Children &Communication Bill Brieger | 29 Oct 2015
Seasonal Malaria Chemoprevention Implementation in Senegalese Children
 Dr Mamadou L Diouf and colleagues[1] from the National Malaria Control Program, Dakar Senegal and the President’s Malaria Initiative/USAID, Dakar, Senegal presented their experiences with Seasonal Malaria Chemoprevention among children aged 3-120 months in four southern regions of Senegal at the 64th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings are outlined below.
Dr Mamadou L Diouf and colleagues[1] from the National Malaria Control Program, Dakar Senegal and the President’s Malaria Initiative/USAID, Dakar, Senegal presented their experiences with Seasonal Malaria Chemoprevention among children aged 3-120 months in four southern regions of Senegal at the 64th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings are outlined below.
Malaria is major cause of disease and death in infants and children, with seasonal transmission, highest in the southern and eastern regions which are the wettest areas. SMC is administration of a complete treatment course of AQ+SP at monthly intervals to a maximum of 4 doses during the malaria transmission season to children aged between 3 and 59 months in areas of highly seasonal malaria transmission (where both drugs retain sufficient antimalarial efficacy).
 Target areas for implementation are areas where more than 60% of clinical malaria cases occur within a maximum of 4 months, the clinical attack rate of malaria is greater than 0.1 attack per transmission season in the target age group, and AQ+SP remains efficacious (>90% efficacy).
Target areas for implementation are areas where more than 60% of clinical malaria cases occur within a maximum of 4 months, the clinical attack rate of malaria is greater than 0.1 attack per transmission season in the target age group, and AQ+SP remains efficacious (>90% efficacy).
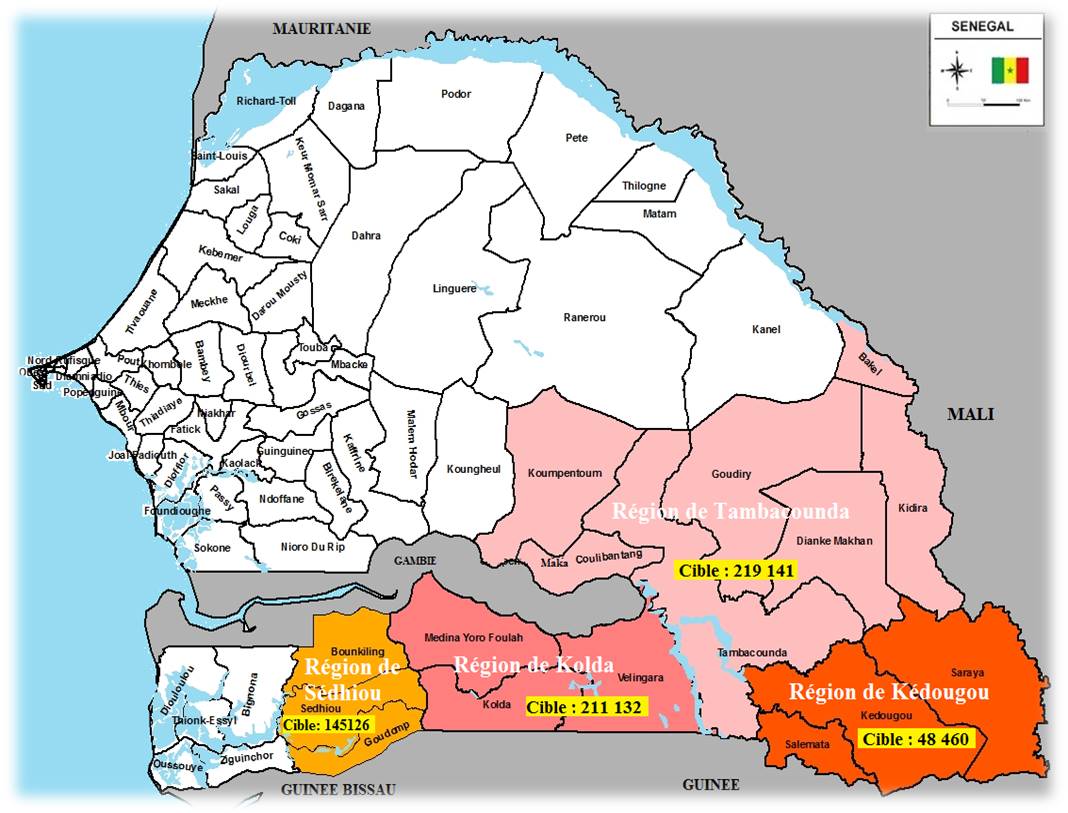
Adoption of SMC in 2013 as a new intervention in malaria control policy. Four south-eastern regions eligible according to WHO criteria for SMC (Tambacounda, Kédougou, Sédhiou and Kolda) chosen
The poster presented Senegal’s experience implementing SMC and focuses particularly on process, challenges and lessons learned. Available information generated from the national SMC implementation guidelines, technical documents, field activity reports, and SMC impact evaluation survey were reviewed.
The medication distribution strategy relied on a door to door campaign strategy with community volunteers. On the first day, the volunteers, trained by health workers, administer drugs to the children under surveillance of their mothers or guardians. For the 2 remaining days, mothers administer the medication.
 In 2014, the SMC Campaign was conducted in the four regions for three months covering the high transmission season (August, September, October, and November). Kedougou, was the only region that conducted 2 SMC rounds as it started implementing in 2013.
In 2014, the SMC Campaign was conducted in the four regions for three months covering the high transmission season (August, September, October, and November). Kedougou, was the only region that conducted 2 SMC rounds as it started implementing in 2013.
The target was extended to children from 3 to 120 months (624,139 estimated in target age group). This age group extension, compared with WHO recommendations (3 to 60 months,) was based on shift of vulnerability towards the ages from 60 to 120 months shown by the epidemiologic data on malaria morbidity in Senegal.
Administrative coverage rates for the 3 passages respectively was 98.6%, 97.9% and 98.0%. Information was obtained from the SMC impact evaluation survey in the south of Senegal, 2015 July by Dr JL Ndiaye.
 Key interventions and process began with the National and regional Steering Committees involving NMCP, health staff, donors/partners and researchers. There was development and update of tools and materials (guidelines, planning forms, data collection and analysis support. Training of staff took place at all levels and operational actors
Key interventions and process began with the National and regional Steering Committees involving NMCP, health staff, donors/partners and researchers. There was development and update of tools and materials (guidelines, planning forms, data collection and analysis support. Training of staff took place at all levels and operational actors
Early field planning was held with staff at regional and district level: identification of activities, dates, estimation of household/child targets, estimation of resources needed (budgets, HR, logistics, etc.). Early delivery of drugs, tools, supports was ensured to be available at health post level at least 1 week before the 1st campaign day.
Rigorous selection of volunteers and supervisors was based on specific criteria. Develop communications activities took place at least 2 weeks before and during the campaign period focusing on SMC gains, HH census, administration by mothers for the 2 remaining days, and possible side effects.
 Campaign roll out included supervision of the process at the districts and health posts (organization model, administration). There was mobilization of logistics for transportation of volunteers, drugs, and materials. Day to day monitoring took place with regional debriefing to analyze data from districts, geographical progression, target coverage progression and identify issues and challenges. Daily electronic distribution of “SMC bulletin” to health staff and partners helped to disseminate information on districts performances.
Campaign roll out included supervision of the process at the districts and health posts (organization model, administration). There was mobilization of logistics for transportation of volunteers, drugs, and materials. Day to day monitoring took place with regional debriefing to analyze data from districts, geographical progression, target coverage progression and identify issues and challenges. Daily electronic distribution of “SMC bulletin” to health staff and partners helped to disseminate information on districts performances.
Post campaign evaluation took place at all levels: workshops for sharing and validating data and information, identification of key issues, lessons learned, and formulation of recommendations to improve future campaigns. Local health agents, NMCP staffs, partners and authorities were involved.
Spontaneous pharmacovigilance system tracked and treated side effects. This consisted of distribution of yellow cards to health facilities, case notification by health agents, availability of a side effects line listing, and immediate and free-of-charge case management.
The following key challenges were faced:
- Correct availability of drugs and tools at health posts
- Complete coverage of all households and children
- Completion of 2nd and 3rd doses by guardians of children
- Availability of children and guardians during harvest period and class time
- Comprehensive communication for population particularly in possible occurrence of side effects
- Case management of side effects free of charge
- Availability and promptness of data
- Long term logistic availability
 Finally there were some outstanding questions. Can we switch SMC from campaign to routine system at health post level? Can we expand SMC to other regions and with what targets? Also, can we improve formulation and taste of drugs for enhancing children’s compliance?
Finally there were some outstanding questions. Can we switch SMC from campaign to routine system at health post level? Can we expand SMC to other regions and with what targets? Also, can we improve formulation and taste of drugs for enhancing children’s compliance?
Financial support: This work was made possible through support provided by the United States President’s Malaria Initiative, and the U.S. Agency for International Development, under the terms of an Interagency Agreement with the Centers for Disease Control and Prevention (CDC). The opinions expressed herein are those of the authors and do not necessarily reflect the views of the U.S. Agency for International Development or the Centers for Disease Control and Prevention.
[1] Dr Mamadou L Diouf, Mr Medoune Ndiop, Dr Mady Ba, Dr Ibrahima Diallo, Dr Moustapha Cisse, Dr Seynabou Gaye, Dr Alioune Badara Gueye, Dr Mame Birame Diouf