Case Management &Children &Mortality Bill Brieger | 22 Nov 2019 07:26 am
Prioritizing Facilities for Malaria Case Management Training In the Era of Limited Resources
 Presenting at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene are James Sarkodie, Amos Asiedu1 Eric LaFary, Richard Dogoli, Raphael Ntumy, Lolade Oseni, and Gladys Tetteh who are sharing experiences on “Prioritizing Facilities for Malaria Case Management Training In the Era of Limited Resources”. The authors are affiliated with the PMI Impact Malaria (IM) Project and Jhpiego Baltimore. Below are their findings.
Presenting at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene are James Sarkodie, Amos Asiedu1 Eric LaFary, Richard Dogoli, Raphael Ntumy, Lolade Oseni, and Gladys Tetteh who are sharing experiences on “Prioritizing Facilities for Malaria Case Management Training In the Era of Limited Resources”. The authors are affiliated with the PMI Impact Malaria (IM) Project and Jhpiego Baltimore. Below are their findings.
Ghana has made significant recent improvements in malaria control, reducing malaria deaths by 70% (1565 in 2015 to 468 in 2018) with a corresponding decline in under-5 malaria case fatality rate (CFR) from 0.51% to 0.19%. However, significant geographical variations in malaria morbidity and mortality persist and to achieve greater impact, a one-size fits all training approach may no longer be the most effective option.
The training aimed to prioritize facilities for refresher malaria case management training by the US President’s Malaria Initiative-funded Impact Malaria Project in collaboration with Ghana Health Service through systematic evidence-based criteria informed by quantitative and qualitative data. The team gathered information using routine health management information system (HMIS) data from October 2017 to September 2018 including total malaria admissions, malaria deaths malaria case fatality rates were determined for all districts in respective regions.
Districts with high burden malaria mortality and morbidity were ranked using a Pareto chart. Districts with CFRs above the regional average were also identified.
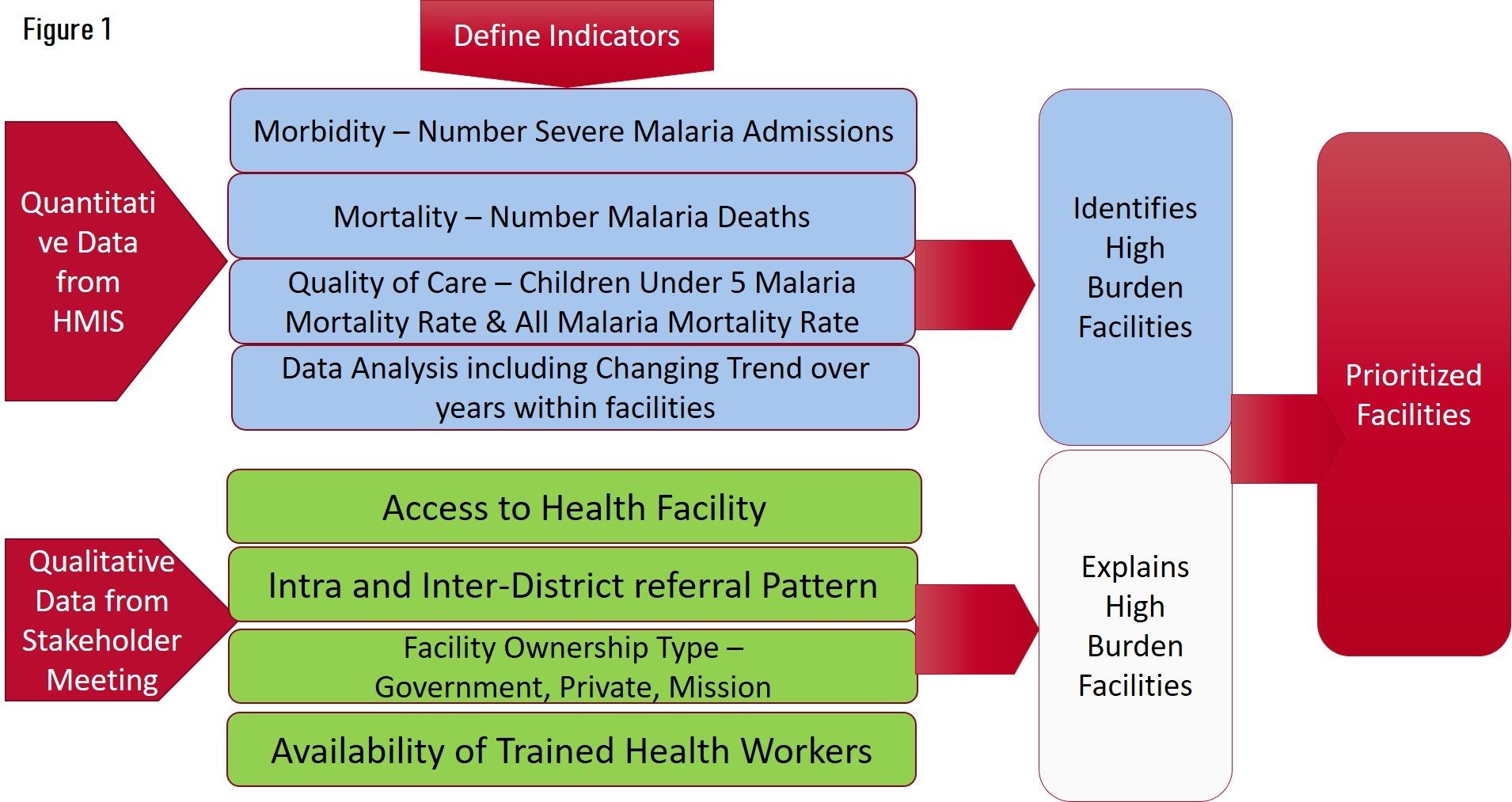 Assessed qualitative data including facility referral patterns, access, and ownership (government, faith-based, private) to explain the observed findings. Information used by Regional health management teams to prioritize districts and facilities for additional malaria case management training focusing on assessment, treatment and management of complications, effective monitoring and using quality improvement methods to identify change ideas to test to improve malaria case management. Figure 1 shows the Scheme of approach to prioritizing facilities for Intervention.
Assessed qualitative data including facility referral patterns, access, and ownership (government, faith-based, private) to explain the observed findings. Information used by Regional health management teams to prioritize districts and facilities for additional malaria case management training focusing on assessment, treatment and management of complications, effective monitoring and using quality improvement methods to identify change ideas to test to improve malaria case management. Figure 1 shows the Scheme of approach to prioritizing facilities for Intervention.
Analysis of Routine HMIS data for FY-2018 reveals 37 Districts accounted for 33.9% of all districts in the 5 IM Target Regions & 14.2% all Districts in Ghana. There were 183 Malaria Deaths. Fiudings also observed that 90.1% all Malaria deaths in 5 IM Target Regions, and 39.1% of all Malaria deaths in Ghana
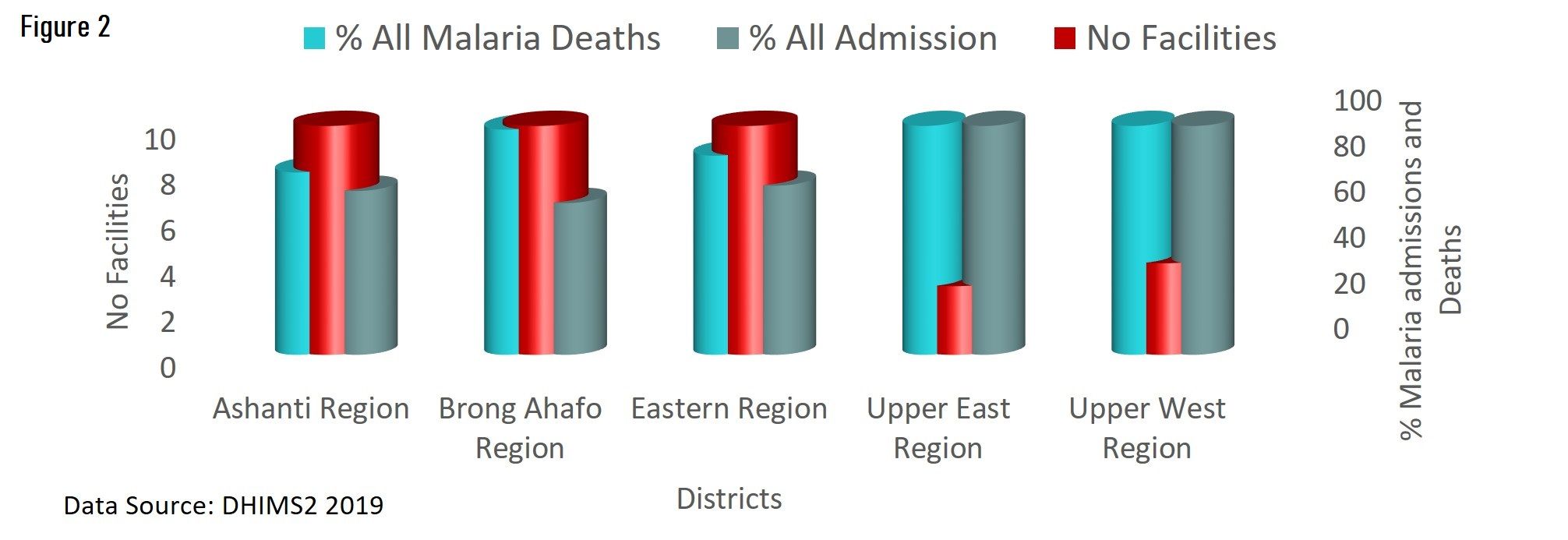 A number of districts had child case fatality rates above the regional average. The Districts with under-5 malaria CFR above the regional average were Ashanti Region (AR) – 31%, , Brong Ahafo Region (BAR) – 28%, Eastern Region (ER) – 31% , Upper East Region(UER) – 15% and Upper West Region (UWR) – 27%. Figure 2 shows the Proportion of Malaria Admissions And Mortality Attributable to TOP 10 Facilities In Target Regions – FY-19
A number of districts had child case fatality rates above the regional average. The Districts with under-5 malaria CFR above the regional average were Ashanti Region (AR) – 31%, , Brong Ahafo Region (BAR) – 28%, Eastern Region (ER) – 31% , Upper East Region(UER) – 15% and Upper West Region (UWR) – 27%. Figure 2 shows the Proportion of Malaria Admissions And Mortality Attributable to TOP 10 Facilities In Target Regions – FY-19
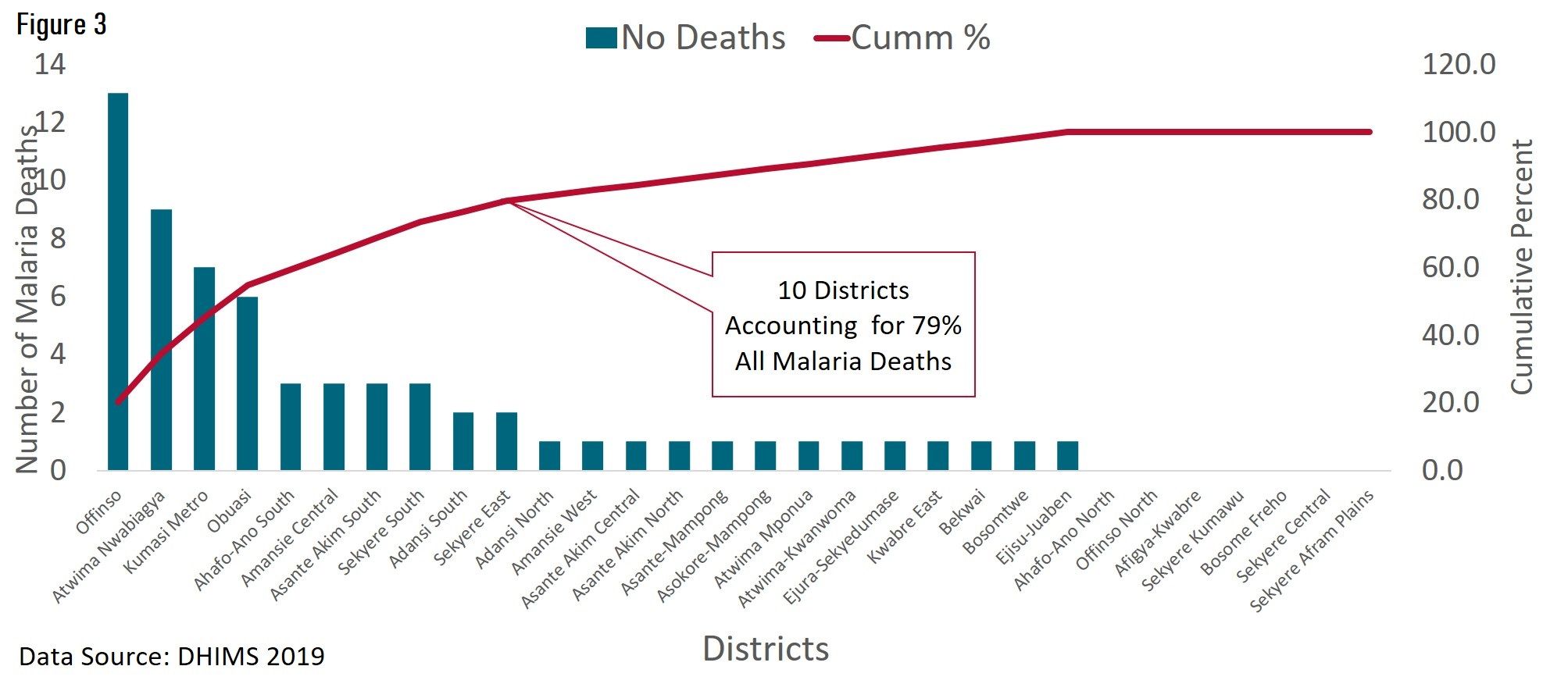 The result of selecting districts and facilities using Pareto Charts is seen in Figures 3 and 4. Figure 3 sows the Distribution of Malaria Deaths in Districts in Ashanti Region, Ghana, FY-2018, and Figure 4 presents the Distribution of Malaria Deaths in Districts in Brong-Ahafo Region, Ghana, FY-2018.
The result of selecting districts and facilities using Pareto Charts is seen in Figures 3 and 4. Figure 3 sows the Distribution of Malaria Deaths in Districts in Ashanti Region, Ghana, FY-2018, and Figure 4 presents the Distribution of Malaria Deaths in Districts in Brong-Ahafo Region, Ghana, FY-2018.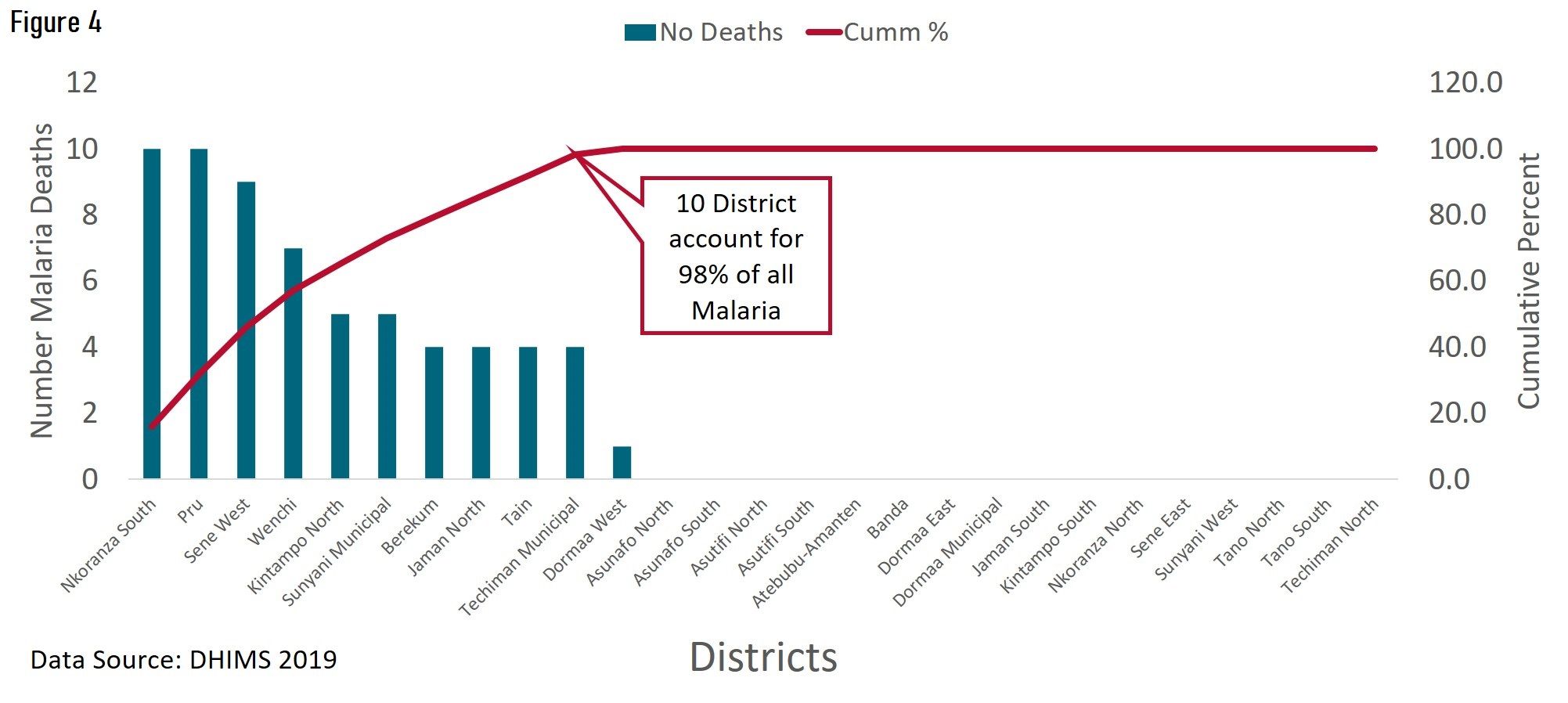
In conclusion, using routine DHMIS2 data backed by qualitative information including access to health facilities, referral patterns and facility ownership, a rational replicable basis for the prioritization of districts and facilities for intervention can be created and facilities prioritized for training based on evidence.
Regional Health Management teams have adopted a rational approach for prioritizing health facilities for intervention with limited resources with the objective of achieving the best outcome.