Antenatal Care (ANC) &Malaria in Pregnancy Bill Brieger | 18 Nov 2020
Group Antenatal Care to Improve Malaria in Pregnancy & ANC in Geita, Tanzania
 Jasmine Chadewa and colleagues are sharing their work on Group Antenatal Care (GANC): A Baseline Initiative to Improve Malaria in Pregnancy & ANC Indicators. A Case from Geita Tanzania at the virtual 69th Annual Meeting of American Society of Tropical Medicine and Hygiene. See their findings below.
Jasmine Chadewa and colleagues are sharing their work on Group Antenatal Care (GANC): A Baseline Initiative to Improve Malaria in Pregnancy & ANC Indicators. A Case from Geita Tanzania at the virtual 69th Annual Meeting of American Society of Tropical Medicine and Hygiene. See their findings below.
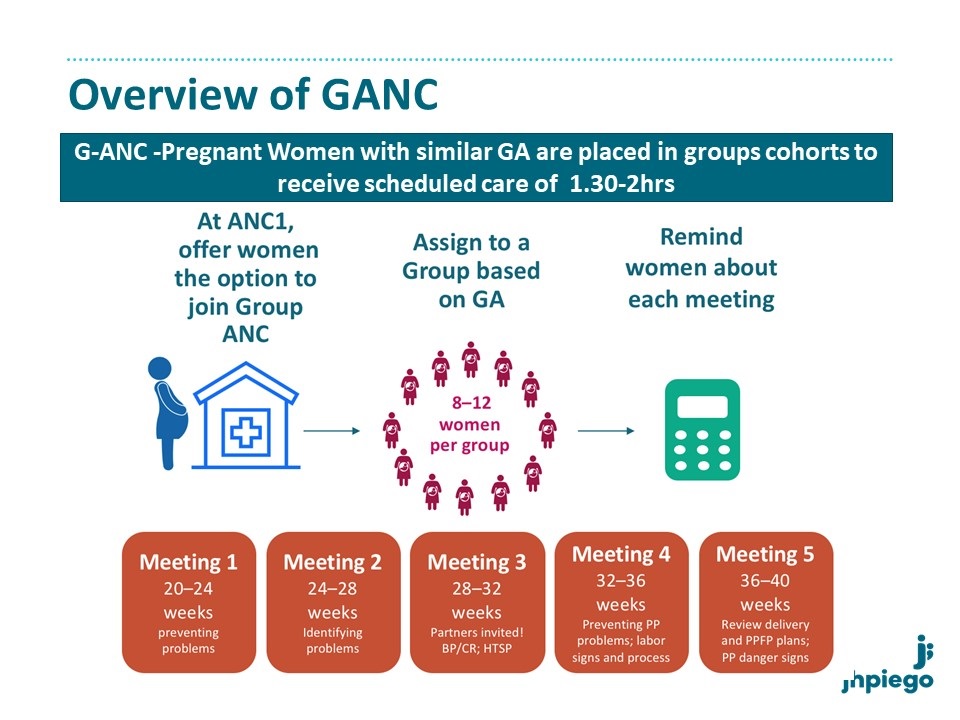
Malaria in pregnancy (MiP) is a major public health concern contributing to poor maternal and newborn health outcomes. Early and frequent Antenatal Care attendance (ANC) could address this problem. Early ANC booking is still low in Tanzania. USAID Boresha Afya and Tanzania Ministry of Health introduced a Group Antenatal Care (GANC) initiative in Geita region where malaria prevalence is high. This model brings 8-15 pregnant women of similar gestational age together for ANC. Group contacts last 1.5-2 hours, and include clinical care, information sharing, and peer support to improve quality of care and women’s engagement, leading to better retention in care.
 Prior to implementation, a baseline cross-sectional household survey was conducted in December 2019 in 40 communities across Geita region. The survey was intended to identify gaps and targets in MiP services delivery which could be addressed through GANC. Women who had delivered a live born infant in the preceding 12 months were included. We interviewed 1111 women; mean age was 27 years. One-third had no education and only 9% had secondary education.
Prior to implementation, a baseline cross-sectional household survey was conducted in December 2019 in 40 communities across Geita region. The survey was intended to identify gaps and targets in MiP services delivery which could be addressed through GANC. Women who had delivered a live born infant in the preceding 12 months were included. We interviewed 1111 women; mean age was 27 years. One-third had no education and only 9% had secondary education.
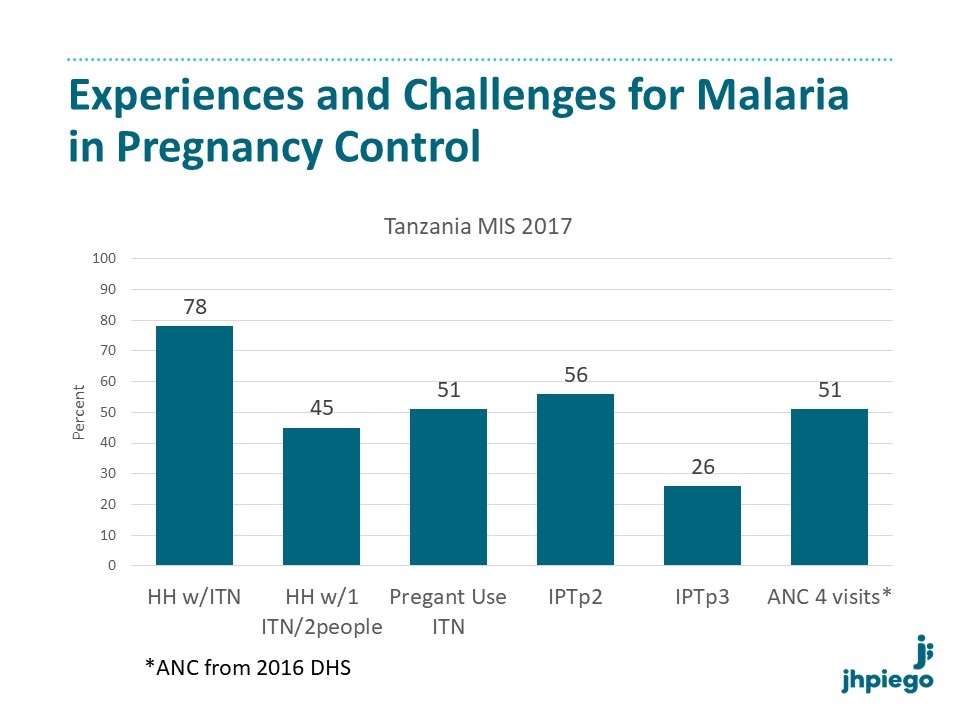 Nearly all 95% of women lived in a house with an Insecticide Treated Net (ITN); 87% reported receiving an ITN during their last pregnancy and 90% reported ITN use on the night before the survey. Nearly all 98% attended ANC at least once, with 17% attending in first trimester. Only 45% attended ?4 visits; 6% of women were stopped by their husbands from attending ANC.
Nearly all 95% of women lived in a house with an Insecticide Treated Net (ITN); 87% reported receiving an ITN during their last pregnancy and 90% reported ITN use on the night before the survey. Nearly all 98% attended ANC at least once, with 17% attending in first trimester. Only 45% attended ?4 visits; 6% of women were stopped by their husbands from attending ANC.
 Median total time spent away from the home for each ANC was 4 hours. 88% received Intermittent Preventive Treatment of malaria in pregnancy (IPTp), with 53% receiving the recommended 3 or more doses. Among those who did not receive IPTp, 42% reported that the provider did not offer it and 25% reported it was not available at the facility. Receipt of other interventions varied: 64% reported that their blood pressure was checked, 95% and 57% had blood and urine samples collected, 74% had received adequate doses of tetanus vaccination, and 94% received iron/folate supplements.
Median total time spent away from the home for each ANC was 4 hours. 88% received Intermittent Preventive Treatment of malaria in pregnancy (IPTp), with 53% receiving the recommended 3 or more doses. Among those who did not receive IPTp, 42% reported that the provider did not offer it and 25% reported it was not available at the facility. Receipt of other interventions varied: 64% reported that their blood pressure was checked, 95% and 57% had blood and urine samples collected, 74% had received adequate doses of tetanus vaccination, and 94% received iron/folate supplements.
We will assess whether GANC improves MiP services as well as quality of ANC care, to promote positive pregnancy outcomes.
Authors and Affiliations
Jasmine Chadewa1, Mary Drake1, Chonge Kitojo2, Ryan Lash3, Stephanie Suhowatsky4, Abdalah Lusasi5, Japhet Simeo6, Goodluck Tesha7, Ruth Lemwayi1, Issa Garimo5, Agnes Kosia1, Alice Christensen1, Rita Noronha1, Zahra Mkomwa7, Naomi Serbantez2, Melkior Assenga1, Erik Reaves8, Samwel Lazaro5, Miriam Kombe9, Alen Kinyina1, Alen Kinyina1, Ally Mohamed5, Gladys Tetteh4, Bill Brieger10, Edward Kenyi4, Annette Almeida1, Julie Gutman3
1USAID Boresha Afya Project -Jhpiego Tanzania, Dar es Salaam, Tanzania, United Republic of, 2President’s Malaria Initiative/United States Agency for International Development, Tanzania, Dar es Salaam, Tanzania, United Republic of, 3Malaria Branch, Division of Parasitic Diseases and Malaria, Center for Global Health, Centers for Disease Control and Prevention, Dar es Salaam, Tanzania, United Republic of, 4Jhpiego Headquarter U.S.A, Baltimore, MD, United States, 5National Malaria Control Program-Tanzania Ministry of Health, Community Development, Gender, Elderly and Children, Dar es Salaam, Tanzania, United Republic of, 6Regional Health Management Team, Dar es Salaam, Tanzania, United Republic of, 7USAID Boresha Afya Project –Path Tanzania, Dar es Salaam, Tanzania, United Republic of, 8President’s Malaria Initiative, Centers for Disease Control and Prevention Tanzania, Dar es Salaam, Tanzania, United Republic of, 9USAID, Dares Salaam, Dar es Salaam, Tanzania, United Republic of, 10Jhpiego Headquarter U.S.A, Dar es Salaam, Tanzania, United Republic of
Antenatal Care (ANC) &CHW &IPTp Bill Brieger | 16 Nov 2020
Increasing Access to Malaria in Pregnancy Services through Community Health Units and Enhanced Supportive Supervision of Community Health Volunteers
 Donald Apat and colleagues address the importance of community health workers and appropriate supervision in their study from Kenya. This was presented today at the 69th Annual Meeting of American Society of Tropical Medicine and Hygiene which is virtual. See their findings below.
Donald Apat and colleagues address the importance of community health workers and appropriate supervision in their study from Kenya. This was presented today at the 69th Annual Meeting of American Society of Tropical Medicine and Hygiene which is virtual. See their findings below.
According to the 2018 Kenya malaria program review, the uptake of malaria in pregnancy interventions by rural communities in Kenya remains low due to late first presentation to antenatal care (ANC), leading to sub-optimal intermittent preventive treatment in pregnancy (IPTp) coverage. Poor healthcare provider-client communication and low investment in advocacy, communication, and social mobilization contribute to late ANC presentation.
 Kenya is using community health volunteers (CHVs) supervised by community health assistants (CHAs) in community health units (CHUs) to increase demand for ANC services and uptake of IPTp but tracking of progress is hampered by a lack of accurate data on the number of estimated pregnancies at the sub-national level and poor household coverage by CHVs at the community level.
Kenya is using community health volunteers (CHVs) supervised by community health assistants (CHAs) in community health units (CHUs) to increase demand for ANC services and uptake of IPTp but tracking of progress is hampered by a lack of accurate data on the number of estimated pregnancies at the sub-national level and poor household coverage by CHVs at the community level.
In July 2019, Impact Malaria supported malaria-endemic Teso South sub-county of Busia county with the reorientation of 354 CHVs (92%) and 14 CHAs (100%), to identify and track pregnant women at the household level within the government established CHUs, provide social and behavior change communication messages, and enhance monthly supervision and reporting by CHAs.
CHVs identified and tracked 917 pregnant women from 32,758 (89.6%) households and identified and referred 273 ANC defaulters. We compared the uptake of IPTp before intervention (January to June 2019) and during the intervention (July to December 2019) using programmatic and Kenya health information system (KHIS) data.
At pre-intervention, 32,898 (90%) households were visited, with 2,160 new ANC visits and 5,342 ANC revisits. During the intervention period, 35,910 (98.3%) households were visited with 1,934 new ANC visits and 5,904 ANC revisits. Uptake of IPTp1 increased from 83.6% to 92.6%; IPTp2 from 73.5% to 87%; and IPTp3 from 51.9% to 75.4%.
Enhanced supervision of CHVs by CHAs to conduct and improve household visits enabled identification and referral of ANC defaulters and contributed to increased IPTp uptake. Supportive supervision and optimal CHU coverage in tracking pregnant women if conducted routinely may provide accurate denominators to track IPTp coverage and inform targeted interventions.
Authors and Affiliations
Donald Apat1, Willis Akhwale1, Moses Kidi1, Edwin Onyango2, James Andati1, Hellen Gatakaa1, Augustine Ngindu1, Lolade Oseni3, Gladys Tetteh3, Daniel Wacira4
1PMI-Impact Malaria, Nairobi, Kenya, 2Department of Health, Busia County, Kenya, 3Jhpiego, Baltimore, MD, United States, 4PMI, Nairobi, Kenya
Antenatal Care (ANC) &IPTp &Malaria in Pregnancy Bill Brieger | 16 Nov 2020
Achieving antenatal care attendance and intermittent preventive treatment in pregnancy in Geita, Tanzania
Ryan Lash and colleagues examined factors associated with achieving antenatal care (ANC) attendance and intermittent preventive treatment in pregnancy (IPTp) and made recommendations in Geita Region, Tanzania, 2019. There findings are being presented at the virtual 69th Annual Meeting of American Society of Tropical Medicine and Hygiene.
Malaria in pregnancy results in an estimated 10,000 maternal and 100,000 infant deaths globally each year. To reduce this burden, the World Health Organization (WHO) recommends pregnant women in high to moderate malaria transmission areas receive at least 3 doses of intermittent preventive treatment in pregnancy (IPTp3) with sulfadoxine-pyrimethamine (SP) starting in the second trimester as part of routine antenatal care (ANC). Tanzania has national coverage goals of 80% coverage for women receiving IPTp3 and at least four ANC visits (ANC4).
 We surveyed women 15-49 years who had given birth in the last 12 months from randomly selected households across 40 communities in Geita Region, Tanzania. ANC attendance and IPTp uptake was recorded from respondent ANC cards if available, or self-reported. Predictors of ANC4 and IPT3 uptake were identified using logistic regression modeling, accounting for clustering and controlling for gravidity.
We surveyed women 15-49 years who had given birth in the last 12 months from randomly selected households across 40 communities in Geita Region, Tanzania. ANC attendance and IPTp uptake was recorded from respondent ANC cards if available, or self-reported. Predictors of ANC4 and IPT3 uptake were identified using logistic regression modeling, accounting for clustering and controlling for gravidity.
Of 1,111 women surveyed, 505 (51.9%) received IPTp3 and 472 (43.4%) achieved ANC4. Among women who achieved ANC4, 295 (62.5%) received IPTp3. IPTp3 was associated with basic knowledge about ANC and IPTp (aOR 2.4, CI 1.9 -3.1), initiating ANC <20 weeks (aOR 1.7, CI 1.3-2.3), waiting at the facility for <120 minutes (aOR 1.4, CI 1.1-1.9), and receiving advice from a health worker about SP (aOR 1.7, CI 1.3-2.2).
ANC4 was associated with better access to care (aOR 1.9, CI 1.3-2.8, for travelling <3.75 km to ANC and aOR 1.9, CI 1.1-2.2, for waiting <90 minutes for the provider), initiating ANC at <20 weeks gestation (aOR 10.7, CI 8.2-14.1), and basic knowledge about ANC and IPTp (aOR 1.4, CI 1.0-1.9). Poor access to care and late initiation of ANC reduced the likelihood that women will attend 4 ANC visits. Knowledge was a predictor of both ANC attendance and IPTp uptake; increasing women’s health literacy may overcome some of the barriers associated with retention in ANC.
New approaches to delivering ANC that focus on improving knowledge and the experience of care among ANC clients could help close coverage gaps for ANC4 and IPTp3 in Tanzania
Authors and Affiliations
R. Ryan Lash(1), Ruth Lemwayi(2), Melkior Assenga(2), Alen Kinyina(2), Annette Almeida(2), Samwel L. Nhiga(3), Lia Florey(4), Chonge Kitojo(5), Erik Reaves(6), Miriam Kombe(5), Ally Mohamed(3), Japhet Simeo(7), Stephanie Suhowatsky(8), Mary Drake(2), Julie Gutman(1) 1.US Centers for Disease Control and Prevention, Atlanta, GA, United States, 2.Jhpiego Tanzania, Dar es Salaam, Tanzania, United Republic of, 3.National Malaria Control Program, Tanzania, Dar es Salaam, Tanzania, United Republic of, 4.US Agency for International Development, Washington, DC, United States, 5.US President’s Malaria Initiative / US Agency for International Development Tanzania, Dar es Salaam, Tanzania, United Republic of, 6.US Centers for Disease Control and Prevention / US President’s Malaria Initiative Tanzania, Atlanta, GA, United States, 7.Regional Medical Office, Geita, Geita, Tanzania, United Republic of, 8.Jhpiego, Baltimore, MD, United States