Antenatal Care (ANC) &CHW &IPTp Bill Brieger | 19 Nov 2021
Changes in ANC Attendance and IPTp Uptake after Introduction of Complimentary Community Interventions
 The TiPToP malaria in pregnancy project of Jhpiego and Unitaid has been aiming to increase coverage of Intermittent Preventive Treatment of malaria in pregnancy. The abstract below shares experiences from Nigeria, one of 4 TiPToP countries, is being presented at the 2021 American Society of Tropical Medicine and Hygiene Annual Meeting. Described are Changes in antenatal care (ANC) attendance and uptake of intermittent preventive treatment of malaria in pregnancy (IPTp) after introduction of community-based distribution of IPTp in three local government areas (LGA) in Nigeria. See Author List below.
The TiPToP malaria in pregnancy project of Jhpiego and Unitaid has been aiming to increase coverage of Intermittent Preventive Treatment of malaria in pregnancy. The abstract below shares experiences from Nigeria, one of 4 TiPToP countries, is being presented at the 2021 American Society of Tropical Medicine and Hygiene Annual Meeting. Described are Changes in antenatal care (ANC) attendance and uptake of intermittent preventive treatment of malaria in pregnancy (IPTp) after introduction of community-based distribution of IPTp in three local government areas (LGA) in Nigeria. See Author List below.
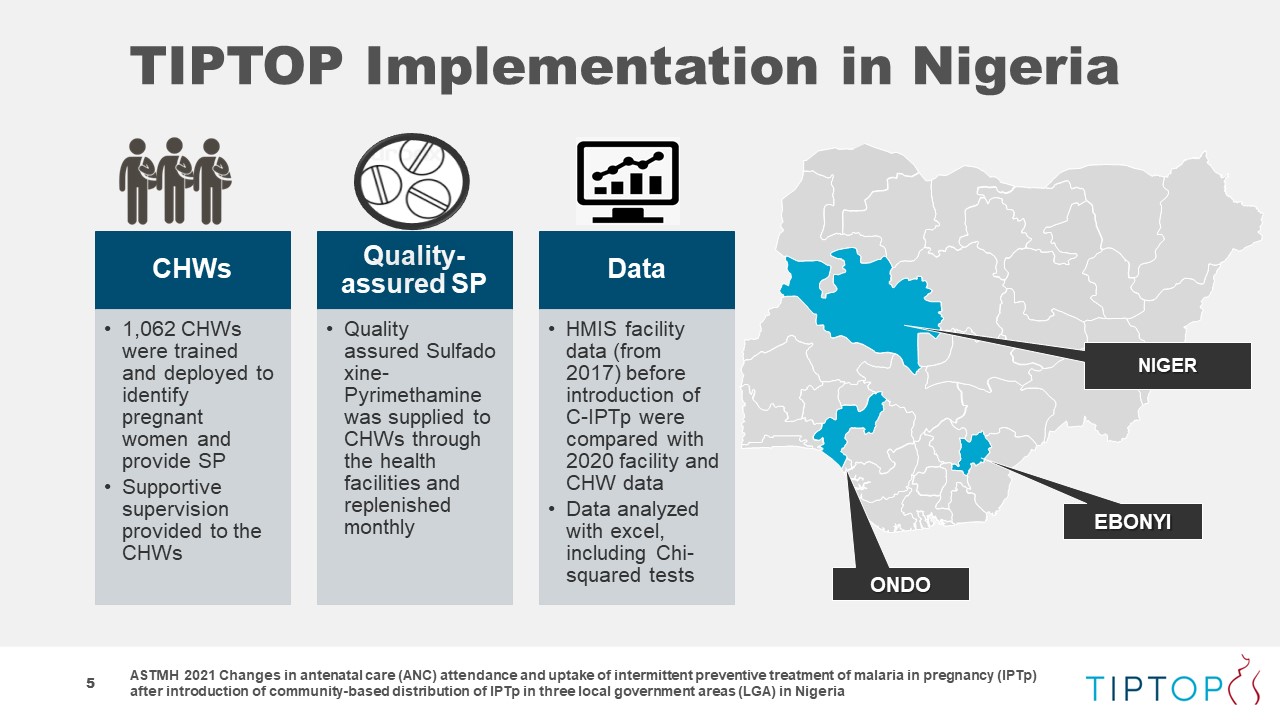
 In Nigeria, community health workers (CHWs) from three LGAs were engaged to introduce community delivery of IPTp (C-IPTp) with quality-assured sulfadoxine-pyrimethamine to prevent malaria. This approach, which complements IPTp delivery during ANC visits, was carried out in Ohaukwu, Akure South, and Bosso LGAs. C-IPTp was introduced in September 2018 in Ohaukwu and in December 2019 in Akure South and Bosso.
In Nigeria, community health workers (CHWs) from three LGAs were engaged to introduce community delivery of IPTp (C-IPTp) with quality-assured sulfadoxine-pyrimethamine to prevent malaria. This approach, which complements IPTp delivery during ANC visits, was carried out in Ohaukwu, Akure South, and Bosso LGAs. C-IPTp was introduced in September 2018 in Ohaukwu and in December 2019 in Akure South and Bosso.
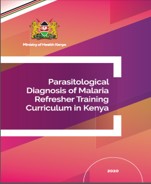
A total of 1,062 CHWs were trained on early identification of pregnant women, referral to ANC, IPTp administration, and use of mobile phones to capture and report data. CHWs conduct household visits, provide malaria health education, refer and encourage pregnant women to attend ANC, and provide IPTp.
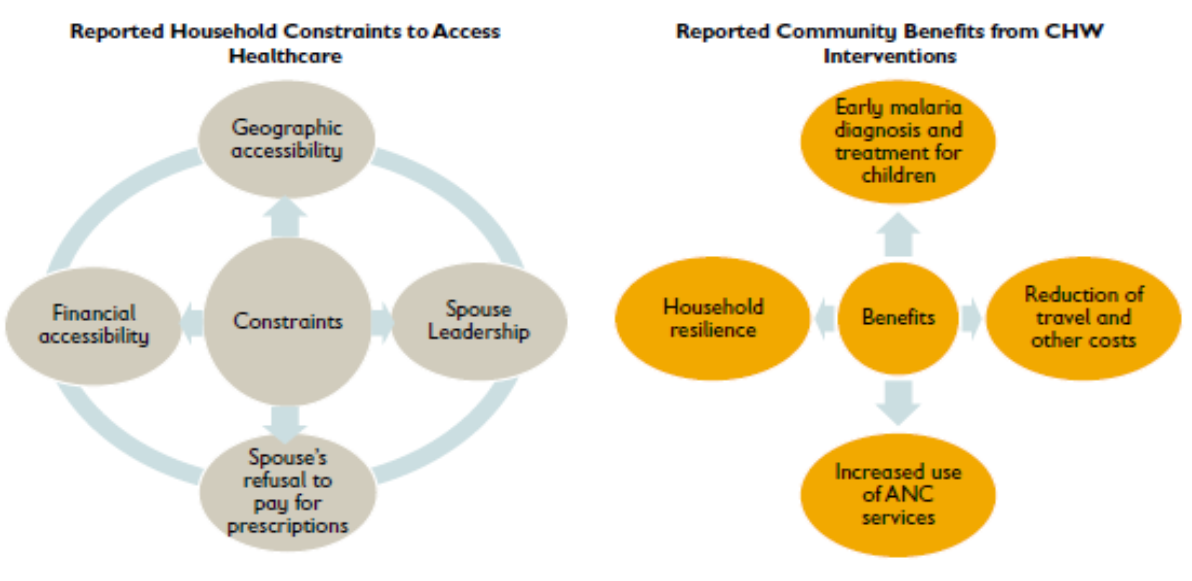
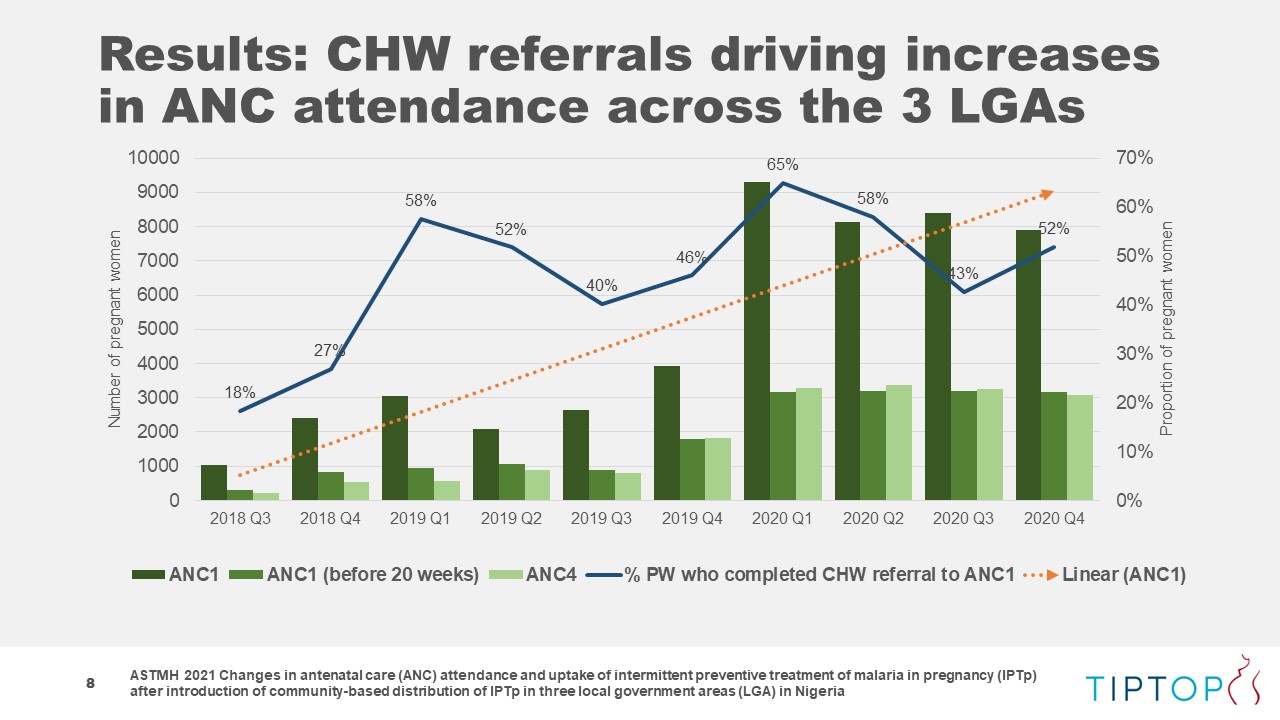
 Routine facility data from 2017 before introduction of C-IPTp were compared with 2020 facility and CHW data to understand the effect of C-IPTp across the LGAs. Before C-IPTp, 43% of the estimated number of pregnant women in these areas attended at least one ANC visit as compared to 57% in 2020 (p<.05).
Routine facility data from 2017 before introduction of C-IPTp were compared with 2020 facility and CHW data to understand the effect of C-IPTp across the LGAs. Before C-IPTp, 43% of the estimated number of pregnant women in these areas attended at least one ANC visit as compared to 57% in 2020 (p<.05).
 Attending at least four ANC (ANC4) visits increased in Ohaukwu by ten percentage points to 29% in 2020 (p<.05). In Akure South, ANC4 remained steady Bosso pre-C-IPTp data on ANC4 visits were of too poor quality to conduct a meaningful analysis. Though this project focused on C-IPTp, it also resulted in statistically significant increases in IPTp distribution during ANC visits.
Attending at least four ANC (ANC4) visits increased in Ohaukwu by ten percentage points to 29% in 2020 (p<.05). In Akure South, ANC4 remained steady Bosso pre-C-IPTp data on ANC4 visits were of too poor quality to conduct a meaningful analysis. Though this project focused on C-IPTp, it also resulted in statistically significant increases in IPTp distribution during ANC visits.
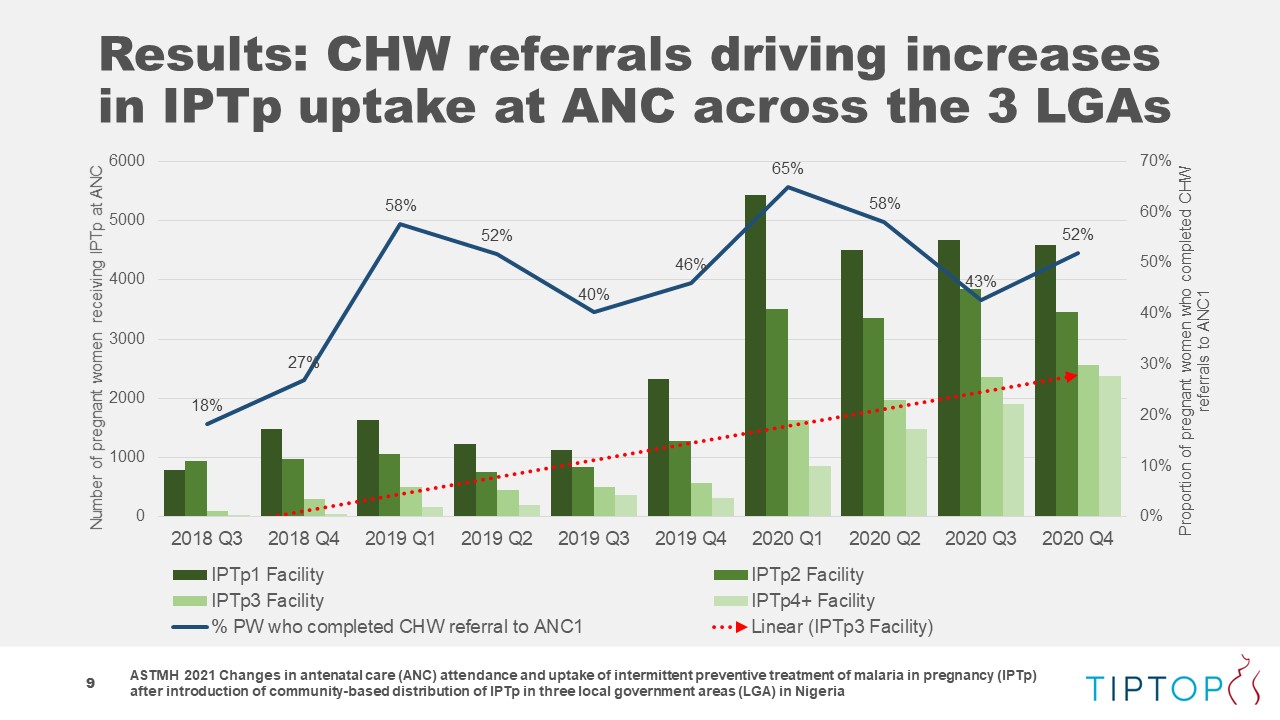
From 2017 to 2020, coverage of IPTp doses 1, 2, and 3 all saw increases across the three sites: IPTp1 increased from 54%?to 57%; IPTp2 from 36% to 42%; and IPTp3 increased 20 percentage points from 5% to 25%. Of pregnant women receiving all doses of IPTp, 39% did so through ANC with 61% receiving IPTp from CHWs.
 These data suggest that in addition to contributing to overall increases in IPTp coverage, C-IPTp may also contribute to increases IPTp delivery in ANC and ANC attendance.
These data suggest that in addition to contributing to overall increases in IPTp coverage, C-IPTp may also contribute to increases IPTp delivery in ANC and ANC attendance.
AUTHORS LIST:
Herbert Enyeribe Onuoha1, Bartholomew Odio1, Christina Maly2, Lawrence Nwankwo3, Folayan Waheed Adewale4, Elizabeth Njoku1, Oniyire Adetiloye1, Orji Bright1, Emmanuel Dipo Otolorin1, Elaine Roman2 — 1Jhpiego, Abakaliki, Nigeria, 2Jhpiego, Baltimore, MD, United States, 3Ebonyi State Ministry of Health, Abakaliki, Nigeria, 4Ondo State Ministry of Health, Alagbaka, Akure, Nigeria