Borders &Diagnosis &Epidemiology &ITNs Bill Brieger | 30 Sep 2015
Individual and Household Level Risk Factors Associated with Malaria in Mutasa District, Zimbabwe: a Serial Cross-Sectional Study
Mufaro Kanyangarara and her PhD thesis adviser, Luke Mullany of the Johns Hopkins Bloomberg School of Public Health Department of International Health, have been looking into the challenges of controlling and eventually eliminating malaria in a multi-country context in southern Africa. We are sharing abstracts from her pioneering work including the following which explores risk factors on the Zimbabwe-Mozambique order.
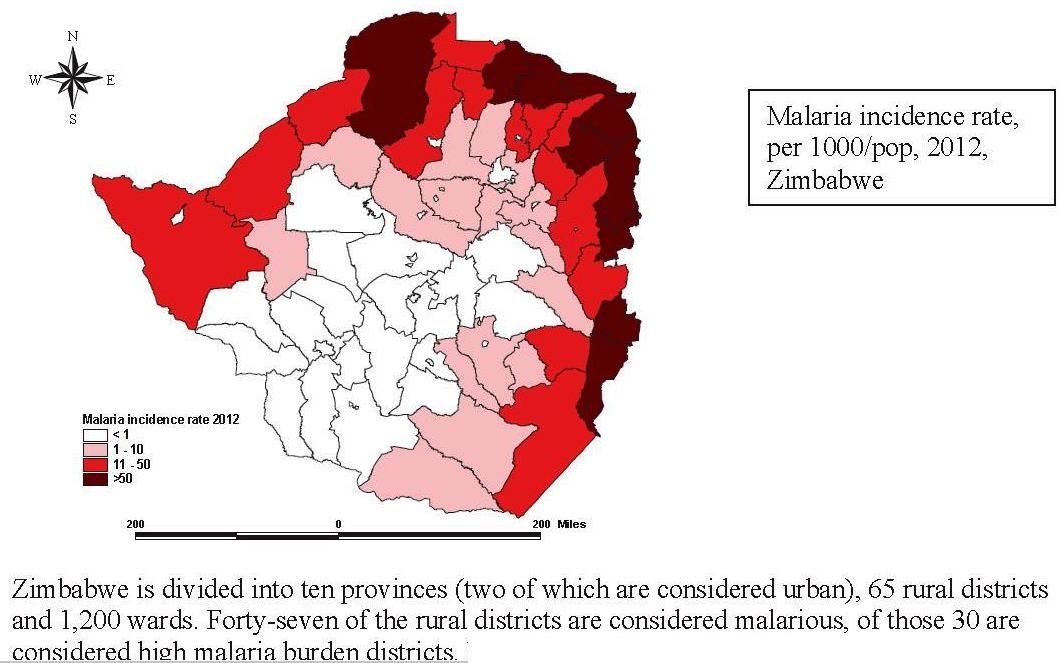
Background: Malaria constitutes a major public health problem in Zimbabwe, particularly in the north and east bordering Zambia and Mozambique. In Manicaland Province in eastern Zimbabwe, malaria transmission is seasonal and unstable. As a result of intensive scale up of malaria interventions, malaria control was successful in Manicaland Province. However, over the past decade, Manicaland Province has reported increased malaria transmission, and the resurgence of malaria in this region has been attributed to limited funding, drug resistance and insecticide resistance. One of the worst affected districts is Mutasa District. The aim of the study was to identify malaria risk factors at the individual and household levels to better understand what is driving factors associated with malaria and consequently enhance malaria control in eastern Zimbabwe.
north and east bordering Zambia and Mozambique. In Manicaland Province in eastern Zimbabwe, malaria transmission is seasonal and unstable. As a result of intensive scale up of malaria interventions, malaria control was successful in Manicaland Province. However, over the past decade, Manicaland Province has reported increased malaria transmission, and the resurgence of malaria in this region has been attributed to limited funding, drug resistance and insecticide resistance. One of the worst affected districts is Mutasa District. The aim of the study was to identify malaria risk factors at the individual and household levels to better understand what is driving factors associated with malaria and consequently enhance malaria control in eastern Zimbabwe.
Methods: Between October 2012 and September 2014, individual demographic data and household characteristics were collected from cross-sectional surveys of 1,116 individuals residing in 316 households in Mutasa District. Factors characterizing the surrounding environment were obtained from remote sensing data. Factors associated with malaria (measured by rapid diagnostic test [RDT]) were identified through univariate and multivariate multilevel logistic regression models.
Results: A total of 74 (6.4%) participants were RDT positive. Parasite prevalence differed by season (10.4% rainy and 2.9% dry, OR 4.52, 95% CI 2.11-9.69). Sleeping under a bednet showed a protective effect against malaria (OR 0.54, 95% CI 0.29-1.00) despite pyrethroid resistance. The household level risk factors protective against malaria were household density (OR 0.89, 95% CI 0.87-0.97) and increasing distance from the border with Mozambique (OR 0.86, 95% CI 0.76-0.97). Increased malaria risk was associated with recent indoor residual spraying (OR 2.30, 95% CI 1.16-4.56).
Conclusions: Malaria risk was concentrated in areas located at a lower household density and in closer proximity to the Mozambique border. Malaria control in these “high risk” areas may need to be enhanced. These findings underscore the need for strong cross-border malaria control initiatives to complement country specific interventions.
Borders &Elimination &Resistance &Surveillance Bill Brieger | 29 Sep 2015
Epidemiology of Resurgent Malaria in Eastern Zimbabwe: Risk Factors, Spatio-Temporal Patterns and Prospects for Regaining Malaria Control
Mufaro Kanyangarara and her PhD thesis adviser, Luke Mullany, of the Johns Hopkins Bloomberg School of Public Health Department of International Health, have been looking into the challenges of controlling and eventually eliminating malaria in a multi-country context in southern Africa. We are sharing abstracts from her pioneering work. The first seen below provides an overview of the three components of the study.
 Despite recent reductions in malaria morbidity and mortality due to the scale up of malaria interventions, malaria remains a public health problem in sub-Saharan Africa, especially among children under five years of age, pregnant women and people living with HIV/AIDS. A recent resurgence in malaria, in areas where malaria control was previously successful, has brought to the forefront the importance of research to understand the epidemiology of malaria and the effectiveness of malaria control efforts in resurgent settings. Using cross-sectional surveys, routine data from health-facility based surveillance and freely available remotely sensed environmental data, this research examined the distribution of malaria and the impact of vector control in Mutasa, a rural district in Zimbabwe characterized by resurgent malaria.
Despite recent reductions in malaria morbidity and mortality due to the scale up of malaria interventions, malaria remains a public health problem in sub-Saharan Africa, especially among children under five years of age, pregnant women and people living with HIV/AIDS. A recent resurgence in malaria, in areas where malaria control was previously successful, has brought to the forefront the importance of research to understand the epidemiology of malaria and the effectiveness of malaria control efforts in resurgent settings. Using cross-sectional surveys, routine data from health-facility based surveillance and freely available remotely sensed environmental data, this research examined the distribution of malaria and the impact of vector control in Mutasa, a rural district in Zimbabwe characterized by resurgent malaria.
Firstly, individual- and household level factors independently associated with individual malaria risk were identified using multilevel logistic regression models based on data from cross-sectional surveys conducted between October 2012 and September 2014. Secondly, geostatistical methods and remotely sensed environmental data were used to model the spatial and seasonal distribution of household malaria risk; then develop seasonal malaria risk maps with corresponding maps of the prediction uncertainty. Lastly, an evaluation of the effect of introducing an organophosphate for indoor residual spraying was conducted using routine health facility data covering 24 months before and 6 months after the campaign.
The results of multilevel model suggested that malaria risk was significantly higher among individuals who were younger than 25 years, did not sleep under a bed net, and lived close to the Zimbabwe-Mozambique border. The spatial risk maps depicted relatively increased risk of finding a positive household in low-lying areas along the Mozambique border during the rainy season. Lastly, the introduction of organophosphates to this pyretheroid resistant area resulted in a significant reduction in malaria incidence following spraying. These findings elucidate the heterogeneous distribution of malaria, identify risk factors driving malaria transmission and assess the quantitative impact of switching insecticide classes on health outcomes. Collectively, the findings provide evidence to guide country-specific decision making for regaining malaria control and underscore the need for strong between-country initiatives to curb malaria in Mutasa District and elsewhere.
Borders &Elimination &Indoor Residual Spraying &Monitoring &Surveillance &Vector Control Bill Brieger | 13 Jun 2015
Moving toward Malaria Elimination in Botswana
 The just concluded 2015 Global Health Conference in Botswana, hosted by Boitekanelo College at Gaborone International Convention Centre on 11-12 June provided us a good opportunity to examine how Botswana is moving toward malaria elimination. Botswana is one of the four front line malaria elimination countries in the Southern African Development Community and offers lessons for other countries in the region. Combined with the 4 neighboring countries to the north, they are known collectively as the “Elimination Eight”.
The just concluded 2015 Global Health Conference in Botswana, hosted by Boitekanelo College at Gaborone International Convention Centre on 11-12 June provided us a good opportunity to examine how Botswana is moving toward malaria elimination. Botswana is one of the four front line malaria elimination countries in the Southern African Development Community and offers lessons for other countries in the region. Combined with the 4 neighboring countries to the north, they are known collectively as the “Elimination Eight”.
The malaria elimination countries are characterised by low leves of transmission in focal areas of the country, often in seasonal or epidemic form. The pathway to malaria elimination requires that a country or defined areas in a country reach a slide positivity rates during peak malaria season of < 5%.
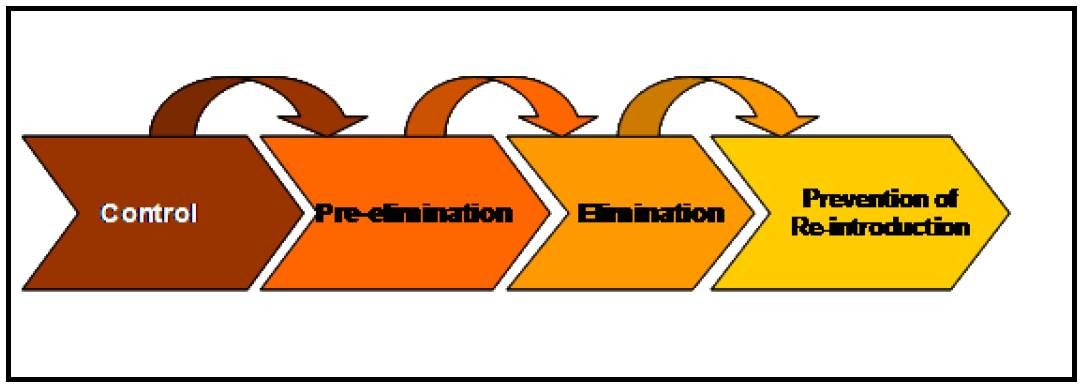 Chihanga Simon et al. provide us a good outline of 60+ years of Botswana’s movements along the pathway beginning with indoor residual spraying (IRS) in the 1950s. Since then the country has expanded vector control to strengthened case management and surveillance. Particular recent milestones include –
Chihanga Simon et al. provide us a good outline of 60+ years of Botswana’s movements along the pathway beginning with indoor residual spraying (IRS) in the 1950s. Since then the country has expanded vector control to strengthened case management and surveillance. Particular recent milestones include –
- 2009: Malaria elimination policy required all cases to be tested before treatment malaria elimination target set for 2015
- 2010: Malaria Strategic Plan 2010–15 using recommendations from programme review of 2009; free LLINs
- 2012: Case-based surveillance introduced
The national malaria elimination strategy includes the following: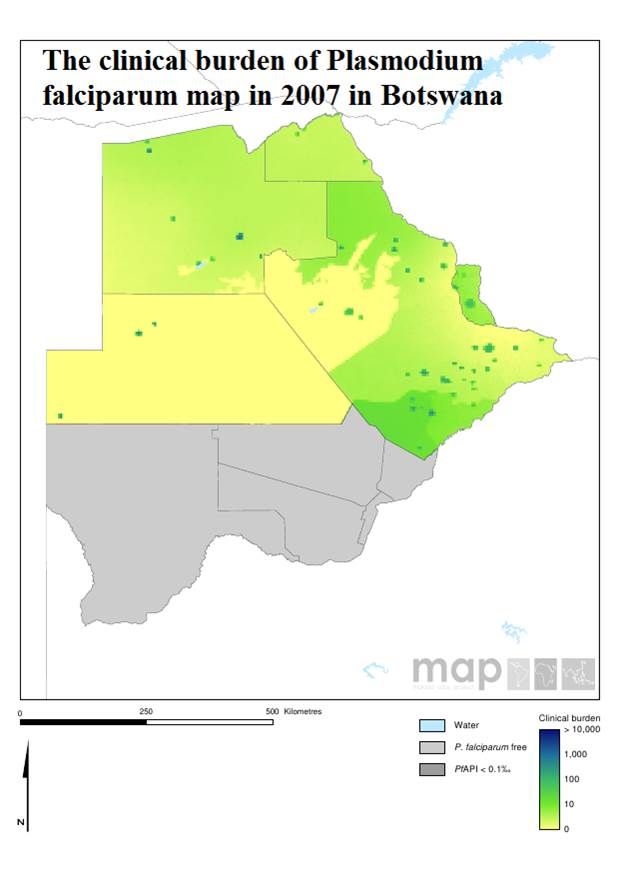
- Focus distribution LLIN & IRS in all transmission foci/high risk districts
- Detect all malaria infections through appropriate diagnostic methods and provide effective treatment
- Develop a robust information system for tracking of progress and decision making
- Build capacity at all levels for malaria elimination
Botswana like other malaria endemic countries works with the Roll Back Malaria Partnership to compile an annual road map that identifies progress made and areas for improvement. The 2015 Road Map shows that –
- 116,229 LLINs distributed during campaigns in order to maintain universal coverage in the 6 high risk districts
- 200,721 IRS Operational Target structures sprayed
- 2,183,238 RDTs distributed and 9,876 microscopes distributed
- While M&E, Behavior Change, and Program Management Capacity activities are underway
 Finally the African Leaders Malaria Alliance (ALMA) provides quarterly scorecards on each member. Botswana is making a major financial commitment to its malaria elimination commodity and policy needs. There is still need to sustain high levels of IRS coverage in designated areas.
Finally the African Leaders Malaria Alliance (ALMA) provides quarterly scorecards on each member. Botswana is making a major financial commitment to its malaria elimination commodity and policy needs. There is still need to sustain high levels of IRS coverage in designated areas.
Monitoring and evaluation is crucial to malaria elimination. Botswana has a detailed M&E plan that includes a geo-referenced surveillance system, GIS and malaria database training for 60 health care workers, traininf for at least 80% of health workers on Case Based Surveillance in 29 districts, and regular data analysis and feedback.
M&E activities also involve supervision visits for mapping of cases, foci and interventions, bi-annual malaria case management audits, enhanced diagnostics through PCR and LAMP as well as Knowledge, Attitudes, Behaviour, and Practice surveys.
Malaria elimination activities are not simple. Just because cases drop, our job is easier. Botswana, like its neighbors in the ‘Elimination Eight’ is putting in place the interventions and resources needed to see malaria really come to an end in the country. Keep up the good work!
Borders &Surveillance Bill Brieger | 02 May 2014
Failure of malaria control efforts in northern Zambia

UNICEF, Zambia http://www.unicef.org/zambia/5109_8454.html
World Malaria Day 2014 was observed at the Johns Hopkins Bloomberg School of Public Health on Friday 25 April. 21 posters were presented. Below is the abstract of a third poster presented William Moss and colleagues from the Southern Africa International Centers of Excellence for Malaria Research.
Despite distribution of insecticide-treated bed nets, indoor residual spraying and case management with rapid diagnostic tests and artemisinin-based combination therapy, the burden of malaria remains high in northern Zambia.

RBM Impact Series Zambia http://www.rbm.who.int/ProgressImpactSeries/report7.html
Through passive case detection at health care facilities and active case detection through community-based surveys, we have documented persistently high parasite prevalence in Nchelenge District, Luapula Province, Zambia on the border of Lake Mweru with the Democratic Republic of Congo. Individual and household level risk factors for malaria were assessed and a spatial risk map constructed.
Pyrethroid resistance in local Anopheles funestus populations likely contributes to failure of current control efforts. Potentially contributing to malaria transmission is population movement from the lakeside to inland as fishing and agricultural seasons alternate.
Equally important may be cross-border movement between Nchelenge District, Zambia and Katanga Province in the Democratic Republic of Congo, suggesting the importance of epidemiological and entomological studies of cross-border malaria.
Borders &Surveillance Bill Brieger | 01 May 2014
Resurgent Malaria in Eastern Zimbabwe
 World Malaria Day 2014 was observed at the Johns Hopkins Bloomberg School of Public Health on Friday 25 April. 21 posters were presented. Below is the abstract of another poster presented William Moss and colleagues from the Southern Africa International Centers of Excellence for Malaria Research.
World Malaria Day 2014 was observed at the Johns Hopkins Bloomberg School of Public Health on Friday 25 April. 21 posters were presented. Below is the abstract of another poster presented William Moss and colleagues from the Southern Africa International Centers of Excellence for Malaria Research.
Eastern Zimbabwe has experienced recent large outbreaks of malaria after a history of successful control. Through passive case detection at health care facilities and active case detection through community-based surveys, we have documented seasonal malaria outbreaks in Mutasa District, Manicaland Province, Zimbabwe on the border with Mozambique.
We identified individuals with subpatent parasitemia who may be responsible for sustaining transmission during the dry season.
Pyrethroid resistance in local Anopheles funestus populations likely contributes to failure of current control efforts.
Potentially contributing to malaria transmission is population movement across the border with Mozambique.
* * * * * * *
Of interest, The Standard newspaper of Zimbabwe recently reported on this problem saying that, “Malaria burden remains high in border towns in Zimbabwe, especially in areas close to Mozambique, health experts have said. While the overall national statistics indicate a major decline from 5 000 deaths to 300 per year, border districts like Mudzi are still recording high cases.”
Borders &Elimination Bill Brieger | 30 Sep 2012
Rwanda Malaria Elimination Forum’s Working Group on Cross-Border Initiatives
 A key focus of the recently completed First Rwanda Malaria Forum was on cross-border initiatives to help eliminate malaria. The two most malaria-endemic districts in Rwanda are situated at borders with other malaria endemic countries. Nyagatare borders Uganda and Tanzania, while Gisagara borders Tanzania and Burundi. The Democratic Republic of Congo, which has some of the highest malaria burden in the world, shares a long border with Rwanda, too.
A key focus of the recently completed First Rwanda Malaria Forum was on cross-border initiatives to help eliminate malaria. The two most malaria-endemic districts in Rwanda are situated at borders with other malaria endemic countries. Nyagatare borders Uganda and Tanzania, while Gisagara borders Tanzania and Burundi. The Democratic Republic of Congo, which has some of the highest malaria burden in the world, shares a long border with Rwanda, too.
The Working Group on Cross Border Planning and Initiatives consisted of Nancy Mock (Tulane), Charles Paluku, Okui Albert Peter (Uganda), James Banda (WHO/GMP), Carol Asiimwe, Harriet Pasquale (South Sudan), Simon Kunene (Swaziland), Dorothy Memusi (Kenya), Corine Karema (Rwanda), Felicien Ndayizeye (Burundi), Patrick Moonasar ( Rapporteur), Georges A. Ki-Zerbo (WHO/AFRO). Their overall strategic considerations are found in the table below.

Key action points focused on defining the problem and drafting a concept paper. Defining the problem would require Two meetings with all 5 countries supported by RBM’s East Africa Regional Network (EARN)Earn Support. The first meeting would focus on a conducting situational analysis and drafting of framework for data collection (before 15 December 2012). The second meeting would bring evidence based on Framework for collaboration in moving towards malaria elimination and a draft concept paper (March 2013).
The draft a concept paper would cover the following key issues:
- Disease burden in all neighboring districts
- Coverage target in all neighboring countries and other factors e.g. demographic and social factors.
- Rational for initiative
- Objectives
- Activities
- Budget
- Coordination mechanism
- Recommendations
- Action plan
Facilitators for this effort should be WHO and EARN. Because of Swaziland’s experience with such cross-border efforts the working group identified its National Malaria Control Program Director, Simon Kunene, as an expert who could provide technical assistance.
In summary key recommendations arising from the Working Group deliberations include:
- A cross border initiative meeting including target district leaders
- WHO/EARN to provide oversight TA, invite target NMCP managers and District Health Management Teams
- Each country shall initiate internal discussions on cross border initiatives
- Each member country to ensure inclusion of Cross-Border initiatives into national strategic plans and share data collection tool at country meetings
Borders &Elimination Bill Brieger | 13 Sep 2012
Collaborate to Eliminate: sub-regional and cross-border
 The Roll Back malaria Partnership supports four sub-regional networks (SRNs) in East, Southern, Central and West Africa. The SRNs are a mechanism for strengthening South-South collaboration in the fight against malaria. Such collaboration is essential as neighboring countries move closer to elimination and policies and transmission patterns in one can affect the success of elimination efforts in another.
The Roll Back malaria Partnership supports four sub-regional networks (SRNs) in East, Southern, Central and West Africa. The SRNs are a mechanism for strengthening South-South collaboration in the fight against malaria. Such collaboration is essential as neighboring countries move closer to elimination and policies and transmission patterns in one can affect the success of elimination efforts in another.
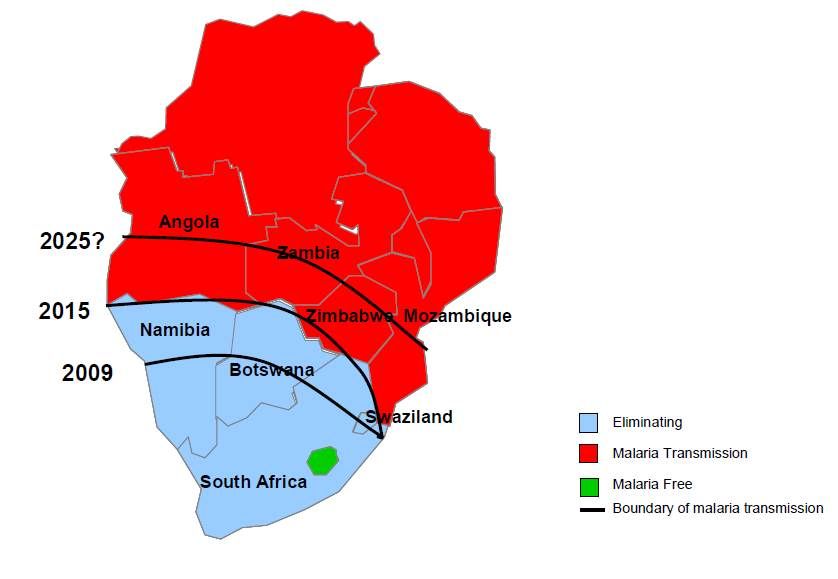
The collaboration is particularly visible and active in the Southern African SRN (SARN), where a meeting has just concluded to plan action along the Angola-Namibia border – otherwise known as the Trans-Kunene Cross-border Malaria Initiative (TKMI). Similar initiatives are ongoing among all of the ten partners who include Botswana, Madagascar, Malawi, Mozambique, Namibia, South Africa, Swaziland, URT-Zanzibar, Zambia, Zimbabwe.
The northern border area of Namibia is its only malaria endemic region. While the area of Angola just across the border has similar transmission patterns, the whole of Angola farther north is highly endemic. Angola’s actions can therefore, affect the fate of malaria elimination in Namibia.
At the TKMI meeting in August 2012 Stakeholders reviewed activities during the 2011-12 malaria transmission season and affirmed commitment of the two governments to continue to work together to eliminate malaria in their cross-border region. An important component of collaborative work is the synchronization of operations and harmonization of policies and guidelines such as joint Monitoring and Evaluation and data systems including exchange of information and best practices will ensure that all cases are reported and traced jointly along the border.
 Another crucial area of collaboration, according to SARN Leadership, is removal of border immigration restrictions and customs requirement will speed up movement malaria workers and malaria commodities especially during epidemics, cross-border referrals, joint outreaches and joint operations/campaigns such as IRS, Larviciding and LLINs mass distribution. This also helps to resolve bottlenecks related to delivery.
Another crucial area of collaboration, according to SARN Leadership, is removal of border immigration restrictions and customs requirement will speed up movement malaria workers and malaria commodities especially during epidemics, cross-border referrals, joint outreaches and joint operations/campaigns such as IRS, Larviciding and LLINs mass distribution. This also helps to resolve bottlenecks related to delivery.
Policy and program guidelines for elimination recommended by the stakeholders included test, treat and trace, and hence, they stressed the need for using rapid diagnostic tests and training all health staff in the region to be proficient in these. Prompt and appropriate case management was also outlined including the need, an mentioned above, for easy cross-border movement of supplies of malaria medicines. Indoor residual spraying is a very appropriate strategy in these low and unstable transmission areas, and will be more effective if communities on both sides of the border are covered equally.
The TKMI meeting ended with a declaration of the collaborating partners. They observed that the considerable effort in malaria control in the two countries had “produced good results in the drastic reduction of mortality and morbidity caused by this disease,” and pledged that this will continue through “reinforcement of
harmonization of policies and strategic components.”
The two countries’ stakeholders recognized that common efforts to improve logistics such as “infrastructures, transport, immigration and customs along the common” were just as important as harmonizing program policies and guidelines. In closing “two parties promised to engage in a process of mobilizing more
resources and partnerships at different levels, with the aim to accelerate the universal coverage along the common border border.” This spirit of collaboration is needed throughout malaria endemic regions.
Asia &Borders &Resistance Bill Brieger | 25 Aug 2012
Asia-Pacific: a region of contrasting hopes for eliminating malaria
The burden of malaria in the Asia-Pacific region, being much lower than that of Africa, has led to some neglect in the past when it comes to rolling back the disease. Two news reports today show why neglect is not an option is global country-by-country elimination os the disease is to be achieved.
 Hope was expressed clearly by national Department of Health authorities in the Philippines who exclaimed that “THE Philippines could be malaria-free by 2020 as the number of cases declined by 80 percent in the recent years, the Department of Health (DOH) said on Friday.” The article in the Manila Sun-Star quoted Health Secretary Enrique Ona who said “The government has recorded 9,642 malaria cases in 2011 as compared to 43,441 in 2003.”
Hope was expressed clearly by national Department of Health authorities in the Philippines who exclaimed that “THE Philippines could be malaria-free by 2020 as the number of cases declined by 80 percent in the recent years, the Department of Health (DOH) said on Friday.” The article in the Manila Sun-Star quoted Health Secretary Enrique Ona who said “The government has recorded 9,642 malaria cases in 2011 as compared to 43,441 in 2003.”
A close accounting of the 58 provinces that are considered endemic in the Philippines found that nine have had no cases in the past three years, and forty have been reporting less than 1 case per 1000. While definitely being optimistic about the prospects of overall elimination from the country, the Health Secretary is realistic as quoted by the Sun-Times: “The journey towards elimination status is more difficult than working for a reduction in cases and we will need more commitments and resolutions of the different sectors to be consolidated into a singular, comprehensive initiative so that the whole country, not just the 58 endemic provinces, will be declared malaria-free by 2020.”
The situation in another regional partner is more dire. VOA reports that the problem of malaria drug resistance is “more severe in Cambodia than anywhere else in the world.” The National malaria Center in Cambodia found that, “About 17 percent of all cases in the Cambodian-Thai border area of Pailin were drug-resistant in 2011, up from 10 percent the year before.”
On the positive side, even though the proportion of drug-resistant cases in increasing, the total number of cases continues to decrease. Still, there is concern about ramification of the situation “beyond borders.” Travel and migration among the Mekong region countries means that resistance may not stay put in Pailin. A comprehensive control program, not just reliance on treatment, needs to be in place throughout the region.
Fortunately there are groups like the Asia Pacific Malaria Elimination Network (APMEN) that brings countries in the region together to address common and cross-border challenges. APMEN recognizes that, “Elimination requires a different strategy than sustained control,” and is thus, in am important position to help the rest of the world learn innovative approaches to put paid to malaria.
Borders &Community &Research Bill Brieger | 23 Nov 2011
Training and Research needs to support community engagement in malaria elimination
 Gawrie Galappaththy guided a session at the Asia Pacific Malaria Elimination Network’s Community Engagement for Malaria Elimination Workshop that helped participants summarize their group work on training and research to support community participation in malaria elimination. Her report follows:
Gawrie Galappaththy guided a session at the Asia Pacific Malaria Elimination Network’s Community Engagement for Malaria Elimination Workshop that helped participants summarize their group work on training and research to support community participation in malaria elimination. Her report follows:
All the participants were agreed and thought that following training areas are necessary for effective community engagement for malaria elimination. Thoughts about training included key topics and target groups as seen below.
- Advocacy – Advocacy is needed for all level including central, district, village level for all the category of staff
- Partnership with other sectors- specially with the public sector as more than 50% of patients in most of the countries seek treatment from the public sector
- Skills on communication methods – As most of the health personnel is not very much familiar with communication, methods it is important to train all the trainers on communication methods eg -COMBI, materials, participatory approach)
- Resource mobilization- funds as well as personals
- Integration with other diseases – community engagement as an integral part of the health (health package)
- Training for community – training of community on every aspects of malaria
- Strategy developments – most of the malaria programmes in their strategic plans not mentions the involvement of community in malaria elimination. It is important to include this aspect along with key activities
- Skills on Monitoring & Evaluation – most of the countries engaged community for malaria control but lack M&E component. It is important to include M&E as an integral part of the elimination statergy
- Empowerment of community for sustainability of community engagement in malaria elimination
Many research areas were identified by the participants, but need to priority areas depending on funds availability. Examples of priority research issues included …
- Cost effectiveness of engagement of community in malaria elimination
- Improvement of drug compliance specially among migrant workers
- Case studies or documentation of success stories
- Promote treatment seeking behaviour specially in  malaria elimination countries
- KAP studies on malaria especially since perceptions may change as we progress toward elimination
- Role of community in malaria elimination
- Effectiveness of village malaria posts/brigade in malaria elimination
- Role of NGOs/FBOs in malaria using community engagement
- Development and testing of Training modules
- Research on new mechanisms of community engagement for mobile population
- Understand community structure and to identify the mechanism to sustain motivationAchieving synchronous cross boarder community engagement for malaria elimination
 Of particular interest in the region are the training and research needs to identify and test strategies for community engagement between countries – cross-border areas present a special challenge in terms of mobile populations and malaria medicine resistance. APMEN therefore, has to play a major role in advocacy as it is important to increase awareness among politicians, decision makers regarding cross border problems between countries. APMEN can raise a voice in international bodies such as SAARC, ASEAN, BIMSTEC etc.
Of particular interest in the region are the training and research needs to identify and test strategies for community engagement between countries – cross-border areas present a special challenge in terms of mobile populations and malaria medicine resistance. APMEN therefore, has to play a major role in advocacy as it is important to increase awareness among politicians, decision makers regarding cross border problems between countries. APMEN can raise a voice in international bodies such as SAARC, ASEAN, BIMSTEC etc.
Regular meetings in cross-border areas are essential at district/state level between countries eg Bhutan and ASSAM, Bhutan and West Bengal. There is need to address the issue of communication methods between countries taking into consideration ethnicity, language, cultural background etc
Priority Research and training needs for cross-border areas include descriptive studies to understand the migrant pattern, behavior, and risk groups. We also require needs assessment studies including assessments of existing facilities among border populations.
On the final day of the workshop, participants refined and prioritized these research and training topics for follow-up action back home.