Case Management &Health Workers &Supervision Bill Brieger | 21 Nov 2019 10:19 am
The Effect of Optimized Supportive Supervision on Improved Quality of Malaria Services in Liberia
 Colleagues from USAID’s Flagship Maternal and Child Survival Program are presenting poster 415 at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene. They include Lauretta N. Se, MPH; George Toe Jr., MPH; Anne Fiedler, MPH; Thomas Hallie; Mantue Reeves, MSc; Birhanu Getahun, MD, MPH; Lolade Oseni, MD, MPH; Gladys Tetteh, MD, MPH. They have shared key points from their presentation below.
Colleagues from USAID’s Flagship Maternal and Child Survival Program are presenting poster 415 at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene. They include Lauretta N. Se, MPH; George Toe Jr., MPH; Anne Fiedler, MPH; Thomas Hallie; Mantue Reeves, MSc; Birhanu Getahun, MD, MPH; Lolade Oseni, MD, MPH; Gladys Tetteh, MD, MPH. They have shared key points from their presentation below.
Background
 Malaria prevalence in children <5 years is 45% (LMIS, 2016), with regional variations with the highest in South-Eastern regions of the country (69%). Malaria accounts for about 42 % of all clinical consultations (2013 Liberia health facility survey).
Malaria prevalence in children <5 years is 45% (LMIS, 2016), with regional variations with the highest in South-Eastern regions of the country (69%). Malaria accounts for about 42 % of all clinical consultations (2013 Liberia health facility survey).
The U.S. President’s Malaria Initiative (PMI) has been committed to supporting the MOH strategy since 2008 when it began working in three out of fifteen malaria-affected counties. PMI prioritizes support to CHTs in their responsibility of directly managing the local health systems and providing oversight for efficient malaria service delivery.
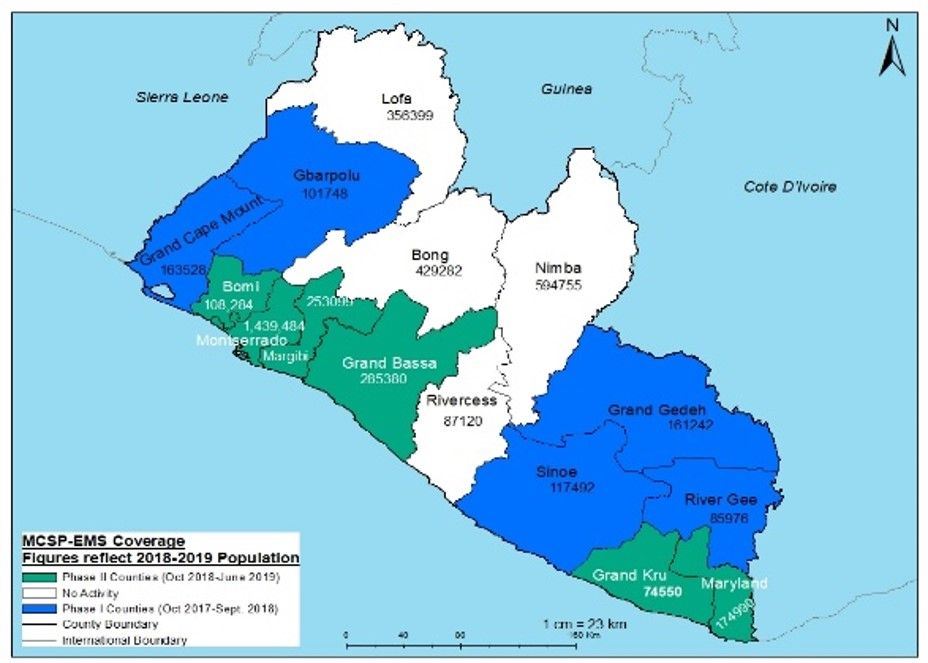
 In 2017 and 2018 PMI through the MCSP/EMS project expanded support to 11 counties (5 phase 1 and 6 phase II) in Liberia, focusing on malaria case management and malaria in pregnancy interventions. To improve the quality of malaria services in Liberia, MCSP/EMS in collaboration with CHT implemented optimized supportive supervision of health workers.
In 2017 and 2018 PMI through the MCSP/EMS project expanded support to 11 counties (5 phase 1 and 6 phase II) in Liberia, focusing on malaria case management and malaria in pregnancy interventions. To improve the quality of malaria services in Liberia, MCSP/EMS in collaboration with CHT implemented optimized supportive supervision of health workers.
Methodology
 At the beginning of each phase (2017 and 2018), MCSP/EMS conducted an organizational capacity assessment of the CHTs/DHTs. One key gap identified was the inconsistent and low quality of the supportive supervision of health facilities by ALL levels of the health system. Expected supervision schedules are:
At the beginning of each phase (2017 and 2018), MCSP/EMS conducted an organizational capacity assessment of the CHTs/DHTs. One key gap identified was the inconsistent and low quality of the supportive supervision of health facilities by ALL levels of the health system. Expected supervision schedules are:
- National level (25% of HFs , semi-annually)
- County level (75% of HFs , quarterly)
- District level (100% of HFs, monthly)
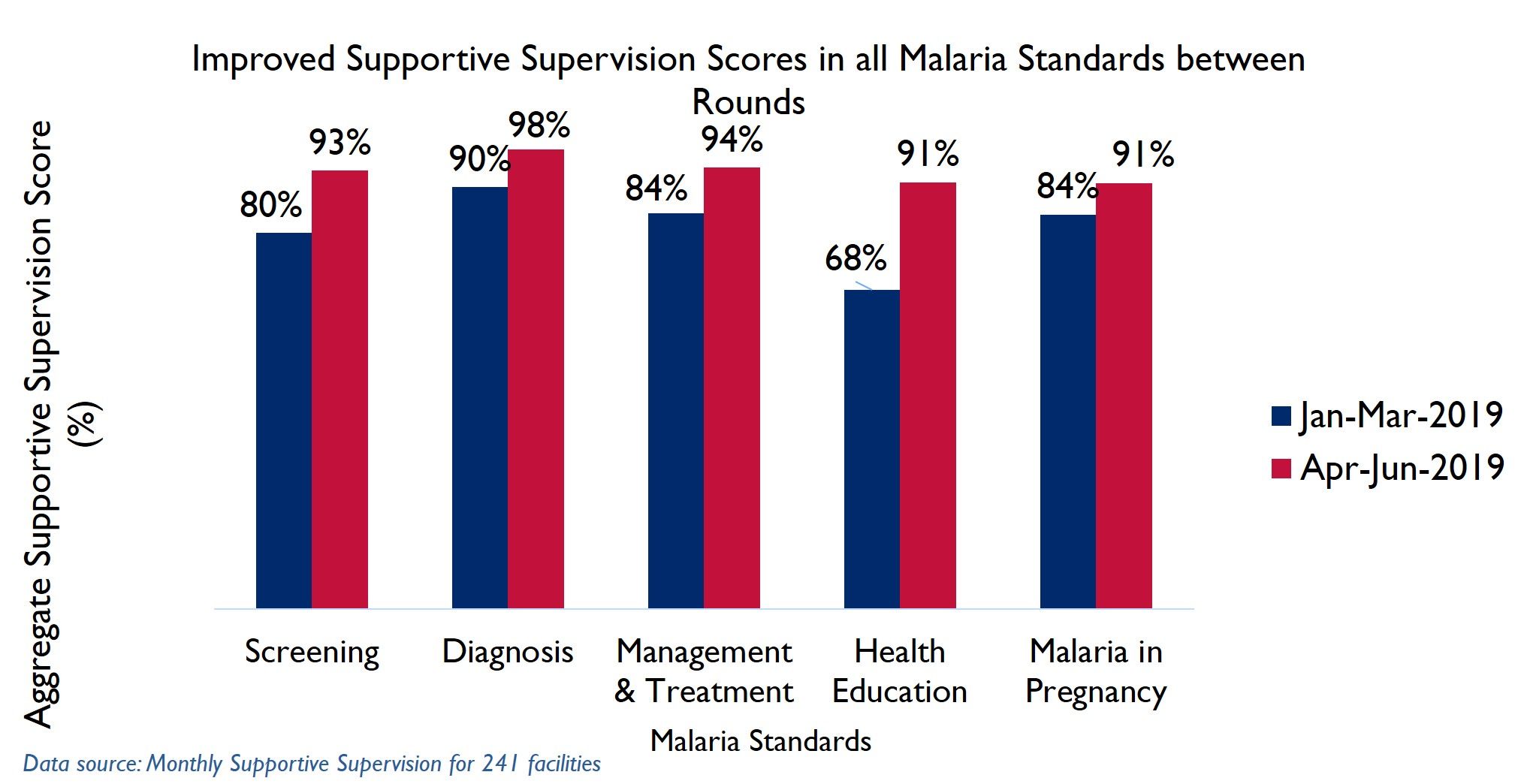
MCSP/EMS worked with Ministry of Health supervisors to employ an optimized supportive supervision program for facility health workers using the updated Joint Integrated Supportive Supervision Tool. The tool has five malaria standards:
- Screening (with 5 verification criteria)
- Diagnosis (with 3 verification criteria)
- Management and Treatment (with 4 verification criteria)
- Health Education (with 2 verification criteria)
- Malaria in Pregnancy (with 6 verification criteria)
 The assessment team provided prior information to the facility staff about the supervision visit during the entry meetings. The supervision team consisted of county, district health team supervisors and MCSP/EMS staff. During the supervision the assessment of malaria standards was done using direct observation, record reviews, and simulation, after which each standard was scored.
The assessment team provided prior information to the facility staff about the supervision visit during the entry meetings. The supervision team consisted of county, district health team supervisors and MCSP/EMS staff. During the supervision the assessment of malaria standards was done using direct observation, record reviews, and simulation, after which each standard was scored.
JISS: Process and Benefits
 The ultimate goal of supportive supervision is to improve the quality of health services provided at the health facility. During each supervision visit, supervisors:
The ultimate goal of supportive supervision is to improve the quality of health services provided at the health facility. During each supervision visit, supervisors:
- Provided on-the-job training, mentoring and coaching on identified gaps
- Reinforced the review of data and its use for program improvement
- Developed an action plan from gaps identified and discussed remedial actions through follow-up
- Initiated subsequent supervision visits based on previous action plans
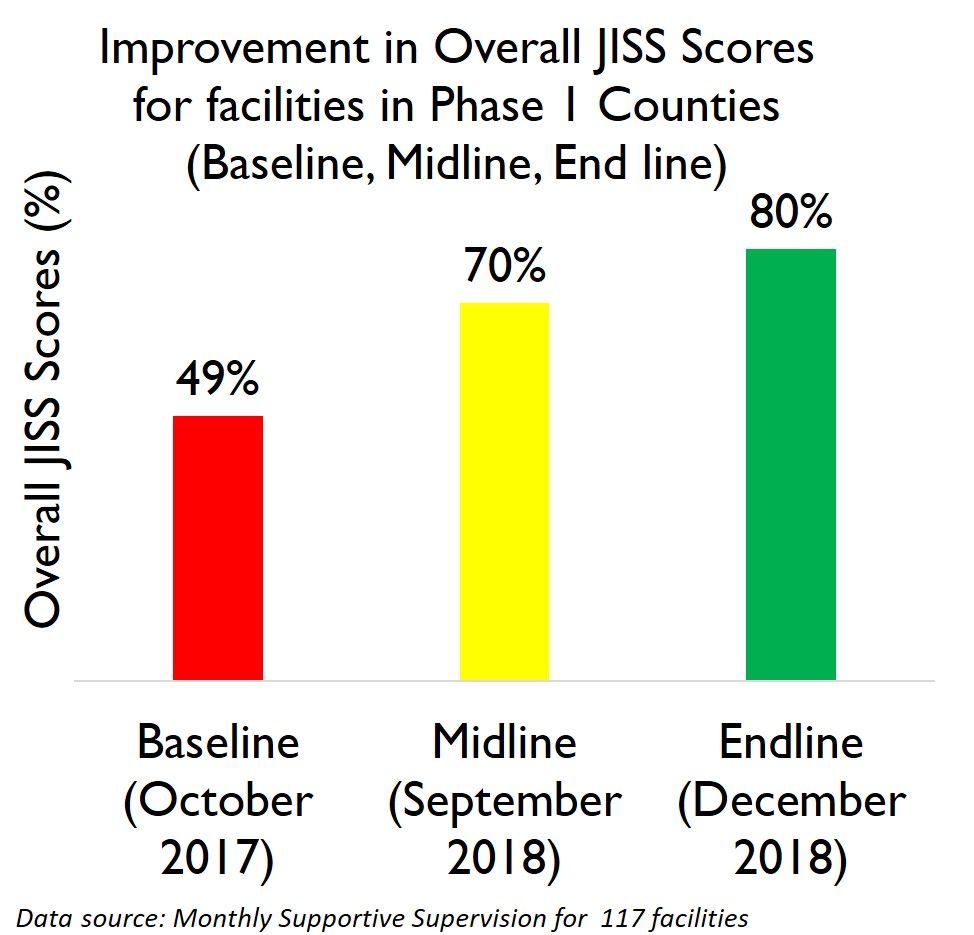
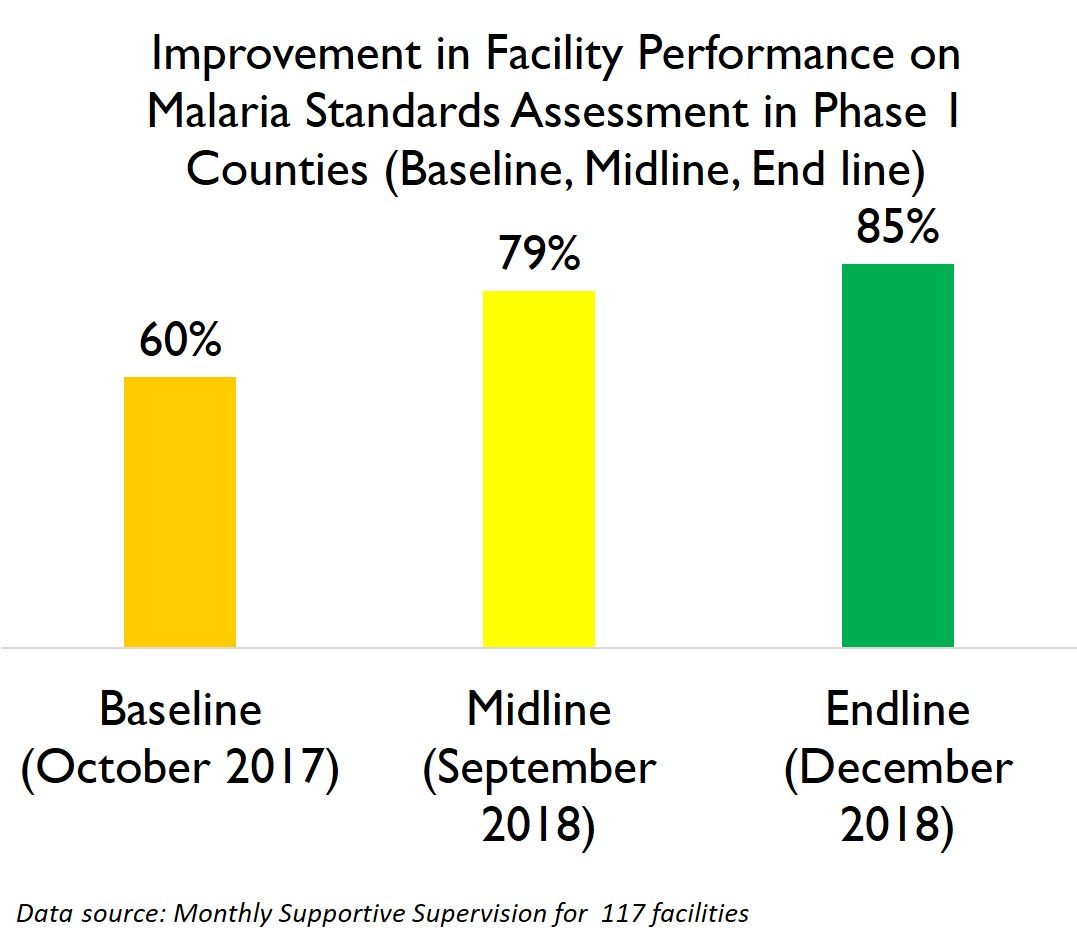 The Improved Performance on Joint Integrated Supportive Supervision (JISS) and Malaria Standards Assessment at 117 health facilities in the 5 Phase 1 Counties is seen in the attached charts.
The Improved Performance on Joint Integrated Supportive Supervision (JISS) and Malaria Standards Assessment at 117 health facilities in the 5 Phase 1 Counties is seen in the attached charts.
Lessons and Conclusions
Training of district and county supervisors in the updated JISS tool improved the quality of supervision and data. Provision of updated MIP and case management guidelines to both facility staff and supervisors, coupled with training, improved adherence to standards Action plans developed during supervision visits helped facilities track their own progress and instill sustained ownership of data and solutions Providing the county and district supervisors the opportunity to lead the supportive supervision planning and execution promoted leadership and ownership among these leaders.
 The optimized supportive supervision and mentoring visits fostered health worker adherence to malaria protocols thereby contributing to measurable improvements in meeting and sustaining malaria standards and compliance. MCSP is sharing the lessons learned in fostering quality improvement from targeted supportive supervision of health care workers to scale up and improve the quality of malaria services delivery in Liberia.
The optimized supportive supervision and mentoring visits fostered health worker adherence to malaria protocols thereby contributing to measurable improvements in meeting and sustaining malaria standards and compliance. MCSP is sharing the lessons learned in fostering quality improvement from targeted supportive supervision of health care workers to scale up and improve the quality of malaria services delivery in Liberia.
Challenges and Recommendations
Most of the county and districts supervisors who were part of the JISS team had not been trained on the revised JISS tools in the EMS supported counties before the start of the project. Supportive supervision is greatly hampered by inadequate and untimely budgetary allocations by the Government of Liberia to the counties, which results in infrequent supervisory visits to the facilities and affects the quality
of services.
 Empowerment of DHT and CHT supervisors: To implement optimized and effective supportive supervision to health facilities, DHTs/CHTs need to be equipped with updated tools, provided mentoring and coaching skills, and timely provision of financial and logistical support. There is need for regular targeted and timely mentoring and coaching of facility staff to improve adherence standards.
Empowerment of DHT and CHT supervisors: To implement optimized and effective supportive supervision to health facilities, DHTs/CHTs need to be equipped with updated tools, provided mentoring and coaching skills, and timely provision of financial and logistical support. There is need for regular targeted and timely mentoring and coaching of facility staff to improve adherence standards.
—–
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID) under Cooperative Agreement No. AID-624-A-13-00010 and the President’s Malaria Initiative (PMI).
The contents are the responsibility of the authors and do not necessarily reflect the views of USAID, PMI or the United States Government.