound and focused activity. Without a clear, reasonable target date, eradication will not happen, but disease control will linger until some financial or other event causes us to drop the ball completely and cases start rising again. This might sound familiar to those who were around for the malaria eradication efforts that floundered in the 1960s.
We may have been premature to start talking about malaria eradication a few years ago, but the discussion is needed about the state of malaria programming as pre-elimination and elimination are being reached in many countries. We must begin looking around for the resources for that last push toward eradication. In the absence of a dedicated malaria eradication effort – a vertical program if you will – will be be able to organize the efforts needed for the final step?
 Let’s draw some lessons from guinea worm. From the start in the 1980s programs were established that were called National Guinea Worm Eradication Programs, not guinea worm programs or guinea worm control programs, but eradication programs. A specific date was set – 1995, and in most cases a dedicated team of people went to work on a well defined set of interventions from the national to regional to district to community levels.
Let’s draw some lessons from guinea worm. From the start in the 1980s programs were established that were called National Guinea Worm Eradication Programs, not guinea worm programs or guinea worm control programs, but eradication programs. A specific date was set – 1995, and in most cases a dedicated team of people went to work on a well defined set of interventions from the national to regional to district to community levels.
Where the guinea worm effort faltered was when countries tried to ‘integrate’ it with other disease control or primary health care services. Work became unfocused and ten or more years were added to what should have been a straight-forward march to elimination in these countries by 1995. What this meant in Nigeria was that the pace slowed, but at least was continual, and now 18 years after the original target date was finally declared free of the disease. In Ghana, with guinea worm hidden amongst the duties of pluripotent district disease control officers, cases began to rise again.
Already some countries that are in a high level of control and witnessing major drops in incidence and mortality have combined their malaria programs into a broader disease control unit or department. There are hints that donors may wish to focus more on high burden areas for major scale-up and control. All partners must be willing to ensure that both the funds/resources as well as the organizational infrastructure (systems) are in place to guarantee elimination in each endemic country.
Elimination &Funding &Surveillance Bill Brieger | 01 Sep 2013
Eliminate Malaria, Not Malaria Funding
As countries begin to see the benefits of sustained malaria intervention, they worry that they may be punished by donor agencies for their success. For example, The Tanzania Daily News reports that, “HEALTH officials in Zanzibar have said that the Islands are likely to experience problems in the fight against Malaria should major donors, including Global Fund and the United States government pull out from financing the project.”
 Zanzibar is nearing pre-elimintion malaria transmission levels but is dependent on donor funding to maintain progress. The Daily News specifies that, “The US through its President’s Malaria Initiatives (PMI) remains the leading financier with 56 per cent of the funds received for the malaria campaign. Global Fund is 40 per cent, WHO and UNICEF two per cent; other donors 1.97 per cent; and Zanzibar government is 0.03 per cent.”
Zanzibar is nearing pre-elimintion malaria transmission levels but is dependent on donor funding to maintain progress. The Daily News specifies that, “The US through its President’s Malaria Initiatives (PMI) remains the leading financier with 56 per cent of the funds received for the malaria campaign. Global Fund is 40 per cent, WHO and UNICEF two per cent; other donors 1.97 per cent; and Zanzibar government is 0.03 per cent.”
Health officials did clarify the actual situation by saying that, “We are happy that PMI has not shown any indication to pull out, but we must prepare ourselves and look for alternative financiers should the US stop supporting Malaria programme.” A look at the latest grant progress report for Zanzibar at the Global Fund website had only a report from August 2012 for Round 8 Malaria Grant that was made near the end of Phase 1 of the grant.
It is not clear if Phase 2 of the Global Fund grant has been or will be funded, but we know that the GFATM has been going through financial difficulties and changes. This is likely why Zanzibar health managers are worried. The last grant rating was files back in 2011 and gave the program a ‘B2’ rating which is cause for caution and possibly hints at reasons why Phase 2 is in limbo.
PMI reports that donor support and Zanzibari leadership, “has resulted in a dramatic decrease in malaria prevalence in Zanzibar. However, persistence of malaria transmission in surrounding areas (Tanzania mainland and Kenya) leaves the island vulnerable to sudden outbreaks and the re-establishment of ongoing, perennial malaria transmission.” Even though Zanzibar is an island, it is still vulnerable, and any withdrawal of support would negate and reverse gains made. For example, PMI explains that Zanzibar is a place where “Malaria Early Epidemic Detection System (MEEDS) … an innovative mHealth system” is being tested.
Pre-elimination not only requires sustaining existing interventions, but also implementing new ones like MEEDS in order to maintain necessary surveillance that will ultimately document whether malaria elimination has succeeded. As PMI notes, “MEEDS and Coconut Surveillance are helping Zanzibar to identify and treat many otherwise undiagnosed malaria cases, identifying hot spots and transmission patterns, and responding rapidly to new outbreaks. These mHealth applications are helping Zanzibar to sustain the remarkable gains it has made against this dangerous and debilitating disease.”
Also, “maintaining and continuing to reduce malaria transmission will require ongoing education for both health care providers and residents to reinforce the importance of using preventive measures,” as the public and health workers perceive the drop in prevalence according to Bauch and colleagues. Malaria prevalence in Zanzibar has been less that 1% for over 6 years, and we need to continue to reduce it.
Interventions in the final phases of malaria elimination may not be as dramatic or visible as distributing millions of insecticide treated bednets, but they are just as essential. We need to maintain support in all endemic countries until we see malaria elimination through to its conclusion. Otherwise years of intervention will be wasted, and new lives will be lost.