Guest Blog Posting: Meike Schleiff is a DrPH Candidate in International Health Systems at JHSPH. She has a background in agriculture and natural resources and holds a Master of Science in Public Health (MSPH) from JHSPH as well. Meike is the Founder and Executive Director of The GROW Project (www.thegrowproject.org) based in West Virginia and working in communities in and around Cap Haitien, Haiti.
The Declaration of Alma Ata (WHO, 1978) sets out a vision for equitable, multi-sectoral, and locally relevant, effective, and affordable health care in holistic terms. The role the community is central, and the local health workers and primary level of contact with the health system create the “central function and main focus” on which other development and levels of care can be built. Ken Newell wrote eloquently in Health by the People (1975) about the importance of “self-sufficiency” of communities to the greatest extent feasible as being the most cost-effective, appropriate, and immediate option to further health.

Mac Henri, a young local leader, heads a cholera information session in the Baptist Church at Soufriere, Haiti.
In 2009, Paul Freeman, Henry Perry and others conducted a Review of Community-Based Primary health Care (CBPHC) approaches to achieving the MDG for child health. Although many projects in the review effectively incorporated a community-based component and delivered Primary Health Care (PHC) interventions, the level of involvement and leadership of the community varied and was difficult to ascertain and may not have been the main reason for conducting the intervention outside of a facility. The findings of the review (which are ongoing) show the difficulty of finding evidence of empowerment and leadership given to communities. The projects seem to have overall positive affects, but there a wide range of levels of engagement and community roles.

A local woman explains to Meike and a Ministry of Health representative where the different drinking water sources (mostly springs and the river) for her neighborhood are. She is helping us decide on the best location for a community water system that will protect and treat a water system against cholera and other water-borne diseases.
Several publications from Africa use language of Community-Directed Initiatives (CDIs) as a model built on PHC principles in order to deliver health interventions in communities. In the CDI model, communities are the driving force of planning and implementing the interventions, and gain a sense of ownership and motivation far beyond financial gains that help ensure sustainability (The CDI Study Group, 2010). This model has been used effectively in Nigeria, Cameroon and Uganda (Ajiyi et al, 2013 & The CDI Study Group, 2010).
In my experience, what is called community-based versus community-directed in the literature can be difficult to differentiate. However, as Dr. Carl Taylor aptly pointed out, empowerment—and I would venture to include leadership and true initiative by communities—can easily be recognized because “you know it when you see it”. When a community feels heard and is effectively engaged, a process to fulfill the original vision of PHC from Alma Ata is possible.
To me, the central argument that spans both CBPHC and CDI is that building capacity and leadership are essential. This can be done within local facilities as well as in people’s homes. Conversely, so-called community projects can still be very much driven by outside agendas and voices. Volunteers, resources, and data should be accountable and shared first with the community and secondly with supervisors. Both are important, but too often in Public Health the latter is only direction of knowledge-sharing to which funds, time, and patience are allocated.
To conclude, terminology can easily become blurred and can be used for a variety of different levels of engagement, leadership, and capacity-building for communities. The importance to me is whether the community has a voice and some level of leadership, control, and responsibility of the destiny of their health and well-being.
————————

The Community Council of Soufriere, Haiti meets along with some spectators to problem-solve and discuss the most important priorities for health–beyond cholera–in their community. The Council includes a Ministry representative and the local judge, but is mostly composed of religious and educational leaders, the local Agent Sante (community health workers), and the nurses who staff the cholera treatment center.
References: Ajayi, I., Jegede, A., Falade, C., Sommerfeld, J. (2013). Assessing Resources for Implementing A Community Directed Intervention (CDI) Strategy for Providing Multiple Health Interventions in Urban Communities in Southwestern Nigeria: A Qualitative Study. Infectious Diseases of Poverty, 2:25. (http://www.ncbi.nlm.nih.gov/pubmed/24156481)
Freeman, P., Perry, H. B.,, Gupta, S.K., Rassekh, B. (2009). Accelerating Progress in Achieving the Millennium development Goal for Children Through Community-Based Approaches. Global Public Health: An International Journal for Research, Policy and Practice, 7:4, 400-419. (http://www.ncbi.nlm.nih.gov/pubmed/19890758)
Newell, K. (1975). Health by The People. World Health Organization, Geneva, Switzerland.
The CDI Study Group. (2010). Community-Directed Interventions Against Health Problems in Africa: Results of a Multi-Country Study. Bulletin of the World Health Organization. 88:509-518. (http://www.who.int/bulletin/volumes/88/7/09-069203/en/)
WHO. (1978). Declaration of Alma Ataz: International Conference on Primary Health Care, Alma-Ata, USSR, 6-12 September, 1978.
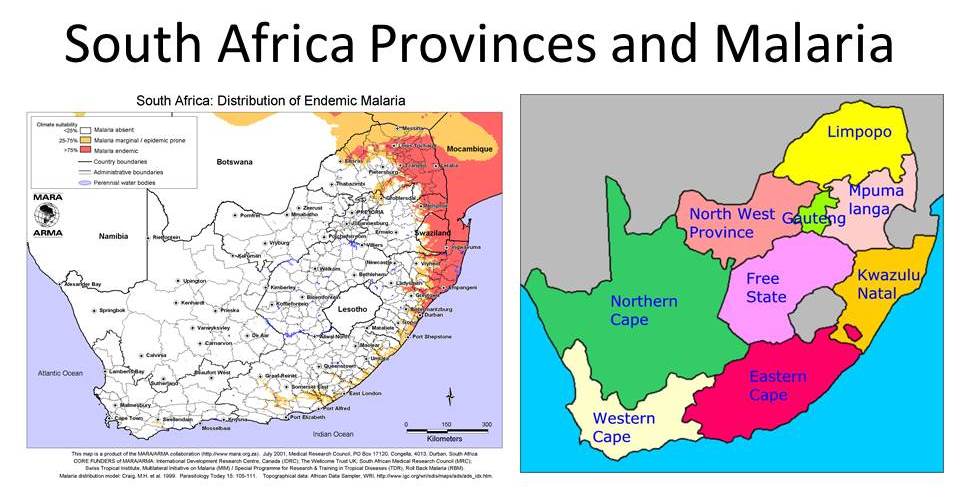 Seven of the 10 poorest districts in the country fall in two of these endemic provinces, Limpopo and KZN. The two districts with the highest HIV prevalence are in Mpumalanga and KZN, and those two provinces themselves have the highest HIV prevalence among all the provinces.
Seven of the 10 poorest districts in the country fall in two of these endemic provinces, Limpopo and KZN. The two districts with the highest HIV prevalence are in Mpumalanga and KZN, and those two provinces themselves have the highest HIV prevalence among all the provinces.